Full Length Research Paper
ABSTRACT
Poor and inadequate glycemic control among patients with Type 2 diabetes constitutes a major public health problem and major risk factor for development of diabetes complications. In clinical practice, optimal glycemic control is difficult to obtain because the reasons for poor glycemic control in Type 2 diabetes are complex. This study aims to determine Acute glycemic level and its association with physical activity recommendations adherence among type 2 diabetic patients in Illubabor zone southwest, Ethiopia. Institution based cross-sectional study was conducted from March 19 to May 19, 2018. Among 422 diabetic patients attending regular follow up at government health facilities in illuababor zone, southwest Ethiopia, participants were selected using systematic random sampling method.Data were collected using interview administered semi structured questionnaires; FBS was used to determine patient’s glycemic control level. Multivariable logistic regression was used to determine the independent predictor’s of diabetic patient’s Acute glycemic control level. In the current, study nearly two third (64.5%) of respondents had poor (inadequate) Acute glycemic control. While 51.8 and 38% of participants were non adherence to dietary and physical activity recommendations respectively. Patients Acute glycemic control was significantly affected by patients occupational status [AOR=0.39 (0.22-0.68)], family history of DM [AOR=0.34 (0.18-0.62)], presence of co-morbidities [AOR= 3.72(1.39-9.94)], and physical activity adherence [AOR=0.46 (0.28-0.75)]. High proportion of diabetic patients had poor Acute glycemic control. Patient’s occupational status, family history of DM, presence of co morbidities, physical activity adherence was an independent predictors of diabetic patient’s Acute glycemic control. Early identification and management of co-morbidities and delivery of focused health information physical activity recommendations should be strengthened.
Key words: Adherence, diabetic, glycemic level, Illuababor.
INTRODUCTION
Diabetes mellitus (DM) is a metabolic disorder characterized by chronic hyperglycemia due to defects in insulin secretion, insulin action, or both, effects of diabetes mellitus include long-term damage, dysfunction and failure of various organs. DM may present with characteristic symptoms such as thirst, polyuria, blurring of vision, and weight loss. In its most severe forms, ketoacidosis or a non-ketotic hyperosmolar state may develop and lead to stupor, coma and, in absence of effective treatment, death (Yigazu and Desse, 2017).
Type 2 diabetes constitutes about 85 to 95% of all diabetes. American diabetic Association (ADA) and International Diabetes Federation (IDF) estimated about 19.8 million adults were estimated to have diabetes in Africa and regional prevalence of DM is 4.9%. Out of this more than 50% lives in four highly populated countries namely: Nigeria, South Africa, Ethiopia and Tanzania, it is estimated that 439 million people would have type 2 DM by the year 2030; ageing populations, increasing urbanization, reduced physical activity and Chronic consumption of high energy, high fat diets and behavioral patterns plays critical role in the incidence of this medical problem (World Health Organization, 2016; Ogurtsova et al., 2017; Al-hayek et al., 2012).
It has been shown that hyperglycemia enhances free radical production, inducing oxidative damage, which in its turn activates the death pathways implicated in cell apoptosis and necrosis. Extant literatures have demonstrated that intermittent high glucose is more dangerous than constant high glucose medium for human umbilical vein endothelial cells (HUVECs) in culture, because in the former condition there was a marked increase in cellular apoptosis. These findings suggest that variability in glycemic control could be more deleterious to HUVECs than a constant high concentration of glucose (Tanaka et al., 1999; Risso et al., 2001).
Presence of macro- and micro vascular complications in patients with diabetes mellitus (DM) is not only related to chronic hyperglycemia represented by glycated hemoglobin (HbA1c) but also to acute glycemic fluctuations (Caprnda et al., 2017). A1C reflects, average blood glucose concentrations over a prolonged period of time; it does not provide much information on the prevalence and amplitude of hyperglycemic blood glucose excursions experienced through short period of time. Intermittent high blood glucose exposure rather than constant high blood glucose exposure has been shown to have deleterious effect in experimental studies (Quagliaro et al., 2003; Piconi et al., 2006). Such information is highly relevant because acute hyperglycemic episodes have been associated with the development of diabetes complications independent from A1C levels, In addition, the level of glycemic variability, which reflects the frequency and amplitude of upward and downward blood glucose excursions throughout the day, has recently been implicated in the development of diabetes complications (Jan-Willem VD and van -Loon JL, 2015; James BM et al., 2002).
