Full Length Research Paper

ABSTRACT
Human immunodeficiency virus (HIV) and Helicobacter pylori (H. pylori) infections are worldwide healthcare burdens. This study aimed to assess the prevalence and associated factors of H. pylori infection among HIV patients at Southern-Ethiopia. A Hospital based cross-sectional study was conducted at Hawassa University comprehensive specialized hospital on 390 HIV infected adults on antiretroviral therapy from September to November 2017. All vital data were collected by designed questionnaires and stool samples were collected using appropriate sample cap for H. pylori stool antigen diagnosis. The overall prevalence of H. pylori infection of HIV infected patients was 17.9%. About 42.6% of the participants had a history of dyspepsia and of them, 4.3% were positive for H. pylori infection. In addition, 48.9% of patients were using either aqua tablet (67 mg-Trocloresene sodium) or water filters for drinking water, of them 11.5% were positive for H. pylori infection. Having a history of dyspepsia: the adjusted odds ratio [AOR (95% CI): 4.8 (1.6–14.7)], and age ≤30 years [AOR (95% CI):3.7(1.6–8.8)] were associated factors of H. pylori infection. Moreover, the association of H. pylori infection ≤ 30 years old and history of dyspepsia indicates the need of further large-scale and cohort type studies to determine the other possible associated factors for the infection.
Key words: Helicobacter Pylori, HIV, stool antigen test, South-Ethiopia.
INTRODUCTION
Helicobacter pylori is a gram negative bacteria, spiral, flagellated bacillus that naturally colonizes humans’ stomach. It lives extra-cellular spaces, mucous layer layer. Then this infection induces a host response that results in mucosal damage and a chronic active gastritis (Ostrow et al., 2010). H. pylori infection is associated with peptic ulcer, gastric cancer, and lymphomas in human (Marshall et al., 2008). The infection has also been associated firmly with the development of gastric neoplasia, including gastric adenocarcinomas and gastric mucosa-associated lymphoid tissue lymphomas (Versalovic, 2003). In addition, the prevalence of H. pylori infection among People Living with Human immunodeficiency virus (HIV) varies from 10 to 76% depending on the period, geographical area and diverse in population (Nkuize et al., 2010; Fialho et al., 2011). Even if antiretroviral treatment (ART) had brought improvements including and increased the life expectancy in HIV infected individuals, however, H. pylori infections are seen more frequent in ART patients compared to those did not receive ART (Palella et al., 1998). The gastro-intestinal tract (GIT) plays an important role in the patho-physiology of HIV/ Acquired Immuno-deficiency syndrome (AIDS) (Khamri et al., 2010). In addition, H. pylori colonizes the gastric and duodenal mucosae and then it induces a specific local in addition with systemic immune response. The CD4+ T cells, dendritic cells, regulatory T cells and Th17cells components also play a role in HIV pathogenesis (Khamri et al., 2010; Mitchell et al., 2007). However, few studies were done on the assessment of problem in Ethiopia and these studies were done based on serological tests of that its own drawbacks and in non-discrimination in between current and past infections, including with its low specificity.
Therefore, this study aimed to assess the prevalence and associated factors of H. pylori infection among HIV-infected adults in Hawassa University Compressive Specialized Hospital (HUCSH) by using stool antigen.
MATERIALS AND METHODS
Study area and study population
This institution based cross sectional study was conducted at Hawassa University comprehensive specialized Hospital, Southern Nations Nationalities and Peoples Region (SNNPR) from September to November 2017. The Hospital was established in November 2005 and it provides teaching and health services. Nowadays, the hospital has over 400 beds and providing health services for patients including practical training for students. About 7125 HIV positive patients were attending the Hospital during the study period. All HIV-positive adults on ART age greater than or equal to 18 years old were eligible in the study. However, patients who were receiving anti-H. Pylori treatment within two weeks, and who were receiving anti-H. Pylori agents currently were excluded from the study.
Ethics clearance and consent to participate
The study was approved by the Institutional Review Board of Hawassa University, College of Medicine and Health Sciences. All the study participants were well versed about the protocol of the study, the involvement was voluntary and written informed consent was obtained from the study participant before data collection.
