ABSTRACT
The aim of this study was to determine the magnitude of HIV/AIDS related stigmatization, discrimination and coping strategies among people living with HIV/AIDS (PLHIV) at University College Hospital Ibadan. The study adopted a descriptive cross-sectional study design carried out among 700 PLHIV selected using a systematic random sampling technique from May to June 2010. A validated pretested questionnaire was used to collect the data which was analysed using SPSS version 16. The mean age of the respondents was 40.0 ± 9.40 years and more were females (474, 67.70%). About 212 (30.30%) have experienced stigmatization with verbal insult (138, 65.10%), subjection to ridicule (134, 63.20%) and avoidance by friends (89, 42.0%) being the most reported forms of induced stigmatization/discrimination. In addition, there was no significant relationship of experiencing stigmatization/discrimination by gender (P=0.097). However, more females experienced physical assault than male. Strategies adopted by respondents in coping with stigmatization and discrimination were unmoved 376 (53.70%), prayer 321 (45.90%) and ignoring the person 281 (40.10%). The study reported prevalence of various forms of stigmatization and discrimination against PLHIV. Therefore, there is need for more awareness campaign in communities on the dangers of HIV-related stigmatization and discrimination on the health of PLHIV.
Key words: Social discrimination, perception, stigmatization, social support, HIV/AIDS.
The Human Immunodeficiency Virus (HIV) infection and the Acquired Immune Deficiency Syndrome (AIDS) remain a disease of public health concern in Nigeria. This is because Nigeria is the most populous country in sub-Saharan Africa and is one of the countries highly affected by the HIV/AIDS scourge (UNAIDS, 2014; Dahlui et al., 2015). The estimated number of people living with HIV (PLHIV) as at 2015 is 3.4 million people giving a prevalence of 3.2% among the adult population (UNAIDS, 2015). Since the first case of AIDS in Nigeria was reported in 1986, Nigeria adopted antenatal care sentinel surveillance as the system for monitoring the epidemic, in line with WHO guidelines (UNAIDS, 2015). The first sentinel survey gave a prevalence of 1.80%; thereafter, it increased to 5.4% in 1999 and peaked at 5.8% in 2001.
The prevalence declined to 4.4% in 2005, 4.1% in 2010 and 3.0% in 2014 (UNAIDS, 2015). Furthermore, in Oyo State, the prevalence of HIV, based on the result of the national sero-surveillance studies conducted in 1992 and 2004, were 0.1 and 4.2%, respectively (FMOH, 2005). It was also reported that there was no town or village that had not reported cases of HIV and AIDS and about 85% of the infections were reported to have been contracted through unprotected heterosexual intercourse (FMOH, 2005). The international community embraced the goal of universal access to HIV prevention, treatment, care and support in 2005. This has led to universal access to diagnosis, treatment and care for PLHIV (Monjok et al., 2009; UNGASS, 2005; World Health Organization, 2006).
The three documented phase of the AIDS epidemic in most countries include “epidemic of HIV infection”, “epidemic of AIDS” and stigmatisation. The third phase is very challenging as it is characterized by discrimination, blame and denial (Mann, 1987). Nigeria appears to be in between the full AIDS epidemic phase and the stigma and discrimination phase. Experiencing the weight of AIDS epidemic and also seeing a lot of discrimination of PLHIV. HIV and AIDS-related stigma and discriminatory conduct provide opportunities for the spread of the infection (FMOH, 2002). This is because to avoid the unpleasing consequences of revealing their status, stigmatized persons may conceal their sero-positivity from others most especially their sexual partners thereby leading to the spread of the infection (Tsai et al., 2013; Pennebaker, 1989; Katz et al., 2013). This practice undermines prevention efforts and support and also increases the impact of the infection on individuals, families, communities and nations (Population Council Horizons, 2002).
Furthermore, the stigma and discrimination attached to being diagnosed with HIV/AIDS is far bigger and considerably different from being diagnosed with more prevalent non-communicable diseases like diabetes, cancer and hypertension. This may be due to the fact that HIV is primarily transmitted through sexual intercourse and people sometimes erroneously link HIV infection with sexual promiscuity. Self-stigmatisation which can manifest as self-blaming and shame can lead to psychological consequences such as depression, withdrawal and feelings of worthlessness (UNAIDS, 2002). The effect of stigmatizing PLHIV and self-stigmatization by PLHIV all lead to social exclusion. This study therefore focuses on exploration of stigma and discrimination from the perspective of the stigmatized and their coping strategies among PLHIV at Anti-Retroviral Viral clinic, University College Hospital Ibadan, Nigeria.
