Case Report

ABSTRACT
The elimination of HIV-AIDS by 2030 is a challenging target for a country such as the D.R. Congo, since currently fewer than 50% of persons living with HIV (PLWH) are under antiretroviral treatment (ART) and have a viral suppression. There also a high rate of death of PLWH in D.R. Congo. Accessible, affordable and sustainable immunotherapy, coupled with ART, can provide a substantial support to eliminating HIV. The purpose of this paper is to describe the measured clinical and biological profiles over a 4-year period of treatment with the immunomodulator 6,6’-dithiodinicotinic acid (CPDS), of a patient who was only 10-months old at the start of treatment. The patient was part of a larger two-year clinical trial of CPDS on HIV-AIDS. This study found that despite his advanced clinical HIV stage (being born to parents with terminal HIV), the patient maintained his weight and lymphocyte counts, and did not experienced any severe HIV-AIDS-related illness during the study period. This suggests a beneficial or protective effect of CPDS treatment. The patient shifted to ARV at 5-years old and is now 17-years old, and under first-line ART. The study concludes that survival of this child could likely be attributed to CPDS. We therefore recommend exploring further the simultaneous use of ART and CPDS immunotherapy for a greater clinical and biological benefit of PLWH. We also recommend further study into the mechanism of action of the compound.
Key words: HIV-AIDS treatment, immunomodulation, 6,6’-dithiodinicotinic acid.
INTRODUCTION
The clinical management of HIV/AIDS by standard antiretroviral therapy (ART) using the combination of antiretroviral (ARV) drugs alone cannot eradicate HIV reservoirs (Williams et al., 2011; Zhang and Crumpacker, 2013; Harrer et al., 1996). The interest of immunotherapy in HIV treatment is theoretically well established (Nishimura et al., 2017; Martrus and Altfeld, 2016; Bahr et al., 2003). Some studies showed the practical benefit of use of immunotherapy in treating HIV (Gontran M, et al, 2009; Ndarabu et al., 2017). With IM28, only patients who received it alone or in combination with HAART showed in particular an increase in the levels of CD4 lymphocytes as well as significant reduction of viral load.
In a recent article, we showed that the use of CPDS alone (without ARV) resulted in equivalent effectiveness of ARV treatment in increasing mean body weight and mean CD4 during the first six months of treatment. Weight gain and CD4 increase indicated a recovering immune system. In addition, the study found no difference in mortality rates during the two years of follow-up between the two groups (Ndarabu et al., 2017). CPDS is a biologically active agent (Grassetti, 1986; Grassetti, 1970) that has pleiotropic anti-cancer and anti-metastatic properties, including functionality as a potent immunomodulator that significantly increases the number and activity of NK cells and increases the lymphoproliferation of T lymphocytes. It is devoid of identified side effects and does not have teratogenic or mutagenic effects (Grassetti and Moro, 2013).
In this case report, the focus is on one of the 34 participants, given the particular fact that he was only 10 months old at the beginning of the trial, in 2002 (Ndarabu et al., 2017). He continued to take CPDS alone for 2 years after the completion of the trial before he shifted to ARV treatment at age 5 (a total of 4 years under CPDS-only treatment). He is now 17-years old and regularly followed at Monkole Hospital under ART. The objective of this case report is to highlight the clinical and biological profile of this participant over the 4-year period under CPDS treatment. The clinical parameters considered are: weight, illness episodes or occurrence; the main biological parameter consists of lymphocytic counts (Grassetti and Moro, 2012).