Sample size and technique
The sample size was calculated based on single population proportion formula and 64.2% prevalence H. Pylori infection among peoples living with HIV in Addis Ababa, Ethiopia (Teka et al., 2015).
Based on the above-mentioned, formula, including with 10% non-response rate, the final sample size was calculated to be 390. To select participants from the study population, daily patients flow was assessed for a week in the ART clinic. Thus, the trend showed that the average weekly HIV patients flow was about 73. Lastly, every fifth HIV-infected patients were selected by systematic sampling method.
Data collection and assessment
Socio-demographic data and other relevant medical related information of the study subjects were collected by trained nurses using pre-tested designed questionnaires. About two gram of stool sample was collected from each patients using sterile stool containers with a spatula in it. Instruction was given for each patient to avoid contamination of sample from the toilet, and covering immediately to avoid sample drying. Sample containers were properly labeled with unique number that was analogous with the patient’s identity number found on the questionnaire. In addition, H. pylori stool antigen test was performed at Hawassa University Comprehensive Specialized Hospital Laboratory by H. pylori stool antigen test kit (CTK H.PYLORI, USA) according to the manufacturer instruction. Moreover, the test kit Sensitivity and specificity was 94.4 and 97.8%, respectively. Further, laboratory performance was strictly managed by following standard operating procedure from sample collection to result releasing.
Statistical analysis
All questionnaires were checked and entered into Epi Data version 3.1 and then exported to Statistical Package for Social Sciences (SPSS) version 20 for statistical analysis. Besides, categorical variables were summarized as frequencies and percentages, while mean values and standard deviations were tabulated for quantitative continuous variables. Chi-square was used for categorical variables. Bivariate analyses were conducted primarily to check the study groups differences in the distribution of categorical variables. Further, to control the possible effect of confounding variables, those variables having a P-value of less than 0.2 were entered in to multivariate logistic regression model. Finally, alpha level was set at 0.05 for statistical significance at 95% of confidence interval (CI).
RESULTS
Socio demographic characteristics of study participants
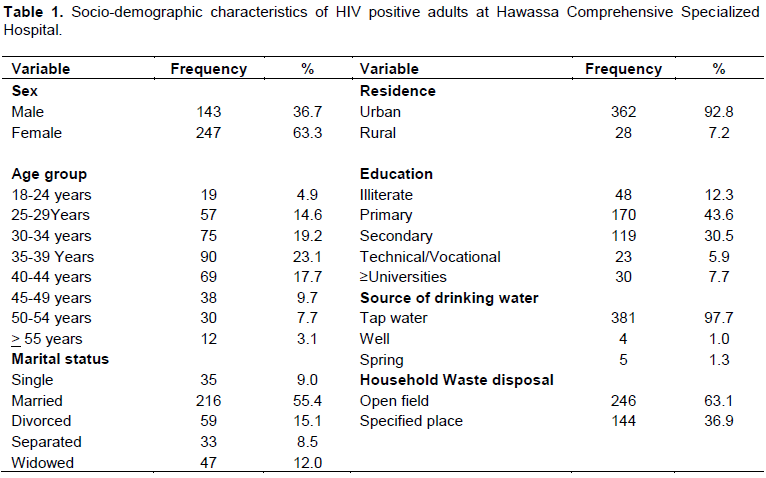
Among the 390 participants, 247 (63.3%) were females and the mean age of the study participant was 37 ± 9.7 with the range of 18 to 62 years old. About 19 (4.9%) of the respondents were aged below 24 years old, while 7519.2%) and 90 (23.1%) were aged between 30-34 and 35-39 years, respectively. In addition, 368 (92.8%), 48 (12.3%), 170 (43.6%) and 72 (44.1%) of the study (subjects were urban inhabitants, had no formal education, primary level of education, and greater or equal to secondary education, respectively. About 35 (9.0%) were non-married and 216 (55.4%) were married, whereas 59 (15.1%) were divorced, 33 (8.5%) were separated and 47 (12.1%) were widowed (Table 1).
