Full Length Research Paper
ABSTRACT
Globally, diarrhoea is considered as a major threat to human health and remains a leading cause of mortality and morbidity. Several studies have shown that incidence of diarrhoea is influenced by source of drinking water and mediated by some compositional and contextual factors. However, not much is known about how mediating factors interact with source of drinking water to influence incidence of diarrhoea in Ghanaian adults. This study was carried out to investigate how compositional and contextual factors interact with source of drinking water to influence incidence of diarrhoea. A survey was carried out in fourteen regions of Ghana. A multivariate regression model was used to determine how compositional and contextual factors mediate the effect of drinking water source on incidence of diarrhoea. The results showed that source of drinking water and geospatial (regional) disparities are the two main factors that affect incidence of diarrhoea in Ghana. Households that depended on river as a source of drinking water were 64% more likely to have diarrhoea compared to those who drink from pipe-borne water. Upper West Region recorded the highest incidence of diarrhoea (37%) and Volta Region recorded the least incidence of diarrhoea (less than 1%). Escherichia coli bacteria was detected in all water sources. Streptococcus was detected in all the water samples except dam water. Some of the causes of diarrhoea were found to be beyond the control of individuals warranting the need for government intervention and policy to improve the sanitation in the country.
Key words: Childhood, morbidity, mortality, spatiotemporal, water quality.
INTRODUCTION
Globally, diarrhoea is considered a major threat to human health and remains a leading cause of mortality and morbidity to people of all ages (WHO, 2017). Globally, about 1.7 billion diarrhoea cases are observed annually and 1.5 million deaths are recorded (WHO, 2008). Diarrhoea is reported to be the second major killer of children under five years in the world. Recent reports suggest that about 1.7 billion cases of childhood diarrhoea are reported globally every year (WHO, 2017). Although the number of deaths, due to diarrhoea disease reduced from 1.731 million per year in 2010 to 700 000 per year in 2011 (Walker et al., 2013) and now 525,000 per year in children (WHO, 2017), it continues to be an important public health problem in low- and middle-income countries (Chowdhury et al., 2015; Fagbamigbe et al., 2021).
Untreated or polluted drinking water, poor sanitation, poor hygiene practices and bacterial contamination are reported to be major contributors to diarrhoea disease in the world (Boadi and Kuitunen, 2005; Prüss?Ustün et al., 2014; Gwimbi et al., 2019). The World Health Organization suggests that basic hygiene related diseases have a significant impact on human health (WHO, 2004). Water quality has become a global concern and so necessitates the need to ensure proper preservation and conservation of water to ensure good water supply for good health. There have also been reports that 11% of the population in the world depend on unimproved water sources such as dug well, surface water and springs (Wolf, 2014).
In Ghana, the most susceptible group to diarrhoea-related morbidity and mortality are children, especially those under five years (Asamoah et al., 2016). About 14000 children die from the disease every month in Ghana (Asamoah et al., 2016). There is a link between poverty on one hand, and poor sanitation, poor nutrition and poor quality water supply to poor households, on the other hand (Cooke et al., 2016; Saboksa et al., 2021). According to Boadi and Kuitunen (2005), poverty is a major contributor to poor health in Ghana. In Ghana, there are more poor people residing in the Northern part than the south while more of the rich are found in the south (Ghana Statistical Service, 2015; Cooke et al., 2016). Ghana may not be able to achieve the Sustainable Development Goals (SDGs) if nothing is done about the socio-economic gap between the rich and the poor in society.
Several studies have shown that incidence of diarrhoea is influenced by source of drinking water and mediated by some compositional and contextual factors. However, not much is known about how the compositional and contextual factors interact with source of drinking water to influence incidence of diarrhoea in Ghanaian adults. Besides, most of the studies have also relied on demographic and health survey data which focus on children under five years. Studies on factors that affect incidence of diarrhoea in Ghanaian adults are limited. This study was carried out to assess how compositional and contextual factors interact with household source of drinking water to influence incidence of diarrhoea in Ghanaian adults.
MATERIALS AND METHODS
Study population
A total of 3521 households across fourteen administrative regions of Ghana were included in the study.
Sampling/data collection technique
Field survey and laboratory analyses were carried out to identify the source of incidence of diarrhoea in Ghanaian households from November 2021 to March 2022.
Structured questionnaires were used to elicit information on the incidence of diarrhoea in the last four weeks prior to administering the questionnaires in households. The country was stratified into regions; the number of households interviewed per region is presented in Supplementry Table 1. The regions were further stratified into urban, rural and peri-urban areas. Communities within these areas were further stratified considering the socio-class and livelihood of the people. Purposive sampling was used to select households and respondents that cut across the social classes and livelihoods in the communities. Using a structured questionnaire, data was obtained from respondents (who were either the head of the family or any member above the age of 18). In each selected household, all residents aged 18 years or more were deemed eligible to respond to questions. This gave all residents of a household equal opportunity to be interviewed. The interviews were conducted in the local language of the people in the locality, where the surveys were carried out. The objectives of the research were made known to the respondents before they were included as subjects of the research. Respondents were assured of their anonymity and confidentiality of their responses to the questionnaires.
Ethical clearance (UCCIRB/EXT/2021/21) was obtained from the Institutional Review Board of the University of Cape Coast, Ghana. All respondents gave their concert before they were included in the study.
Response variable
The dependent/response variables considered in this study was incidence of diarrhoea. Incidence of diarrhoea was represented as dichotomous variable. The respondents, who have had diarrhoea in the past four weeks were coded as ‘1’ and respondents who answered no to diarrhoea incidence in the same period were coded as ‘0’.
Key predictor variable
The choice of predictor or independent variable for this study was based on parsimony, literature review and practical significance. The foremost independent variable was derived from main source of drinking water. Six observations were recorded under the main source of drinking water; pipe-borne water, well, spring, river, bore- hole and sachet water.
