Full Length Research Paper

ABSTRACT
Deliberate efforts to halt human immunodeficiency virus infection (HIV) propagation and mitigate human immunodeficiency virus infection and acquired immune deficiency syndrome (HIV/AIDS) impact in resource-poor communities are critical elements of HIV/AIDS control and care. This study investigated the HIV/AIDS prevention programmes and mitigating measures (HIV/AIDS PPMM) among the Idoma-speaking people in Benue State, North Central Nigeria. From a purposive sample of 25 relatives of people living with HIV/AIDS (PLWHA), nine health workers and six community leaders selected from two HIV treatment centres and six nine communities in three Local Government Areas (LGAs) (that is, district level), data were collected through Integrated Disbursement and Information System (IDIS) and focus group discussions (FGDs), and analysed thematically to meet study objectives. Findings on community-initiated measures on HIV/AIDS control in Idoma land were presented under the following heading: sanctions on prostitution, training/credit facilities for affected persons (OVC), government and non-governmental (NGO) programmes such as free anti-retroviral drugs, counselling services and AIDS awareness campaigns. Some of the government and NGO sponsored initiatives to curtail HIV/AIDS situation had drawbacks – some campaign messages were themselves perceived to be stigmatising, while supply of drugs was erratic. It was concluded that inconsistencies of some of the HIV/AIDS interventions may worsen the HIV/AIDS situation in this socially and economically disadvantaged community. There is need for consistent treatment programmes, appropriate HIV/AIDS mass education and other social strategies using healing and destigmatising messages, drama and effective community sanctions. These should be appropriately designed and disseminated to reduce HIV/AIDS-related stigma and discrimination, while curbing HIV spread, and mitigating the consequences of the HIV/AIDS epidemic.
Key words: HIV/AIDS mitigating measures, HIV/AIDS prevention strategies, Idoma people, Benue state, Nigeria.
Abbreviation: HIV/AIDS PPMM, HIV/AIDS prevention programmes and mitigating measures.INTRODUCTION
The Society for Women against acquired immune deficiency syndrome (AIDS) in Nigeria (SWAAN, 1999) emphasized that people living with human immunodeficiency virus infection and acquired immune deficiency syndrome (HIV/AIDS) need love, support and care by all, and that legislative processes can be used to formalize such initiatives. According to UNAIDS/WHO (2004), successful national responses require a strong political will and leadership, societal openness and determination to fight against stigma, and strategic responses (such as the Behaviour Change Communication [BCC 2004 to 2008 strategy in Nigeria]) (SWAAN, 1999; Factsheet, 2011). Other responses suggested include a multi-sectoral and multilevel action against AIDS, community-based responses and social policy reform to address the factors that make the population more vulnerable to the infection (NACA, 2005; FMWA/UNICEF, 2007). Sustained responses with adequate resources are necessary (Gilk et al., 1998; Ehiri et al., 2005). Counselling centres and churches have provided the needed individual or group counselling to help people with HIV infection or AIDS share their feelings, problems, and coping mechanisms with others (SWAAN, 1999). Family counselling addressing the emotions of other family members disturbed by the diagnosis of HIV infection in another family member and grief counselling also helps people who have lost friends or family members to AIDS are also reported (UNAIDS, 2004).
In the United States, grassroots organizations sprang up to meet the various needs of people living with HIV/AIDS (PLWHA). The role of Los Angeles Shanti Group established in 1983 to provide emotional support and medical guidance to people with AIDS and other life-threatening illnesses is documented (ENCARTA, 2007). Other activist organizations such as the AIDS Coalition to Unleash Power (ACT UP), founded in 1986, focused on effecting changes in public policies and accelerating the course of AIDS clinical research. The American Foundation for AIDS Research (AMFAR), created in 1985, has a pivoted contribution in supporting AIDS research in addition to the advocacy for fair and compassionate AIDS-related public policies. In Canada, similar groups were formed for the civil rights of people infected with HIV.