CASE REPORT
The patient was born in December 2001 to HIV positive parents. He was initially admitted at Monkole Hospital in Kinshasa, D.R. Congo at 10-months of age, in October 2002. At that time he was at Stage 2 per the World Health Organization (WHO) Clinical Staging of 1990 criteria, and Stage B2 per the US Centers for Disease Control and Prevention (CDC) pediatrics HIV classification (WHO, 1990; CDC, 1994). There were no medical details about circumstances of birth or the past medical history of the mother and the child. The patient’s birth weight was unknown. He was the sixth out of seven siblings. The last-born was premature and died at 6 days after birth. The father died few months later from HIV-AIDS. The mother was previously followed for HIV-AIDS
in another medical facility in Kinshasa, without ART. At that time, access to ARV was not universal and required a significant expense that the mother could not afford. The Prevention of Mother to Child Transmission of HIV (PMTCT) policy then in force advocated only a single-dose of Nevirapine (NVP) for the exposed newborn and NVP single-dose/Tritherapy, depending on the mother’s eligibility to receive ART (CD4 < 350/µl or WHO clinical stage ≥ 3). Breastfeeding was the rule. When the mother was 36-years old, she started her medical visits at Monkole Hospital (in September, 2002). She was at stage 4 of WHO HIV clinical staging (WHO, 1990), with a severe wasting syndrome, weighing only 38 Kg and displaying low values for counts of lymphocytes: CD4 at 145/µl, CD8 at 392/µl and CD4/CD8 at 0.37. This advanced clinical stage resulted in her death 7 months later, in April 2003. The patient was enrolled in the study following the settled inclusion criteria reported in the previous study with the approval of the Ethical Committee, assigned reference N/Réf: 002/CEFA-MONKOLE/CE/2002 as noted in (Ndarabu et al., 2017), and also with the consent of parents and the research team, considering the expected benefit of the intervention respect to any potential risk which in this case was very unlikely. At the beginning of the treatment, the clinical and biological parameters of the patient were as follows: 8 Kg of body weight at 10-months old, T° 36.8°C. WBC 11,500 mm3 (N27L69E2M2), HCT 21%. Lymphocytes count (absolute number/µl): CD4 787; CD3 3021; CD8 >2000; CD4/CD8: 0.39. Viral load was not available. The immunomodulator used was CPDS (12 mg/Kg oral capsule twice a day).
Description of clinical and biological parameters
The patient’s clinical and biological parameters of weight, ailment episodes, psychomotor development, CD4 count, and clinical evolution were monitored as part of this study. The results are summarized below.
Weight
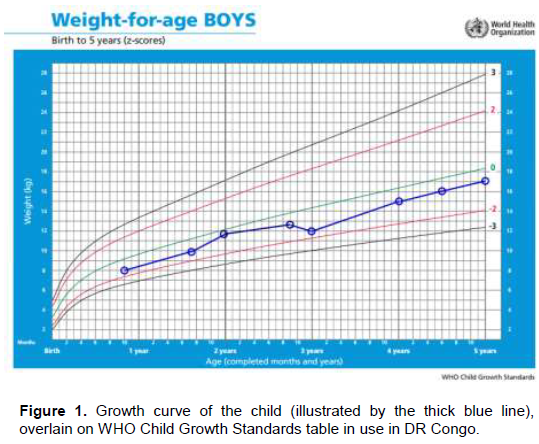
As per the specified parameters in well-recognized tables for growth (Figure 1) from the World Health Organization (WHO) using the Z-scores of weight-for-age for boys from birth to 5-years old, we recorded the weight of the patient at different medical visits. The weight curve from the beginning to the end of CPDS treatment remained between 0 and -2 Standard Deviation. A slight drop in weight was noticed at 36-months of age.
Ailment episodes
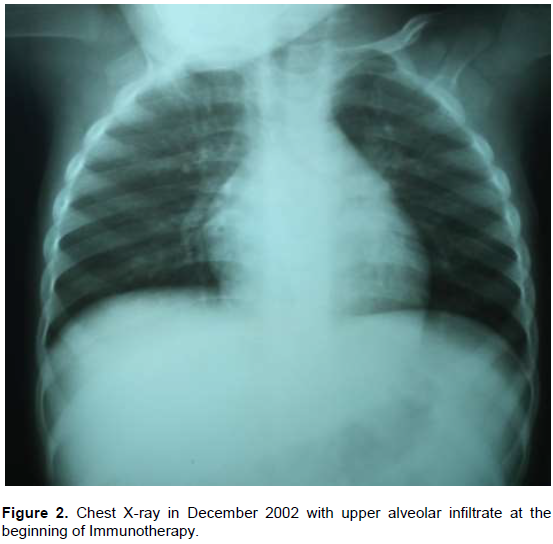
Table 1 shows the different clinical visits of the patient under CPDS treatment, along with the illnesses identified and biological findings. Leukocyte count is in absolute number. The relevant illnesses were made of bronchopneumonia (Figure 2), rhinitis, enteritis, prurigo and shingles. No AIDS-related ailments were noted.
Psychomotor development
The child was awake according to his age throughout CPDS intake. The evidence for spoken language occurred around 12 months of age with a slight stuttering. Walking also occurred at this time.
CD4 count
Numbers of CD4, CD3 and CD8 lymphocytes are expressed by microliter on Table 1. With respect to lymphocytic count, CD4 values remained at a mild (moderate) suppression level at less than 12 months of age, and also from 12 months up to 5-years old, suggesting the maintenance of immune system function under CPDS treatment.
