Full Length Research Paper
ABSTRACT
This study aimed to use carbohydrate counting as an educational tool to improve the diet habits and reduce fat mass in obese children exposed to videogames. It involved analytical and comparative pilot study in 10 children, 5 to 10 years of age with obesity and who were exposed to video games for more than five hours a day. It formed two study groups (five in each). One used carbohydrates count tool plus a diet plan and food orientation and the other group, although similar but was without the counting carbohydrates tool. To both groups, anthropometric (fat mass), biochemical, dietetics and clinical indicators were measured. The reduction of body fat in the 10 children was 4%, with a reduction in the consumption of simple sugars. In making the comparison, at the end of the intervention there was decreased consumption of sugar-sweetened beverages and food and an increase in the consumption of vegetables. No significant correlation was found between carbohydrate consumption and exposure to video games and also there was no difference (p < 0.05). The carbohydrate count tool improved the consumption of vegetables and decreased consumption of sugar-sweetened beverages and food, but was not clearly so for the fat mass reduction. These early findings showed a first approximation to apply this experience in a large sample.
Key words: Sugar-sweetened beverages, body fat, obesity, video games, children.
INTRODUCTION
The prevalence of childhood obesity has been increasing since the 90s. In 2010 it was estimated that 43 million children worldwide were overweight and obese; 35 million of them lived in developing countries (Méndez et al., 2007; Martinez et al., 2011). In Mexico, according to the 2012 Health and Nutrition Survey (ENSAUT, 2012), the overall prevalence of overweight and obesity combined is 34.4% (19.8 and 14.6%, respectively), with 5,664,870 school-aged children making up this number (Trejo et al., 2012).
Overweight and obese children are at a higher risk of suffering from metabolic diseases such as diabetes mellitus (DM), hypertension, arteriosclerosis, and other orthopedic, respiratory, digestive, dermatological, neuro-logical and endocrine conditions, as well as certain types of cancer at an early age (Martinez et al., 2011; Trejo et al., 2012; Chiesa et al., 2005). An estimated 55% of metabolic diseases, such as child resistance to insulin have been linked to the amount of body adipose tissue, which is also the main risk factor for metabolic syndrome (Chiesa et al., 2005; Scavone et al., 2010). Lifestyle factors have a direct impact on the development of obesity and its consequences. A personalized healthy diet with a food intake suited to the individual’s socio-cultural context promotes weight loss, reduces adipose tissue, improves insulin resistance and prevents the development of chronic degenerative diseases (Rodríguez, 2006).
Children in both urban and rural areas have adopted watching television and playing video games as recrea-tional activities (Poletti and Barrios, 2007). According to the World Health Organization (WHO), the rise in time spent watching television or playing video games is directly responsible for 60% of children worldwide failing to fulfill the minimum 30-min-a-day recommendation for physical activity (Denot et al., 1998). It is estimated that 50% of children aged four to six have been exposed to video games, mostly girls (56%) (Poletti and Barrios, 2007). A study in the US found that children spend an average of 5.5 h a day engaged in these activities, which amounts to a full working day for an adult (Poletti and Barrios, 2007).
Another US study defines 7 h and 57 min as the period of time that determines an increased risk of developing obesity due to sedentarism in children and teenagers (González and Atalah, 2011). The risk of obesity increases 1.7 times after being exposed for ≥ 4 h to television or video games. Other studies have found that children aged 9 ± 1.5, after being exposed to video games for five hours, start developing a number of physiological obesity and obesity-related symptoms such as increased cardiovascular activity, breathing responses and cortisol release due to the stress produced by the constant noise and music (Denot et al., 1998; National Institute of Public Health México, Ministry of Health, 2012; Yeste and Carrascosa, 2011).
Eventhough obesity is a multifactorial disease, as described earlier, an important correlation has been found between obesity and television and video game use. Obesity is also linked to the development of diabetes mellitus type 2 and to inflammatory responses (Rodríguez, 2006). The combination of a low-glycemic diet and regular aerobic exercise has positive effects on postprandial glucose levels, thus reducing hyperglycemia and the inflammatory response (Kelly et al., 2011). The high prevalence of childhood obesity in Mexico, linked to bad eating habits, and the sedentary lifestyle associated with video games could lead to a future of diabetes mellitus, hypertension and hypertriglyceridemia for these children. Helping to prevent this is the main motivation for our study. Our goal was to develop and test an educational carbohydrate-counting tool to help promote healthy eating and improve the eating habits (that is, de-crease the intake of sugary foods and sugar-sweetened beverages) of obese children habitually exposed to video games. Its impact should be measurable as a decrease of adipose tissue over a short period of time.