Study design
The study was a descriptive cross sectional study of persons living with HIV and AIDS at the President Emergency Plan for AIDS Relief (PEPFAR), University College Hospital (UCH).
Study area
University College Hospital Ibadan is one of the 15 Federal University Teaching Hospitals in Nigeria. The hospital is located in Ibadan, the largest city in West Africa. It is established to serve as a teaching hospital for medical and allied professionals. The hospital consists of various clinics, including PEPFAR; the PEPFAR clinic UCH is jointly managed by the Government of the United State of America, the Nigerian government in collaboration with UCH, Ibadan and Harvard School of Public Health.
Study population
Adult persons attending PEPFAR clinic constituted the study population. They were persons living with HIV and AIDS. The clinic as at the time of the study had approximately 11000 patients of different socio-demographic characteristic; approximately 35 new patients were admitted per day.
Sample size determination
The formula for single proportion was used in calculating the sample size with 50% used as the proportion and 99% as the confidence interval.
N = z2 × p (1 - p) / d2
N = 2.5782 × 0.5 (1 - 0.5) / 0.052 = 665
The calculated sample size of 665 was increased to 700 so as to address possible cases of attrition or incomplete responses. Thus, the study recruited 700 participants out of 11,000 in the PEPFAR register as at September, 2009.
Sampling procedure
A sampling interval of 16 was calculated, thus the first respondent was randomly selected; thereafter, every 16th patient on the PEPFAR register was selected for the study. Peradventure any of the 16th person decline to participate, then the 17th person was selected. Thus, 420 females and 280 males were selected for the study in all HIV/AIDS clinic days between the month of May and June 2010.
Instruments for data collection
The instrument for data collection was a semi-structured validated
questionnaire divided into five sections (sections A to E). Section A focused on respondents’ demographic characteristics; section B was on experiences relating to HIV-related stigma and discrimination. Section C was used to assess respondents’ attitude, consequences/effects of HIV-related stigma and discrimination; while section D explored respondents’ past and prevailing coping strategies to HIV-related stigma and discrimination experiences.
Method of data collection
On each day of data collection, the questionnaire was administered to the respondent after adequate explanation of the purpose of the study. The interview was either interviewer-administered or self-administered depending on the respondents’ level of education. The questionnaires were retrieved back from each respondent immediately after completion and reviewed for incompleteness and necessary correction.
Validity and reliability
The questionnaire was reviewed in-house among experts in health promotion and education, medical sociologists, and a medical statistician for face, construct and content validity. Similarly, to improve the reliability of the instrument, the questionnaire was pre-tested among 70 PLHIV receiving care at Saint Mary Catholic Hospital Eleta, Ibadan. The Cronbach Alpha Correlation Co-efficient was used to determine the reliability of the instrument.
Data analysis
Administered questionnaires were edited and coded with the use of a coding guide. The data in each questionnaire were entered into a computer and was analysed using the Statistical Package for Social Sciences (SPSS Version 16, IBM Corp., Chicago, USA). In addition, descriptive statistics, Chi square and t-test were used to test for variables of interest at P<0.05.
Ethical consideration
The study proposal was submitted to the UI/UCH Ethical Review
Committee for evaluation and approval. Official permission and approval was also obtained from the management of Saint Mary Catholic Hospital, Eleta Ibadan where the pre-test was carried out and from the PEPFAR authority where the actual study was conducted.
