Full Length Research Paper

ABSTRACT
In the fast changing scenario of the world, youths especially students of the youthful age are considered to be future assets of the family and the nation at large. These youngsters can contribute a lot for the welfare and the advancement of the family or nation in a truly global sense only if their energies and potentialities are channelized in the most appropriate and desired manner. On the contrary, if they indulge in undesirable activities like drug abuse and alcoholism, which have become the most prevalent social evil in the present times, they can never utilize their potential and energies for self growth, family welfare as well as welfare and development of the nation. The prevalence of an alarming growth rate of drug abuse and alcoholism warrants us to take preventive steps for proper utilization of human resources. Alcoholism has a higher prevalence among men, though in recent decades, the proportion of female alcoholics has increased. Current evidence indicates that in both men and women, alcoholism is 50–60 percent genetically determined, leaving 40–50 percent for environmental influences. Most alcoholics develop alcoholism during adolescence or young adulthood. The various health problems associated with long-term alcohol consumption are generally perceived as detrimental to society, for example, money due to lost labour-hours, medical costs, and secondary treatment costs. Alcohol use is a major contributing factor for head injuries, motor vehicle accidents, violence, and assaults. Beyond money, there are also significant social costs to both the alcoholic and their family and friends. For instance, alcohol consumption by a pregnant woman can lead to foetal alcohol syndrome, incurable and damaging condition.
Key words: Drug abusers, alcoholism, Haldwani, Uttarakhand.
INTRODUCTION
A complex mixture of genetic and environmental factors influences the risk of the development of alcoholism. Genes which influence the metabolism of alcohol also influence the risk of alcoholism, and may be indicated by a family history of alcoholism. One paper has found that alcohol use at an early age may influence the expression of genes which increase the risk of alcohol dependence. Individuals who have a genetic disposition to alcoholism begin drinking at an earlier age than average. Also, a younger age of onset of drinking is associated with an increased risk of the development of alcoholism, and about 40 percent of alcoholics will drink excessively by their late adolescence.
Severe childhood trauma is also associated with a general increase in the risk of drug dependency. Lack of peer and family support is associated with an increased risk of alcoholism developing. Genetics and adolescence are associated with an increased sensitivity to the neurotoxin effects of chronic alcohol abuse. Cortical degeneration due to the neurotoxin effects increases impulsive behaviour, which may contribute to the development, persistence and severity of alcohol use disorders.
There is evidence that with abstinence, there is a reversal of at least some of the alcohol induced central nervous system damage .A lot of research has been conducted by socialist like Donal Howard; he determined drinking behaviour by interactions of psychological and cultural variables and primary function of alcohol to reduce anxiety and Richard et al. established a relationship between alcoholism and peaks of “anomie”. Not much has been done in the field of alcoholism and the factors leading to this act.
A lot of people due to family pressure, cultural issues, isolation, stress, anxiety indulge in taking alcohol to suppress their feelings.. This is usually encountered in upper class, upper – middle as a status symbol or a stress buster. Thus, the spread and entrenchment of drug abuse and alcoholism need to be prevented, as the cost to the people, environment and economy will be colossal. The unseemly spectacle of unkempt drug abusers dotting lanes and by lanes, cinema halls and other public places should be enough to goad the authorities to act fast to remove the scourge of this social evil. Moreover, the spread of such reprehensible habits among the relatively young segment of society ought to be arrested at all cost. There is a need for the government enforcement agencies, the non-governmental philanthropic agencies, and others to collaborate and supplement each other's efforts for a solution to the problem of drug abuse and alcoholism through education and legal actions.
The present study thus focuses on the magnitude of the problem, causes leading to alcoholism and various rehabilitation techniques undertaken by the NGOs in Haldwani, Uttarakhand.
Peter Perk pointed out that “Drug phenomenon “like any other phenomenon cannot be explained or understood outside social and cultural contexts. Every issue about drugs beginning with the question, ‘what is drug’ is interpreted and mediated by social and cultural factors. Even different culture attaches widely divergent and sometimes contradictory meanings to a given drug and expect different experience and behaviour from it. The word drug has a variety of meaning depending upon the surrounding circumstances. Weissman has observed that” Drug is any substance (other than food) which by its chemical nature affects the structure or functioning of living organism.” But the most widely adopted definition of drug is suggested by World Health Organisation –“ Drug is a substance that when taken in the living organism may modify one or more of its functions”.[1]
Drugs have been used since time immemorial, mainly to get relief from the stress and strain of life and for ritual purposes. Historical evidence suggests that people have been using cannabis for 8000 years. It was used by many early civilizations as medicines for anxiety to digestive problems. Six hundred years ago ancient Sumerian texts considered poppy plant from where opium is produced, a "Joy Plant". There it is mentioned in the ancient books as the old Hindu medicine for chronic alcoholism and even delirium tremens. The Aryan invaders of India used beverage called Samaras.[2]
The Aryans knew the narcotic and euphoric properties of the cannabis plant thousands of years ago and there is little doubt that they made use of these substances. Buddhism in India contributed much to the habit of sobriety among the masses. Since 2500 years the natives of South America chewed coca leaves to derive pleasure and relaxation. Allauddin Khilji, who imposed total prohibition and Aurangzeb who practiced abstinence, were the exceptions in their times. It is to be pointed out that for the whole of the pre-British period the masses in general remained free from the effects of drinks and drugs. The British administration attempted to derive regular revenue from the sale of drinks and drugs. The Government in the year 1790 enacted excise laws for taxation purposes and excise departments were established in all the provinces. Their policy was maximum revenue with the minimum consumption. The first enquiry about drug addiction of opium and cannabis was made a hundred years ago when the Government of India appointed two Commissions in 1893, and 1895.
