Full Length Research Paper

ABSTRACT
In resource limited countries, there is scarcity of information regarding the degree of immunological and clinical recovery in remote communities with ART service. This study retrospectively assessed the degree of immune recovery by CD4 count after initiation of ART. A retrospective cohort study was conducted on adult HIV patients who have been on ART for more than one year at Karamara Hospital. All analyses were performed using SPSS software version 19.0 and findings were compared using the appropriate statistical tests. The median change from baseline to the most recent CD4 cell count was 141 cells/μl. By 5 years, the overall median CD4 cell count was 472 cells/μl while the median CD4 cell count was 401 cells/μl among patients with baseline CD4 cell counts ≤100 cells/μl, 467 cells/μl among those with baseline CD4 cell counts of 100 to 199 cells/μl, and 586 cells/μl among those with baseline CD4 cell counts equal to greater 200 cells/μl. At the end of the study, patients with higher baseline CD4 cell stratum returned to normal CD4 cell counts compared to those with the least baseline CD4 cell stratum. The findings suggest that consideration be given to initiation of ART at a CD4 cell count >350 cells/μl to achieve better immune recovery.
Key words: Antiretroviral therapy, CD4 cell count, HIV infection.
INTRODUCTION
Human immunodeficiency Virus (HIV), the agent that causes acquired immune deficiency syndrome (AIDS), is classified as members of the lentivirus subfamily of retroviruses. The virus principally infects cells with a CD4 receptor, including T helper lymphocytes, macrophages, and other cell types. Viral replication results in progressive T-cell depletion and diminished cell-mediated immunity. The gp120 virus surface antigen binds with high affinity to the cell surface CD4, promoting fusion between virus and cell membranes. Co-receptor chemokine receptors CXCR4 and CCR5 may also play a role in internalization as well as immunoglobulin that assist in antibody dependent uptake. The natural history of HIV depicts the outcome of HIV infection, which leads to destruction of lymphocytes and development of AIDS (Actor et al., 2007).
Since its recognition, HIV has created an enormous challenge worldwide, it has infected close to 70 million people, and more than 30 million have died due to acquired immunodeficiency syndrome (AIDS). More than 66% of the 40 million people living with HIV/AIDS are in sub-Saharan Africa, where AIDS is the leading cause of death. Ethiopia is the second most populous and one of the seriously affected countries in sub Saharan Africa. With more than 1.3 million people living with HIV and an estimated 277,800 people requiring treatment, the Government of Ethiopia has taken measures to reduce the risk of HIV transmission and mitigate the impact of the epidemic on society. In 2003, the Government of Ethiopia introduced its ART program with the goal of reducing HIV-related morbidity and mortality, improving the quality of life of people living with HIV and mitigating some of the impact of the epidemic (Seoane et al., 2008).
According to the 2012 UNAIDS Report on the HIV epidemic, there were 333,434 people (249,174 adults and 16,000 children) on antiretroviral treatment at the end of 2011. This represents 86% coverage of adults in need of treatment and 20% in children. In Ethiopia, after the beginning of free ART, though the adult prevalence of HIV showed reduction its epidemic continued and estimated to be 1.5% (1.9% among women and 1.0% among men) with marked regional variations which ranges from 0.9% in Southern Ethiopia (SNNPR) to 6.5% in Gambella region in the Western part of the country. There is also wide urban rural variation in HIV prevalence with urban areas estimated to have a prevalence of 4.2% compared to 0.6% in rural areas (UNAIDS, 2012; WHO, 2005; ORC Macro, 2012).
Much is not known about immune recovery of patients taking ART in Somali region. Hence, aims of this study are to explore immune recovery by CD4+ T-cell count according to baseline CD4+ T-cell and to investigate clinical outcome in a retrospective cohort of HIV-infected patients over the 60 months of treatment.
MATERIALS AND METHODS
Study site and design
A retrospective cohort study was employed from January 2015 to January 2016 in Jigjiga to assess the immunological response mainly of their CD+4 count after ART initiation. Jigjiga is the capital city of Ethio-Somali regional state that located about 620 km East of Addis Ababa. It is one of the cities where wide ART services are given in the region. Karamara hospital provides general outpatient and inpatient services, including surgical and obstetric emergency care. The adult HIV prevalence rate of the region is 1.1% based on EDHS (2011).