Socio-demographic characteristics
The ages of respondents ranged from 14 to 79 years with a mean age of 40.0 ± 9.4 years. A large proportion of the respondents 474 (67.7%) were females. Respondents’ occupations include the following: trading 330 (47.2%), retired civil servants 128 (18.3%), artisan 76 (10.9%) and 35 (5.0%) were unemployed. Majority of the respondents were married 483 (69.0%) and 498 (71.1%) had secondary education and above Table 1). According to Table 2, majority of the respondents (508, 72.50%) were screened for HIV because they were sick while less than two third (448, 64.0%) and 178 (25.40%) of facilities where the respondents were screened was owned by the Federal Government and individuals, res-pectively. In addition, majority of the respondents (666, 95.10%) had sexual partners, of which 582 (87.30%) and 55 (12.40%) sexual partners were their spouse and boyfriend/girlfriend, respectively. Furthermore, more than two third of the respondents 508 (72.60%) were aware of their partners HIV status and only less than one third 212 (30.30%) affirmed that they had ever experienced stigmatization or discrimination as a result of their HIV status. According to Figure 1, 36.90% of the respondents’ sexual partners were HIV positive, while 39.0% were HIV negative and 24.10% do not know the HIV status of their sexual partners.


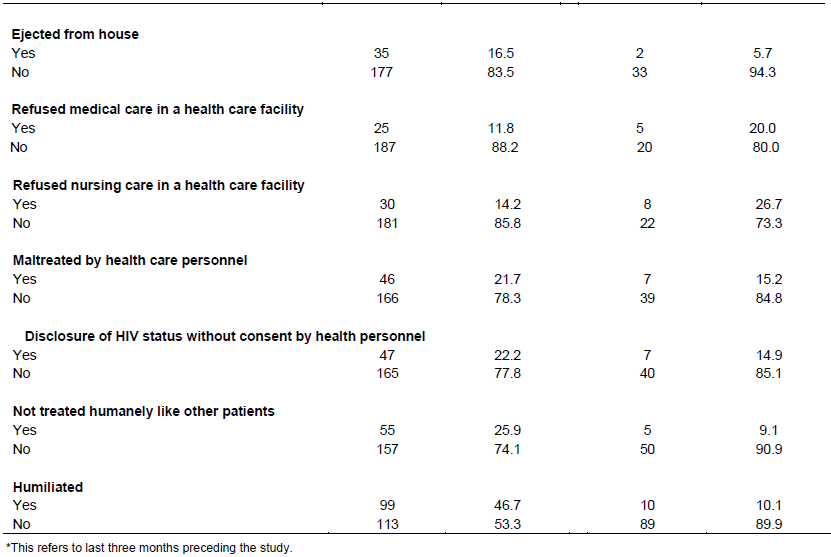
The HIV/AIDS induced stigma and discrimination ever perpetrated against PLHIV were manifested in several forms including the following: physical assault 51 (24.1%), verbal abuse/insult 138 (65.1%), subjection to ridicule 134 (63.2%), avoidance by friends 89 (42.0%) and not treated humanely like other patients 55 (25.9%). Experiences of induced stigma within the three months preceding the study also includes physical assault 7 (13.7%), denial of job opportunity 7 (15.2%), sacked from job 5 (14.7%) and refusal of medical care in a health care facility 5 (20.0%) (Table 3).The forms of self-stigmatization ever experienced included: fear of HIV status disclosure to family members 377 (53.9%), fear of disclosing HIV status to friends 485 (69.3%), stoppage of attendance to social functions 124 (17.3%), stoppage of visiting friends 137 (19.6%), feeling ashamed of accessing medical care 206 (29.4%) and limiting social functions or gatherings attended by them 177 (25.3%). Within the last three months preceding the study, however, only 111 (29.4%) were afraid of dis-closing their HIV status to family members, 128 (26.4%) were afraid of disclosing to friends (Table 4).



As shown, Table 5 highlighted the attitudinal tendencies of others perceived by respondents to be stigmatizing. More than half of the respondents 365 (52.2%) were of the view that people with HIV are often treated as if it is their fault. Slightly above half of the respondents 363 (51.8%) agreed that people physically back away from or refuse to associate with someone because of HIV. In addition, less than half of the respondents 329 (47.0%) agreed that some close relations were afraid of rejection by the society when a family member has HIV. Four hundred and three (59.0%) of the respondents agreed that some friends withdraw from interacting or visiting after hearing that he/she has HIV. Appreciable proportions of the respondents either disagree or strongly disagree with the attitudinal tendencies of others (Table 5).