According to the Narcotic Control Bureau figures, the annual heroin seizures in the country are about one ton. Alcohol and drug dependence is a serious disease that affects the health and well of millions of Indians, treatment to a broad range of services, including identification, intervention, assessment, diagnosis, counseling, medical services, psychiatric services, psychological services, social services, and follow-up, for persons with alcohol and drug dependence. The components of treatment include management of withdrawal, long-term management of alcohol and drug dependence, and prevention of relapse. A number of alternative treatments are available for alcohol and drug dependence ranging from pharmacologic therapy to counseling, marital therapy and family therapy.
Frequently two or more treatment modalities are combined in one therapeutic approach.[3]
Alcoholism has a higher prevalence among men, though in recent decades, the proportion of female alcoholics has increased. Current evidence indicates that in both men and women, alcoholism is 50–60 percent genetically determined, leaving 40–50 percent for environmental influences. Most alcoholics develop alcoholism during adolescence or young adulthood.
The various health problems associated with long-term alcohol consumption are generally perceived as detrimental to society, for example, money due to lost labour-hours, medical costs, and secondary treatment costs. Alcohol use is a major contributing factor for head injuries, motor vehicle accidents, violence, and assaults. Beyond money, there are also significant social costs to both the alcoholic and their family and friends. For instance, alcohol consumption by a pregnant woman can lead to foetal alcohol syndrome, incurable and damaging condition. A lot of people due to family pressure, cultural issues, isolation, stress, anxiety indulge in alcohol to suppress their feelings.[4] This is usually encountered in upper class, upper – middle as a status symbol or a stress buster. Thus,the spread and entrenchment of drug abuse and alcoholism needs to be prevented, as the cost to the people, environment and economy will be colossal. The unseemly spectacle of unkempt drug abusers dotting lanes and by lanes, cinema halls and other public places should be enough to goad the authorities to act fast to remove the scourge of this social evil. Moreover, the spread of such reprehensible habits among the relatively young segment of society ought to be arrested at all cost. There is a need for the government enforcement agencies, the non-governmental philanthropic agencies, and others to collaborate and supplement each other's efforts for a solution to the problem of drug abuse and alcoholism through education and legal actions.
Stages for treatment
Drawing on the various approaches which have been attempted to treat addicts, we can divide them into three major stages, namely intervention, rehabilitation, and maintenance. The stages incorporate the commonly used activities, and phases that have been identified by various researchers and practitioners all over the world. James Proschaska and his team from the University of Rhode Island have come up with an excellent model to explain how people change, because addiction treatment is basically a process of change.
The first stage is pre contemplation. This is the denial stage, which we described earlier, where other peopleexcept the addict realizes that something is wrong. Here the emphasis is on that though the addict is not accepting change, he is somehow on the path to change.
The second stage is called Contemplation stage. At this stage the addict realizes that something is going wrong, but he is not sure what is to be done about it.
The third is Preparation stage. At this stage the alcoholic takes concrete steps towards change.
The fourth stage is called the Action phase. At this stage the person puts his heart into change and makes personal commitment.
The fifth stage is known as the Maintenance phase, which is the crucial one. In the treatment of addiction, change is not something that happens once, but something that is ongoing.
The sixth and the final stage is the termination phase, the compulsion to use Lessens. This description emphasizes the fact that addiction is a process that is ongoing.[5]
An addict has to continue to recover .All the sick people in the world would long for recovery. The addict also longs for recovery, but he will not go for treatment, because he believes that other people caused his illness and they need treatment. To get a person off the drugs we need to motivate him for treatment. The first step in motivating the addict is called intervention.
The first step in intervention is the identification, by the person seeking treatment or another individual (whether a family member, supervisor, or law enforcement or medical professional), of the existence of a problem with alcohol or drug. Dependence is followed by a referral for treatment. Intervention with chemically dependent individuals is an important step in the direction of treating one of the most widespread diseases in our culture. Knowledgeable and caring persons around the abuser, who come together with an interventionist who will motivate the group and show them how to present their accumulated data to the alcoholic in a compassionate way, also know this as Confrontation. It is a process by which the harmful progressive and destructive effects of chemical dependency are interrupted and the chemically dependent person is helped to stop using mood-altering chemicals and to develop healthier ways of coping with his or her needs and problems.[6]
It implies that the person need not be an emotional or physical wreck, before such help can be given. The goal of the intervention is to break down those defenses so that reality can shine through long enough for the person to accept it. It is a way of presenting reality to a person out of touch with it in a receivable way. By 'presenting reality', we mean presenting specific facts about the person's behavior and the things that have happened because of it. 'A receivable way': is one that the person cannot resist because it is objective, unequivocal, nonjudgmental and caring. An intervention is a confrontation, but it differs in some very important respects from the sort of confrontations with which most people are familiar and which have little or no positive effects.