MATERIALS AND METHODS
An analytical, comparative and longitudinal study was conducted for four months in a total of 10 children aged 5 to 10 years. The study was approved by the Ethical and Research Committees of the General Regional Hospital of the Ministry of Health, in Guanajuato, Mexico. The children were recruited between January and May, 2013 from the outpatient clinic at the Uriangato General Hospital, in Uriangato, Guanajuato. A total of 50 children were invited to participate through a series of informational meetings conducted in primary and secondary state health care facilities. Of an original 24 participating children, 10 were able to complete the process due to the limitations of the study. Inclusion criteria were a body mass index (BMI) above the 85th percentile and exposure to video games for more than five hours a day. Patients with an existing healthy eating plan were not considered. Informed consent was obtained from the parents and two groups of five children each were formed. Consultation appointments were scheduled for each child according to their, respective group. Each child was seen once every 15 days (four appointments in total), with an average appointment duration of 1.5 h.
Lifestyle was assessed using the IPAQ (International Physical Activity Questionnaire) (IPAQ, 2012). Each patient’s nutritional state was evaluated using anthropometric, biochemical, clinical and nutritional parameters. As to anthropometric indicators, weight was measured with a SECA® scale (1 g accuracy). Four subcutaneous folds (bicipital, tricipital, subscapular and suprailiac) were also measured using a Lange® plicometer (1 mm accuracy). These measurements were used to determine initial and final percentages of fat using the Durnin equation (Secretaría de Salud, Guanajuato México (in spanish), 2010).
For the biochemical indicators, 8 h fasting samples were obtained from the children to measure glucose, glycated hemoglobin and lipid profile (triglycerides and cholesterol). These biochemical indicators were analyzed and processed by hospital laboratory technicians (American Diabetes Association, 2010). The measurements were analyzed at the beginning and at the end of the study. To assess dietary indicators, each consultation included a 24-h recall using food replicas. Interviews were conducted to investigate eating habits at the first and last interventions (Rodríguez et al., 2008). Each group of participants received a different intervention. Group A was prescribed a hypocaloric plan, 500 kcal lower than the estimated maintenance energy intake, based on the Guanajuato Ministry of Health’s Guidelines, which recommend a calorie intake between 1000 and 1500 kcal for children. The caloric distribution among the three macronutrients (proteins, fats and carbohydrates) was 60% for carbohydrates, 15% for protein and 25% for lipids, in keeping with official guidelines (Secretaría de Salud, Guanajuato México (in spanish), 2010). Group B (hypocaloric plan plus carbohydrate-counting tool) was prescribed a hypocaloric plan 500 kcal under maintenance energy intake, with 55% carbohydrates, 15% protein, and 30% lipids. Caloric requirements were calculated using the Harris-Benedict equation, adapted for a population aged 1 to 18 (Secretaría de Salud, Guanajuato México (in spanish), 2010). No patient was prescribed an intake below 1000 kcal (Table 1).
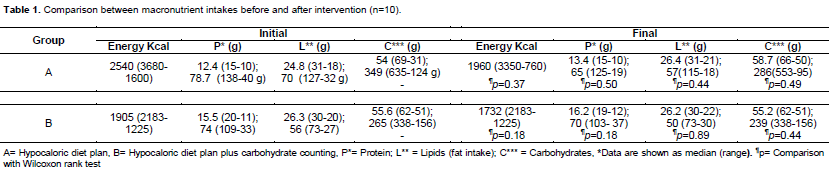
Three to four (45 to 50 g) servings of carbohydrates per meal were prescribed. Servings of fruit, cereal, pulses and milk were also recommended (Pérez et al., 2008). Dietary guidance was provided as to basic carbohydrate-counting, where 15 g of carbohydrates equals one serving. Patients were able to identify various food groups as established by the Mexican food system equivalents: vegetables, fruit, sugar, cereal, pulses, animal products, milk, oil and fat (Pérez et al., 2008; Karmeen, 2005). From these they learned to identify the ones with high carbohydrate contents, examples of foods belonging to each food group and the recommended servings for some types of foods (Karmeen, 2005).