Glycemic control is more than just taking medicine; Most behaviors that are appropriate for everyone to prevent diabetes are also appropriate for people who are diagnosed with diabetes. These same behaviors can help people with diabetes manage their condition and prevent complications. These behaviors includes weight management, healthy eating, participation in regular physical activity, tobacco free habit, adequate sleep, participation in diabetes prevention education programs and adherence to personalized diabetes treatment plans (North carolina diabtes advisory council, 2015; Diabetes Australia, 2014; Kassahun et al., 2016).
In clinical practice, optimal glycemic control in Type 2 diabetes is difficult to achieve because of intricate reasons, both patient and health care provider related factors may contribute to poor glycemic control (Wallace et al., 2000). Study conducted in different parts of Ethiopia, Ambo, Mekele, Gonder and TikurAnbessa Specialized Hospital reported different level of poor glycemic control among type 2 diabetic patients which extends from 48 to 80% (Minyahil A et al., 2014; Tadele et al., 2016; Solomon et al., 2015 Yohannes T et al., 2018), another study conducted in Saudi arebia and India both reported poor glycemic control among three fourth of patients, patients poor level of glycemic control were significantly associated with patients sex, age, BMI, hypertriglyceridemia, hypercholesterolemia treatment modality, family history, duration of diabetes mellitus, diabetic management and diabetic complications (Almutairi et al., 2013; Gopinath et al., 2013).
Significance of the study
Similar to any developing countries, Ethiopia generally and the study area particularly is currently undergoing one of the most rapid epidemiological transitions. Despite the facts that increased diseased burden and critical importance of glycemic control, majority of the patients fail to achieve adequate level of glycemic control and factors responsible for poor glycemic control are also complex and interrelated. As a result, this study was conducted to determine Acute level of glycemic control and identify factors associated with poor glycemic control among patients with Type 2 diabetes who attended regular follow up at two government hospitals in illuababor zone, south western Ethiopia.
MATERIALS AND METHODS
Study area and period
Institution based cross sectional study was conducted from March 19 to May 19, 2018, in Ilu Abba Bora Zone of Oromia Region,south western Ethiopia. Metu Town is the administrative center of the zone which is 600 km south west of Addis Ababa. The study was conducted in two governmental hospitals (Metu Karl Referral Hospital and Darimu Hospital) both gives follow up care for diabetic and NCD patients.
In the current study, all adults diagnosed with type 2 diabetes mellitus who were on regular follow up at MKRH and Darimu hospital NCD follow up units were considered as a source population and selected adults diagnosed with type 2 diabetes mellitus who were on regular follow up at MKRH and Darimu hospital NCD follow up units were a study populations. Critically ill and patients with severe mental illness were excluded from the study.
Sample size determination and sampling technique
Sample size was separately calculated for the outcome (Gycemic control) and for each associated factors using previously published parameters and the largest sample size was taken using the assumption of 50% poor glycemic level which was reported in a study conducted another part of Ethiopia (Minyahil A et al., 2014) 95% level of confidence (α), 80% power (ß) and 10% non-response rate, the final sample size was 422. The final sample size was allocated proportionally to two hospitals based on their number of diabetic patients on follow-up accordingly 756 and 338 patients were in a regular follow-up in MKRH and darimu hospital respectively accordingly 291 and 132 patients were proportionally taken from Metukarl hospital and Darimu Hospital respectively. Finally study participants were selected using systematic random sampling technique.
Data collection method and tools
Semi-structured interviewer administered questionnaire was used to collect socio-demographic. Patients health profile, including; duration of disease, type of treatment, co morbidity, family history, and Fasting blood sugar was reviewed from patient follow up card. Diabetic health belief was assessed using 26 questions, 5 questions each assessing the perceived susceptibility to diabetes complications and perceived severity constructs, perceived benefit and barrier to diet and physical regimen was assessed using 4 and 8 questions respectively likewise self-efficacy towards following dietary and physical activity recommendation was assessed by 4 questions. The other section of the tool assess emotional and active or instrumental family and non-family members support which was modified from “The Diabetes Social Support Questionnaire-Family Version: developed in 2002 (Greca et al., 2002). Dietary adherence status was assessed using 12 item scale (Worku et al., 2015) which is modified from eight-item Morisky medication adherence scale (MMAS-8) which was developed in 2008 (Morisky, 2011; Woods et al., 2011) )(World Health Organization(WHO), 2009).