DETOXIFICATION: The first stage of treatment offered is called detoxification. It is the management of acute alcohol or drug intoxication and withdrawal while in either independent living or in a sheltered living environment. This is the medical process of taking the affected person safely through the predictable sequence of symptoms that occur when blood alcohol/other chemical level drop during withdrawal. Alcohol withdrawal symptom ranges from the trivial to the markedly unpleasant and life threatening reactions like the delirium tremens or withdraw fits. A patient suffering from the dependence syndrome may therefore require immediate specialized medical assistance in corning out of alcohol. A variety of drugs may be used to provide treatment for withdrawal, and especially skilled nursing care is needed for the delirious and agitated patient. Modem methods of care are very successful in treating this acute phase of the problem and risks to life have been much reduced. The development detoxification centers over the last few years has shown that alcohol dependents can be safely and effectively helped to overcome withdrawal symptoms. Detoxification can usually be achieved in a non-medical setting provided medical service is readily available when necessary.
REHABILITATION
This stage of treatment consists of 3 components:-
(i) Evaluation and assessments,
(ii) Primary care,
(iii) Extended care.
Evaluation and assessment: The development of an individualized treatment strategy aims at eliminating or reducing alcohol or drug consumption by a thorough assessment of person's physical, psychological and social status and the environmental forces that contribute to the drinking behavior. Evaluation and assessment is done by screening the easily and inexpensively administered procedures in an attempt to establish the presence/absence or degree of severity of a condition. It is undertaken for many physical and psychiatric disorders.
Diagnosis is the conformation of the nature and circumstances of a condition. It has been that alcohol and drugs usually are accompanied by recommendations for intervention and treatment. Screening is an important preliminary step in the diagnosis of alcohol use disorder. It is needed to ensure the early identification of individuals who have begun to develop or are at risk of developing alcohol use problems. Screening tests serve to direct these individuals towards mere assessment, which may include a medicals and psychiatric history, physical and psychiatric examinations. Screening methods include questionnaires and interviews for assessing psychosocial indicators of alcohol problems and laboratory tests and other biological measures for detecting biochemical markers of excessive drinking.
Screening questionnaires are often self- administered. Screening instruments typically do not provide information that is useful in selecting treatment programs and specifying treatment goals, whereas the more complex questionnaire and interviews collect richer information and permit more detailed evaluation of patient with regard to treatment planning. Many traditional screening questionnaires ask questions in 'ever' terms to determine the presence or absence of symptoms. Other screening instruments require subjects to indicate present-state habits, behaviors, and feelings. Each type has advantages and limitations.
The CAGE questionnaire is a simple method and can be easily administered. It uses a four-item instrument to detect the symptoms or problem. They are:
1. "Have you ever felt you should cut down on your drinking?”
2. "Have people annoyed you by criticizing your drinking?"
3. "Have you ever felt bad or guilty about your drinking?"
4. "Have you ever had a drink first thing in the morning to steady your nerves or get rid of a hangover (eye opener)?"
One "yes" response raises suspicions of an alcohol use problem, and more than one is a strong indication that a problem exists. CAGE takes only 30 s to administer. When included as part of a routine health screening it may detect alcohol use problems that might be missed otherwise. Primary care: It is the application of therapeutic activities to help the individual reduce alcohol or drug consumption and attain a higher level of physical, psychological and social functioning while in either independent living or in a sheltered living environment. Extended care (stabilization ): It is the consolidation of gains achieved in primary care through continued participation in treatment and supportive activities while in either independent living or in a motivational supportive, sheltered living environment. [7]
MAINTANCE
This stage consists of 3 components:-
(i) Aftercare,
(ii) Relapse prevention,
(iii) Domiciliary me.
Aftercare: It is the continued provision of some therapeutic input to maintain the gains in functioning achieved through intensive intervention and stabilization while in either independent living or in a transitional or long-term supportive, sheltered living environment
Relapse prevention: It is the continued provision .of therapeutic activities to avoid treatment alcohol and the return to prior patterns of drinking; it also involves maintaining the gains in functioning Drug Dependence achieved through brief intervention or intensive intervention and stabilization. This is done either while living independently or in a transitional or long-term supportive, sheltered environment. Relapse prevention believes that patients with the more severe type of drinking and drug abuse should be offered continuing contact with a helping agency, at least for the first year or two after commencing treatment. [8]
In recent years, relapse prevention strategies have been widely publicized, and training has been offered to practitioners. The addition of relapse prevention procedures to a treatment program is intended to reduce the probability and rapidity of relapse, although the techniques can be used for primary rehabilitation as well as relapse. The self-efficacy approach, a behavioral treatment strategy derived from Bendura's social learning theory of self-efficacy, behavioral self-control training and cue therapy are described below as examples of these techniques. The key assumption underlying this strategy is that drinking Prevention and Treatment of Alcohol and Drugs or drug abuse alone does not lead to a return to chronic excessive drinking or drug dependence.
Domiciliary care: It is the provision-protected and ongoing supportive, protected living environment for those who are disabled by prior alcohol/drug use to return to independent community living. This situation is warranted for those who are physically unable to lead community life due to illness or other disabilities.
