Full Length Research Paper

ABSTRACT
INTRODUCTION
Drug addiction affects the whole society irrespective of age, sex, caste, creed, and so forth. Individual may become dependent on a wide variety of chemical substances, ranging from stimulants to depressants. Drugs are taken for treatment or enjoyment; they do not pose any problem but their excessive use has definitely raised bio-psycho-social problems. In ancient times, drugs were mainly used for the treatment of ailments, but ritualistic abuse is considered as the sign of enjoyment. The habit of addiction in India is evident from the eras of Rig-Veda and Mahabharata. According to Morrow and Suzanne (1975), the use of drug to alter consciousness is nothing new. It has been a feature of human life in all places on earth and in all ages of history. The use of drugs in India is not a new phenomenon. Interestingly, it has a mythical past and also a long history of nearly ten thousand years. Soma and Sura, the two famed celestial drinks, origins of which are attributed to the mythological ‘Sagar-Manthan’, became essential parts of the Rig-Vedic ritualistic sacrificial ceremonies. Of the two headier liquors soma and sura to which the Aryans were addicted, soma, libation of which constituted an essential part of sacrifice, was liberally and convivially drunk after the sacrifice (Modi, 1985; Thapar, 1986). Drinking of soma has been eulogized time and again in no uncertain words in the hymns of the Vedas.
Ganja, bhang and charas which are derivatives of cannabis sativa are other types of drugs very much prevalent in India. They are used during religious and social ceremonies among the Hindus. On Shivratri, bhang is poured on Shivlinga, reflecting the presence of the invisible transcendental reality of Shiva. Other festivals during which cannabis is used are Janmashtami and Holi. During the Holi festival, men and women drink a beverage made of cannabis leaves, milk, and dried fruit (Fisher, 1975).
There are number of different factors of drug addiction. Some reasons cited by Persaud (2007) are “to celebrate, drown sorrows, for pleasure, enjoyment and excitement, escapism and avoidance of stressful situations, to feel socially comfortable, boredom, peer pressure, coping with withdrawal symptoms and craving, coping with depression and low self-esteem, to increase confidence, relieve other psychological, psychiatric and physical symptoms or pain, increase energy and concentration, or to enhance performance, to lose weight, unwind and to have fun”. Chatterjee (1985) identified the following factors which contribute to drug addiction:
Other most important factor is place of rearing of children i.e. where children spend their youth. That place is known as neighbourhood. People living next door are an important group which affects one’s life. People living within the same neighbourhood may be more similar to each other than people living in other neighbourhoods; not only because similar people move to similar neighbourhoods, but also because they share similar lifestyle. Neighbourhood can be an important socializing agent for children, especially when ties are strong and the community is close. Research into urban villages shows that strong neighbourhood ties are associated with children who are more socially competent, who are less depressed, and who perform better in school (Marshall et al., 2001).
In a study by Elliot et al. (2006), Neighbourhood is generally assumed to play an essential role in raising children. When the strong interpersonal ties, shared socialization, values, utilization of community resources fail to materialize or develop in the neighbourhood, children are put at risk for poor developmental outcomes and dysfunctional lifestyle. Elliot et al. (2006) very well defined two types of neighbourhoods i.e. the advantaged and disadvantaged neighbourhood. Youths living in disadvantaged neighbourhood may be more vulnerable to official action for their delinquency than are youths living in more advantaged neighbourhood. Some neighbour-hoods are good places to raise children. Living in these areas increases the chances that children will grow up to be healthy, responsible and productive adults. Other neighbourhoods are bad places to raise children, places where they are exposed to violence, dysfunctional lifestyles, negative role models, unfriendly neighbours and poor quality schools. Children living in these neighbourhoods may have little opportunity to acquire the personal skills and experiences necessary for effective participation in mainstream community life.
Objective
The present study has focused on the role of neighbours in helping the drug addicts to get de-addict.
METHODOLOGY
The total sample of the present study was targeted at 200. The data were collected with the help of an interview schedule. 200 drug addicts were interviewed in the year 2014 to get responses about the participatory role of neighbours play in their lives. The rationale behind this objective was to know various efforts neighbours play towards community. The area selected for the present study was community based de-addiction clinics held in and around Chandigarh by two pioneer hospitals i.e. PGIMER and government medical college and hospital, Chandigarh. All who visited community based de-addiction clinics were interviewed. Self constructed interview schedule was prepared for the research.