Similarly, in Africa, communities have responded variously to the increasing and staggering HIV prevalence in the region. For example, Uganda brought its estimated prevalence rate down to around 8% from a peak of close to 14% in the early 1990s using strong
prevention campaigns (UNAIDS, 2004). Other active steps to fight HIV spread through action by the Government and other groups in society included religious leaders and community development organizations (Barnett and Whiteside, 2002). These contributed to a reduction in HIV infections among young pregnant women (UNAIDS, 1998). A large increase in condom use probably contributed to these lower rates of infection. This was accompanied by significant declines in teenage pregnancies. In Zambia, for instance, the government involved the health, educational, agricultural and industrial sectors as well as religious leaders and church groups in HIV prevention, resulting in an appreciable drop in HIV prevalence by almost half in six years. Studies of sexual behaviour in Zambia conducted in 1990, 1992, 1996 and 1998 suggested that falling HIV rates were due in part to a decrease in the prevalence of some types of risky sexual behaviour in urban areas (UNAIDS/WHO, 2011). An increasing number of young people had access to free condoms. This was in addition to sex-related behaviour changes due to educational sessions.
In Nigeria, documented functional support groups as HIV control programme were not common, until recently where voluntary community services are now being encouraged in affected communities to assist in giving care and support to those infected (Hilhorst et al., 2004). Even government-sponsored programmes reported to lacking or at best chaotically present. There have been reports and allegations in the media and in the political circles that governments at various levels and communities are reluctant in formulating and implementing policies on AIDS control programmes, what Oke (1999) calls “inactions” of relevant authorities.
Hilhorst et al. (2004) in their impact on HIV/AIDS in Benue State had identified some attempts by rural communities to tackle the effects of the epidemic. However, that study focused on proxy indicators of HIV/AIDS. In the effects of community-based care for PLWHA on their well-being in Benue State, Nigeria, Ilebani and Fabusoro (2011) had indicated the need for HIV/AIDS intervention programmes to be tailored towards appropriate information to provide a conducive environment to support the formation of support groups for PLWHA and to encourage PLWHA to seek knowledge on how to overcome stigmatization and discrimination. They opined that such programmes should be developed by the government, NGOs and other concerned agencies. In 2012, the World Health Organization in its document “HIV/AIDS Programme - Prevention and Treatment of HIV and other Sexually Transmitted Infections for Sex Workers in Low- and Middle-Income Countries: emphasized the need for community role in HIV/AIDS interventions using qualitative research “to better characterize and understand community empowerment” to ensure appropriate measurement instruments for community-level and individual-level empowerment-related outcomes. It added that such qualitative and descriptive studies should be conducted in diverse geographical locations, but that these are scanty in Asia and Africa.
This qualitative study is an attempt to fulfil such calling. The study focuses on PLWHA, their relatives (PABA), HIV/AIDS health workers, and community members in an attempt to evaluate their views on the HIV/AIDS control and mitigating measures (HIV/AIDS PPMM) among the Idoma-speaking communities of Benue State, Nigeria. Information about the community and government involvements is required from these sample population to examine the level of involvement of various community and government organizations in the prevention and management of HIV/AIDS in Idoma land.
METHODS AND MATERIALS
Study design
The qualitative study assessed community-based HIV/AIDS prevention programmes and mitigating measures (HIV/AIDS PPMM) among the Idoma-speaking people of Benue State. It is a part of larger study conducted in the area to determine the socio-economic consequences of the epidemic in the land.
Sample and sampling procedure
Site and community selection
This was conducted in Idoma land, a resource-scarce ethnic group reported to be one of the worst hit areas by the HIV/AIDS epidemic in Nigeria (FMOH, 2007). The area is predominantly rural and agrarian and consists of nine Local Government Areas. Three local Government Areas were selected using quota sampling, one from each of three dialectical clusters of Idoma (namely, Idoma West or IdomaEnone made up of Okpokwu and Ogbadibo LGAs, Idoma North or IdomaIcho consisting of Otukpo, Ohimini, and Agatu and the Agila-Igede cluster which include Ado, Obi , Oju, and Apa LGAs) (ICD, 2009). The three selected local governments areas were then stratified into rural and urban settlements (the urban being the local government headquarters while one of the other districts from each local government area represented the rural areas). The urban areas (that is, the local government headquarters) were included purposively based on the presence of HIV/AIDS care support groups, and treatment centres and activities at the headquarters. Most general hospitals, usually situated at the local government headquarters, have HIV/AIDS care and treatment facilities and HIV/AIDS support groups.