TREATMENT MODALITIES
The content of treatment is usually referred to as the technique, method, procedure, or modality. The specific activities that are used to relieve symptoms or to induce behavior change are referred to as modalities. Many treatment modalities have been used to address alcohol and drug dependence problems, alone or in combination with, psychotherapy, self help groups, aversive counter conditioning, Alcohol and Drugs anti-anxiety medication, self-control training, stress management, massage therapy, physical exercise, vocational counseling, marital and family therapy, hypnosis, education about the effects of alcohol, milieu management, and social skills training,[9]
Six general categories
(1) Pharmacological,
(2) Social,
(3) Psychological,
(4) Behavioral,
(5) Psychodynamics, and
(6)Spiritual
Pharmacological treatment modalities
There have been a number of attempts to classify the different drugs used in the treatment of alcohol and drug dependence. The major distinctions have been in terms of (a) drugs used to counter or antagonize the acute effects of alcohol and drug intoxication, (b) drugs used in the management of withdrawal, and (c) drugs used in long-term treatment (rehabilitation and relapse prevention).
Social treatment modalities
Alcohol and drug dependence is also a social disease. Treatment components such as marital and family therapy, women's groups, alcoholic anonymous, employee and assistance programmes are used in the treatment of chemical dependency.
i) Marital and Family Therapy: Many therapists now require the participation of the patient's spouse and sometimes other family members as an essential ingredient of recovery. The spouse of the problem drinker or drug abuser often needs an opportunity to discuss the stresses that the family has experienced and to obtain information about the nature of the alcohol and drug dependence. Some therapists have endeavored to move away from a patient centered approach to alcohol problems and have come to regard the abuse as one facet of a disturbed family system. In consequence they focus attention on this system itself. Whichever approach is adopted, it is clear that the family will have to undergo significant readjustments as the problem drinker and, drug abuser finds a new style of life. There is good evidence that a spouse, who is supportive but does not collide with the drinker's or drug abuser's evasion or minimize the seriousness of the drinking problems, makes a major contribution to a favorable treatment outcome.
ii) Women's Groups: As increasing number of women develop alcohol-related problems, it has become evident that programmes must accommodate to their specific needs. Worsen commonly feel more guilty and stigmatized about having a drinking or drug abuse problem and some way find it easier to speak freely if they can have part of their treatment within a service for women only. In such a setting they find it easier to talk openly about their difficulties and particularly to discuss some of the sexual abuses many women alcoholics have experienced. In facilitating access to treatment for women, additional services such as neighborhood based clinics and the provision of crèches are important considerations.
iii) Alcoholics Anonymous, AI-Anon, and AI-Ateen: Alcoholics Anonymous celebrated its fiftieth anniversary in 1985 and claims worldwide to have helped more than a million members. It is unwise for anyone who is significantly Treatment of AICO~OI and Alcohol dependent not to have at least looked very closely at AA. This is Drug Dependence, often best achieved through initial personal introduction to a member of AA with whom the problem drinker can identify. It is too much to expect the drinker just to go to a meeting. It usually requires fifteen to twenty meeting at more than one group before any sensible opinion can be made about its value for an individual. Many people have found in AA exactly the help and understanding they require. Others may take something from AA's philosophy, but not become regular attendees. AI-Anon, an organization for relatives and friends of alcoholics, deserves similar recognition as an extremely valuable resource. It is well worth exploring by anyone closely involved with a problem drinker, as it teaches the relative or friend to find support even when the drinking partner is unwilling to recognize or deal with the problem. Al Ateen has evolved specially for the teenage children of alcoholics. Alcoholics Anonymous provides a fellowship which encourages frankness about alcohol problems in a group surrounded by others who can readily identifier with the drinker's suffering and shame and at the same time offer support in finding a new way of life.
iv) Employees’ Assistance Programme: Alcohol and drug dependence frequently manifest as impaired work performance. This fact can be turned to therapeutic advantage by the creation of 'Employee Assistance Programmes whereby a company establishes a policy for dealing with employees whose work performance is impaired by alcohol misuse or other factors. The policy needs to be developed in joint consultation between union and management and applied equally to all levels within the organization. If alcohol or drug dependence appears to be affecting an employee's work performance then he or she can choose to accept referral to an appropriate source of help with guaranteed continued employment provided they cooperate with treatment. v) Narcotic Farms: It was a method employed by the US government in the early part of the last century. The basic idea was to provide medical model of treatment in a farm setting. The clients stayed back in the farm engaging themselves as workers for a period of time as the social workers and the doctors did the follow up on them.
vi) Herapiutic Communities: Charles Dederich in the USA developed the method after the Second World War: "Modern therapeutic communities immerse patients in a comprehensive 18-24 month treatment regimen built around the philosophy that the addict's primary problem is not the drug he abuses, but himself'. In this approach, the primary therapist is the community itself. Drug abuse is a symptom of deeper personal disturbances and Treatment [10]
Psychological treatment modalities
There are a wide variety of psychological treatments, both behavioral and psychodynamic that have been used in the treatment of alcohol and drug abuse problems. Sometimes it is difficult to determine whether a specific approach is primarily behavior or psychodynamic. Group therapy and marital and family therapy, for example, cannot truly be classified as either psychodynamic or behavioral because practitioners from each orientation use them. In fact, the current practice is to combine different modalities and orientations to fashion multi-model treatment approaches. There are, however, certain specific modalities that, for descriptive purposes are identified with one or the other model because of the rationale for their use and effect.