Behavioral characteristics of study participants
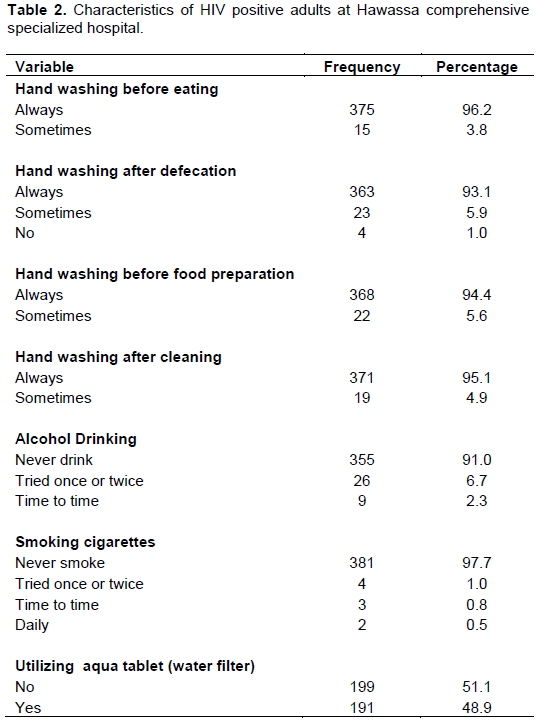
Participants who had a habit of continuously hand washing before meal, after defecation and before food preparation were 375 (96.2%), 363 (93.3%), and 368 (94.4%), respectively. About 35 (9.0%) and 9 (2.3%) of the study participant never drank alcohol and never smoked cigarette. Besides, 191 (48.9%) were using either aqua tablet (67 mg-Trocloresene sodium) or water filter to treat and purify water for drinking (Table 2).
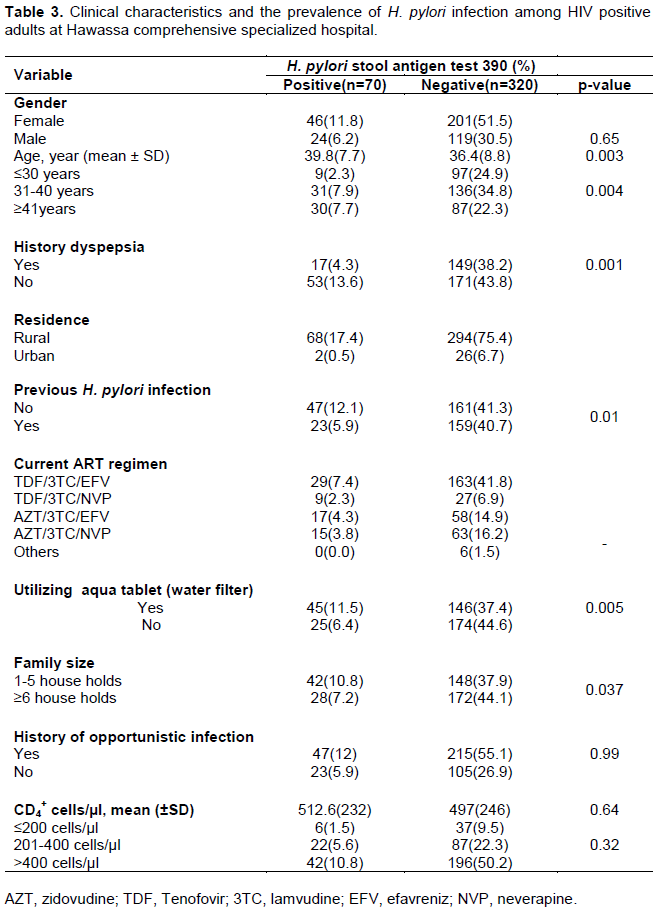
Clinical characteristics and the prevalence of H. pylori infection
Patients on TDF/3TC/EFV of ART regimen were 192 (49.2%) followed by AZT/3TC/EFV: 75 (19.2%). The majority, 169 (43.3%) of the patients were received ART for greater than or equal to five years. In addition, Participants with the previous history of opportunistic infection were 262 (67.2%) and about 43 (11%) of the participants had CD4+cells count less than or equal to 200 cells/µl. There were 166 (42.6%) of the participants had a history of dyspepsia. Moreover, the overall prevalence of H. pylori infection in the study participants was 70 (17.9%) and females had high prevalence rate 46 (11.8%) compared to males 24 (6.2%). The mean age of H. pylori infected participants was significantly higher (39.8±7.7 years) when compared to H. pylori negatives (36.4±8.8 years), p=0.003 and 31 (7.9%) H. pylori infection was observed in age group between 31-40 years old. Among dyspeptic patients, 17 (4.3%) were positive for H. pylori infection. Furthermore, 191(48.9%) were using either aqua tablet (67 mg-Trocloresene sodium) treatment or water filters for drinking water, about 45 (11.5%) were positive for H. pylori infection (Table 3).