The learning strategies used included presenting interactive materials and connecting elements. The materials used were flashcards, posters and food replicas. A 2.5 to 2.7% fat loss was considered positive in terms of reducing long-term risk of obesity-related diseases, in keeping with recent studies (Hlavatý et al., 2010).
Statistical analysis
Results are described as median and range. A Wilcoxon rank test was used to compare baseline medians with the final measurements (after the four-month intervention period). These values were later compared using a Z-test. Spearman’s rank correlation was considered between the different parameters analyzed: fat, carbohydrates, lipids, cholesterol and triglycerides, exposure to video games, age, glucose and glycated hemoglobin. A value of p < 0.05 was de?ned as the level of signi?cance. The data were processed using Minitab 16 statistical software and Microsoft Office Excel 2013®.
RESULTS
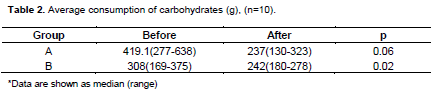
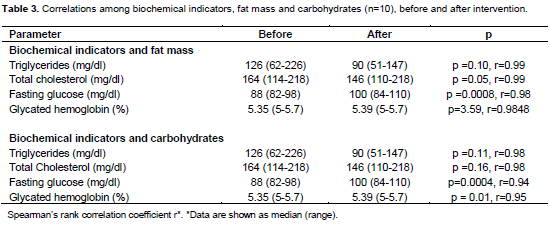
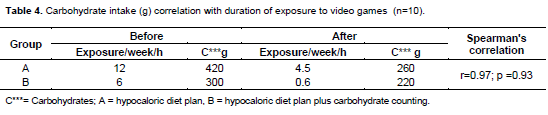
Patients were aged 5 to 10; 5 of them were male and 5 female. Four months after the dieting intervention, the change in body fat was 4% in both groups: 5% for group A (from an initial 28% to a final 23%) and 4% for group B (from 28% to 24%). Consumption of carbohydrates assessed in both groups by counting changed towards a reduced final intake (Table 2). After comparing changes between initial and final carbohydrate consumption, a 4% decrease in body fat was observed, with intakes of 210 g of fruit, cereal, pulses and milk. As to correlations between biochemical indicators and total carbohydrate intake, a positive, significant correlation was observed with fasting glucose levels (p = 0.0004, r = 0.94) and glycated hemoglobin (p = 0.01, r = 0.95) (Table 3). Fat mass and biochemical indicators showed strong correlations in total cholesterol (p = 0.05, r = 0.99) and fasting glucose (p = 0.0008, r = 0.98). No correlation was found between video game use and carbohydrate intake (p = 0,93, r = 0.97) (Table 4).
DISCUSSION
The aim was to determine whether this sort of intervention was more efficient in reducing body fat than simply prescribing a hypocaloric diet. A 4% fat reduction was found when 17 servings of carbohydrates (210 g) a day were distributed among 5 meals.
The resulting reduction in fat mass coincides with previous studies by Foster et al. (2003), who focused on reducing fat with a low-carbohydrate diet. Their results showed that there was a decrease in the risk of early complications caused by childhood obesity when fat decreased by 4% (Foster et al., 2003). Even though our results on reduction coincide with those of Foster et al. (2003) the dietary changes we introduced based on difference in counting carbohydrates. Our counts recommended a 50 to 55% carbohydrate intake and no less (Karmeen, 2005; Tomoyuki, 2007). By contrast, Foster et al. (2003) recommended a 20 to 30% carbohy-drate intake (Foster et al., 2003). In turn, Mullan et al. (2004) studied the effects on growth and development of reducing carbohydrates to very low levels (20 to 30%) (Mullan et al., 2004). A moderate reduction in carbohy-drate intake was shown to be effective by Bourges et al. (2004) whose recommended 55 to 63% carbohydrate percentages had fewer collateral effects on metabolism when compared to lower levels (Carvalhal et al., 2007; Bourges, 2004; Demol et al., 2009).
The educational carbohydrate-counting tool helps keep the carbohydrate percentage at 55% and focuses on avoiding sugars while maintaining a balance between reducing simple carbohydrates and increasing complex carbohydrates. In the long term there is a sustained reduction of fat that does not compromise the metabolism in ways that may affect the child's development (Carvalhal et al., 2007; Demol et al., 2009). Children following this plan have an appropriate diet, with a balanced distribution of food types that does not interfere with their development (Bourges, 2004; Demol et al., 2009; Foster et al., 2010).