Initially, it was decided to use quota sampling but we could not fix any quota or stratified the sample into male and female categories. During the pilot study, a few practical difficulties were faced in selecting the sample. Firstly, the patients were not willing to give interviews. Secondly, women patients were not available and thirdly, CBDCs were held once in a week for two and a half hours. Thus, purposive sampling was used. Respondents in the present study comprised those who were willing to give an interview. Thus, whosoever visited the CBDCs irrespective of age and sex and was willing to give interview was made part of the study.
SOCIO-ECONOMIC PROFILE
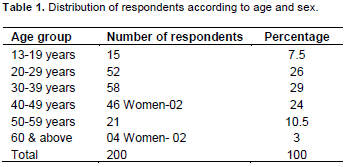
Age and sex
Data on age are presented in Table 1 and it shows that majority of the respondents i.e.29% belonged to the age group of 30-39 years, followed by 26% in the category of 20-29 years of age group.
Respondents of the age group of 40-49 years comprised 24 per cent of the sample and 10.5 per cent of the respondents in the age group of 50-59 years. Data in Table 1 highlight that 7.5 per cent respondents were found to be between 13 to 19 years of age and 3% of the respondents were above 60 years of age. 4 women also became part of sample as shown in Table 1. Drug addiction among women is a hidden problem and various studies indicate that it is increasing among women. Representation of women in the present study was negligible. No separate column in the tables is made for them. Wherever there was a response by women, it has been specifically highlighted in all the relevant tables.
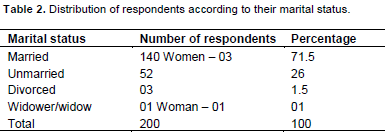
Marital Status
Data in Table 2 indicate a vast majority of the respondents i.e. 71.5 per cent who were married and 26% who were unmarried. Three cases of divorce were also recorded, and the reason for divorce was attributed to drug addiction of the spouse. Only two cases fall in the category of widower/widow among the respondents.
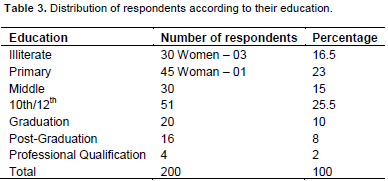
Education
Educational status of drug addict respondents is presented in Table 3. It shows that 16.5 percent of respondents were women and illiterate, 23 percent respondents had their education up to primary level, 15 percent respondents had their education up to middle level and 25.5 percent had their education up to high school or secondary level.
A small percentage of respondents i.e. 10 and 8 percent had completed their graduation and post-graduation respectively. Only 2% respondents were found with professional education, one had completed his MBBS degree and three had done B. Tech.
Occupation
The data indicate that a significant proportion of respondents were self-employed, labourers and had private jobs. Occupation distribution of respondents is presented in Table 4. Data show that 29 per cent of the drug addict respondents were employed in private jobs like working as computer operator, medical transcriptionist, news reporter, courier boy, sales man, pantry worker, etc. 25 per cent of drug addict patients were self-employed and were engaged in farming, tailoring, motor mechanic, barber, stall-keepers, street hawkers, etc. 20.5 per cent of respondents were engaged as daily wagers like white washers, masons, plumbers, welding workers, rickshaw pullers, etc?.
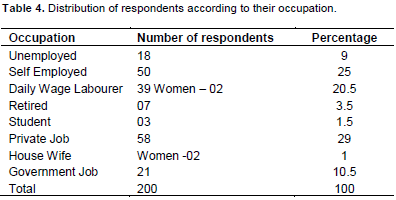
Seven (7) 3.5% were found to be retired from govern-ment jobs. All these retired respondents were drivers and were addicted to bhukki. It was disclosed by the respondents that they were consuming bhukkias it helped to keep them awake and alert during driving at night. Further it was found that there were 10.5 percent respondents on government jobs and on different ranks. One of them was inspector from the Department of Excise & Taxation. The remaining respondents were unemployed (9%) and they were dependent on other family members. Amongst women, 1% were house wives and 1% were daily wagers. Out of the total sample there were 3 students.
Income
Income is a source of livelihood and presents economic status of an individual. Income distribution of respondents is presented in Table 5 and it shows that 37 percent respondents were earning less than Rupees 3500 per month followed by 21, 11.5, 9, 5.5 and 4.5 percent in group of Rupees 3501-7000, 7001-10,000, 10,001-15000, 15,000-20,000 and 20,000 and above, respectively.
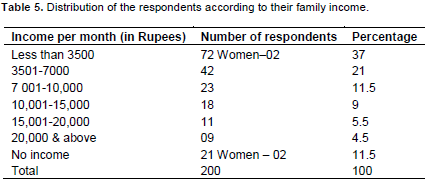
11.5 per cent respondents belonged to the category of ‘no income’. Out of these, 8 of the respondents reported that they always forced their mothers or wives to give them money. It was also narrated by the respondents that they used to beat their wives to get money (wives were earning as daily wage labourers). Respondents who had no source of money were 4%.