Factors associated with H. pylori infection
In bivariate analysis: family size greater than or equal to six households had the crude odds ratio [COR (95% CI): 1.7 (1.0–2.9); p = 0.038] and age ≤30 years [COR (95% CI): 3.7(1.7-8.3); p = 0.001] were associated with H. pylori infection. In addition, having a history of dyspepsia [COR (95% CI): 2.7 (1.5-4.9); p = 0.001], being unmarried [COR (95% CI): 10.7(1.3–87); p = 0.03] and having a previous history of H. pylori infection [COR (95% CI):2.0(1.2-3.5); p = 0.012] were also associated with H. pylori infection (Table 4).
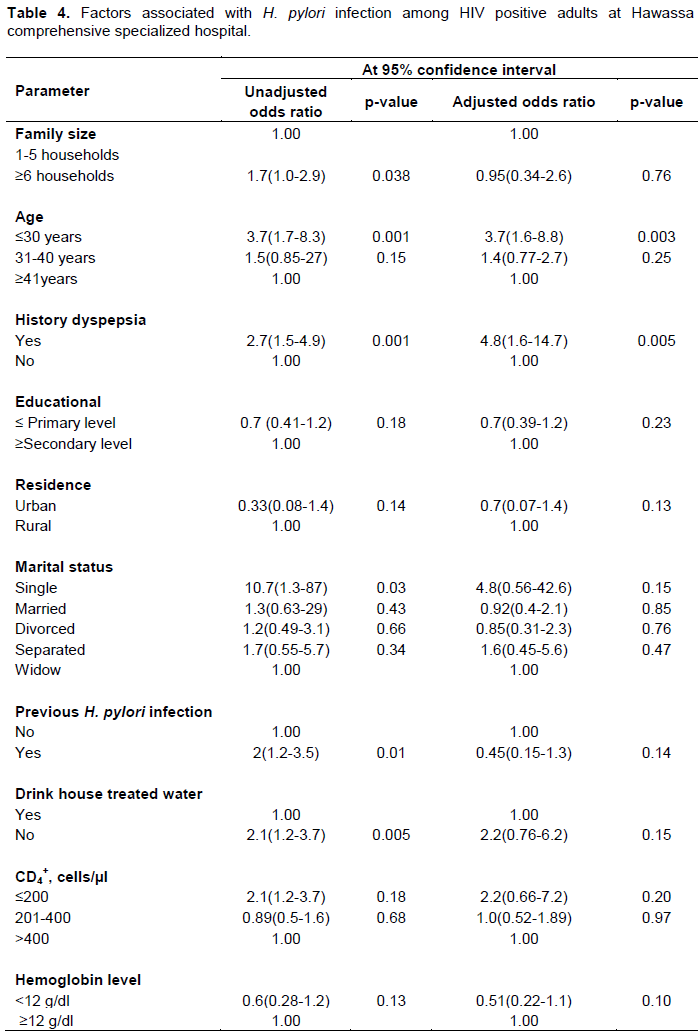
However, multivariate analysis was adjusted for possible confounding factors, only having a history of dyspepsia: the adjusted odds ratio [AOR (95% CI): 4.8 (1.6–14.7); p = 0.005], and age less than or equal to 30 years [AOR (95% CI):3.7(1.6–8.8); p = 0.003] were the associated factors of H. pylori infection (Table 4).