Compositional and contextual factors
Compositional factors are defined as factors relating to the socio-demographic characteristics of individuals (Collins et al., 2017). They comprise biosocial and socio-cultural factors. Biosocial factors are biological or physical characteristics present at birth and not amenable to change (Pol and Thomas, 2000). The customs, beliefs, values and lifestyles are referred to as socio-cultural factors. The compositional factors considered in this study are gender (male and female), age (18-25, 26-35, 36-45, 46-55, 56-65 and above 65 years), marital status (single, married, divorced and widow/widower), household size (1-5, 6-10, 11-15 and 16-20 people), educational attainment (no literacy, non-formal, basic education / middle school, secondary/ technical School and tertiary) and household income (Up to $16.95, $17- 84.75, $84.92- 169.49, $ 169.66-254.24, $254.41-338.98 and above 338.98).
Contextual factors are the broader physical and social opportunities in a region, such as availability of and access to services (Collins et al., 2017). In this study, the contextual factors included region (Greater Accra, Ashanti, Eastern, Central, Upper West, Upper East, Volta, Oti, Bono East, Bono, Northern, Savanna, Western, and Western North) and community type (urban, peri-urban, rural and cottage)
Data analysis
The statistical analyses were carried out in STATA 16 MP (Stata Corp, College Station, TX, USA). Descriptive statistics were done to describe the level of incidence of diarrhoea in Ghana across the fourteen regions. Inferential and multivariate statistics were carried out to assess relationships between incidence of diarrhoea and source of drinking water, while controlling the relevant compositional and contextual factors.
Univariate analysis
Univariate analysis of independent variables of incidence to diarrhoea was done using Pearson Chi-Square and Cramer’s V statistics. Pearson Chi-Square was used to assess the relationship between the predictors and incidence of diarrhoea. Cramer’s V statistic was used to estimate the strength of the association.
Multivariate regression
The effect of source of drinking water on incidence of diarrhoea was estimated using a negative log-log regression and reported as exponentiated coefficients or odds ratios (OR). An OR of 1 implies that predictor does not affect odds of incidence of diarrhoea, OR greater than 1 means predictor is associated with higher odds of incidence of diarrhoea; and OR less than 1 means predictor is associated with lower odds of incidence of diarrhoea. Robust estimates of variance were used to correct for the clustering of observations in units of household and any statistical outliers in the estimation of standard errors. The study used 95% confidence interval and level of statistical significance was set at 0.05.
Some compositional and contextual variables known in literature to affect incidence of diarrhoea were controlled for in the models. Zero-order negative log-log regression model of the relationships between incidence of diarrhoea and source of drinking water and compositional and contextual factors was first run. Three models were run under multivariate statistics; source of drinking water and biosocial factors (model 1), socio-cultural factors (model 2) and contextual factors (model 3).
Microbial analysis
Samples of water sources identified to be used by households from the field survey for domestic activities (Example Rivers, springs and dams) were sampled for microbial load analysis in the laboratory.
Some 500 ml plastic containers were sterilized with warm distilled water and used for sampling. The sterilized sample bottles were submerged to a depth of 0.5 m, opened, filled, corked, and removed using the grab method. Using a multipurpose (Palintest multipurpose device) probe, pH, conductivity, total dissolved solutes and temperature of samples were measured in-situ. After the measurement of the physical parameters, sampling was carried out and samples immediately kept on ice for onward transport to the science laboratory at the College of Agriculture for microbial load assessment. Analysis was carried within 24 h of sampling.
Microbiological analyses
Total and faecal coliforms
The most probable number (MPN) method was used to determine total and faecal coliforms bacterial in the samples. Serial dilutions of 10-1 to 10-3 were prepared by picking 1 ml of each sample into 9 ml of Phosphate Buffered Saline (PBS). One millilitre aliquot from each dilution was inoculated into 5 ml of MacConkey broth (prepared according to manufacturers’ instructions) in culture tubes. Incubation of total coliforms was done in an incubator at 35 to 37°C for 48 h and that of faecal coliforms were incubated at 45 to 47°C for 48 h. Tubes showing colour change after 48 h of incubation were identified as positive for both total and faecal coliforms for further biochemical tests.
Escherichia coli
MacConkey agar was prepared according to manufacturers’ instructions and poured in sterilized petri plates in a sterilized cabinet to solidify. After solidification of the media, 1 ml of each sample from phosphate buffered saline was inoculated on the plates and incubated for 48 h. Colonies showing pink were counted as presumptive results and were sub cultured for further biochemical tests.
Sub culturing of sample (pure culture)
Nutrient agar was prepared according to manufacturers’ instructions for microbial analysis. Positive colonies were streaked (sub cultured) on the nutrient agar using a sterilized inoculation loop. Incubation was done for 24 h at the temperature of 35 to 37°C.
Gram staining
Fresh culture was used for the gram staining. Isolated colony on the nutrient agar after incubation was touched with a sterilized inoculation loop after putting a drop of distilled water on a clean slide. Picked cells from the isolated colony on the nutrient agar was smeared with the distilled water on the slide and allowed to dry. After drying, cells on the slide were heat fixed and a few drops of crystal violet were put on the part of the slide containing the cells for 60 seconds. The slide was rinsed with distilled water after 60 s and a few drops of Gram’s iodine applied on the slide. The iodine was rinsed after 60 s and a drop of 95% alcohol applied. The sample was rinsed with distilled water after 5 s. Counter stain was done with Safranin for 30 s and again rinsed with distilled water. Slide was allowed to dry and a drop of immersion oil applied and was viewed under microscope with ×100 lens for observation. All Gram positives samples showed violet and Gram negatives samples showed pink.
Triple sugar iron (TSI) test
Triple sugar Iron (TSI) consists of glucose, lactose, and sucrose. Bacteria inoculated in it can provide positive results with a yellow coloration for either one of the sugars or all with even the production of gas and/or ferrous ammonium sulphate (black precipitate). In this test, the TSI were streaked with the test bacteria and the butt stabbed with the aid of a sterile inoculation loop. The inoculated TSI were incubated for 24 h at 35°C. After incubation, change in colour at the slope, the butt and gas production were recorded and compared with a chart.