Sample selection
A purposive sample of 25 relatives of PLWHA (that is, people affected by AIDS (PABA)), nine health workers, six community/ group leaders identified as key informants, and 18 willing PLWHA from two HIV/AIDs treatment centres and six communities were also selected and interviewed. The PLWHA consisted of two groups: those who were in support groups (the ‘organised’ group) and those who were not members of any support group (the ‘unorganised’ group) but could be accessed. The researcher (the principal investigator) came across the 122 PLWHA in the clinics and community during the period of the study. From these, 18 of them were purposively selected.
Data collection
Qualitative data were also gathered from 11 PLWHA through FGDs and seven PLWHA through IDIs. The PABA at the centres were interviewed individually over a 2 week period. Two focus group discussions (FDGs), using a guide, were also conducted with the eleven HIV/AIDS Patients: one group with five males and the other with six females (at one of the treatment centres). In addition, in-depth interviews (IDIs) were conducted on the health workers and community/group leaders for between half an hour and 45 min each. All the in-depth interviews and focus group discussions were conducted by the principal investigator, in the native language (Idoma) except that of the health workers which was conducted in English. Records of support groups at the two treatment centres were scrutinised for 122 PLWHA that the researcher came across in the clinics during the period of the study.
Due permission had earlier been obtained from the Hospital Managements and the Local Government Chairmen through their Supervisory Councillors. The PLWHA were accessed with the assistance of the Chairmen and Secretaries of Care Support Groups. The PLWHA individually gave informed consent to participate in the study. Community leaders had also given permission to access the group leaders, who themselves agreed to be interviewed, following an explanation of the purpose of the study.
Data analysis
Data from the IDIs and FGDs were transcribed. All the qualitative data were thematically presented to meet the study objectives. Verbatim presentations were used to drive home points made by informants/discussants.
RESULTS AND DISCUSSION
All the data analysed show that both the government and community have programmes towards preventing and mitigating the social and economic impact of HIV/AIDS in Idoma land. These measures are categorised into the following:
Awareness campaigns, public awareness and community behaviours
All the community/group leaders and health workers who gave information agreed that awareness campaigns are carried out in the media, groups and community members adequately. These campaigns have been sponsored by the government in some cases. All the community leaders interviewed believed that there is high level of HIV awareness in their communities/groups, and that people discuss HIV/AIDS freely, because of the awareness exercises. Governments are also involved in the campaign efforts through radio messages, health education programmes like workshops for barbers and posters. In particular, the local government is involved in the awareness campaigns. One AIDS Control officer at a local government office summarized their role in awareness thus:
We do health talk, we go to the open places, we bring people together to give health talks on HIV: how it is transmitted, how it can be prevented. We do such talks. Sometimes we show to people films especially the young people. They gather and show them films, and after the films we also talk to them, sometimes we do it inform of group discussion for us to know what they know and then tell them what they don’t know as well.
However, some of such campaign strategies have been counter-productive. For instance, a HIV/AIDS patient interviewed expressed disappointment with those responsible for HIV/AIDS enlightenment campaigns. She showed the researcher one of such messages: “AIDS has no cure” in a pamphlet she had been given in town. She also said “certain AIDS role plays” (drama or play let on AIDS) in the community, on radio and television; tend to impact negatively on the patients psychologically. This is because these messages depict HIV/AIDS as incurable and a consequence of moral decadence.
Therefore, they (that is, the messages) do not support the clients’ hopes of improved health that they build after counselling sessions. Another informant, an FGD participant, also said those AIDS role plays (drama or play lets on AIDS) convey stigma and moral judgement. This was corroborated by two other PLWHA (FGD participants) who said they no longer bother themselves as these cause them fears. One of them complained, saying:
I don’t disturb myself listening to those people again, If I hear them I even fear to do any meaningful trade because of the fears generated in such drama and pamphlets as if I will die tomorrow...
Thus, two PLWHA said they were no longer doing much anymore to educate themselves through such means; neither do they engage in any meaningful trade because of the fears of impending short life span generated in such campaign messages.
Some PLWHA also lamented that the awareness of HIV/AIDS has “reduced (their) desire to enjoy life,” implying that respondents feel they have been limited in giving vent to their desires. Some stated the effect of this awareness on their general lifestyle “as many people have become faithful to their partners, by abstaining from casual or extra marital sexual intercourse” while others have “become more religious.”