Study population
The study population were all HIV positive patients at Karamara hospital who have been on ART for more than or equal to 12 months.
Sample size
Eligible adults who started ART treatment during the period of September 2007 to September 2014 were included. The study included all cases with complete baseline information from Karamara hospital ART clinic during the period of September 2007 to September 2014. Therefore, this was a census type study and didn’t involve any sampling. Clinical documents of all patients who started HAART and who had a minimum of two follow up period at study period were recruited for this study.
Sampling technique
General information about patients in the hospital enrolled during the study period was evaluated. Using ART unique identification number from ART register in Karamara Hospital documents of all patients enrolled for ART care between September 2007 and September 2014 were evaluated.
Study criteria
Inclusion criteria
The inclusion criteria for the recruitment of the study participants included those HIV positive adult patients above 15 years of age and who started HAART between September 2007 and September 2014; and all HIV positive patients on HAART, who have at least been treated for 1 year and have a baseline CD4 determination for at least two follow-up or above.
Exclusion criteria
All transferred HIV patients on HAART and those who have incomplete baseline, CD4 determination or clinical and socio-demographic information were excluded.
Measurement
Outcome variables
Change in immune recovery (that is, CD4+ T cell number) between initiation of HAART and the most recent available follow-up times.
Independent variables
Socio-demographic characteristics (Age, sex, marital status, educational status, employment, religion), behavioral factors (adherence to treatment/loss to follow-up), clinical information (Weight, WHO stage, past history of TB treatment, baseline regimens, substitution of regimen from baseline, OI at baseline) and laboratory result information (CD4 + T cell counts category at the time of initiation of ART) were included.
Ethical consideration
This study was conducted after formal approval of the protocol was made by Research, Publication and Technology Transfer Committee of Jigjiga University. Prior to data collection the necessary permission letter was obtained from the study hospital. In order to maintain patient confidentiality all information was kept in code and data collection were made by trained staff nurses working in the clinic.
RESULTS
Patient’s socio-demographic characteristics
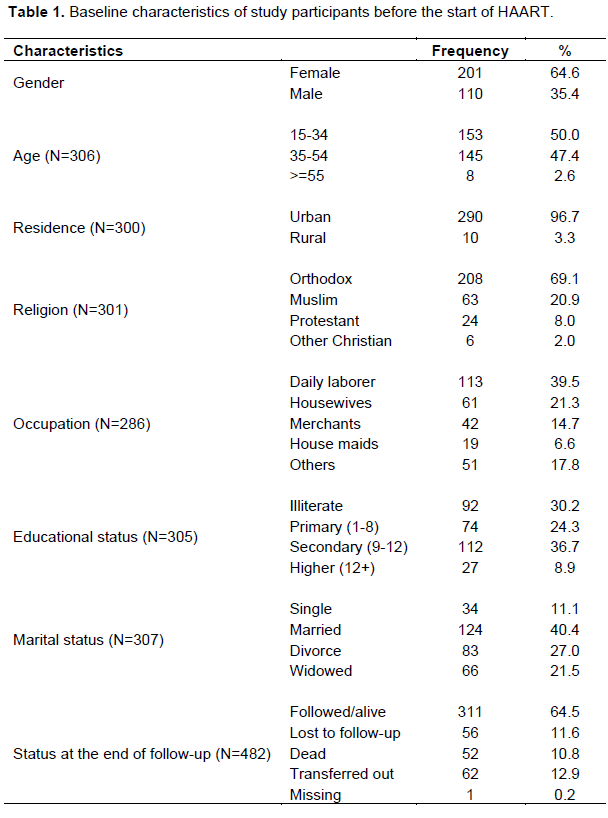
A retrospective cohort study was conducted by reviewing 482 medical records of adult ART treatment HIV patients at Karamara Hospital ART clinic. Of these, 311 were eligible for this study based on the inclusion criteria. Among these 311 eligible patients who had have a completed five year CD4 records within the appropriate time intervals and were under active monitoring, 56 had died, 62 had been transferred out, 52 were lost to follow-up.
A total of 311 with the complete CD4 were included in the analysis as shown in the following table (Table 1). The median age was 34.5 years (interquartile range [IQR] 28 to 40), 201(64.6%) were females, 124 (40.4%) were married, 208 (69.1%) were orthodox, 290 (96.7%) were from urban residence, 112 (36.7%) were completed secondary school and 113 (39.5%) were daily laborer at the time of their ART initiation.