Data processing and analysis
Data were cleaned, edited, coded and entered to Epi data version 3.1 and was exported to SPSS windows version 20 for analysis. Exploratory data analysis and Descriptive statistics including proportion, percentage, ratios, frequency distribution, mean and standard deviation was used to describe the data. Wealth index was constructed using the principal component analysis(PCA) form 27 items after checking all assumptions. Bivariate logistic regression analysis were done to see the association between individual explanatory and outcome variables; variables with P-value <0.25 were a candidate for multi variable logistic regression. Odds ratio with 95% C.I was used to measure the strength of association between dependent and independent variables. P value <0.05 was used to declare level of statistical significance.
The scores of each diabetic health belief construct were summed up, to come up with a single scoring for each construct, for every respondent. Participants were labeled to have high or low level of individual constructs based on correct response of mean value as a cutoff, social support scores of every respondent were also summed up. Participants were labeled to have poor or good social support based on mean value. Dietary adherence status score was computed by taking the mean values of 12 questions assessing patients’ dietary recommendation adherence.
Ethical consideration
Ethical clearance and permission were obtained from the Research Review Board of Jimma University and offered to illuababor zone Health office and respectivehospital administrative officials, information about the objective of the study, confidentiality, autonomy and justice were explained for the participants during data collection. Informed verbal consent was obtained from each study participant.
Operational and standard definitions
Good glycemic control
Fasting blood glucose of 70–130 mg/dl (29).
Poor glycemic control
Fasting blood glucose of<70 mg/dl and >130mg/dl (29).
Acute glycemic control
In the current study, FBS measured during the last follow up visit was considered as recent glycemic control.
Adult
A person who has reached 18 years old.
Diet
This refers to the recommended diet for people with DM who should eat small meals spread throughout the day (at least 5/day), eat fruits and vegetables daily, and eat foods high in fibers and whole grain but low in fats, sugars and carbohydrates that have high glycemic index (30).
Physical activity
This refers to bodily movement produced by the contraction of skeletal muscle that requires energy expenditure in excess of resting energy expenditure (Westerterp, 2013).
Non adherent to dietary recommendation
These are those who scored the mean and above the overall dietary recommendation score.
Adherent to dietary recommendation
These are those who scored below the overall mean dietary recommendation score.
Non Adherent to physical activity recommendation
These are those who scored less than 600 METs per week based on the GPAQ incorporated scoring mechanism (World Health Organization, 2009).
Adherent to physical activity recommendation
These are those who scored greater than 600 METs per week based on the GPAQ incorporated scoring mechanism (World Health Organization, 2009).
RESULTS
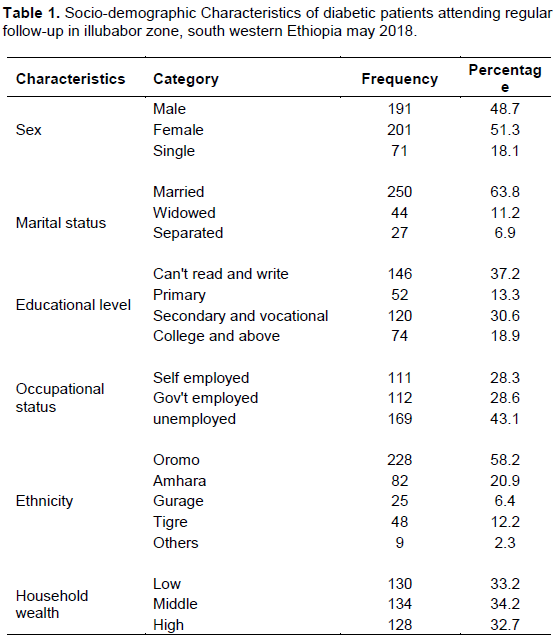
A total of 392 respondents participated in the study, yielding a response rate of 92.9%; females account for 51.3%. The mean age of respondents were 47 (SD±13); nearly two third (63.8%) of respondents were married, 37.2% of them cannot read and write, regarding occupational status. 43.1% of respondents were government employers, similarly more than half (58.2%) of respondents were Oromo by ethnicity furthermore one third of the participants were in the lowest wealth tertiales (Table 1).