The high level of awareness seen in the public is attested to by almost all informants from the various interviews conducted. For instance, the village/clan heads reported being actively involved in the campaigns within their localities while members of associations did similarly at social club levels. Typically, a community leader stated that:
Yes, we talk about it; very well, we talk about it a lot. We know there is HIV in the community. There have some enlightenment many years ago, almost 13 years now, and before the widespread of this disease we actually talk to them, that if anyone gets this disease, that is the end for that person. And that it is a very dangerous disease, and indeed our community is trying it avoid it.
This general idea that community leaders were all engaged in the HIV awareness creation was somewhat disputed by the matron in charge of an outlet centre of one of the Treatment Centres. She narrated how she organized an awareness campaign at Ogobia on the World AIDS in 2010 (1st December) where secondary school students and health workers carried placards with AIDS prevention and destigmatisation messages, from one street to another; and how her efforts were thwarted by some community leaders. But she decried:
My brother (maintaining eye contact with the principal investigator, shaking her head vigorously in disagreement), you see, we have a major problem in your fatherland here. Our elders are only interested in (some) one gathering them together, buy them drinks and they enjoy themselves. Since we could not do that (that is, during the HIV/AIDS rally), our message did not go down well with them, we created anger in most of them instead.
She was obviously saying that some community leaders were not as committed to the HIV awareness programme as generally portrayed by them. The informant however said that in some communities, “the leaders are really working” because before the AIDS rally, she claimed they (the health workers) used to go to the leaders in the villages and they used to cooperate. And she added:
I think it is when they think one has been given money, they believe the money should be shared or at least they should benefit from it… by calling them together and buy them drinks.
However, reports from some of the PLWHA revealed that some of the campaign messages are counter-productive. They faulted such giggles on radio and television as “breaking the confidence built” after counselling and educational sessions at HIV treatment centres and care support groups. By this they mean that each time certain giggles and messages are presented they become moralized because many of the awareness messages and activities tend to portray HIV/AIDS as death sentence, (‘AIDS has no cure’), and presented strictly as a disease of people with moral decadence. Such methods have left many PLWHA confused and unwilling to adhere to some of them instructions given or the care they receive.
Care support groups
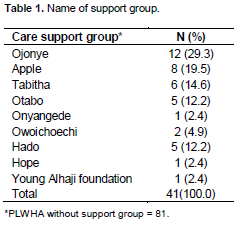
Care support groups are currently available in Idoma land. They provide physical and emotional support for members, although many PLWHA do not subscribe to any care support group. The PLWHA membership of Care Support groups is indicated in Table 1. There are many support groups; nine functional groups Centre A and six registered one in Centre B. An interaction at the two treatment centres/communities from where some of PLWHA were selected to participate in the study showed that most of the PLWHA (66.4%, n=81) with whom the researcher came in the contact within the two weeks of data collection did not either indicate or belong to any care support group. The rest (33.6%, n=41) belong to nine different groups, majority (29.5%, n=8) belonging to the Ojonye care support group (Table 1). Out of the 18 PLWHA who participated in the study (IDIs and FGDs), 12 belonged to Care/Support groups while 6 did not. Although not mentioned by any of the PLWHA, a key informant said a support group called the IdomaImeli Care and Support Association, with 96 PLWHA as members, exists to assist them cope with social alienation. As he put:
People that are infected, we also care for them. We have support groups to take care of those that are infected. These are some of the things we do…
We coordinate the support group of PLWHA in the local government. There are other support groups that are here, we also have group located within the primary health care department called the IdomaImeli Care Support to the people that care for them, that is the people affected. They also provide some level of care for them.
All the nine functional care support groups have PLWHA as the leaders with support from some organisations. Some of the PLWHA who did not belong to any group said that they did not see any need for membership of such groups (Support Groups). But others stated that they were “planning to join one”. One newly diagnosed HIV positive person stated that she needed “to inform my (her) people first before contemplating joining any group.”