Indole test
The test detects the presence or absence of the enzyme tryptophynase which break down tryptophan. In this test, Kovac’s reagent was added to peptone water inoculated with bacterial isolate. A pinkish to reddish ring at the top level of peptone water was taken as indole positive.
RESULTS
Descriptive
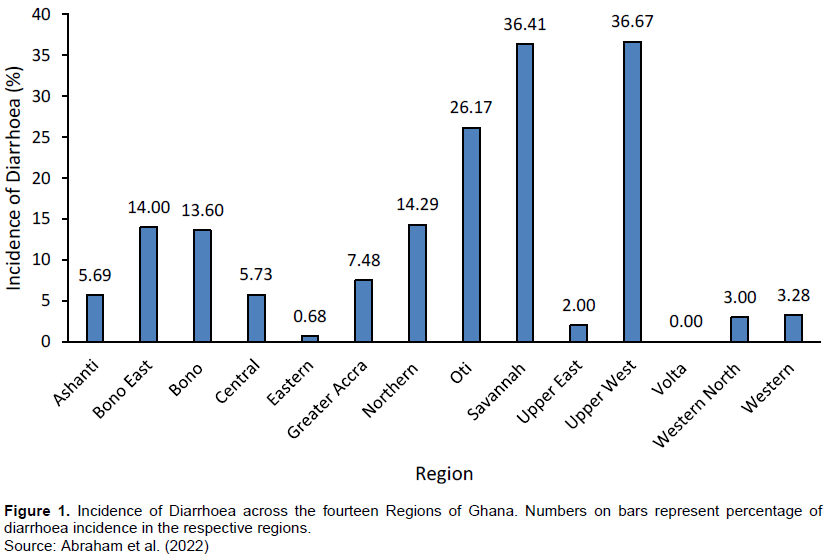
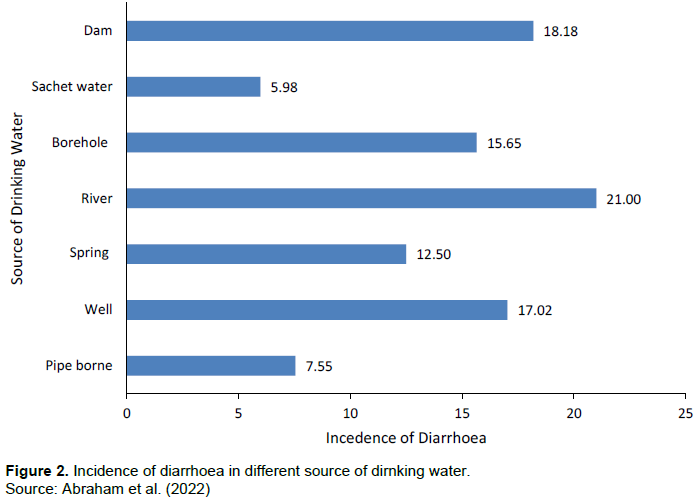
The analysis of results showed that the incidence of diarrhoea in Ghana was 9.5% among Ghanaian household. The results of the descriptive analysis of incidence of diarrhoea show that Upper West Region recorded the highest incidence of diarrhoea (36.67%) followed by the Savannah Region (36.41.90%) (Figure 1). Volta Region recorded the least incidence of diarrhoea of 0.00%. The magnitude of diarrhoea incidence across the various sources of drinking water varied. For instance, river recorded the highest incidence of diarrhoea (21.00%) whereas sachet water had the least incidence of diarrhoea (5.98%) (Figure 2).
Univariate analyses
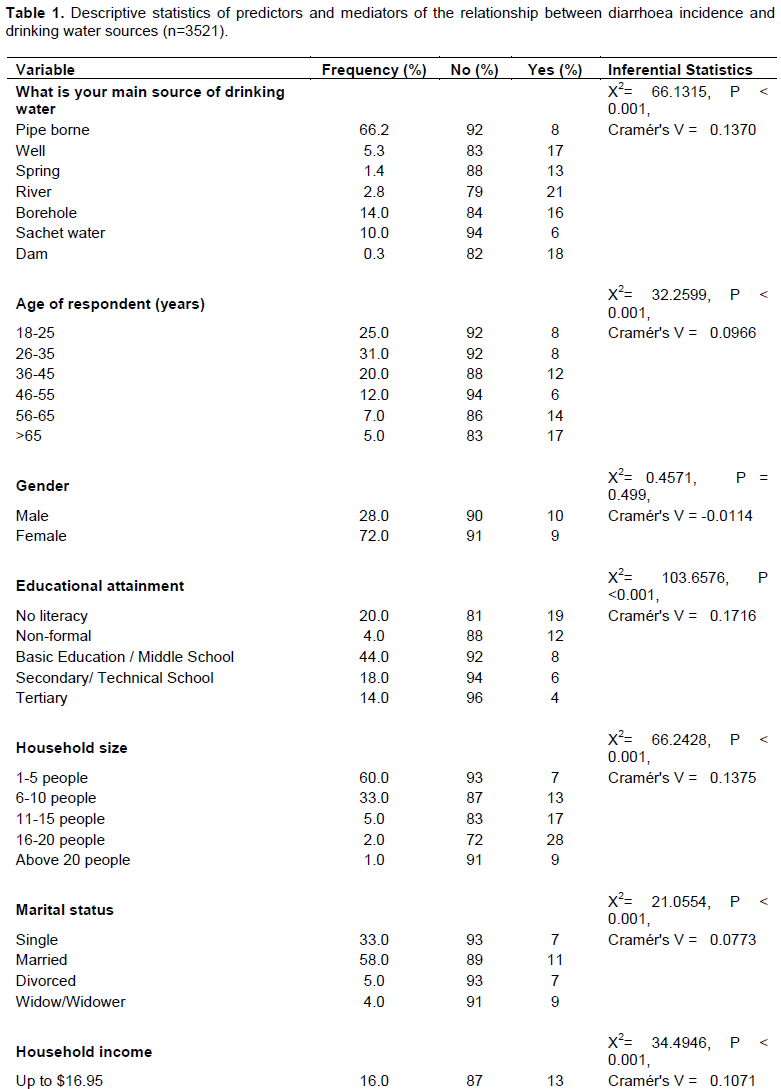
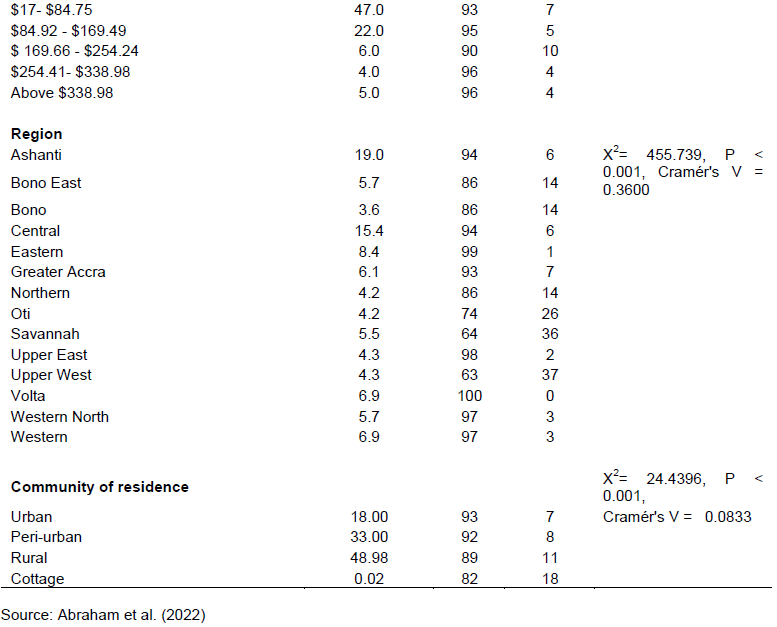
Table 1 provides inferential statistics of the relationship between incidence of diarrhoea and drinking water sources as well as the compositional and contextual factors. The results show that incidence of diarrhoea is not independent of source of drinking water (P<0.0001). Similarly, chi-square statistic results indicate that there are associations between the compositional factors and incidence of diarrhoea except gender (P=0.499). The observed differences in