Respondents used to borrow money from their friends or some of their friends themselves gave drugs to the respondents without asking for money. For example, in one case a respondent was addicted to Ganja and was consuming it by plucking leaves of the plant Cannabis Sativa. This plant is found abundantly as a weed in India. Two women respondents got money from their spouses to fulfill some of the family’s daily needs, and they also managed to buy drugs with this money. In majority of the cases respondents were earning on their own, and never asked for money from their family members.
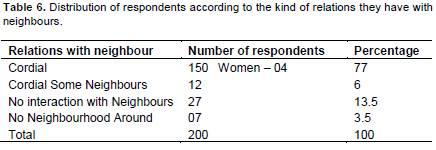
In our society, the neighbours occupy very important place in the social life. In the event of any problem the first help always comes from the neighbours, as, it takes time for their relative to reach the family from distant places. The degree of help received by the neighbours may differ due to interpersonal relations and various other factors. Still this aspect was probed and their responses are tabulated in Table 6. 77 per cent of the respondents reported good/nice relations with their neighbours and they were helped by them in difficult times. Table 6 further reveals that 6 per cent of the respondents claimed good relations with only some of the neighbours. It was found that 13.5% of the respondents did not believe in maintaining relations with their neighbours thus, had no interaction with them. Another 3.5% of respondents living in rural areas resided in isolated fields and did not have any population in the vicinity.
In modern times the importance of neighbours and role played by them is seen to be decreasing. People are seen busy in their own worlds, private lives, not bothered about what is happening, neither help is asked nor it is provided. All forms of crimes are happening both in rural and urban localities, but people hardly come out of their houses to help.
In one of the cases of the village, it was told by one of the respondents that, a drug addict used to come on the road during midnight screaming, shouting, and use abusive language. His family (wife and kids) never came out of the house to stop him nor did the neighbours ever come out to say anything to him. He sold some of his property (land) under the influence of drugs. Property dealers, and neighbours used to look for the favourable times (when he was heavily drunk) to make deals with him. He died after consuming some cheap, local made drugs. The whole village gathered for his last prayers and remarked that his death is a boon for the family and village. Now, the present situation is his son is also a drug addict.
There goes a saying that the people are known by the locality they live in. This is the reason people try to choose good localities for their abode, free of anti-social activities and crime, where neighbours are good and gentle people. Generally neighbours of deviant behaviours are avoided by people in such localities. Respondents revealed that 59 per cent (Table 7) of them still enjoyed due recognition given by their neighbours and well aware of their habit of substance abuse. It later transpired that a large number of people residing there were consuming one or the other drug in their locality. So it was not considered that much of evil in that social set up and was accepted as normal than other localities.
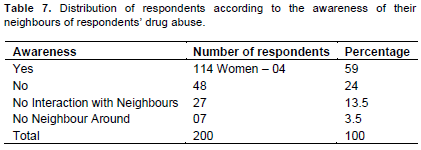
Table 7 further reveals that 24 per cent of the respon-dents reported that their neighbours did not pay any attention to them and were ignoring them. 13.5 and 3.5 per cent of the respondents did not have any interaction with each other and did not have any neighbours respectively.
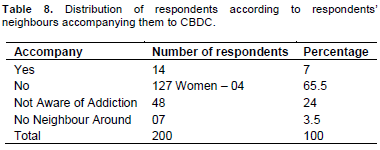
Only the people feeling concerned about the drug addicts accompany them to the Community based de-addiction clinics for treatment. An effort was made to know the number of such neighbours. But only 7 per cent respondents reported that their neighbours extended help and accompanied them to the Community based de-addiction clinics as the occasion demanded.
Table 8 shows that a majority of the respondents (65.5 per cent) told that their neighbours did not bother to accompany them to the community based de-addiction clinics. It was seen that a good number of women neigh-bours acted as Samaritans and took the respondents for treatment. According to a women resident of Mohali (Punjab), she and her husband were very active in social work. 17 years ago, they came to Mohali to settle permanently. Once she had noticed some deviant boys in her locality, who were addicted. All locality members were feeling unsafe. Once, some of the locality members urged her and her husband to do something about these boys because they were polluting their locality. She wanted to help those boys by making them drug free. She tried to make them understand but the boys ignored her advice and misbehaved. Then she called the police and the boys got arrested. When the boys left the grip of the police they took revenge on her by grabbing her two young boys (16 and 18 years old) and introduced them to drugs. Both boys are still addicted to drugs. This incident changed her view and she decided to never help anyone. The fear of revenge or disturbance in the family because of immoral people discourages a common man to help others.