Clinical characteristics of study participants
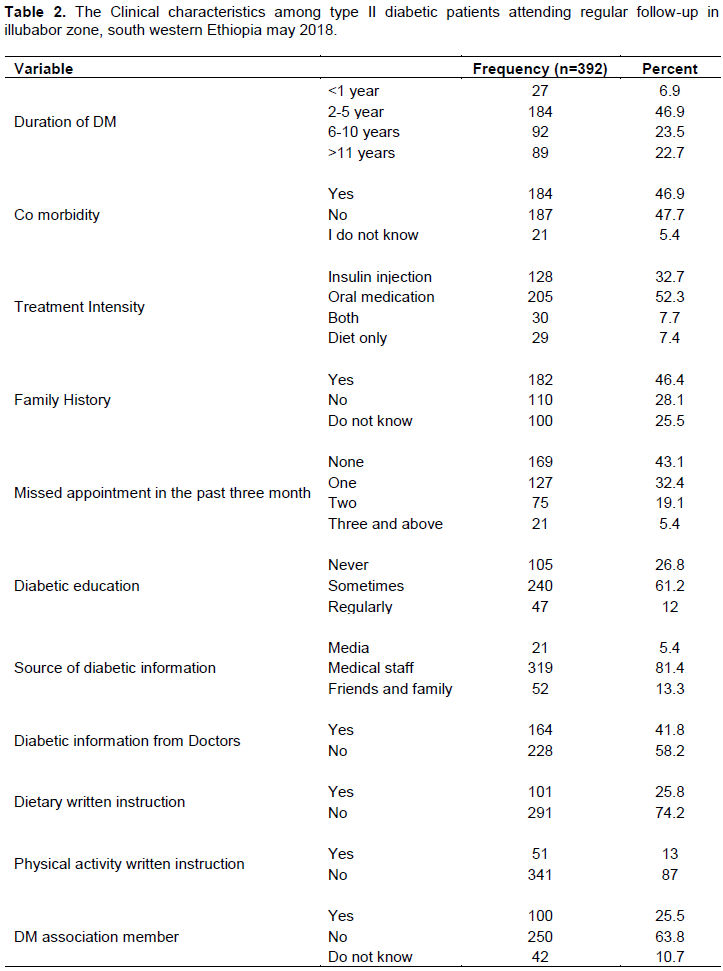
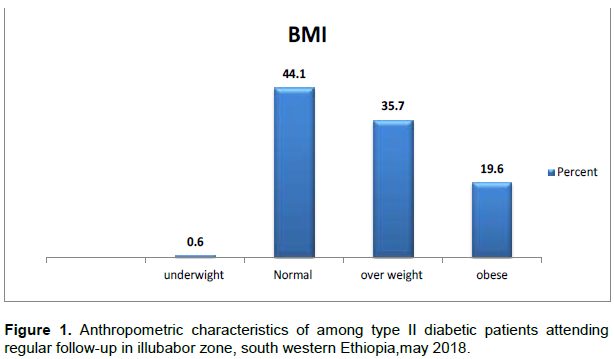
The mean illness duration since diagnosis was 6.9 (SD±5.3) years. One hundred and eighty two (46.4%) patients reported that they had family history of DM and nearly half of the respondents (46.9%) had additional co-morbidity. More than half of patients (52.3%) used oral hypoglycemic agent. One hundred and sixty nine (43.1%) of patients never missed their diabetic follow up appointment in the past three month. Additionally more than one fourth of participants, 105 (26.8%) reported that they did not attend diabetic education while 47 (12%) attended regularly. In the current study, one fourth (25.5%) of diabetic patients were member of Ethiopian diabetic association, the mean BMI was 27 (SD±13) and 44.1% of respondents had normal BMI while 19.6% of respondents were obese. Furthermore 62 (17.3%) of the respondents had abdominal obesity (Table 2 and Figure 1).