Clinical characteristics of study participants
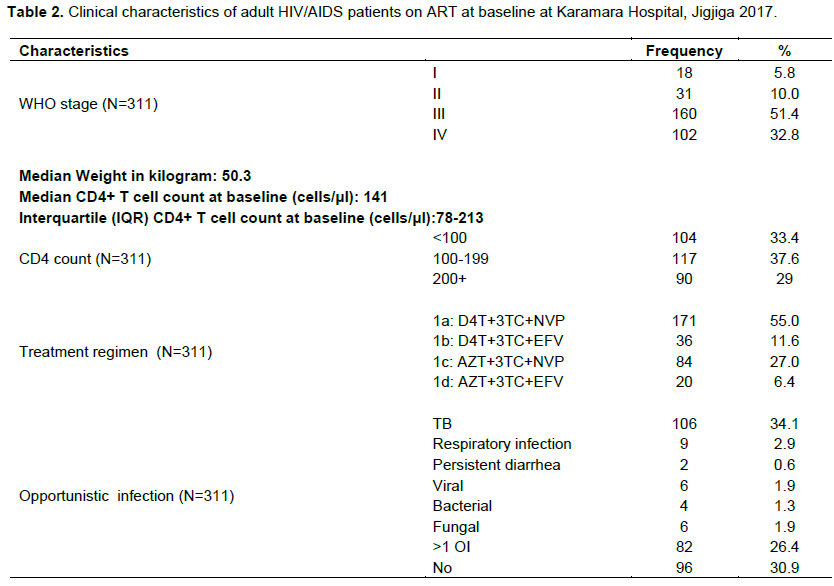
As described in the following (Table 2) the median CD4 cell count was 141 cells/µl (IQR 78-213), majority 37.9% of them had a CD4 count between 100 to 199 and 51.4% had a WHO clinical stage III at ART initiation time. Patients with history of tuberculosis were 34.1% at baseline. Antiretroviral therapy consisted of a nevirapine-based regimen in 82% of individuals. Majority, 55% of all patients were started on stavudine /lamivudine/ nevirapine (D4T+3TC+NVP), 11.6% on (D4T+3TC+EFV) stavudine/lamivudine/efavirenz, 27% on (AZT+3TC+NVP) zidovudine /lamivudine/nevirapine, 6.4% on (AZT+3TC+EFV) lamivudine/stavudine/efavirenz on drug combinations.
Immune recovery by CD4 count
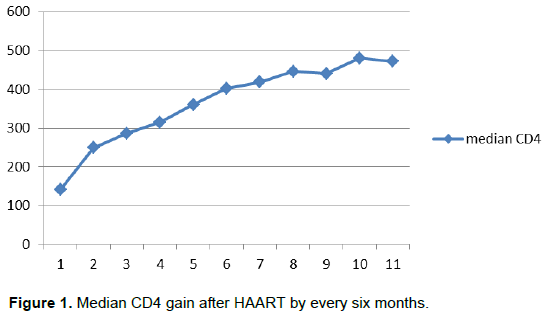
Overall, median CD4 increased from a baseline value of 141 cells/mm3 (IQR, 78 to 213 cells/mm3) to 249 cells/mm3 (IQR, 180 to 341 cells/mm3) at 6 months and to 446 cells/mm3 (IQR, 298 to 584 cells/mm3) by year 5 (Figure 1). Although CD4 continued to increase throughout the 5 years, the ï¬rst 2 years after ART initiation showed a steeper increase compared to the latter 3 years.
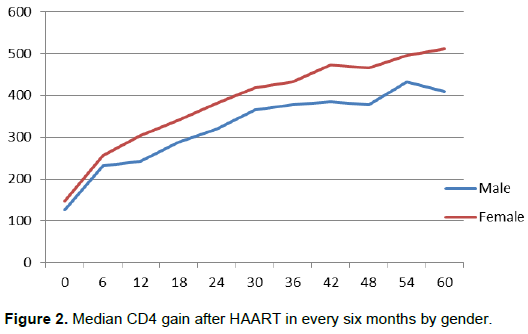
Gender response to HAART
Among the adherent patients in the study, there were a higher proportion of women (64.6%) than men (35.4%). Women exhibited higher median CD4 count values (148 cells/μl) than men (127 cells/ μl) before the start of therapy. The respective CD4 increases for men and women were 232 and 258 cells/ μl at 6 months, and 243 and 304 cells/μl at 12 months, respectively (Figure 2). At five years follow up of treatment, CD4 count had increased from baseline of 127cells/μl to 409.5 cells/μl in men, and from baseline of 148 cells/μl to 511 cells/μl in women.