DISCUSSION
H. pylori infection has been known to be more associated with gastritis, duodenal ulcer, gastric cancer, and mucosa associated lymphoid tissue lymphoma (Lepper et al., 2004). The actual infection rates vary from nation to nation; the developing countries have much higher infection rates (90%) due to different factors when compared to developed countries (1.2-12%) (Frenck et al., 2003).
The current study showed that the prevalence of H. pylori infection among HIV infected patients was 17.9%. The finding is lower than the studies reported from Iran (Kafil et al., 2011), India (Nkuize et al., 2010), Ghana (Sarfo et al., 2015), two studies of Nigeria (Anejo-Okopi et al., 2016; Ejilude et al., 2011) and other part of Ethiopia (Teka et al., 2015), which was 69.7, 33, 51.5, 46.8, 47.4 and 64.2%, respectively. Conversely, Perry et al. (2006) from Romania, reported low rate of prevalence, which was 8.3%. The differences might be due to the socio-economic differences, environmental sanitation condition and the changes in health care practice across countries (Anejo-Okopi et al., 2016 and Mynepalli et al., 2014).
It was found that the high prevalence of H. pylori infection in women (11.8%) when compared to males6.2%). And similar findings were reported by Fialho et al. (2011) from Brazil and Anejo-Okopi et al. (2016) from Nigeria. We found that lower prevalence of H. pylori infection among patients with CD4+ cells count below or equal to 200 mm3 and the finding is in line with the studies conducted by Fialho et al. (2011) and Sarfo et al. (2015). In support, the low rate has been suggested that CD4 cells play a role in inducing or perpetuating tissue and epithelial damage that may facilitate H. pylori colonization (Bontems et al., 2003). Further studies suggested that decreased gastric acid secretion might be predisposed to gastric colonization by other microorganisms that might compete with H. pylori bacteria and the use of either antibiotics or proton pump inhibitors in the low count of CD4+ cells in HIV patients my decreases colonization of H. pylori (Panos et al., 2007; Nevin et al., 2014).
This study showed that 2.3% of participants with age ≤30 years were infected with H. pylori, and this was lower than study report from Nigeria with similar age group, (Anejo-Okopi et al., 2016).
In addition, the current study indicated that the presence of dyspepsia was found to have a significant association with H. pylori infection. It in line with the study reported by Anejo-Okopi et al. (2016) that indicated that dyspepsia was associated with H. pylori infection. Furthermore, the association of H. pylori with dyspepsia condition has triggered a major paradigm change in patients’ management (Jemilohun et al., 2011).
The present study revealed that no association in between hemoglobin level and H. pylori infection. This in line with the study conducted by Fraser et al., 2010 and Kermati et al., 2007. However, one study from Turkish teenager reported that association between H. pylori infection and anemia (Süoglu et al., 2007). This might be attributed to favors of poor hygienic status for parasitic infestation and sharing of a similar transmission route with H. pylori infection and the condition of co-morbidity might increase risks of anemia.
It was found that no association of H. pylori infection with CD4+ cells. In support, different studies depicted that CD4+ cells has been shown to be raised in H. pylori gastritis, but gastric inflammation has been correlated with lower H. pylori bacteria load, and pro-inflammatory genetic profiles are associated to lower H. pylori sero-prevalence. Besides, H. pylori infection requires an intact mucosal cellular immunity, and that the loss of the CD4+ cell population in the gastric mucosa may prevent H. pylori persistence (Sarfo et al., 2015; Aebischer et al., 2010).
In this study, there is association of H. pylori infection with age less than or equal to 30 years of participants and this in line with the other studies report (Anejo-Okopi et al., 2016; Abebaw et al., 2014; Chen et al., 2013). Furthermore, current study showed that no significant association in the prevalence of H. pylori infection with family size, educational status, marital status, alcohol consumption, residence and occupation.
Limitations of the study
This study was conducted on HIV patients who had many underline disease conditions as a confounding factor that was not completely controlled, so as to have impact on the outcome of the statistical associations between H. pylori infection and different variables of interest. The other limitations were Immuno-chromatographic stool antigen test characteristics, (non-ELISA method), lack of HIV negative controls and cross sectional nature of the study that did not show cause and effect relationship between the variables.