Care/Support groups have been advocated by many authors as a source of strength of PLWHA. For example, Gilks et al. (1998) had posited that Care and Support Groups reduce the impact of HIV/AIDS by improving quality of life of PLWHA and their care givers, decreasing stigma of having HIV/AIDS, strengthening HIV prevention activities as target audiences have contact with PLWHA and keeping PLWHA healthy and able to work for as long as possible. Many other studies subsequently presented similar positions.
In one of the groups at Centre A, the secretary to the Care Support Group informed the principal researcher that his own wife (whom he also introduced to the researcher), was also HIV positive but their 18 month old baby boy (whom the woman was carrying at her back) was HIV negative. Both had been HIV positive for over ten years. Although he was a vice principal of one of the special schools in the State (Benue), he spent more time at Care Support Office as a volunteer worker at treatment centre.
Many other PLWHA also work at the centre as volunteer cleaners, attendants and record assistants (personal observation on field). This was confirmed by the Secretary of the Care Support Group. He told the principal researcher (first author) that some of the PLWHA have been employed by the IHVN-ICAP as full time, tenure employees at the centre. These PLWHA participate in counselling and educating both old and newly enrolled HIV positive persons. This indicates that some of the PLWHA in Idoma land are already ‘carrier patients’, meaning that PLWHA also have job opportunities in this community related to their disease status.
Supply of government’s HIV/AIDS drugs
The supply of ARV drugs is an effort of government and NGOs to mitigate the impact of HIV/AIDS. All health workers, community leaders interviewed and PLWHA respondents agreed that the government is providing ARV drugs to patients at either subsidized rate in the 1990s to early 2000s or completely free. However, some informants reported that the supply of AIDS drugs by the government had been sometimes irregular, causing HIV patients to miss medication regimens. The implication of this pattern of supply is that patients could develop resistance to these drugs, making the AIDS treatment more difficult and expensive to procure. As at time of this study (April 2011), the treatment centres feared they were running out of the ARV drugs because the new handlers, ICAP, had not supplied drugs for months. The drugs were being triaged. Almost all the PLWHA FGD participants said if the situation persisted, they engage in a street protest!
Counselling services and health education
Counselling services, nutritional care and education are other attempts to curb the spread and consequences of HIV/AIDS in Idoma land. The two treatment centres used for this study provide both in and outpatient’s pre-and post-test voluntary counselling services for those who wish to have a HIV test or donate blood, as a matter of policy. All the health workers and PLWHA interviewed acknowledged this. These services are free to clients. Three IDI informants (PLWHA) diagnosed in the hospital confirmed that their sexual contacts (spouses, partners) were invited, educated and advised to do the HIV screening, after which they too tested positive. This is however voluntary. On other related services, the health workers interviewed said the hospitals provide other in-and out-patient care for PLWHA. These services consist of treatment of opportunistic diseases free, and nutritional care, including nursing care usually carried out with patient relations. All health workers interviewed also said patients are expected to come for follow-up and for their drugs or monthly or as scheduled, except if they were sick before the appointment date. The hospitals were also said to provide enlightenment campaigns for hospital workers and the general public.
Community sanctions and position on pre-marital HIV screening
The community/group leaders interviewed said that the traditional/community leadership has place sanctions on certain practices that are believed to propagate HIV. Strategy, in form of community response, takes the form of sanctions on commercial sex work hence micro-credit facilities and other strategies are being put in place. Two informants emphasized other rules in their communities such as that all new marriages must be preceded by HIV testing by the individuals wishing to marry. Otherwise, community leaders and members will not participate in such in such marriages.
Credit facilities and training
Credit facilities and training have also been organised by Idoma communities to help curb the HIV/AIDS impact. One community leader, who gave key information on government support and control activities on AIDS, said that the Benue State Government has provided some micro-credit facilities, and has established garri-processing industries for young people through cooperative societies to increase the economic capacity of the youth. This is thought to discourage risky behaviours of the youth especially the young women.
Similarly, they also said that children orphaned by AIDS who have been separated from immediate families, and cannot continue their school, are also being enrolled into apprenticeship trainings such as tailoring and mechanic services. The community is responsible for their training. Community-sponsored credit facilities are one of the community approaches to the control the impact of disease. The government of Benue State was said to have provided the micro-credit facilities through the State Agency for Control of AIDS (BENSACA). Similarly, most of the campaigns were also said to have been supported by the State government. This finding contrasts with the widely speculated government inactions in AIDS activities (Oke, 1999).