incidence of diarrhoea and contextual factors as indicated in the chi-square results also rejected the hypothesis that incidence of diarrhoea and community of residence and region are independent. The Cramer’s V statistic reported weak association between incidence of diarrhoea and access to drinking water source. Likewise, the result indicated weak associations between incidence of diarrhoea and the compositional and contextual factors with the exception of region which showed strong association.
Zero-order relationship between incidence of diarrhoea and predictors
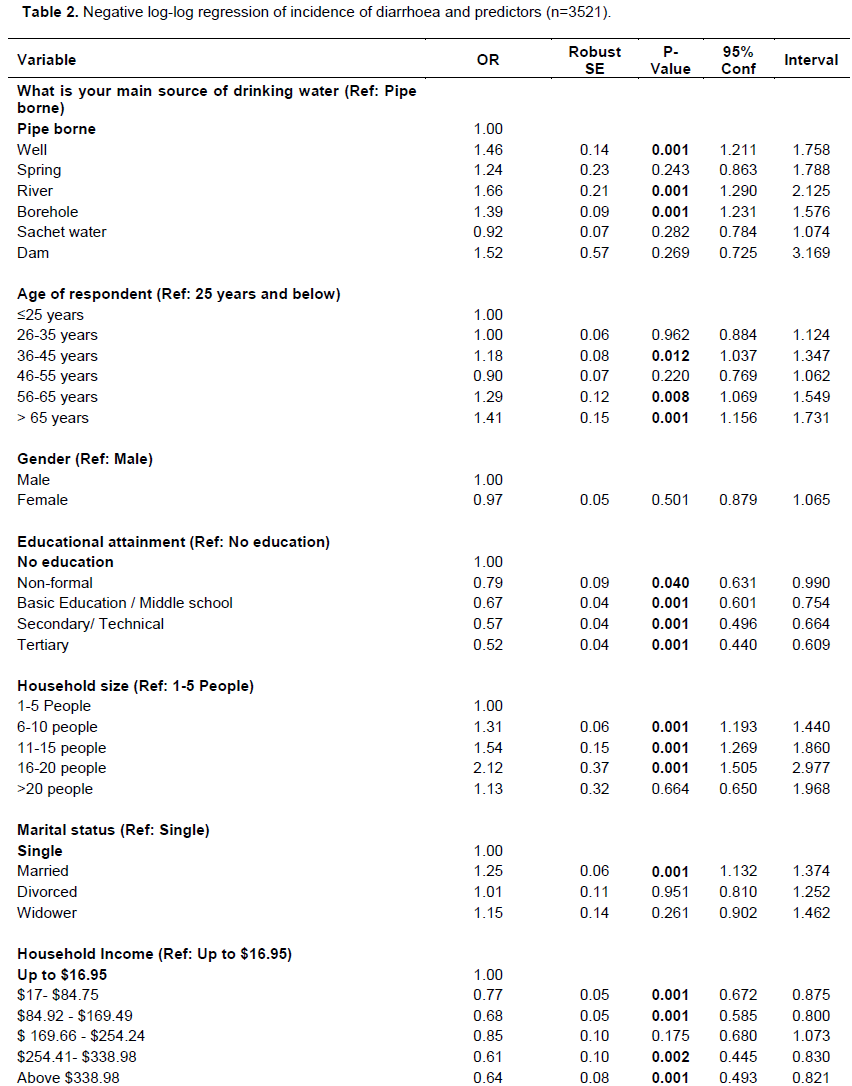
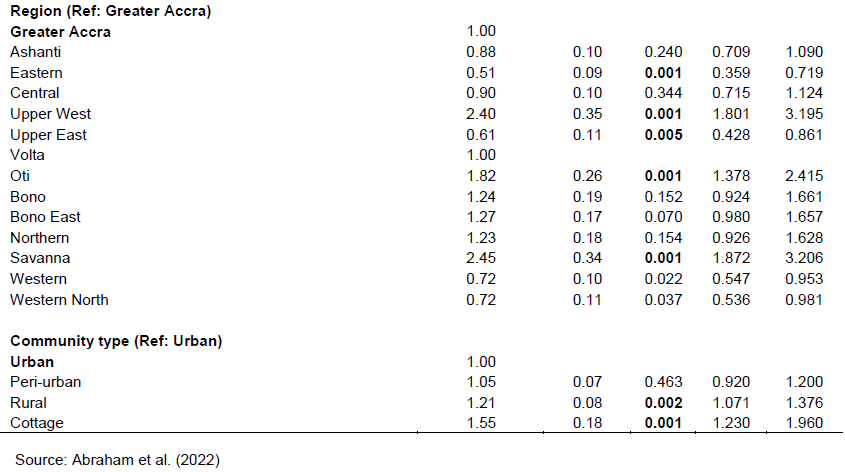
The results of the bivariate relationship between incidence of diarrhoea and predictors are presented in Table 2. The respondents, whose source of drinking water were well (OR=1.46, P<0.0001), river (OR=1.66, P<0.0001) and borehole (OR=1.39, P<0.0001) were more likely to have diarrhoea than those who depended on pipe borne water. Respondents, whose were aged 36-45 years (OR=1.18, P<0.0120), 56-65 years (OR=1.29, P<0.0080) and above 65 years (OR=1.41, P<0.0010) were more likely to have diarrhoea compared to those who were below 25 years. Furthermore, respondents with non-formal education (OR=0.79, P<0.0400), basic education/middle school (OR=0.67, P<0.0001), secondary/technical (OR=0.57, P<0.0001) and tertiary education (OR=0.52, P<0.0001) were less likely to have diarrhoea than those with no education. Respondents in households with 6-10 (OR=1.31, P<0.0001), 11-15 (OR=1.54, P<0.0001) and 16-20 (OR=2.20, P<0.0001) members