The carbohydrate-counting tool contributed to finding significant differences between initial and final glucose levels (r = 0.32; p = 0.0004) and glycated hemoglobin (r = 0.2892; p = 0.01) when simple carbohydrate intake was reduced. (Demol et al. (2009) and Carmel et at. (2011) argued that the main food group related to postprandial glucose control is carbohydrates; reducing them im-proves glucose metabolism (Demol et al., 2009; Carmel et al., 2011). Evidence shows that decreasing total carbohydrate intake can reduce the risk of obesity-related complications, especially in children, whose sugar intake may be excessive because of their preference for sweets (Poletti and Barrios, 2007; Perrot et al., 2006; Carmel et al., 2011). Carbohydrate counting does not involve any recommendations regarding sugar intake. 35 It makes up for the daily requirements for children by incorporating carbohydrates from other sources such as pulses, milk and cereal (Karmeen, 2005; Kulkarni, 2005; Zipp et al., 2011).
Regarding the unchanged cholesterol levels, Perrot et al. (2006) in earlier studies clearly described reductions in blood pressure and circulating triglycerides achieved by decreasing carbohydrate intake (Perrot et al., 2006). Unfortunately, the sample size in this study was limited because patient attendance dropped after the third consultation. This was due to a combination of factors: parents’ lack of interest, difficulty acknowledging their child’s habits, work-related time constraints, and children’s rejection of the diet plan and reluctance to undergo laboratory testing. The acceptance of the educational tool was low, in line with other studies on perseverance in dieting and its impact on body composition. It is reported that up to 68% of patients fail to adhere to a prescribed eating plan, which suggests that sticking to the diet is key to modifying body composition in a positive way (González et al., 2007).
A comparison of the data on frequency of food intake before and after the intervention with the carbohydrate-counting tool reveals that the daily intake of vegetables increased. This is significant, given the difficulties commonly encountered in the search for strategies to encourage eating more vegetables (Johnston et al., 2011).
The tendency to drink sugar-sweetened beve-rages like juice and soda decreased significantly; sugar as a group was avoided because it was not included for calculating servings in the eating plan. Mexico is considered the leading consumer of soft drinks worldwide (16 million liters of soda were consumed nationally in 2005) (Barquera et al., 2008). Counting carbohydrates could help revert the habit of drinking excessive amounts of soda, juice, flavored water and other sugar-sweetened drinks.
Dietary guidance based on counting carbohy-drates played a significant role in the changes revealed by the results of our study. The focus on an educational approach based on concepts patients can understand increases patients’ nutri-tional knowledge (Friedman et al., 2007), which in turn stimulates a preference for non-sugary foods. Observing healthy eating habits is traditionally considered expensive. The carbohydrate-counting tool made it possible to diversify choice by including fruit and vegetables. The decrease of fried foods and foods rich in simple carbohydrates reflects an increase in the number of informed decisions made. Counting carbohydrates was considered by most parents as a cheap option because it did not involve additional shopping expenses, as the recommended foods can be found in the regular weekly shopping basket. The key lies in keeping a record of what is eaten and of the servings eaten.
Despite its limitations, the study showed an improvement in some metabolic and habit indicators, which can have an immediate clinical application and contribute to collecting more data with further interventions.
CONCLUSION
This study found beneficial effects of a dietary intervention based on a carbohydrate-counting tool: a significant increase in the consumption of fruit and vegetables and a decrease in the consumption of fried foods and sugar-sweetened beverages (juice and soft drinks). Even though the reduction in body fat using the carbohydrate-coun-ting tool was not significant, improvements were made in terms of the food choices made. This fin-ding alone suggests that this tool could be useful in the counseling and treatment of obese children, for improving their eating habits, decreasing exposure to video games and preventing weight gain. Finally, this carbohydrate-counting tool could help parents decide which foods to eliminate from their children's diet and which to offer according to age and diet requirements.