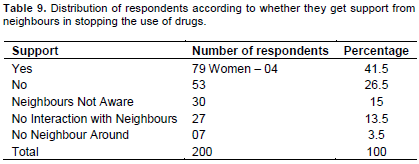
Drug addiction is a disease of the brain. Its patients require sympathy and encouragement during their treatment but it is a painstaking process to be with them, continuously encouraging them, emotionally supporting them, educate them, and reinforcing them during the period of relapse. Some neighbours involve themselves in the above process considering it their social responsibility to help the addicts recover from the drug dependence.
Table 9 revealed that 41.5 per cent of the respondents encouraged them to shun drugs and lead a healthy life. They convinced them that it was a medical condition and can be cured with the therapy. They acted as motivators to break the cycle of drug dependence. They encouraged them to abstain from drugs totally. 26.5 per cent of the respondents said that they did not get any encouragement from their neighbours. 15 and 3.5 per cent respondents apprised that their neighbours were not aware about their condition. 13.5 respondents did not like to interact with their neighbours.
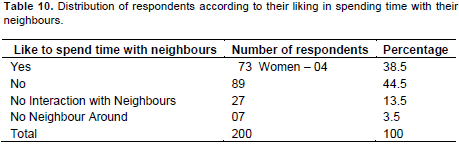
Drug de-addiction requires the services of medical doctors who could take care of patients physically and mentally. Drug addiction is a complex diseases . Drugs bring changes in the brain which triggers compulsive drug abuse. The science of psychiatry plays an important role in understanding the disease of the addict at an individual level and suggests a remedy for it. Drugs make the addict disenchanted with his family, friends and neighbours. An attempt was made to figure out how many addicts liked to spend time in the company of their neighbours.
Table 10 indicates that 44.5 per cent addicts said that they did not like to spend time with their neighbours whereas 38.5 per cent of them liked to spend time in the company of their neighbours. 13.5 and 3.5 per cent of the respondents did not have interaction and did not have any neighbours respectively.
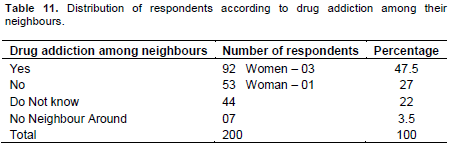
The prevalence of drug addiction becomes high in localities where drug addicts already exist and influence the vulnerable people to their fold. Social environment influences the risk of addiction. An addict neighbour can easily influence an individual if he is more prone to it or is at a vulnerable age of development and lacks judgment, self control, and ability of decision making.
In the study it was found that 47.5 per cent addicts had neighbours already caught in the habit of substance abuse whereas 27 per cent addicts did not have any addict neighbours (Table 11). Table 11 also reveals that 22 per cent drug addicts were not aware that their neighbor was addicted to drugs.
CONCLUSION
In the present study, the majority of the drug addicts had cordial relations with their neighbours. A very few neighbours accompanied addicts to the Community based de-addiction clinics. Less than half the number of respondents received encouragement from their neighbours to shun drugs and lead the healthy life.
It was concluded from above that there is a lot of difference between interacting in a normal way with neighbours. Very less number of neighbours extended their arms to help their drug addict neighbours. Due to lack of emotions, intimacy, warmth, time, and possessing of jealous and self-centered behaviour neighbours are not proven as remedy for their drug problem. They were not seen as to coming forward to become a helping hand to the addicts.
REFERENCES
|
Chatterjee SK (1985). Drugs and the Young: Some legal Issues. Bulletin on Narcotics. 37(2&3):157-168. |
|
|
|
|
|
Elliot SD, Scott MB, Amanda RE, William JW, David H (2006). Good Kids from Bad Neighbourhoods. U.K.: Cambridge University Press. |
|
|
|
|
|
Fisher J (1975). Cannabis in Nepal: An overview. In Rubin, fifth edition, Cannabis and Culture. The Hague: Mouton Publishers. |
|
|
|
|
|
Marshall NL, Noonan AE, McCartney K (2001). It Takes an Urban Village: Parenting Networks of Urban Families. J. Family. 22(2):163-182. |
|
|
|
|
|
Modi I (1985). Leisure, Mass Media, and Social Structure. Jaipur: Rawat Publication. |
|
|
|
|
|
Morrow, Suzanne W (1975). Drugs in American life. New York: The H.W. Wilson Company. |
|
|
|
|
|
Persaud R (2007). The Mind: The User's Guide. London: Sage Publications. |
|
|
|
|
|
Thapar R (1986). A History of India. Vol. 1, New Delhi: Penguin Books. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