Common strategies adopted by respondents for coping with stigma and discrimination as a result of their HIV status included the following: unmoved 376 (53.7%), ignore the person 281 (40.1%), and prayer 321 (45.9%). Others include challenging the person discriminating against them 65 (9.3%), threaten legal action 27 (3.9%) or report that experience to support group 53 (7.6%) (Table 6). As shown in Figure 2, a small proportion of the respondents (27.7%) reported that they were members of a social support group for PLHIV; while 72.3% were not in any support group. Coping strategies discussed among PLHIV in support group as highlighted by the respondents were: Not stigmatize one-self 34 (19.6%), living positively 66 (38.1%), not giving room for discrimination to occur 25 (14.5%) (Table 7).
The study showed majorities of the respondents were between the ages of 30 and 49 years and were females. This is similar to the findings of a study carried out in Abeokuta South-West Nigeria (Ojieabu et al., 2014). This finding is in line with those of the National Agency for the Control of AIDS 2016, report and a study by Dahlui et al. (2015), which highlighted the occurrence of stigmatization and discrimination among PLHIV. Similarly, the study reported various forms of stigmatization and discrimination which were perpetrated against the respondents. This finding is in line with previous studies which showed stigma and discrimination perpetrated against PLHIV from colleagues, friends and the community (Ogbuji and Oke, 2010; Blackstock, 2005; Zierler et al., 2000; Bharat, 2011). Furthermore, the respondents also highlighted various forms of self-stigmatization they adopted primarily to conceal their HIV/AIDS status. This fear of revealing their HIV status might breed a culture of silence, sadness, hopelessness, anxiety and fear which can impact their quality of life negatively (Ogbuji and Oke, 2010).
The findings of the study shows that the society still exhibit some attitudinal tendencies which is stigmatizing to PLHIV. This finding is consistent with previous study which reported negative attitude such as the use of the cynical phrase “AIDS family” towards PLHIV (Alubo et al., 2002). This calls for more enlightenment campaign targeted at communities in order to reduce the attitudinal stigma and discrimination associated with HIV/AIDS. The study also highlights various strategies adopted by the respondents in coping with HIV/AIDS-related stigma and discrimination. Some of the coping strategies highlighted are in line with a previous study in Ibadan South-West Nigeria (Ogbuji and Oke, 2010). The most important strategy as underlined by the respondents is belonging to an HIV/AIDS social support group which can act as reinforcing mechanism in coping with stigma and discrimination which according to the study is still prevalent in the society. The possible limitation in the study is that the authors relied absolutely on the responses of the participants of the study in reporting the various forms of stigma and discrimination. There was no independent confirmation of the various forms of stigmatization and discrimination reported in the study.
The study has shown prevalence of various forms of stigmatization and discrimination against PLHIV. Consequently, it appears that there is a general negative perception about HIV/AIDS and the people living with it; and unfortunately this has resulted in negative attitude towards PLHIV within the society. Although, the HIV and AIDS (Anti-Discrimination) Act, 2014, has been passed to protect the rights and dignity of PLWHA by eliminating all forms of discrimination based on HIV status; there is need for more health education campaigns across com-munities nationwide to translate the phobia associated with HIV/AIDS to caring for PLHIV.
The authors have not declared any conflict of interests.
The authors appreciate the Management and Staff of PEPFAR at the University College Hospital, Ibadan and the respondents who voluntarily participated in the research.
REFERENCES
|
Alubo O, Zwandor A, Jolayemi T, Omudu E (2002). Acceptance and stigmatisation of PLWA in Nigeria. AIDS CARE 14(1):117-126.
Crossref
|
|
|
|
Bharat S (2011). A systematic review of HIV/AIDS-related stigma and discrimination in India: Current understanding and future needs. Sahara J. 8(3):138-149.
Crossref
|
|
|
|
|
Blackstock O (2005). Curing stigma- The limits of antiretroviral access. N. Engl. J. Med. 353(8):752.
Crossref
|
|
|
|
|
Brieger W, Delano G, Lane C, Oladepo O, Oyediran K (2001). West African youth initiative: outcome of a reproductive health education programme. J. Adolesc. Health 29(6):436-446.
Crossref
|
|
|
|
|
Dahlui M, Azahar N, Bulgiba A, Zaki R, Oche OM, Adekunjo FO, Chinna K (2015). HIV/AIDS Related Stigma and Discrimination against PLWHA in Nigerian Population. PLoS One 10(12):e0143749.