were more likely to have diarrhoea than those in households with 1-5 members. Married respondents (OR=1.25, P<0.0001) were more likely to have diarrhoea compared to the single respondents. Household with income between $17 and 84.75 (OR=0.77, P<0.0001), $84.92 - 169.49 (OR=0.68, P<0.0001), $254.41- 338.98 (OR=0.61, P<0.0020) and above $338.98 (OR=0.64, P<0.0010) were less likely to have diarrhoea than those whose income were Up to 16.95. Households in Eastern (OR=0.51, P<0.0001), Upper East (OR=0.61, P<0.005) were less likely to have diarrhoea compared to those in Greater Accra Region. Households in Upper West (OR=2.40, P<0.0001), Oti (OR=1.81, P<0.0001) and Savanna (OR=2.45, P<0.0001) region were more likely to have diarrhoea than those in Greater Accra Region. Rural households (OR=1.21, P<0.0020) and cottage households (OR=1.55, P<0.0001) were more likely to have diarrhoea than urban households.
Multivariate analyses
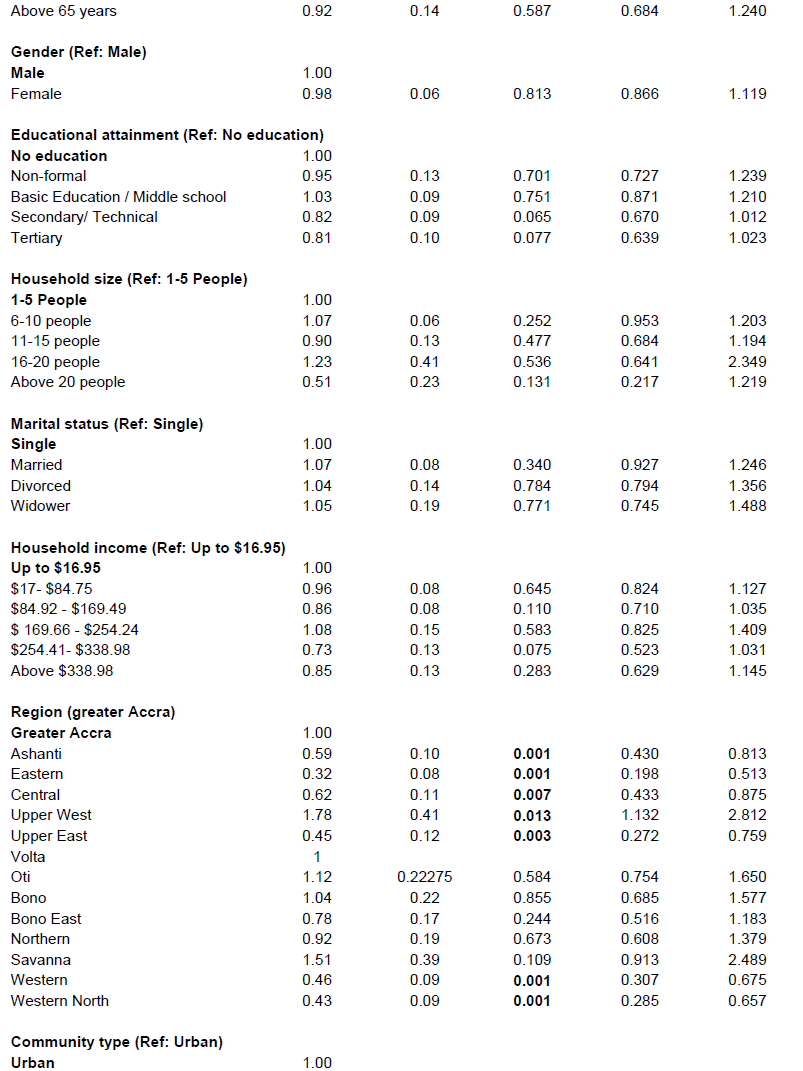
Table 3 provides the results of negative log-log multivariate regression model of the relationship between incidence of diarrhoea and predictors. In the model 1, respondents whose source of drinking water were well (OR=1.45, P<0.0001), river (OR=1.67, P<0.0001) and borehole (OR=1.36, P<0.0001) were more likely to have diarrhoea than those who relied on pipe borne water as their source of drinking water. Respondents, whose ages were between 56-65 years (OR=1.21, P<0.046) and above 65 years (OR=1.34, P<0.0050) were also more likely to have diarrhoea compared to those whose ages were below 25 years.