CONCLUSION
Findings have highlighted some HIV/AIDS prevention and mitigating measures in a traditional African community; the Idoma land. These are in the areas of AIDS awareness campaigns, supply of anti–retroviral drugs, counselling services, as well as other community-initiated sanctions on prostitution, training/credit facilities for affected people, among others. Some of the identified measures such as the awareness campaign messages and supply of ART drug have setbacks, which have the potential of complicating the HIV/AIDS prevention and mitigation initiatives. The study has thus identified certain weak-nesses in some of the initiated measures in HIV/AIDS awareness campaign messages.
RECOMMENDATIONS
HIV/AIDS mass education strategies using healing and destigmatising messages, drama, and consistent treatment programmes should be appropriately designed and disseminated to curb HIV spread and mitigate the consequences of the HIV/AIDS epidemic, including stigma and discrimination. Authorities managing HIV/ AIDS programmes should curb drug shortages at treatment centres to prevent treatment failures, and resistance. Similarly, health workers, the mass media and communication managers, and relating persons of PLWHA need to use appropriate languages to present messages on HIV/AIDS prevention. Community-initiated sanctions need to be strengthened to effectively achieve their aims.
HIV/AIDS workers such as health workers (for example, nurses), social workers, and the information/media managers especially in resource-poor communities, should take cognisance of culture-initiated measures and communication content of HIV/AIDS campaign messages and build such into AIDS care. AIDS care in Primary Settings is particularly implicated. There is also the need for those involved in HIV/AIDS control and care to brainstorm on culture- and situation-appropriate modalities of communication HIV/AIDS control measures resource-poor settings like the traditional African community. Further studies are required to determine the effectiveness of community-initiated programmes on HIV/AIDS prevention and control especially in traditional African community.
CONFLICTS OF INTEREST
The authors have not declared any conflict of interests.
REFERENCES
|
Barnett T, Whiteside A (2002). AIDS in the twenty-first century: Disease and Globalization. New York: Palgrave Macmillan. pp. 3-23. |
|
|
Ehiri J, Anyanwu E, Donath E, Kanu I, Jolly P (2005). AIDS-related stigma in sub-Saharan Africa: its context and potential intervention strategies. AIDS Public Policy J. 20: 25-39. |
|
|
Factsheet (2011). Update on the HIV/AIDS epidemic and response in Nigeria. |
|
|
Federal Ministry of Health (FMOH) (2007). HIV/STI biological and behavioral surveillance survey. National AIDS/STI Control Programme and the Federal Ministry of Health, Abuja. |
|
|
Gilks C, Floyd K, Haran D, Kemp J, Squire B, Wilkinson D. (1998). Sexual Health and Health Care: Care and Support for People living with HIV/AIDS in Resource Poor Setting. Department of International Development (DFID), London. |
|
|
Hilhorst T, van Liere M, Konning K, Abeda F, Jolayemi T, Saror S (2004). Impact of AIDS on rural livelihoods in Benue State, Nigeria: Implications for policymakers. Royal Tropical Institute. |
|
|
Idoma Community Development (ICD) (2009). The Idoma Cultural Day, Zaria: Xubu Prints. |
|
|
Ilebani OA, Fabusoro E (2011). Effects of Community-Based Care for People Living with HIV/AIDS on Their Well-Being in Benue State, Nigeria. Res. J. Med. Sci. 5(5):294-304. |
|
|
National Agency for the Control of AIDS (NACA) (2005). BCC Strategy: FMoH Abuja. |
|
|
Oke E (1999). The HIV/AIDS Scourge: Look at Yourself. Natl. Health Dig. 2(6):8-12. |
|
|
SWAAN (Society for Women against AIDS) (1999). How to Live with AIDS.SWAAN. Abuja, Nigeria. |
|
|
UNAIDS (2004). Report on the Global AIDS epidemic. |
|
|
World Health Organization (2012). "HIV/AIDS Programme - Prevention and Treatment of HIV and other Sexually Transmitted Infections for Sex Workers in Low- and Middle Income Countries: Recommendations for a Public Health Approach." Geneva: World Health Organization. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