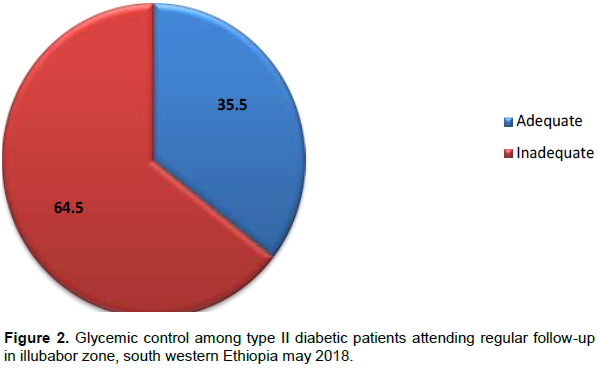
In the present study, level of glycemic control was assessed using FBS; the mean FBS was 183.4 mg/dl and accordingly 64.5 % of respondents had inadequate glycemic control (Figure 2).
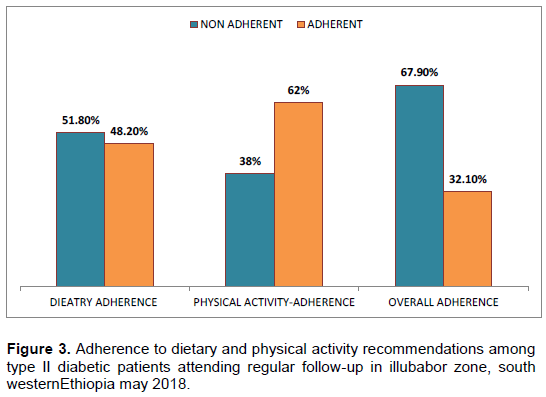
Diabetic patient’s dietary and physical activity recommendation adherence
The present study showed 51.8% of the respondents were non-adherent to dietary recommendation while 38% of participants were non adherent for physical activity recommendations and overall non adherence accounted for 67.9% (Figure 3).
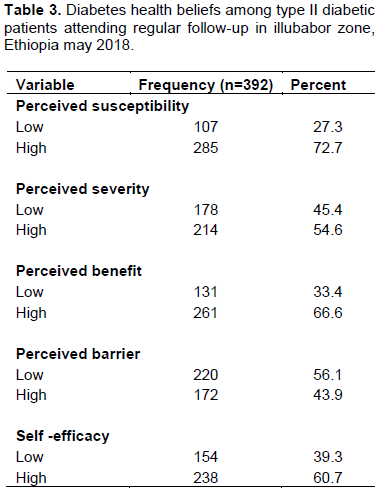
In the present study patients diabetic health beliefs was assessed, nearly three fourth of participants had high perceived susceptibility, while diabetic patients with high perceived severity, perceived barrier and self-efficacy accounts 54.6, 43.9 and 60.7% respectively (Table 3).
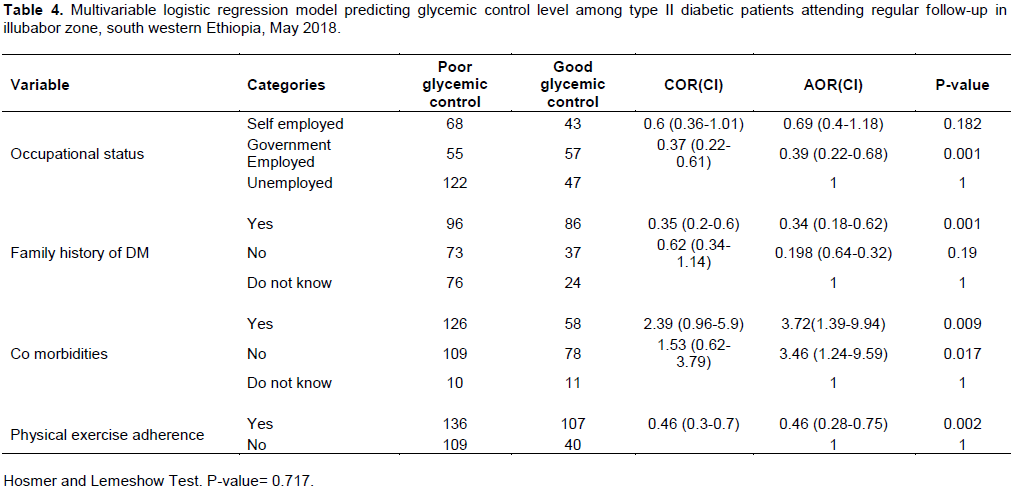
In multivariable logistic regression analysis, patient’s occupational status, family history of DM, co-morbidities, physical activity recommendation adherence and written diabetic instruction were an independent predictors of diabetic diabetic Acute glycemic control (Table 4). Patients who were government employers had less odds than unemployed patients [AOR=0.39 (0.22-0.68)], similarly patients who had diabetic family history had 0.34 less odds than patients who did not know their family history [AOR=0.34 (0.18-0.62)]; patients who had another co-morbidities were 3.7 times likely to have poor glycemic control [AOR= 3.72(1.39-9.94)] furthermore patients who were adherent to physical activity recommendations were 54% less likely to have poor glycemic control.