Clinical evolution and comments
The death of the patient’s father and mother from HIV-AIDS-related symptoms occurred when he was 13 and 16-months old, respectively, suggesting that they had been already in advanced stages of AIDS at the time he was born. This suggests the possibility that he was potentially infected in utero. At 10 months of age, when we started following the patient, the hospital did not have access to a biomolecular tool for HIV testing, and the diagnosis of HIV was made according to the National Policy in force (Minister of Health DRC, 2004), using an algorithm combining the risk factor (HIV exposed infant), the clinical pattern (small for age) and antibody testing (positive Elisa testing). The diagnosis was later confirmed at 18-months old with the concordance of three positive rapid test of HIV: DetermineTM; Double-CheckTMand UnigoldTM. In this context, we could therefore not definitively establish whether the maternal-to-child transmission of HIV occurred between the pre-, peri- or post-natal period.
DISCUSSION
As the patient was at stage B2 of CDC pediatric HIV classification at baseline, this suggests a certain level of disease advancement (CDC, 1994). Throughout CPDS treatment, the child did not experience any severe ailment episodes that could indicate a Stage 3 WHO pediatrics classification. Because of low weight, the child was considered at Stage 2 (WHO, 1990). The steadiness of the weight curve suggests a certain benefit from CPDS despite the nutritional insecurity generated by the advanced illness of the mother and early death of the father. The child’s weight slightly dropped at 36 months-old due to a shingles episode but recovered immediately to its previous upward trend as shown in the weight curve (Figure 1).
Evidence for episodes of fever was very scarce under CPDS treatment. Two fever episodes were recorded, at 2 and 8 months of follow-up, respectively, due to non-life-threatening bronchopneumonia and malaria episodes. The patient was not under Cotrimoxazole prophylaxis. In addition to the bronchopneumonia with fever, the only other observed episode of respiratory tract infection appeared to be from a flu syndrome as reported in Table 1. No lymph node enlargement was observed during the trial. The two diarrhea episodes observed were irrelevant, one of them related to diet. No tuberculosis, meningoencephalitis, or oral thrush episodes occurred (Yotebieng et al., 2010).
Hemoglobin was low particularly at the beginning of the follow up. At two months of CPDS treatment, hemoglobin was 7.5 g/dl. The values available up to 22 months of follow-up treatment were all below 10 g/dl. However, at any time the patient could require blood replacement. This multifactorial anemia was likely influenced by the poor nutritional status of the patient. Being a child in growth, the level of CD4 remained steady throughout CPDS uptake and did not drop (Weiser et al., 2011; Edmonds et al., 2012).
The child did not display an increase of weight during the 3-6 months interval in course of the therapy, as observed in the mean weight of the group in a previous study (Ndarabu et al., 2017); however, the weight did not drop into the red area of growth curve during the four years under CPDS treatment, which is up to 60-months old. This low weight for age in this case can be attributed to a deficient nutritional intake. During breastfeeding, the mother was already in cachexia with concordant, very advanced HIV-AIDS. Moreover, the socio-economic level of the housing where the child grew was one of the low-income. The data therefore suggests a protective effect of CPDS in the maintenance of weight of this child (Grassetti and Moro, 2012). The illness episodes he displayed were mainly made by rhinitis, enteritis, shingles, prurigo and mild bronchitis. The patient shifted to ART in 2006, when it became universally accessible. At the time of preparation of this paper, at age 17, he is still in first-line therapy made of 1 NNRTI + 2 NRTI, weighing 62 Kg at his last medical visit (September, 2018), with a height of 1.67 m as recorded in his medical history.
Interpretation of CPDS treatment results
Given the fact that, in Africa, 52% of untreated children born with HIV had died by age 2 (Newell et al., 2004), our interpretation of the studies described in this paper is that the survival of this child could likely be attributed to CPDS. This is consistent with the findings in our earlier study reviewing the multi-patient CPDS trial, which found the CPDS-treated group death rate at 23.5% compared to 23.3% of the ARV-treated group, for a 24-month follow-up period (Ndarabu et al., 2017). The rate of death among PLWH in D.R. Congo is still high despite availability of ARV, displaying a value of 24.1% (Catwaba et al., 2017). This has put the D.R. Congo at risk of missing the year 2020 90-90-90 targets (90% of all PLWH will know their HIV status; 90% of all PLWH will receive antiretroviral therapy and 90% of all PLWH receiving antiretroviral therapy will have viral suppression). Patients in the D.R. Congo display, for the two last target parameters, modest values of 42 and 31%, respectively (UNAIDS, 2017). Our clinical use of CPDS suggests that treatment with the compound could contribute substantially towards achieving the 2030 AIDS elimination target (UNAIDS, 2016) by adding immuno-modulation to the viral suppression efforts (Martrus and Altfeld, 2016).