Baseline CD4 and treatment response
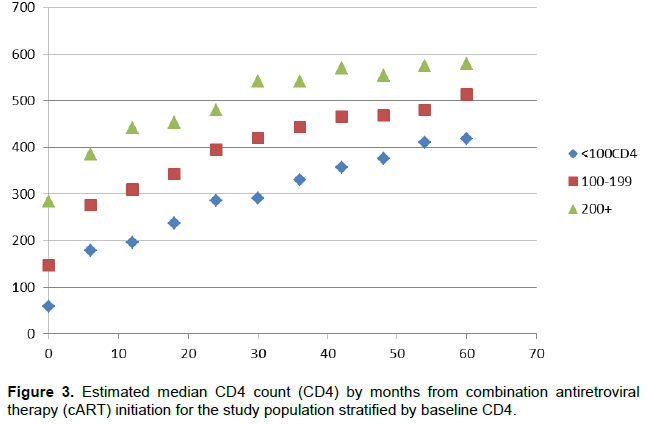
Among those who were adherent, patients were categorized into three CD4 strata: (median baseline CD4 count of <100 cells/ μl), (baseline CD4 counts between 100 to 199 cells/μl) and (Baseline CD4 counts =>200 cells/ μl) for this study. CD4 increases from baseline were 122.47 and 160.8 cells/ μl at 6 and 12 months, respectively for category (median baseline CD4 count of <100 cells/ μl), and 129.19 and 162.07 cells/μl for category (baseline CD4 counts between 100-199 cells/μl) and 100.65 and 157.45 cells/ μl for category(Baseline CD4 counts =>200 cells/ μl) (Table 3).
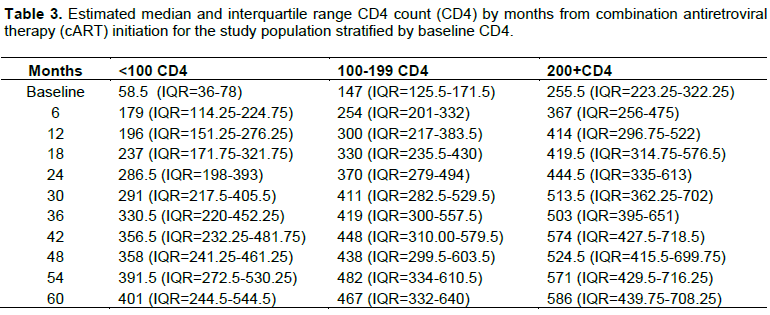
Median CD4 at year 5 was 401 cells/mm3 (IQR, 244 to 544.5 cells/mm3), 467 cells/mm3 (IQR, 332 to 640 cells/mm3), and 586 cells/mm3 (IQR, 439 to 708 cells/mm3) for those with baseline CD4 <100, 100 to 199, and ≥200 cells/mm3, respectively (Figure 3).
DISCUSSION
This retrospective cohort study was carried out to assess the trends in CD4 cell recovery and clinical response among HIV patients on ART utilization and the effect of baseline characteristics on CD4 cell count response. CD4+ cell responses was evaluated whether patients failed to attain mean CD4+ cell count increase from baseline of at different interval months (defined as immunological non-response) and whether patients achieved an absolute CD4+ count of 200 cells/μl at the 12th months visit (Kelley et al., 2009)
At baseline, the mean CD4 cell count of ART-naïve HIV infected patients was 141 cells/μl, this is comparable with other reports from Tigray (Asfaw et al., 2015) and Burkina faso (Tiba et al., 2012) but higher than the reports from Zewditu hospital Addis Ababa, 81 cells/ul (Moges et al., 2013) and Lao, 41 cells/ul (Bastard et al., 2013). This could be due to the delay in presentation or ART initiation. As like other studies so far conducted on this area, better improvements in overall CD4 cell count among the patients was seen over time mainly for the first two years generally up to year 3 after these it showed slight increment until five years. These findings are consistent with the study conducted in northern and eastern Ethiopia where the median CD4 lymphocyte count had improved over the five year period in the similar fashion to our study (Asfaw et al., 2015; Reda et al., 2013) and elsewhere clearly investigated that CD4 cell counts were increased significantly until year 4 though varied among different CD4 cell strata thereafter (Moore et al., 2009).