DISCUSSION
Good glycemic control among T2DM patients prevents short-term complications, decrease risk of long-term complications and decrease health care resource use and costs. In the current study, nearly two third (64.5%) of respondents had poor (inadequate) glycemic control.
This study also reported higher dietary and physical activity non adherence, and this could be one of the possible justification for the high proportion of poor glycemic control, on the other hand the result is comparable with a study finding from Gonder (Solomon et al., 2015), however the finding is lower than findings from Tikurambesa, Malysiaand India (Ababa et al., 2018; Almutairi et al., 2013; Gopinath et al., 2013) and higher than a finding from northern Ethiopia, Mekelle, which reported 48.7% had poor glycemic control (Tadele et al., 2016), the discrepancy might arise fromin socio-cultural, economic and dietary consumption difference among study populations, in addition the variation might be due different blood glucose measurement modality used. In this study, fasting blood sugar was used to monitor patient’s blood glucose level while most of referenced studies used glycated hemoglobin, furthermore the variation might arise from difference in level of urbanization between conducted comparatively in less urbanized area. It is well known that urbanization is commonly associated with motorized way of life and unhealthy eating pattern like consumption of ready-to-eat food products containing high levels of salt, sugar and fat (Tadele et al., 2016), which are the common factors adversely affect patients glycemic control.
In the current study patients occupational status was found to be an independent predictor of patients Glycemic control, the result is in line with finding from Jimma University Teaching Hospital, which also indicated a positive correlation between patient’s occupational status and glycemic control. The observed association might be due to low educational achievements among unemployed patient’s; it is known that education offers opportunity to learn more about health generally and glycemic control particularly. Likewise, the result is also supported by low economic level of unemployed patients which directly interfere with patients capacity to afford medicine and strictly follow healthy dietary and physical activity recommendations.
The present study point out that patients who know their family diabetic history were found to less likely to have poor glycemic control; the result is incoherent with the study done in Saudi Arabia and Malaysia; both reported significantly higher proportion of poorly glycemic control among patients who know their family history of diabetes (Almutairi et al., 2013; Riyadh and Alzaheb, 2018); the disagreement might arise from the possible lifestyle and family attachment difference between study setups. In the current study area, family members commonly lived in a common shelter and there was also a strong social attachment which facilitates exchange of health information between family members, in view of the fact that diabetic self-care is a continuous activity, it’s likely for other family members to gain diabetic self-care knowledge’s.
This study also revealed that presence of other co morbidities was associated with poor glycemic control; the association can be explained by the possible effect of co-morbidities in precipitating hyperglycemia among diabetic patients, likewise the result might also be due to likely diversion of patient’s attention from the routine diabetic self-care to management of acute co–morbidities symptoms, which likely impose adverse economic, psychological and physical pressure which likely had undesirable effect on patients adherence towards health recommendations and later leads to inadequate glycemic control.
In this study, adherence to physical activity recommendation was found to be an independent predictor of diabetic patients Acute glycemic control. The result is similar with the study conducted in Tepi (southern Ethiopia) (Biru, 2017); Netherlands (Jan-Willem VD and Luc JCV , 2015) and Yemen (Rita de Cássia, 2011). A healthy lifestyle with regular physical activity are very important tools in reaching and maintaining an adequate glycemic control in patients with diabetes. The benefits of exercise for glycemic control are largely explained by an increase in whole-body insulin sensitivity furthermore exercise also lowered glycemic variability throughout the day, indicating a decline in the frequency and/or amplitude of glucose fluctuations.