CONCLUSION
The overall prevalence of H. pylori infection in the study participants was 17.9%. About 42.6% of the participants had a history of dyspepsia and of them, 4.3% were positive for H. pylori infection. In addition, having a history of dyspepsia and age ≤30 years were associated factors of H. pylori infection. HIV-positive subjects receiving ART co-infected with H. pylori tend to have higher levels of CD4+ T-lymphocytes (>200 cells/µl) when compared to patients withCD4+ T-lymphocytes <200 cells/µl and patients with low immune status, reflected by CD4+ T-lymphocyte levels below 200 cells/μl, are less probable to be infected with H. pylori. Moreover, dyspepsia in HIV-positive patients suggests the need to investigate alternative etiologies, besides H. pylori infection. In addition, this study indicated the need for further large-scale study in HIV patients to determine the possible factors for infection. Furthermore, cohort type studies are recommended to formulate a cause and effect relationship between associated factors and H. pylori infection among HIV infected patients.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGEMENTS
The authors appreciate ART clinic nurses for their endless support throughout the data collection. They also acknowledge the Hawassa University comprehensive specialized hospital laboratory for materials support and people living with HIV for their voluntary participation.
REFERENCES
|
Abebaw W, Kibret M, Abera B (2014). Prevalence and Risk Factors of H. pylori from Dyspeptic Patients in Northwest Ethiopia: A Hospital Based Cross-sectional Study. Asian Pacific Journal of Cancer Prevention 15(11):4459-4463. |
|
|
Aebischer T, Meyer TF, Andersen LP (2010). Inflammation, immunity, and vaccines for Helicobacter. Helicobacter 15:21-28. |
|
|
Anejo-Okopi AJ, Audu O, Adaiche AR, Okojokwu OJ, Ali M, Adekwu A, et al (2016). Prevalence of Helicobacter Pylori Infection among HIV-1 Infected patients using Stool Antigen Tests in Jos, North-Central, Nigeria. Govares 21:55-63. |
|
|
Bontems P, Fabienne R, Van Gossum A, Cadranel S, Mascart F (2003): Helicobacter pylori modulation of gastric and duodenal mucosal T cell cytokine secretions in children compared with adults. Helicobacter 8:216-226. |
|
|
Chen S, Ying L, Kong M, Zhang Y, Li Y (2013). The Prevalence of Helicobacter pylori Infection Decreases with Older Age in Atrophic Gastritis. Gastroenterology Research and Practice 2013:494783. |
|
|
Ejilude O, Akinduti PA, Idowu M, Ogunbileje JO, Akinbo JA (2011). HIV and Helicobacter Pylori Co- Infection in Dyspeptic Patients In Abeokuta, Nigeria. ew York Science Journal 4(9):1-5. |
|
|
Fialho AB, Braga-Neto MB, Guerra EJ, Fialho AM, Fernandes KC, Sun JL, Braga LL (2011). Low prevalence of H. pylori infection in HIV-positive patients in the northeast of Brazil. BMC Gastroenterology 11(1):13. |
|
|
Fraser AG, Scragg R, Schaaf D, Metcalf P, Grant CC (2010): Helicobacter pylori infection and iron deficiency in teenage females in New Zealand. New Zealand Medical Journal 123:38-45. |
|
|
Frenck WR, Clemens J (2003). Helicobacter in the developing world. Microbes and infection 5(8):705-713. |
|
|
Jemilohun AC, Otegbayo JA, Ola SO, Oluwasola AO, Akere A (2011). Diagnostic accuracy of rapid urease test for the diagnosis of Helicobactor pylori in gastric biopsies in Nigerians with dyspepsia. African Journal of Clinical and Experimental Microbiology 12:62-66. |
|
|
Kafil HS, Jahromi FF, Hajikhani B, Pirayeh SN, Aghazadeh M (2011). Screening for the presence of Helicobacter pylori in stool of HIV- positive patients. Journal of AIDS and HIV Research 3:85-87. |