On the other hand, the present work reported that patients with lower baseline CD4 cell counts had lower peaks of CD4 cell counts. While patients with a high baseline CD4 cell count (>200 cells/μl) had CD4 cell counts that returned to almost normal levels. These results are consistent with reports from other studies which shows only patients with high baseline CD4 cell count had CD4 cell counts that returned to nearly normal levels though CD4 cell count (WHO, 2005; MacLennan et al., 2007).
In this study, female HIV patients showed a better CD4 cell count after HAART initiation was pointed out than male. This is consistent with other report by Asfaw et al. (2015), Zhou et al. (2010), Kumar et al. (2017), and Malaza et al. (2013). In contrast, a study of immunological recovery in patients indicated that gender was not associated with the increase in CD4 counts (Smith et al., 2004; Lawn et al., 2006).
This study attempted to determine the loss to follow up from ART treatment program among adult population. The loss to follow up rate was 11.6% in this study. This finding is comparable with studies which were conducted in Northwest Ethiopia but lower than studies from Bahrdar Felege Hiwot Hospital and Gonder Referral Hospital which showed that the lost to follow up rate were 8.4, 18 and 19% respectively (Gezie et al., 2017; Molla et al., 2018).
CONCLUSION
The findings of this study depicted that there are an improvement in CD4 recovery and the highest CD4 cell counts were achieved when HAART was started at a high baseline CD4 cell count. The CD4 cell count is less likely to return to normal when HAART is started at lower CD4 cell counts, this could be a reason to consider initiating HAART before high CD4 cell count decreases. The present findings confirm the previous studies that the degree of CD4 depletion prior to ART initiation is the most consistent determinant of subsequent immune reconstitution. Therefore, initiation of HAART before the CD4 cell count decreases to <200 cells/μl is recommended to achieve and maintain normal CD4 cell count. Females HIV patients achieved better immune recovery as compared with male.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGMENTS
The authors appreciate ART clinic staffs for their unreserved support throughout the data collection. Authors are also grateful to Karamara Hospital for support in provision of data and necessary materials, and Jigjiga University for the financial support of this research work.
REFERENCES
|
Actor JK (2007). Elsevier's Integrated Immunology and Microbiology. Mosby Incorporated. |
|
|
Asfaw A, Ali D, Eticha T, Alemayehu A, Alemayehu M, Kindeya F (2015) . CD4 Cell Count Trends after Commencement of Antiretroviral Therapy among HIV-Infected Patients in Tigray, Northern Ethiopia: A Retrospective Cross-Sectional Study. PLoS ONE 10(3): e0122583. |
|
|
Bastard M, Soulinphumy K, Phimmasone P, Saadani AH., Ciaffi L, Communier A, Phimphachanh C, Ecochard R, Etard JF (2013). Women experience a better long-term immune recovery and a better survival on HAART in Lao People's Democratic Republic. BMC Infectious Diseases 13(1):27. |
|
|
Central Statistical Agency [Ethiopia] and ORC Macro (2012). Ethiopia Demographic and Health Survey 2011: Addis Ababa, Ethiopia, and Calverton, Maryland, USA: Central Statistical Agency and ORC Macro. |
|
|
Gezie LD, Gelaye KA, Worku AG, Ayele TA, Teshome DF (2017). Time to immunologic recovery and determinant factors among adults who initiated ART in Felege Hiwot Referral Hospital, Northwest Ethiopia. BMC Research Notes 10(1):277. |
|
|
Joint United Nations Programme on HIV/AIDS (UNAIDS): Report on the global AIDS epidemic, 2012, "UNAIDS / JC2417E". |
|
|