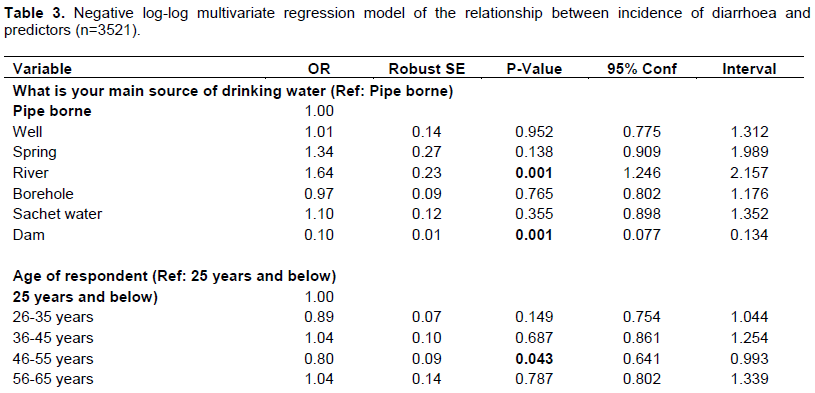

In the socio - cultural model, respondents whose source of drinking water were well (OR=1.52, P<0.040), and river (OR=1.60, P<0.0010) were more likely to have diarrhoea than those who relied on piped water as their source of drinking water. Respondents whose source of drinking water was dam (OR=0.12, P<0.0001) were less likely to have diarrhoea compared to those who depended on pipe borne water as their source of drinking water. Respondents who were aged 46-55 years (OR=0.79, P<0.0300) were less likely to have diarrhoea compared to those whose ages were below 25 years. Respondents with secondary/technical (OR=0.78, P<0.0130) and tertiary education (OR=0.78, P<0.0300) were less likely to have diarrhoea compared to those with no education. Respondents in households with 6 to 10 members (OR=1.13, P<0.0360) were more likely to have diarrhoea than those in households with 1 to 5 members. Households with income of $17- 84.75 (OR=0.84, P<0.0150), $84.92 - 169.49 (OR=0.76, P<0.0010), $169.66 - 254.24 (OR=0.69, P<0.0250) and above $338.98 (OR=0.74, P<0.0360) were less likely to have diarrhoea than those whose income were up to $16.95 (Table 3)
In the contextual model, respondents whose source of drinking water was river (OR=1.64, P<0.0001) were more likely to have diarrhoea than those who depend on pipe borne water as their source of drinking water. Respondents whose source of drinking water was dam (OR=0.10, P<0.0001) were less likely to have diarrhoea compared to those who relied on piped water as their source of drinking water. Respondents whose ages were between 46 and 55 years (OR=0.80, P<0.0430) were less likely to have diarrhoea compared to those whose ages were below 25 years. Households in Ashanti (OR=0.59, P<0.001), Eastern (OR=0.32, P<0.0001), Western (0.46, P<0.0001 and Western North (OR=0.43, P<0.0001) were less likely to have diarrhoea compared to those in Greater Accra Region. Households in Upper West (OR=1.78, P<0.013) region were more likely to have diarrhoea than those in Greater Accra Region (Table 3)
Microbial load analysis
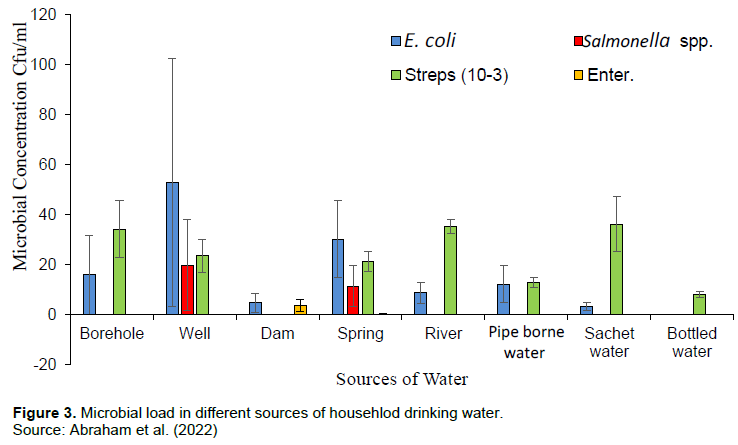
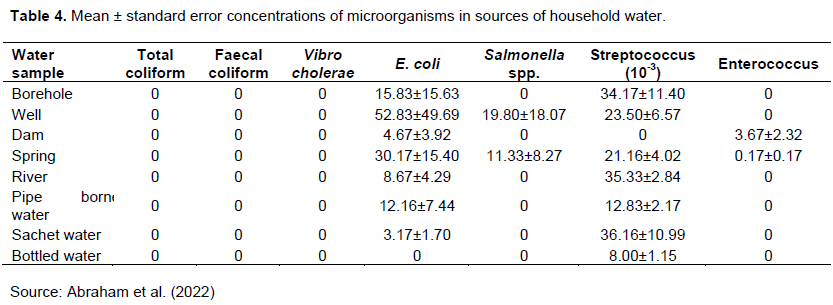
The results from the microbial load analysis showed that all the sources of household water analysed had no total coliform, feacal coloform and Vibro cholerae detected in the water sources. Escherichia coli was not detected in the bottled water but detected in all the other sources of household water figure 3. Salmonella spp. were not detected in borehole, dam, river, pipe borne, sachet and bottled water but present in well and spring sources of water. Streptococcus was detected in borehole, well, spring, river, pipe borne, sachet and bottled water sources but not in dam water sources figure 3. Enterococcus was also detected in the dam and spring water sources but not in the other sources of household water (Table 4).