Although this study provides basic information addressing knowledge gap, institutional based nature of the study might not infer for other diabetic patients. The cross-sectional nature of thestudy design does not show temporal relationship or causality, additionally in this study, contrary to scientific plausibility, diabetic health belief and patients dietary adherence were not found tobe predictors of patients glycemic level, this might arise from sample size, study design used and some biases in particular recall and social desirability bias.
CONCLUSION AND RECOMMENDATIONS
The study found that majority (64.5%) of diabetic patients had poor glycemic control. Occupational status of patients, family diabetic history, co-morbidities, and physical activity adherence was found to be independently associated with patient’s glycemic control level. Therefore early identification and management of co-morbidities should get due attention during regular diabetic follow up sessions and Health professionals should give due attention and take sufficient time while delivering information’s about physical activity recommendations.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGEMENTS
The authors would like to thank study participants and staffs who are working in the respective unit for their kind support.
REFERENCES
|
Al-hayek AA, Robert AA, Nusair HM, Al-eithan MH (2012). Association between diabetes self-care, medication adherence, anxiety, depression, and glycemic control in type 2 diabetes, Saudi Med Journal 33(6):681-683. |
|
|
Alison BE, Jackie LB, Marjorie, Stephanie AD, Marion JF, Elizabeth JMD, Joshua JN, Robin N, Cassandra LV, Patti U, William SY (2014). 'Nutrition Therapy Recommendations for the Management of Adults With Diabetes', Diabetes Care 37(Supplement_1):120-143. |
|
|
Almutairi MA, Said SM, Zainuddin H (2013). Predictors of Poor Glycemic Control Among Type Two Diabetic Patients, American Journal of M edicine and M edical Sciences 3(2): 17-21. |
|
|
American Diabetes Association (ADA) (2013). 'Standards of medical care in diabetes - 2013', Diabetes Care 36(SUPPL.1). |
|
|
Biru TT (2017). Glycemic Control and its Determinants among Ambulatory Patients with Type 2 Diabetes, Journal of Diabetes and Metabolism 8(8). |
|
|
Gopinath B, Sri-Sai PM, Jayarama NPK (2013). study of factors associated with poor glycemic control in Type -2 Diabetic patients, Global Journal of Medicine and Public Health 2(2):1-5. |
|
|
Greca AM, Bearman KJ (2002). 'The Diabetes Social Support Questionnaire-Family Version : Evaluating Adolescents' Diabetes- Specific Support From Family Members', Journal of Pediatric Psychology 27(8) 665-676. |
|
|
James BM, David MN, Ralph BD, Peter WFW (2002). 'Fasting and Postchallenge Glycemia and Cardiovascular Disease Risk', Pathophysiology/Complications 25(10):1845-1850 |
|
|
Jan-Willem VD, Luc JCV (2015). Exercise Strategies to Optimize Glycemic Control in Type 2 Diabetes: A Continuing Glucose Monitoring Perspective, SPECTRUM.DIABETESJOURNALS.ORG 28:24-31. Kassahun T, Eshetie T, Gesesew H (2016). Factors associated with glycemic control among adult patients with type 2 diabetes mellitus: a cross-sectional survey in Ethiopia, BMC Research Notes. BioMed Central 9(1):78. |
|
|
Martin C, Dasa M, Pablo FO, Boris K, Emmanuel E, Luis R, Peter K, Ioana M, Ludovit (2017). Glycemic Variability and Vascular Complications in Patients with Type 2 Diabetes Mellitus, Folia Medica, 59(3):270-278. |
|
|
Minyahil A, Chala D, Jimma L, Gobezie T, Gurmu T, Hunduma D (2014). Factors Associated with Poor Glycemic Control among Patients with Type 2, Endocrinology & Metabolic Syndrome 3(4):2-7. |
|
|
Morisky DE, Di-Matteo MR (2011). Improving the measurement of self-reported medication nonadherence:, clinical epimology, 64(3). |
|
|