|
|
Kermati MR, Siadat Z, Mahmoudi M (2007). The correlation between H pylori infection with serum ferritin concentration and iron deficiency anemia. International Journal of Hematology and Oncology 27(4):016-020. |
|
|
Khamri W, Walker MM, Clark P, Atherton JC, Thursz MR, Bamford KB, Lombardi G (2010). Helicobacter pylori stimulates dendritic cells to induce interleukin17expression from CD4+ T lymphocytes. Infection and immunity 78(2): 845-853. |
|
|
Lepper PM, Moricke A, Vogt K, Bode G, Trautmann M (2004). Comparison of different criteria for interpretation of immunoglobulin G immunoblotting results for diagnosis of Helicobacter pylori infection. Clinical and Diagnostic Laboratory Immunology 11(3):569-576. |
|
|
Marshall B, Adams CP (2008). Helicobacter pylori: A Nobel pursuit? Canadian Journal of Gastroenterology and Hepatology 22(11):895-896. |
|
|
Mitchell P, Germain C, Fiori PL, Khamri W, Foster GR, Ghosh S, et al (2007). Chronic exposure to Helicobacter pylori impairs dendritic cell function and inhibits Th1 development. Infection and immunity 75:810-819. |
|
|
Mynepalli CKS, Maureen O, Mumuni A (2014). Prevalence of Helicobacter pylori and hygiene practices among public secondary school students in Ikeja Local Government Area, Lagos, Nigeria. Journal of Health 6:250-258. |
|
|
Nevin DT, Morgan CJ, Graham DY, Genta RM (2014). Helicobacter pylori Gastritis in HIV-Infected Patients: A review. Helicobacter 19:323-329. |
|
|
Nkuize M, Dewit S, Muls V, Arvanitakis M, Buset M (2010). Upper gastrointestinal endoscopic findings in the era of highly active antiretroviral therapy. HIV Medical 11:412-417. |
|
|
Ostrow B (2010) Peptic Ulcer Disease-the impact of Helicobacter pylori on management in the developing world. Surgery in Africa Monthly Review. |
|
|
Palella Jr FJ, Delaney KM, Moorman AC, Loveless MO, Fuhrer J, Satten GA, HIV Outpatient Study Investigators (1998). Declining morbidity and mortality among patients with advanced human immunodeficiency virus infection. New England Journal of Medicine, 338(13):853-860. |
|
|
Panos GZ, Xirouchakis E, Tzias V, Charatsis G, Bliziotis IA, Doulgeroglou V, Falagas ME (2007). Helicobacter pylori infection in symptomatic HIV-seropositive and-seronegative patients: A case–control study. AIDS Research and Human Retroviruses 23(5):709-712. |
|
|
Perry S, De La Luz Sanchez M, Yang S, Haggerty TD, Hurst P, Perez-Perez G, Parsonnet J (2006). Gastroenteritis and transmission of Helicobacter pylori infection in households. Emerging Infectious Diseases 12(11):1701. |
|
|
Sarfo FS, Eberhardt KA, Dompreh A, Kuffour EO, Soltau M, Schachscheider M, Bedu-Addo G (2015). Helicobacter pylori infection is associated with higher CD4 T cell counts and lower HIV-1 viral loads in ART-naïve HIV-positive patients in Ghana. PloS one, 10(11):e0143388. |
|
|
Süoglu OD, Gökçe S, Saglam AT, Sökücü S, Saner G (2007). Association of Helicobacter pylori infection with gastroduodenal disease, epidemiologic factors and iron-deficiency anemia in Turkish children undergoing endoscopy, and impact on growth. Pediatrics International 49(6):858-863. |
|
|
Teka B, Gebre-Selassie S, Abebe T (2015). Sero - Prevalence of Helicobacter Pylori in HIV Positive Patients and HIV Negative Controls in St. Paul's General Specialized Hospital, Addis Ababa, Ethiopia. Science Journal of Public Health 4:387-393. |
|
|
Versalovic J (2003). Helicobacter pylori Pathology and Diagnostic Strategies. American Journal of Clinical Pathology 119(3):403-412. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