ACKNOWLEDGEMENTS
We thank the following people for their support during our study: LDN Carolina Cabrera de la Cruz, Dr. Pablo Sánchez Gastelum, Dr. Miguel Ángel Carrillo Godínez, Dr. Antonio Orozco López, LN Joel Flores Reyes, LN Luis Fernando Sámano Orozco, LN Gabriela Guzmán Gaona, LN Cesia Karem García Torres, Dr. Julio Leyva Ruiz. We are grateful for the statistical assistance provided by: Instituto Tecnológico Superior del Sur de Guanajuato (ITSUR): Lic. Cristina Orozco, Rogelio López, MS; Professor Germán Guzmán Guzmán. Finally, special gratitude goes to the Research and Graduate Studies Unit of the University of Guanajuato (Dirección de Apoyo a la Investigación y al Posgrado, in Spanish), for their support with the translation of this manuscript.
CONFLICT OF INTEREST
The author(s) have not declared any conflict of interests.
REFERENCES
|
American Diabetes Association (ADA) (2010). Diagnosis and Classification of Diabetes Mellitus. Diabetes Care 33:62-69. Crossref |
||||
| IPAQ (2012). Assessment of physical activity: An international perspective. Res. Q. Exerc. Sport 71(2):s114-20. | ||||
|
Barquera S, Hernandez-Barrera L, Tolentino ML, Espinosa J, Ng SW, Rivera JA, Popkin BM (2008). Energy Intake from Beverages Is Increasing among Mexican Adolescents and Adults. J. Nutr. 138(12):2454-2461. Crossref |
||||
| Bourges H (2004). What is the treatment of the obese patient nutriológico? J. Endocrinol. Nutr. 12(3):120-127. | ||||
|
Carmel E, Lori KH, Burgess D, Collins EC (2011). Biting off more than you can Chew is it possible to precisely count carbohydrate? Nutr. Diet. 68(3):227-230. Crossref |
||||
|
Carvalhal MM, Padez CM, Moreira AP, Rosado MV (2007). Overweight and obesity related to activities in Portuguese children, 7-9 years. Eur. J. Public Health 17:42-46. Crossref |
||||
|
Chiesa G, Piscopo MA, Rigamonti A, Azzinari A, Bettini S, Bonfanti R, Viscardi M, Meschi F, Chiumello G (2005). Insulin therapy and carbohydrate counting. Acta Biomed 76:44-48. Pubmed |
||||
|
Demol S, Yackobovitch GM, Shalitin S, Nagelberg N, Keren Gillon M, Phillip M (2009). Low-carbohydrate (low & high-fat) versus high-carbohydrate low-fat diets in the treatment of obesity in adolescents. Pediatr. Acta 98(2):346-351. Crossref |
||||
|
Denot LS, Vardon G, Perruchet P, Gallego J (1998). The effect to attentional load on the breathing pattern in children. Int. J. Psychophysiol. 29:13-21. Crossref |
||||
|
Foster GD, Wyatt HR, Hill JO, Makris AP, Rosenbaum DL, Brill C, Stein RI, Mohammed BS, Miller B, Rader DJ, Zemel B, Wadden TA, Tenhave T, Newcomb CW, Klein S (2010). Weight and Metabolic Outcomes After 2 Years on a Low-Carbohydrate Versus Low-Fat Diet. Ann. Intern. Med. 153(3):147-157. Crossref |
||||
|
Foster GD, Wyatt HR, Hill JO, McGuckin BG, Brill C, Mohammed BS, Szapary PO, Rader DJ, Edman JS, Klein S (2003). Randomized trial of a low-carbohydrate diet for obesity. N. Engl. J. Med. 348:2082-2090. Crossref |
||||
|
Friedman AL, Snetselaar L, Stumbo P, Horn VL, Singh B, Barton AB (2007). Influence of intervention on beverage choices: trends in the dietary intervention study in children (DISC). J. Am. Diet. Assoc. 107(4):586-594. Crossref |
||||
| González C, Atalah E (2011). Regulating TV advertising of food to prevent childhood obesity. Am. Arch. Nutr. 61(3). | ||||
| González ZLI, Giraldo GAN, Estrada RA, Mu-oz RLA, Mesa SE, Herrera MC (2007). Adherence to the nutritional treatment and body composition: a cross-sectional study in patients with obesity or overweight. Rev. Chil. Nutr. 34(1):46-54. | ||||
|
Hlavatý P, Zamrazilová H, Kunesová M, Dusátková L, Sedlácková B, Hainer V (2010). Reduction of abdominal obesity and cardiometabolic health risks in obese adolescents in response to a short-term spa weight management program. Cas. Lek. Cesk. 149:537-541. Pubmed |