Behavioral treatment modalities
The first clinical use of techniques derived from learning theory to reduce alcohol consumption was by the Soviet physician Kantorovich more than fifty years ago. Kantorovich used electrical aversion, but the method was shown to be ineffective, and its use as a clinical procedure discontinued. The major continuing use of behavioral methods over the intervening years was 'chemical aversion', a technique initiated at the Shade1 Sanatorium in Seattle, USA. The more widespread application of behavioral methods to a range of psychopathological disorders began in the early 1960's. These initial efforts reflected a comparatively simple view of the etiology of problem drinking as an attempt to reduce conditioned anxiety. The first, uni-dimensional learning theories about the causes of excessive drinking were primarily derived from animal laboratory studies and clinical observations that alcohol eased high levels of anxiety in persons under treatment for alcohol problems.
However, behavioral research with humans challenged the view that conditioned anxiety was the sole cause of excessive drinking, and suggested that cognitive elements must also be considered.
1. Chemical Aversion remains the best-known behavioral treatment procedure that focuses on drinking behavior. In chemical aversion as currently practiced, a noxious stimulus is paired with a drink of the person's favorite alcoholic beverage. Vomiting is induced to condition the individual to react adversely to the sight, smell or taste of alcohol. Five aversion treatments are generally administered on alternate days during a 10 to 15 day hospitalization. Some persons develop adequate aversion in fewer than five treatments; others require additional treatments. Because aversion is not generalized to all alcoholic beverages, the individual receives a number of different beverages at some time during the treatment.
2. Covert Sensitization is a verbal aversion therapy that uses the person's imagination to pair unpleasant, often nausea provoking events with the anticipated acts involved in drinking. The person visualizes the drinking sequence - ordering of a drink, touching the glass to the lips, and drinking itself- all in his or her usual drinking environments. [11]
3. Stress Management Training has also been found to help persons with alcohol problems in staying sober, particularly when anxiety) is a significant Drug Dependence concomitant problem. Bio-feedback is one such technique. It uses an electronic apparatus to monitor physiological responses and to display them to the individual through visual or auditory feedback. The individual is trained to produce the feedback by practicing the desired response (usually the relaxation of muscle groups or meditation). The person learns to recognize the subjective states that indicate heightened muscle tension as measured in electromyography (EMG) bio-feedback or alpha waves as measured by the electroencephalograph (EEG). Contingency Management is another behavioral technique. It attempts to formalize through contracts the naturally occurring contingencies both positive and negative, reinforcing and punishing that result from excessive drinking or drug abuse. The keys to developing effective contingency management are to: (a) idem through assessment, consequences that are meaningful to the persons; (b) develop mutual agreement about the contingency; and (c) carefully and consistently carry out the contingency with all parties to the agreement performing their designated roles.
4. Community Reinforcement Counseling is a contingency management approach that is designed to provide focused behavioral training to person with chronic alcohol and drug dependence. The goal of the counseling is to improve long-standing vocational interpersonal and familial problems.
5. Harm Reduction is a set of interventions that concentrates not on ending drug dependence but on controlling the harm that drug dependence does to the society at large. First introduced in the Netherlands in the 1980's, harm reduction policies attempt to integrate drug abusers into the larger society had to distinguish between use and abuse .Harm reduction began when it was first discovered that HIV was often transmitted through the sharing of needles for drug injections. A needle exchange programme whereby heroin addicts trade in their contaminated needles for clean ones was introduced as part of the harm reduction programmes. Harm reduction advocates also want to reduce the criminal activity that results from drug abuse.[12]
Psychodynamic treatment modalities
A simple yet helpful definition of psychotherapy is that it is "an interpersonal process designed to bring about modifications of feelings, attitudes, and behaviors which have proven trouble to the person seeking help from a trained professional". Contemporary psychotherapy is characterized by a variety of theoretical orientations. Very often the psychotherapy offered to a person with alcohol or drug abuse problems reflects the orientation and training of the therapists; there have been no real comparisons of the effectiveness of the different theoretical varieties of psychotherapy in treating persons with alcohol or drug abuse problems. What has emerged, however, is a set of principles or techniques that are recommended for use with persons experiencing alcohol or drug dependence. As with the other modalities described current practice is to include psychotherapy as a component in a multimodality approach. Duration has ranged from short-term to long-term. There does not appear to be substantial evidence, supporting the greater effectiveness of longer periods of time in the few studies that have considered this variable. The various formats are discussed in the paragraphs as follows:-
1. Individual Psychotherapy: In recent years 'individual psychotherapy' has not been seen as a major contributor to the treatment of persons with alcohol and drug dependence. The lack of support for use of this approach comes from a history of failure in the use of psychoanalytically oriented methods, which viewed alcohol and drug dependence as symptom of underlying pathology and sought to resolve the underlying conflict through the use of interpretations and development of insight. There are those, however, who feel that individual psychotherapy or counseling continues to play an important role in the treatment of alcohol and drug dependence. Individual psychotherapy generally is recommended only as part of a more comprehensive rehabilitation effort that can include alcohol and drug education, referral to Alcoholics Anonymous, family intervention with reference to AI-Anon and AI-Ateen, the prescription of disulfirarn, and specific efforts to remove life problems that contribute to continued drug abuse and problem drinking.