Kelley CF, Kitchen CM, Hunt PW, Rodriguez B, Hecht FM, Kitahata M, Crane HM, Willig J, Mugavero M, Saag M, Martin JN (2009). Incomplete peripheral CD4+ cell count restoration in HIV-infected patients receiving long-term antiretroviral treatment. Clinical Infectious Diseases 48(6):787-794. |
|
|
Kumar AM, Gupta D, Kumar A, Gupta RS, Kanchar A, Rao R, Shastri S, Suryakanth MD, Rangaraju C, Naik B, Guddemane DK., Bhat P, Nair AS, Harries AD, Dewan P (2017). HIV-infected presumptive tuberculosis patients without tuberculosis: How many are eligible for antiretroviral therapy in Karnataka, India? Journal of Epidemiology and Global Health 71:11-19. |
|
|
Lawn SD, Myer L, Bekker L, Wood R (2006). CD4 cell count recovery among HIV-infected patients with very advanced immunodeficiency commencing antiretroviral treatment in sub-Saharan Africa, BMC Infectious Diseases 6:59. |
|
|
MacLennan CA, Liu MK, White SA, van Oosterhout JJ, Simukonda F, Bwanali J, Moore MJ, Zijlstra EE, Drayson MT, Molyneux ME (2007). Diagnostic accuracy and clinical utility of a simplified low cost method of counting CD4 cells with flow cytometry in Malawi: Diagnostic accuracy study. British Medical Journal 335(7612):190-190. |
|
|
Malaza A, Mossong J, Ba¨rnighausen T, Viljoen J, Newell M-L (2013). Population-Based CD4 Counts in a Rural Area in South Africa with High HIV Prevalence and High Antiretroviral Treatment Coverage. PLoS ONE 8(7):e70126. |
|
|
Moges Derbe, Monga DP, Deresse Daka (2013). Immunological response among HIV/AIDS patients before and after ART therapy at Zewuditu Hospital Addis Ababa, Ethiopia. American Journal of Research Communication 1(1):103-115 View |
|
|
Molla AA, Gelagay AA, Mekonnen HS, Teshome DF (2018). Adherence to antiretroviral therapy and associated factors among HIV positive adults attending care and treatment in University of Gondar Referral Hospital, Northwest Ethiopia. BMC Infectious Diseases 18(1):266. Published 2018 Jun 8. |
|
|
Moore DM, Harris R, Lima V, Hogg B, May M, Yip B, Justice A, Mocroft A, Reiss P, Lampe F, Chêne G, Costagliola D, Elzi L, Mugavero MJ, Monforte AD, Sabin C, Podzamczer D, Fätkenheuer G, Staszewski S, Gill J, Sterne JA, Antiretroviral Therapy Cohort Collaboration (2009). Effect of baseline CD4 cell counts on the clinical significance of short-term immunologic response to antiretroviral therapy in individuals with virologic suppression. Journal of Acquired Immune Deficiency Syndromes 52(3):357-63 |
|
|
Reda AA, Biadgilign S, Deribew A, Gebre B, Deribe K (2013). Predictors of Change in CD4 Lymphocyte Count and Weight among HIV Infected Patients on Anti-Retroviral Treatment in Ethiopia: A Retrospective Longitudinal Study. PLoS ONE 8(4):e58595 |
|
|
Seoane E, Resino S, Micheloud D, Moreno A, Juan CL, Lorente R, Rubio R, Gonzalez J, Pulido F, Arribas JR, Moreno S (2008). Lipid and apoprotein profile in HIV-1-infected patients after CD4-guided treatment interruption. Journal of Acquired Immune Deficiency Syndromes 48(4):455-459. |
|
|
Smith CJ, Sabin CA, Youle MS, Kinloch-de Loes S, Lampe FC, Madge S, Cropley I, Johnson MA, Phillips AN (2004). Factors influencing increases in CD4 cell counts of HIV-positive persons receiving long-term highly active antiretroviral therapy. The Journal of Infectious Diseases 190(10):1860-1868. |
|
|
Tiba F, Nauwelaers F, Traoré S, Coulibaly B, Ouedraogo T, Compaoré A, Kräusslich HG, Böhler T (2012). Immune reconstitution during the first year of antiretroviral therapy of HIV-1-infected adults in rural Burkina Faso. The Open AIDS Journal 6:16. |
|
|
Zhou J, Sirisanthana T, Kiertiburanakul S, Chen YMA, Han N, Lim P, Kumarasamy N, Choi JY, Merati TP, Yunihastuti E, Oka S (2010). Trends in CD4 counts in HIV-infected patients with HIV viral load monitoring while on combination antiretroviral treatment: Results from The TREAT Asia HIV Observational Database. BioMed Central Infectious Diseases 10(1):361. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