||||
|
Johnson KR, Appel JL, Brands M, Howard VB, Lefevre M, Lustig HR, Sacks F, Steffen LM, Wylie-Rosett J (2011). Dietary Sugars Intake and Cardiovascular Health: A Scientific Statement From the American Heart Association. Circulation 120:1011-1020. Crossref |
||||
|
Johnston AC, Palcic LJ, Tyler C, Stansberry S, Reeves SR, Foreyt PJ (2011). Increasing Vegetable Intake in Mexican-American Youth: A Randomized Controlled Trial. J. Am. Diet. Assoc. 111(5):716-20. Crossref |
||||
|
Karmeen D (2005). Carbohydrate Counting: A practical Meal- planning option for people with diabetes. Clin. Diabetes 23(3):120-122. Crossref |
||||
|
Kelly KR, Haus JM, Solomon TP, Patrick-Melin AJ, Cook M, Rocco M, Barkoukis H, Kirwan JP (2011). A low-glycemic index diet and exercise intervention reduces TNFa in isolated mononuclear cells of older, obese adults. J. Nutr. 141:1089-1094. Crossref |
||||
|
Kulkarni KD (2005). Carbohydrate Counting: A Practical Meal-Planning Option for People With Diabetes. Clin. Diabetes 23(3):120-122. Crossref |
||||
| Martinez BA, Maldonado HJ, López AM (2011). Diagnostic methods of insulin resistance in a pediatric population. Bol. Med. Hosp. Infant Mex 68:397-404. | ||||
| Méndez CJE, Flores SJ, Noyola DE, Cruz ME, Calderón HJ, García AC (2007). Association index insulin resistance with cortisol levels by gender and anthropometric measures of school age Mexican children. Bioquimia 32:126-133. | ||||
|
Mullan AB, Ennis NC, Fee PJH, Young SI, Mc Cance RD (2004). Protective effects of ascorbic acid on arterial haemodynamics during acute hyperglycemia. Am. J. Physiol. Heart Circ. Physiol. 287(3):H1262-8. Crossref |
||||
| National Institute of Public Health México, Ministry of Health (2012). INSP- ENSANUT: National results, 2012. 1. Sistema Mexicano de Alimentos equivalentes. Fomento de Nutrición y Salud AC. 3rd ed. Mexico City | ||||
| Pérez Lizaur AB, Palacios González B, Castro Becerra AL (2008). Fomento de Nutrición y Salud AC. 3rd ed. Mexico City. Perrot AA, Clifton P, Brouns F (2006). Low-carbohydrate diets: nutritional and physiological aspects. Obes. Rev. 7(1):49-58. | ||||
| Poletti H, Barrios L (2007). Overweight, obesity, eating habits, physical activity and use of free time in school Corrientes (Argentina). Rev Cubana Pediatr. 79. | ||||
| Rodríguez R (2006). Childhood obesity and the effects of electronic media. Health Res. 8:95-98. | ||||
|
Rodríguez TI, Ballart FJ, Pastor CG, Jorda BE, Val AV (2008). Validation of a short questionnaire on frequency of dietary intake: reproducibility and validity. Nutr. Hosp. 23:242-252. Pubmed |
||||
|
Scavone G, Manto A, Pitocco D, Gagliardi L, Caputo S, Mancini L, Zaccardi F, Ghirlanda G (2010). Effect of carbohydrate counting and medical nutritional therapy on glycaemic control in Type 1 diabetic subjects: a pilot study. Diabetic Med. 27:477-479. Crossref |
||||
| "Secretaría de Salud, Guanajuato México (2010)." Nutritional Protocol for guidance on prevention and control of chronic diseases: overweight, cardiovascular risk and diabetes (in Spanish). | ||||
| Tomoyuki K (2007). The importance of carbohydrate counting in the treatment of children with Diabetes. Pediatr. Diabetes 8(6):57-62. | ||||
| Trejo OPM, Jasso CS, Mollinedo MFE, Balderas LG (2012). Relation between the physical activity and obesity in schoolchildren. Rev. Cubana Med. Gen. Integr. 28:34-41. | ||||
| Yeste D, Carrascosa A (2011). Metabolic complications of childhood obesity. Ann. Pediatr. 75:135. | ||||
|
Zipp C, Roehr TJ, Weiss BL, Filipetto F (2011). Impact of intensive nutritional education with carbohydrate counting on diabetes control in type 2 diabetic patients. Patient Prefer. Adherence 5:7-12. Pubmed |
||||
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