2. Group Psychotherapy: Unlike individual psychotherapy, group psychotherapy is among the most commonly used psychotherapeutic techniques for the treatment of alcohol and drug dependence. Group therapy is used in most primary and extended rehabilitation programmes. Group therapy as a distinct singular treatment is rare. As with individual psychotherapy, group therapy is offered in concert with alcohol and drug education, referral to Alcoholics Anonymous, and additional supportive activities. When group therapy is used an extended care of aftercare modality, the group may meet as frequently as three times a week and as infrequently as once a month.[13]
3. Group Dynamics: In addition to group psychotherapy, organized programs often use the principles of group dynamics in conducting other components for the overall treatment programmes. These components may include educational groups .Educational groups vary in size and style. The most common format is large group presentation of material through lectures, films and videotapes, followed by a discussion period in which the goal is both to clarify and amplify the factual material and to correct misconceptions and emotional dons.
4. Activity Groups are another type of group psycho-therapy organized around a specific recreational event and used widely in organized programs. The objectives of 'activity group participation are to relearn social skills by interacting with other people in sober contexts, to learn and practice alternative recreational activities that will eventually replace drinking, and to become familiar with community resources. Many organized programmes also use community meetings or ward management meetings as group therapy vehicles.
Spiritual treatment modalities
Alcohol and drug dependence is also a spiritual disease. The person addicted to alcohol and drugs gives primary importance to drinking and using drugs. A sense of the higher power is necessary to fight against the compulsion to drink and use the drugs. Prayer and meditation is universally accepted as one of the methods of recovery of alcohol and drug dependence. In meditation, the individual leans to concentrate on a thought, a sensation, a word, an object, or some mental state. Some techniques are very active and require that the person make a strenuous effort to focus on a specific thing. Certain yoga techniques, for example, require that the practitioner maintains specific postures and deliberately controls his or her breathing or other bodily functions. Other meditation techniques, such as transcendental meditation, are passive approaches.[14]
Drinking is considered part of culture in some communities. As per the statistics Native Americans and Irish Americans have the highest rates of alcoholism in the United States. In the United States, for instance, alcohol related statistics show that approximately 15 percent of the population experiences some sort of problem that is associated with their consumption of alcohol. Regarding these individuals, alcoholism affects roughly 4% of the overall population, or 12.5 million men and women. In India, an estimated 7.5 crore Indians are drug addicts and the amount is working over importantly, opening to semi-urban and backward areas, according to formal numbers. Reported to the National Survey on Extent, Pattern and Trends of Drug misuse in India conducted by the Focus in collaboration with UN Office on Drugs and Criminal Offence, the actual preponderance values inside the age group of 12-18 age was Alcoholic Drink ( preceding21), Cannabis (3), Opiates (0.7) and other illicit drugs (3.6 per cent) . (20). In India Nagaland is reported to have the highest rate of drug abuse followed by Punjab. According to the report, which is based on studies conducted by government agencies including NACO and NGOs in 2009, out of 35,000 to 40,000 drug users, 18,000 to 20,000 are injecting drug users and exchange of needles among them is one of the major routes of HIV/AIDS transmission. According to the report of Drug demand reduction - UNDCP Regional office for South Asia – New Delhi, 2000 one of the commonly abused substance among the youth was alcohol (4 - 13 %). [15]
Few theories related to drug habit are explained in Social- cultural approach. It talks about drug habit being part of social behaviour. It is explained under two schools of thought- (a) social structure orientation, (b) naturalistic orientation .The former attempts to formulate a general theory of deviance, of which drug habit is viewed only as type. Various theories related to this are explained by Sellin(1938) and Merton(1964).(16) On the other hand naturalistic orientation also views deviance in terms of sociological factors but it does so from the point of view of the individual. Apart from this there are Biological theories which include Genetic factor and Metabolic Imbalance. Psychological theories underplay personality factors and personality theory as we might expect.[i]
[1]Chopra R.N. & Chopra .c. (1965), “Drug Addiction with Special Reference to
India, Council of Scientific and Industrial Research, New Delhi.
[2]Eaves. Derek , Swinson.R.P,1978- “Alcoholism and Addiction.” Macdonald and Evans Publications.