CONCLUSION
The steady clinical and biological profile of this child during the four years of CPDS treatment suggests a beneficial impact for this immunotherapeutic agent even in a very young patient. Thus, we retain high interest of exploring further the simultaneous use of ART and CPDS
immunotherapy for a greater clinical and biological benefit of PLWH. In light of previous findings that CPDS can activate NK cells in standard models of NK cell-mediated cytotoxicity, the significant evidence for the role of activated NK cells for treating various infectious and malignant diseases, as presented in multiple reviews (Tomin et al., 2016; Goldfarb and Herberman, 1982), and increasingly specific evidence for a role for NK cell-mediated immunotherapy for control of AIDS/HIV (Garrido et al., 2018; Mavillo et al., 2005; Mikulak et al., 2017; Scully and Alter, 2016), the authors believe that additional investigation of the potential beneficial effects of CPDS immunotherapy on treatment of AIDS/HIV is justified.
Further investigation of CPDS also is warranted because this immunomodulator has a very low cost of goods and manufacture that would allow it to be pragmatically available to under-served and economically disenfranchised patient populations including those in the D.R. Congo. This is in stark contrast to currently available drugs that are often financially out of reach to patients, resulting in unmet medical needs. In sum, the data and economics both argue for further investigation of CPDS for its role as an immuno-modulator that could play a role in augmenting treatment of HIV/AIDS. Towards that end, the potential immunologic, mechanism of CPDS in regulating NK cell activities are undergoing more thorough investigation. This will be the subject of an additional communication.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Bahr GM, Tribonnière DLX, Darcissac E, Ajana F, Bocket L, Sissoko D, Yazdanpanah Y, Dewfulf J, Amiel C, Mouton Y (2003). Clinical and immunological effects of a 6-week immunotherapy cycle with murabutide in HIV-1 patients with unsuccessful long-term antiretroviral treatment. Journal of Antimicrobial Chemotherapy 51:1377-1388. |
|
|
Catwaba KJ, Mutate B, Kashia D, Wembonyama S (2017). Causes of deaths of HIV infected patients at the HIV/AIDS Center of Excellence of the University of Lubumbashi in Lubumbashi, Democratic Republic of Congo. Journal of Infectious Diseases and Medicine 2:3. |
|
|
Centers for Disease Control and Prevention (1994). The Morbidity and Mortality Weekly Report. Revised classification system for human immunodeficiency virus infection in children less than 13 years of age 43(12):1-10. |
|
|
Edmonds A, Yotebieng M, Lusiama J and Behets F (2012). Quantification of CD4 Responses to Combined Antiretroviral Therapy Over 5 Years Among HIV-Infected Children in Kinshasa, Democratic Republic of Congo. Journal of Acquired Immune Deficiency Syndromes 61(1):90-98. |
|
|
Garrido C, Abad-Fernandez M, Tuyishime M, Pollara JJ, Ferrari G, Soriano-Sarabia N, Margolis DM. (2018). Interleukin-15-stimulated natural killer cells clear HIV-1-infected cells following latency reversal ex vivo. Journal of Virology 92:00235 |
|
|
Goldfarb RH, Herberman RB (1982). Characteristics of natural killer cells and possible mechanisms for their cytotoxic activity. Advances in Inflammation Research 4:45 72. |
|
|
Gontran M, Jerome LT, Yvonne AM, Mavoungou-Poaty V, Elie M, Brice O, Donatien M (2009). Effects of IM28 on HIV-1 and metabolic disorders-induced highly active antiretroviral therapy in Gabonese patients. Journal of Antivirals and Antiretrovirals 1:076-081. |
|
|
Grassetti DR, Moro C (2013). European patent specification. Method of immunomodulation using thione-forming disulfides EP1383499B1. |
|
|
Grassetti DR, Moro C (2012). Method of immunomodulation using thione-forming disulfides. United States Patent No.US (8)163:776 BS |