DISCUSSION
This study examined the effect of source of drinking water on incidence of diarrhoea in Ghana. Drinking water source is known in literature to influence incidence of diarrhoea. Low incidence of diarrhoea is associated with improved water sources such as pipe borne water and unimproved water sources have a positive relationship with incidence of diarrhea (Godana and Mengiste, 2013; Boadi and Kuitunen, 2005).The findings of this study indicate that the odds of having diarrhoea is high in households that depend on river as their main source of drinking water compared to households that rely on pipe borne water. Tumwine et al. (2002) reported that the use of surface water as the main source of drinking water increases the likelihood of having diarrhoea. Boadi and Kuitunen (2005) also found that incidence of dirrhoea increases with the use of untreated water as the source of drinking water in the Northern Region of Ghana. These findings suggest that unimproved source of drinking water such as river is highly liable to feacal contamination, which is known to be the cause of diarrhoea. Conversely, our findings show less likelihood of having diarrhoea in households that rely on dam water as their main source of drinking water than those which depend on pipe borne water. Dam is classified as unimproved drinking water source by World Health Organization (WHO) and UNICEF (2017)and ideally should have had a higher odds of incidence of diarrhoea. This means that even though dam is unimproved water source and may contain some contaminants, they may be well preserved by the users making them less contaminated by diarrhoea causing pathogens such as feacal coliform. Besides, Osumanu (2007), posited that even though the sources of water for household drinking is important to incidence of diarrhoea, practices associated with fetching, storage and handling could contaminate even improved sources. Hence, as much as the source of drinking water is essential, storage and handling can also expose households to diseases (Kumi-Kyereme and Amo-Adjei, 2015).
The study showed that among all the compositional factors, age is the only factor that had association with incidence of diarrhoea. Respondents aged 46-55 years had lower odds of contracting diarrhoea compared to those with ages below 25 years. Root (2001) suggested that older people have greater awareness of disease hazards than younger people and this makes them more careful on disease causal factors. Older people too are more resourceful which puts them in a better position to afford improved services including source of drinking water. Although socio - economic status have reported in studies (Marmot, 2005; Marmot, 2017; Thiam et al., 2017)to have strong association with health, our findings indicated that the household income did not influence incidence of diarrhoea. Root (2001) explained that wealthy parents may be unable to reduce the risk of diarrhoea of their children owing to factors beyond their control such as polluted environment or absence of improved source of drinking water. The findings of this study also indicated that level of education does not influence incidence of diarrhoea. This is contrary to the findings of Boadi and Kuitunen(2005). It means irrespective of your educational level, when you live in a contaminated environment with lack of improved basic services such as improved drinking water source, you can do little to reduce your odds of having diarrhoea.
Region was found in this study to have a strong association with incidence of diarrhoea. This was indicated in both the bivariate and the multivariate analyses. Besides, in the univariate analysis it was the only variable that had strong association with incidence of diarrhoea. This is a major finding of this study indicating that in Ghana, the odds of having diarrhoea is highly dependent on the geographical region. This highlights the disparities among the fourteen regions in terms of access to improved drinking water sources. Upper West region had the higher odds of incidence of diarrhoea signifying their lower access to improved drinking water sources. The former three northern regions (Upper West, Upper East and Northern) are the poorest (Cooke,et al., 2016)and it has been reported that they have the lowest access to improved water and sanitation services (Molini and Paci, 2015). Reduction in poverty levels has been observed to accompany improvement in access to basic household services such as sanitation, electricity and clean drinking water in Ghana (Molini and Paci, 2015)which decreases incidence of diarrhoea. Community type was not found to affect incidence of diarrhoea in the multivariate analyses (Table 3). This can be attributed to the urban health penalty hypothesis (Kumi-Kyereme and Amo-Adjei, 2015; Thiam et al., 2017). This hypothesis suggests that the poor in the urban areas often reside in the marginalized areas known as slums which lack improved access to drinking water and sanitation. These conditions potentially increased the odds of having infectious diseases such as diarrhoea. The high rate of migration is expanding the slum communities in cities in Ghana; more urban dwellers are becoming vulnerable thereby equalizing the odds between urban and rural dwellers with regards to incidence of diarrhoea.
The microbial load analysis from the household water sources studied showed that there were no coliform (total and feacal) and V. cholerae in all the water samples which conform to the WHO standards for water quality. This makes the water sources excellent for domestic use. On the other hand, E. coli contamination was observed in all the sources of water used for the study except bottled water. The presence of E. coli in the other sources of water poses a public health risk (Chowdhury et al., 2015; Fagbamigbe et al., 2021). The sachet water, dam and rivers had mean concentrations of E. coli within the WHO acceptable range for potable water. However, the quality of such water needs to be monitored regularly so that, the level of E. coli would not increase. The spring, borehole and pipe borne water contained levels of microbial loads that make them unacceptable for consumption/use according to WHO standards for domestic use. Well water in this study was polluted because it contained high levels of microbial load. This supports the report that polluted drinking water, poor sanitation, poor hygiene practices and bacterial contamination causes diarrhoea in households (Boadi and Kuitunen, 2005; Prüss?Ustün et al., 2014; Gwimbi et al., 2019). This implies that, with the exception of bottled water all the household water sources are potential sources of diarrhoea disease in the household. The presence of Streptococcus in almost all the household water studied indicates the potential risk of diarrhoea to the consumers of such water.