[3]Graymore ,Clive. 1987. “Alcoholism insight into the addictive mind “.David and Charles publications
[4]Reid. Sue. Titus. 2006,Crime and Criminology .Mcgraw hill publications
[5] Miller WR, Zweben A, DiClemente CC, Rychtarik RC. “Motivational Enhancement Therapy manual: A clinical research guide for therapists treating individuals with alcohol abuse and dependence. “Vol. Project MATCH Monograph Series, Vol. 2. Rockville, Maryland: National Institute on Alcohol Abuse and Alcoholism; 1992
[6]Vernon E. Johnson, D.(1 986), “Intervention”. Johnson Institute Books,Minneapolis
[7] Miller WR, Zweben A, DiClemente CC, Rychtarik RC. “Motivational Enhancement Therapy manual: A clinical research guide for therapists treating individuals with alcohol abuse and dependence. “Vol. Project MATCH Monograph Series, Vol. 2. Rockville, Maryland: National Institute on Alcohol Abuse and Alcoholism; 1992
[8] Miller WR, Zweben A, DiClemente CC, Rychtarik RC. “Motivational Enhancement Therapy manual: A clinical research guide for therapists treating individuals with alcohol abuse and dependence. “Vol. Project MATCH Monograph Series, Vol. 2. Rockville, Maryland: National Institute on Alcohol Abuse and Alcoholism; 1992
[9] Miller WR, Zweben A, DiClemente CC, Rychtarik RC. “Motivational Enhancement Therapy manual: A clinical research guide for therapists treating individuals with alcohol abuse and dependence”. Vol. Project MATCH Monograph Series, Vol. 2. Rockville, Maryland: National Institute on Alcohol Abuse and Alcoholism; 1992
[10] Miller WR, Zweben A, DiClemente CC, Rychtarik RC. “Motivational Enhancement Therapy manual: A clinical research guide for therapists treating individuals with alcohol abuse and dependence. “Vol. Project MATCH Monograph Series, Vol. 2. Rockville, Maryland: National Institute on Alcohol Abuse and Alcoholism; 1992
[11] Miller WR, Zweben A, DiClemente CC, Rychtarik RC. “Motivational Enhancement Therapy manual: A clinical research guide for therapists treating individuals with alcohol abuse and dependence. “Vol. Project MATCH Monograph Series, Vol. 2. Rockville, Maryland: National Institute on Alcohol Abuse and Alcoholism; 1992
[12]Miller WR, Zweben A, DiClemente CC, Rychtarik RC. “Motivational Enhancement Therapy manual: A clinical research guide for therapists treating individuals with alcohol abuse and dependence. “Vol. Project MATCH Monograph Series, Vol. 2. Rockville, Maryland: National Institute on Alcohol Abuse and Alcoholism; 1992
[13]Rathus.A. Spencer, Psychology- in the new millennium .Earl Mcpeek publications
[14]Paul.c.Madan.1996.Drugs , Youth and Society .Madhu Deep publications
[15]Miller WR, Zweben A, DiClemente CC, Rychtarik RC. Motivational Enhancement Therapy manual: A clinical research guide for therapists treating individuals with alcohol abuse and dependence. Vol. Project MATCH Monograph Series, Vol. 2. Rockville, Maryland: National Institute on Alcohol Abuse and Alcoholism; 1992.
RESEARCH METHODOLOGY
Exploratory Research Design has been used for the current study. The researcher has chosen this design for the only purpose of exploring the area that needs a fresh approach. Even though research has been conducted in the field of drug abuse and alcoholism, the area related to role played by NGO officials and family of the alcoholics needs to be researched in Uttarakhand. Due to various physical, social and sociological factors, one is forced to take alcohol. The main focus of this study is to examine the role of family leading to alcoholism. Nevertheless, studies related to male alcoholics, causes leading to alcoholism has been carried out by many scholars, but the area regarding family especially as a whole is not been touched upon. The study includes relevant literature from books, Records, Consultation with experts from de-addiction centers, academicians and case explorations. The objective of the research is to explore the main causes of alcoholism. The research problem is described. The purpose behind the study partially is to evolve strategies or solution to the problem.
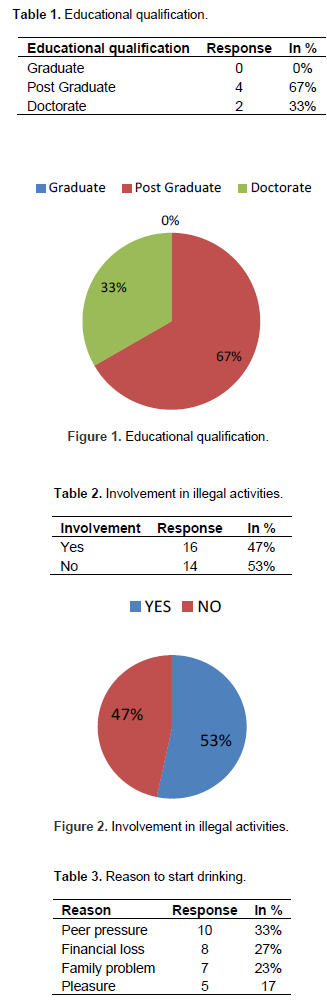
The counselors were generally post graduates out of which two were doctorate holders (Table 1 and Figure 1).
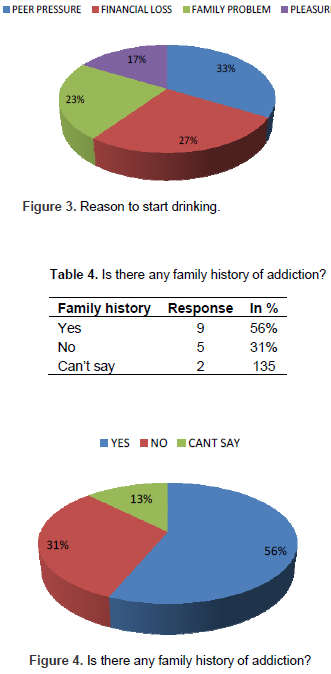
53% of the addicts were involved in illegal activities rest 47% were not (Table 2 and Figure 2). 33% said that peer pressure was the reason to indulge in drinking, 23% said family problem was the reason while 27% said financial loss (Table 3 and Figure 3). 56% of the addicts had family history related to alcohol, 31% did not have a family history whereas 13% were not aware (Table 4 and Figure 4).
FINDINGS AND SUGGESTIONS
The following findings were noted from the data provided:-
1. It is noted that even though the counsellors appointed by the NGO were quite qualified and were post graduates from psychology, medicine (Table 1), their knowledge in imparting rehabilitation therapies was limited. The therapies like Alcoholic Anonymous, Pharmacotherapy’s, Women’s group were unknown to them (Table 1).