Crossref
|
|
|
|
|
D'Cruz-Grote D (1996). 'Prevention of HIV infection in developing countries" Lancet 348(9034):1071-1074.
Crossref
|
|
|
|
|
Federal Ministry of Health (2002). HIV/AIDS; what it means for Nigeria (background, Projections, impact, intervention & policy), December, 2002. Federal Ministry of Health, Abuja.
|
|
|
|
|
Federal Ministry of Health (2005). National AIDS and STI Control Programme. National health sector strategic plan for HIV & AIDS 2005–2009. Federal Ministry of Health, Abuja.
|
|
|
|
|
Joint United Programme on HIV/AIDS (2002). World Aids Campaign 2002-2003. A conceptual framework and basis for action. HIV/AIDS stigma and discrimination. Available at:
View
|
|
|
|
|
Joint United Programme on HIV/AIDS (2014). Highlights from the high-level side event. Fast-Tract: Ending the AIDS epidemic by 2030. 25 September 2014. Available at:
View
|
|
|
|
|
Joint United Programme on HIV/AIDS (2015). AIDS by the numbers global report 2015. Geneva, 2015. Available at:
View
|
|
|
|
|
Katz IT, Ryu AE, Onuegbu AG, Psaros C, Weiser SD, Bangsberg DR, Tsai AC (2013). Impact of HIV-related stigma on treatment adherence: systematic review and meta-synthesis, J. Int. AIDS Soc. 16(3 Suppl 2):18640.
Crossref
|
|
|
|
|
Mann J (1987). Statement at an informal meeting on AIDS to the 42nd session of the UN General Assembly, October 20, 1987. Available at:
View
|
|
|
|
|
Monjok E, Smesny A, Essien EJ (2009). HIV/AIDS - Related Stigma and Discrimination in Nigeria: Review of Research Studies and future directions for Prevention Strategies. Afr. J. Reprod. Health 13(3):21-35.
|
|
|
|
|
National Agency for the Control of AIDS (NACA) (2016). Stigma and Discrimination Reduction in the National HIV/AIDS Response.
|
|
|
|
|
Ogbuji QC, Oke AE (2010). Quality of life among people living with HIV infection in Ibadan, Nigeria. Afr. J. Med. Sci. 39(2):127-135.
|
|
|
|
|
Ojieabu WA, Eze UIH, Fashola OS, Bello SI, Arute JE (2014). HIV/AIDS Related Stigmatization and Discrimination. Afr. J. Pharm. Res. Dev. 6(1):37-43.
|
|
|
|
|
Oyediran K, Oladipo O, Anyanti J (2005). HIV/AIDS Stigma and Discrimination in Nigeria. Paper presented at XXV International Population Conference, International Union for the Scientific Study of Population (IUSSP), Tours, France. July 18-23, 2005. Available at:
View
|
|
|
|
|
Pennebaker JW (1989). Confession, inhibition, and disease. Adv. Exp. Soc. Psychol. 22:211-244.
Crossref
|
|
|
|
|
Population Council Horizons (2002). Stigma and discrimination. Research update" Washington, D.C., Population Council, Horizons, Jan. [2] p. Research Update, USAID Award No. HRN-A- 00-97-00012-00.
|
|
|
|
|
Tsai AC, Bangsberg DR, Kegeles SM, Katz IT, Haberer JE, Muzoora C, Kumbakumba E, Hunt PW, Martin JN, Weiser SD (2013). Internalized stigma, social distance, and disclosure of HIV seropositivity in rural Uganda. Ann. Behav. Med. 46(3):285-94.
Crossref
|
|
|
|
|
United Nations General Assembly (2005). Resolution adopted by the General Assembly sixtieth session, 24 October, 2005, 2005 World Summit Outcome ARES/60/1. Available at:
View
|
|
|
|
|
World Health Organization (2006). Fifty-Ninth World Health Assembly: Decisions and Resolutions. Prevention and control of sexually transmitted infections: global strategy. Resolution WHA59.19. Available at:
View
|
|
|
|
|
Zierler S, Cunningham WE, Andersen R, Shapiro MF, Nakazono TY, Morton S, Crystal S, Stein M, Turner B, St Clair P, Bozzette SA (2000). Violence victimization after HIV infection in a US probability sample of adults patients in primary care. Am. J. Public Health 90(2):208-215.
Crossref
|
|