|
|
Grassetti DR (1970). Effect of 6,6-ditiodinicotinic acid on the dissemination of Ehrlich ascites tumor. Nature 5258(228):282-83. |
|
|
Grassetti DR (1986). The antimetastatic and tumor growth retarding effects of sulfur containing analogs of nicotinamide. Cancer Letters 31:187-195. |
|
|
Harrer T, Harrer E, Kalams SA, Elbeik T, Staprans SI, Feinberg MB, Cao Y, Ho DD, Yilma T, Caliendo AM, Johnson RP, Buchbinder SP, Walker BD (1996). Strong cytotoxic T cell and weak neutralizing antibody responses in a subset of persons with stable no progressing HIV type 1 infection. AIDS research and humans retroviruses 12(7):585-592. |
|
|
Martrus G, Altfeld M (2016). Immunological strategies to target HIV persistence. Current Opinion in HIV-AIDS 11(4):402-408. |
|
|
Mavilio D, Lombardo G, Benjamin J, Kim D, Follman D, Marcenaro E, O'Shea MA, Kinter A, Kovacs C, Moretta A, Fauci AS (2005). Characterization of CD56-/CD16+ natural killer (NK) cells: a highly dysfunctional NK subset expanded in HIV-infected vermeil individuals. Proceedings of the National Academy of Sciences USA. 102(8):2886-2891. |
|
|
Mikulak J, Oriolo F, Zaghi E, Di Vito C, Mavilio D (2017). Natural Killer cells in HIV-1 infection and therapy. AIDS 31(17):2317-2330 |
|
|
Minister of Health, DRC/Programme National de lutte contre le SIDA (PNLS) (2004). Guide pratique des prestataires de prévention de la transmission du VIH de la mère à l'enfant, Ministère de la Santé Publique, DRC, Kinshasa, DRC. |
|
|
Ndarabu A, Mbombo W, Mulumba P, Mbuyi D, Tshilolo L (2017). Trial of immunotherapy in HIV patients: our experience with the immuno-modulator dithiodinicotinic Acid (CPDS) in 34 Congolese patients. The Global Journal of Medical Research 17:2. |
|
|
Newell ML, Coovadia H, Cortina-Borja M, Rollins N, Gaillard P, Dabis F (2004). Mortality of infected and uninfected infants born to HIV-infected mothers in Africa: A pooled analysis. The Lancet 364(9441):1236-1243. |
|
|
Nishimura Y, Gautam R, Chun TW, Sadiadpour R, Foulds KE, Shingai M, Gazumyan A, Gollianin J, Donaldson M, Donau OK, Plishka RJ, Buckler-White A, Seaman MS, Lifson JD, Koup RA, Fauci AS, Nussenzweig MC, Martin MA (2017), Early antibody therapy can induce long lasting immunity to shiv. Nature 543(7646):559-563 |
|
|
Scully E, Alter G (2016). NK cells in HIV disease. Current HIV/AIDS Reports 13(2):85-94. |
|
|
Tomin K, Goldfarb RH, Albertsson P (2016). In Vitro Assessment of Human Natural Killer Cell Migration and invasion. : Natural Killer Cells: Methods and Protocols, Methods in Molecular Biology 1441:65-74. |
|
|
United Nations Programme on HIV and AIDS (UNAIDS) (2017). Data |
|
|
United Nations Programme on HIV and AIDS (UNAIDS) (2016). Fast Track commitments to end AIDS by 2030 |
|
|
Weiser SD, Palar K, Frongillo EA, Tsai AC, Kumbakumba E, dePee S, Hunt PW, Ragland K, Martin J, Bangsberg DR (2013). Longitudinal assessment of associations between food insecurity, antiretroviral adherence and HIV treatment outcomes in rural Uganda. AIDS 28(1):115-120. |
|
|
Williams BG, Lima V, Gouws E (2011). Modeling the impact of Antiretroviral Therapy on the Epidemic of HIV. Current HIV Research 9(6):367-382. |
|
|
World Health Organization (1990). Interim proposal for a WHO Staging System for HIV infection and disease. Weekly Epidemiological Record 65(29). |
|
|
Yotebieng M, Rie AV, Luisiama J, Behets F (2010). Survival, clinical, immunological and hematological outcomes of antiretroviral therapy among HIV-infected children attending a public clinic in Kinshasa, Democratic Republic of Congo. International Journal of Infectious Diseases 14(1). |
|
|
Zhang J, Crumpacker C (2013). Eradication of HIV and cure of AIDS, Now and How? Frontiers in Immunology 4:337. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