CONCLUSION
The study assessed how compositional and contextual factors interact with source of drinking water to influence incidence of diarrhoea in Ghanaian adults. The findings of the study indicated that source of drinking water and geospatial disparities (region) are the two main factors that affect incidence of diarrhoea in Ghana. This implies that efforts by individuals or households to reduce incidence of diarrhoea may not yield the expected results because the underlying drivers cannot be controlled by the households alone. Based on the findings of the study, the responsibility rather lies on the government and its agencies who are tasked to provide basic social amenities such as improved source of drinking water. Closing the gap in terms of access to improved drinking water and sanitation facilities at the regional level will have direct impact on incidence of diarrhoea in Ghana.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Asamoah A, Ameme DK, Sackey SO, Nyarko KM, Afari EA (2016). Diarrhoea morbidity patterns in Central Region of Ghana. The Pan African Medical Journal 25(Suppl. 1):17. |
|
|
Boadi KO, Kuitunen M (2005). Childhood diarrhoeal morbidity in the Accra Metropolitan Area, Ghana: socio-economic, environmental and behavioral risk determinants. Journal of Health & Population in Developing Countries, (January) 1-13. |
|
|
Chowdhury F, Khan IA, Patel S, Siddiq AU, Saha NC, Khan AI, Saha A, Cravioto A, Clemens J, Qadri F, Ali M. (2015) Diarrheal illness and healthcare seeking behavior among a population at high risk for diarrhea in Dhaka, Bangladesh. PLoS One 10(6):e0130105. |
|
|
Collins J, Ward BM, Snow P, Kippen S, Judd F (2017). Compositional, contextual, and collective community factors in mental health and well-being in Australian rural communities. Qualitative health research 27(5):677-687. |
|
|
Cooke E, Hague S, McKay A (2016). The Ghana Poverty and Inequality Report - 2016. Unicef. |
|
|
Fagbamigbe AF, Uthman AO, Ibisomi L (2021). Hierarchical disentanglement of contextual from compositional risk factors of diarrhoea among under-five children in low-and middle-income countries. Scientific Reports 11(1):1-17. |
|
|
Ghana Statistical Service (2015). Ghana poverty mapping report. |
|
|
Gwimbi P, George M, Ramphalile M (2019). Bacterial contamination of drinking water sources in rural villages of Mohale Basin, Lesotho: exposures through neighbourhood sanitation and hygiene practices. Environmental health and preventive medicine 24(1):1-7 |
|
|
Kumi-Kyereme A, Amo-Adjei J (2015). Household wealth, residential status and the incidence of diarrhoea among children under-five years in Ghana. Journal of Epidemiology and Global Health 6(3)131-140. |
|
|
Marmot M (2005). Social determinants of health inequalities. Lancet 365(9464):1099-1104. |
|
|
Marmot M. (2017). Social justice, epidemiology and health inequalities. European journal of epidemiology 32(7):537-546. |
|
|
Molini V, Paci P (2015). Poverty Reduction in Ghana Progress and Challenges. |
|
|
Osumanu IK (2007). Household environmental and behavioural determinants of childhood diarrhoea morbidity in the Tamale Metropolitan Area (TMA), Ghana. Geografisk Tidsskrift--Danish Journal of Geography 107(1):59-68. |
|
|
Thomas RK (2000). The demography of health and health care. Springer Science & Business Media. |
|
|
Prüss?Ustün A, Bartram J, Clasen T, Colford Jr JM, Cumming O, Curtis V, Cairncross S. (2014). Burden of disease from inadequate water, sanitation and hygiene in low?and middle?income settings: a retrospective analysis of data from 145 countries. Tropical Medicine & International Health 19(8):894-905. |
|
|
Root GPM (2001). Childhood Diarrhoea in Rural Zimbabwe. Journal of Health, Population and Nutrition 1919(22):73-8273. |
|
|
Saboksa NE, Gari SR, Hailu AB, Mengistie Alemu B (2021). Childhood Malnutrition and the Association with Diarrhea, Water supply, Sanitation, and Hygiene Practices in Kersa and Omo Nada Districts of Jimma Zone, Ethiopia. Environmental Health Insights 15 |
|
|
Thiam S, Diène AN, Fuhrimann S, Winkler MS, Sy I, Ndione JA, Schindler C, Vounatsou P, Utzinger J, Faye O, Cissé G (2017). Prevalence of diarrhoea and risk factors among children under five years old in Mbour, Senegal: A cross-sectional study. Infectious Diseases of Poverty 6(1):1-12. |
|
|
Walker CL, Rudan I, Liu L, Nair H, Theodoratou E, Bhutta ZA, O'Brien KL, Campbell H, Black RE (2013). Global burden of childhood pneumonia and diarrhoea The Lancet 381(9875):1405-1416. |
|
|
Wolf J, Prüss?Ustün A, Cumming O, Bartram J, Bonjour S, Cairncross S, Clasen T, ColfordJr JM, Curtis V, De France J, Fewtrell L (2014). Systematic review: Assessing the impact of drinking water and sanitation on diarrhoeal disease in low- and middle-income settings: systematic review and meta-regression. Tropical Medicine & International Health 19(8):928-942. |
|
|
World Health Organization (WHO) (2008). Safer water, better health: Costs, benefits and sustainability of interventions to protect and promote health. Geneva: World Health Organization. |
|
|
World Health Organization (WHO) (2017). Diarrhoeal disease. |
|
|
World Health Organization. (2004). Health & Environment: Tools for Effective Decision-Making: Review of Initial Findings. |
|
|
World Health Organization (WHO) and UNICEF (2017). Progress on Drinking Water, Sanitation and Hygiene: 2017 Update and SDG Baselines. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