2. According to the authorities maximum cases were from middle class which totally rejects the myth that the addicts belong to lower class.
3. It is observed that maximum number of addicts denied that they were involved in any illegal activity (Table 2) whereas the counsellors agreed that they were involved.
4. Maximum addicts were of 30-40 yrs (43%) followed by 20-30yrs (23%) who hailed from broken family and were not employed or rather forced to leave their job due to their habit of drinking and were indulged in this activity from adolescence. The basic reasons were Peer pressure, financial loss, pleasure and broken marriage (Table 3).
5. The maximum cases encountered were of alcohol followed by ganja .Generally the addicts were also in the habit of taking other drugs.
6. The most frequently used therapy was behavioural therapy (cognitive), yoga (spiritual therapy). Apart from the therapies used, recreational facilities like T.V, Games, Drawing competition were also conducted.
7. The addicts were allowed to meet their family after 15 days of their stay and then every Sunday.
8. The follow up of the cases was done by the NGO officials to ensure if any addict had indulged in the activity again after undergoing rehabilitation.
9. After interacting with the family members it was found that maximum addicts possessed family history of addiction (Table 4).
10. The families of maximum addicts were quite supportive and were involved in various family therapies and recreational activities.
11. The behaviour of the officials was quite sympathizing. They were supportive as told by the addicts. The rapport between the counsellors and the addict seemed quite strong.
12. It was quite surprising that maximum addicts were keen to indulge in the activity again , even after their rehabilitation.
SUGGESTIONS
Rehabilitation of the addicts needs a look by the government. In the name of rehabilitation, not much is being done. Few suggestions for the improvement of rehabilitation of the addicts are as follows -
1. Family counselling: Bard (1982) stresses that the combination of tolerance, stability and reassurance is essential. Therefore, “Rehabilitation starts from the home”. The support of the family is a must during rehabilitation. Positive approach is a quite necessary in handling of the addicts.
2. The NGOs should conduct seminars and impart awareness among people. This should be made compulsory for boys/girls from 14 years onwards.
3. Alcohol advertising: it should be restricted and TV advertising should be banned. International agreements should ensure that national public health policies in relation to advertising not undermined by the international media.
4. Treatment: All people who experience drinking problems should have the right to free access to treatment and support services in the community in which they live.
5. Work-place: All employees and trade union associations should develop alcohol policies to discourage alcohol impairment and consumption at work and safeguard the employment of those who seek help and their drinking problem.
6. Publicity campaign. Governments should subject alcohol to a campaign at least as vigorous and high profile and support education and training programmes for appropriate professional workers.
7. Tax increase: tax imposed on the alcohol should be increased; this might discourage the common man from wasting his hard earned money.
8. Promote non drinking by having a national non drinking week or day.
9. Rope in celebrities and other youth icons to discourage young generation from drinking.
10. The number of NGOs working in this field should be increased by the government as only three NGOs are developed in Uttarakhand who are currently working in this area.
11. Women to have candle light marches or similar campaigns to stop men from drinking highlighting the after effects it has on their families.
12. Liquor shops to pay heavy fines in case they sell alcohol to underage children.
13. Parents should be made knowledgeable about drinking hazards and how it can affect their children; this can be done with the help of school and college authorities by conducting seminars and meetings.
CONCLUSION
The present study was aimed at exploring the role of NGOs for the rehabilitation of addicts in Haldwani, Uttarakhand. The study has, to a basic extent, tried to understand the various steps and techniques involved in the rehabilitation of the addicts.
This problem emerges primarily from peer pressure, financial loss and family problem. Certain rehabilitation techniques are not been enforced and number of rehabilitation centres specially dealing with addicts are quiet less in number; therefore the government itself should take certain measures in this field.
Here, a wider society has to take the blame. For one, no law or penalty can put an end to a man’s craving, which will only increase .It is hoped that this study has been able to highlight the various techniques adopted by the NGOs for the rehabilitation and for the behavioural study of the addicts, an issue which is very sensitive and yet needs to be understood and openly discussed further for the betterment of all.
CONFLICT OF INTERESTS
The author has not declared any conflict of interests.
REFERENCES
|
Ahmad A, Sen KA (1999). Drug Abuse and Youth –a psychological study. Gyan Publishing house. |
|
|
|
|
|
Chopra RN, Chopra C (1965). "Drug Addiction with Special Reference to India, Council of Scientific and Industrial Research, New Delhi. |
|
|
|
|
|
Eaves D, Swinson RP (1978). "Alcoholism and Addiction." Macdonald and Evans Publications |
|
|
|
|
|
Irwin GS, Barbara RS (1996). 8'h Edition: Abnormal Psychology, Prentice-Hall of India Ltd., New Delhi. |
|
|
|
|
|
Paul CM (1996). Drugs, Youth and Society .Madhu Deep publications,page.45 |
|
|
|
|
|
Rathus AS, Psychology- in the new millennium .Earl Mcpeek publications. |
|
|
|
|
|
Reid ST (2006). Crime and Criminology. Mcgraw Hill publications, p.213. |
|
|
|
|
|
Thakur D (2003). Research Methodology in social sciences. Deep and deep publications. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