North Carolina Diabtes Advisory Council (2015). Diabetes Prevention and Management 2015-2020. Rita- de CA, PhiliPPi Ts (2011). Identification of malnutrition risk factors in hospitalized patients, Revista da Associação Médica Brasileira 57(6):623-629. |
|
|
Ogurtsova K, Fernandes JDR, Huang Y, Linnenkamp U, Guariguata L, Cho NH, Cavan D, Shaw JE, Makaroff LE (2017). IDF Diabetes Atlas: Global estimates for the prevalence of diabetes for 2015 and 2040, Diabetes Research and Clinical Practice. Elsevier B.V., 128, pp. 40–50. |
|
|
Parinya CH, Rebecca KS, Nita GF, Robert NL, Kay-Tee KH, Nicholas JW, SIMON JG (2011). Incidence of Type 2 Diabetes Using Proposed HbA 1c Diagnostic Criteria in the European Prospective Investigation of Cancer – Norfolk Cohort, Epidemiology/Health Services Research 34. |
|
|
Piconi L, Quagliaro L, Assaloni R, Da-Ros R, Maier A, Zuodar G, Ceriello A (2006). Constant and intermittent high glucose enhances endothelial cell apoptosis through mitochondrial superoxide overproduction, Diabetes/Metabolism Research and Reviews 22(3):198–203. |
|
|
Quagliaro L, Piconi L, Assaloni R, Martinelli L, Motz E, Ceriello A. (2003). Intermittent High Glucose Enhances Apoptosis Related to Oxidative Stress in Human Umbilical Vein Endothelial Cells: The Role of Protein Kinase C and NAD(P)H-Oxidase Activation, Diabetes 52(11):2795-2804. |
|
|
Rasool-Hassan BA (2013). Overview on Diabetes Mellitus (Type 2), Journal of Chromatography and Separation Techniques 4(3):7064. |
|
|
Risso A, Mercuri F, Quagliaro L, Damante G, Ceriello A (2001). Intermittent high glucose enhances apoptosis in human umbilical vein endothelial cells in culture, American Journal of Physiology-Endocrinology and Metabolism 281(5):E924-930. |
|
|
Riyadh AA, Abdullah HA (2018). The prevalence and determinants of poor glycemic control among adults with type 2 diabetes mellitus in Saudi Arabia, Dove press open access to scientific and medical research pp. 15-21. |
|
|
Solomon MA, Yemane B, alemayehu W, Shitaye A, Nebiyu M (2015). evel of sustained glycemic control and associated factors among patients with diabetes mellitus in Ethiopia : a hospital-based cross-sectional study, Dovepress pp. 65-71. |
|
|
Tadele E, Abrahaley M, Hailekiros G, Getu K, Dagim A, Yerra R (2016). Factors Associated with Poor Glycemic Control in Type 2 Diabetic Patients Investigated at Ayder Referral Hospital, Human Journals (IJPPR). |
|
|
Tanaka Y, Gleason CE, Tran TOP, Harmon JS, Robertson PR (1999). Prevention of glucose toxicity in HIT-T15 cells and Zucker diabetic fatty rats by antioxidants., Proceedings of the National Academy of Sciences of the United States of America, 96(19):10857-62. |
|
|
Wallace TM, Matthews DR (2000). Poor glycaemic control in type 2 diabetes : a conspiracy of disease, suboptimal therapy and attitude, Q J Med pp. 369-374. |
|
|
Westerterp KR (2013). Physical activity and physical activity induced energy expenditure in humans: Measurement, determinants, and effects, Frontiers in Physiology pp. 1-11. |
|
|
Worku A, Abebe SM, Wassie MM (2015). Dietary practice and associated factors among type 2 diabetic patients : a cross sectional hospital based study , Addis Ababa , Ethiopia, Springer Plus 4:1-8. |
|
|
World Health Organization (WHO) (2016). Global report on diabetes. |
|
|
World Health Organization (WHO) (2009). Global Physical Activity Questionnaire. |
|
|
Yigazu DM, Desse TA (2017). Glycemic control and associated factors among type 2 diabetic patients at Shanan Gibe Hospital, Southwest Ethiopia, BMC Research Notes. BioMed Central 10(1):1-6. |
|
|
Yohannes T, Adamu A, Tedla K, Wondimu A (2018). Magnitude of glycemic control and its associated factors among patients with type 2 diabetes at Tikur Anbessa Specialized Hospital, PLoSONE 13(3):5-16. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


