Full Length Research Paper

ABSTRACT
Hepatitis B virus (HBV) coinfection with HIV is becoming a major challenge in developing countries, including Ethiopia. The problem has not received adequate attention by researchers since the introduction of antiretroviral treatment. This study aims to determine the magnitude of coinfection and identify factors associated with it between ARV-exposed and ARV- naive individuals. Comparative cross-sectional study was conducted among HIV/AIDS clients. Data were gathered from 760 patients. HBV infection was confirmed using hepatitis B surface antigen (HBsAg) tests. Logistic regression analysis was carried out to identify determinant factors using statiscal package for social sciences (SPSS) Version 18. The prevalence of HBsAg was 3.9% irrespective of treatment status; 5.3 and 2.6% among ARV-exposed and naive individuals, respectively. Men had higher risk of developing HBV infection than women. In ARV-naive individuals, HBsAg sero-prevalence was correlated with poor CD4 cell recovery and previous TB treatment. Moreover, male sex with previous liver disease were risk factors for HBsAg positivity in ARV-exposed individuals. The magnitude of HBV infection among HIV- infected individuals was high among treatment exposed individuals. High HBsAg positivity among ARV-exposed individuals warrants molecular studies to determine the real cause thereby guide future treatment approaches.
Key words: active antiretroviral treatment (HAART), HBsAg, HBV/HIV co-infection, ARV-exposed, ARV-naive.
INTRODUCTION
Since the introduction of highly active antiretroviral treatment (HAART) for treatment of HIV infection, morbidity and mortality have decreased. But the management of other HIV-associated chronic diseases, including hepatitis B coinfection, has become increasingly important (Levy and Robert, 2006; WHO, 2006). HBV is the leading cause of chronic liver disease and liver-related deaths worldwide, with the majority of these cases occurring in Africa and Asia, where HBV prevalence is higher than 8% (Hoffmann and Thio, 2007; Mauss et al., 2009). Worldwide, 90% of HIV-infected persons have biological signs of prior HBV infection (defined by the presence of serum anti-HBcAb) and 5 to 15% suffer from chronic infection (defined by detection of serum HBsAg) (Alter, 2006; Lacombe et al., 2010).
An estimated 2 to 4 million of the 34 million people living with HIV globally are co-infected with HBV (Lacombe et al., 2010; Lacombe and Rockstroh, 2012). Conditions associated with hepatitis B and C are currently among the leading causes of hospital admission, and recent studies have shown increasing rates of liver disease and related death among people infected with HIV (Kenneth et al., 2007). Infection with HIV and HBV are often found in the same individual because of shared routes of transmission (mostly sexual intercourse in adolescents and adults) (Hoffmann and Thio, 2007). Many of the countries with a high HBV disease burden are also highly affected by HIV, resulting in frequent HIV/HBV coinfection (Lacombe et al., 2010). The introduction of HAART has led to the emergence of HBV liver related disease and mortality as HBV infection increases HAART related hepatotoxicity (Puoti et al., 2002; Peters, 2007; Easterbrook et al., 2013).
Despite these mounting challenges, there is limited information regarding the prevalence, physiopathology and associated factors of coinfection with HBV amongst HIV-positive individuals in Africa, a continent where more than 23.6 to 26.8 million of the world’s 35.3million HIV infected individuals live in 2012 (UNAIDS, 2013; WHO, 2013). In Ethiopia, previous population surveys have reported medium to high endemicity of HBV infection (Tesga et al., 1986; Abebe et al., 2003; Techalew et al., 2008). However, the magnitude of the infection in different risk groups, including people living with HIV/AIDS before and during antiretroviral therapy is understudied (Techalew et al., 2008). There is a clear gap in explaining the natural history of HIV/HBV coinfection, magnitude, its effect on immune recovery as well as drug related hepatotoxicity, after long term HAART. Therefore, this study intended to determine the magnitude of HIV/HBV coinfection and factors affecting treatment outcomes among HIV/AIDS patients after Ethiopia introduced lamivudin based regimens for over five years.
MATERIALS AND METHODS
Ethical clearance was obtained from the Institutional Ethical Review Committee of Debre Berhan University. Both oral and written consent was obtained based on interest and educational status from each participant once the purpose, confidentiality, protection and anonymity of data for this study were explained to each individual.
Study area, design and population
The study was conducted in North Shewa Zone of Amhara Region in Ethiopia. The zone was estimated to have a total population of 1,907,392 in 2009 (BoFED, 2009). At the time of the study, the zone had three hospitals and 72 health centers. The study was carried out in one public hospital (Debre Berhan Referral Hospital) and six health centers (Shewa Robit, Debre Sina, Mendida, Deneba, Enewary and Debre Berhan) that deliver care and treatment services for HIV- infected individuals. All facilities, including Debre Berhan Referral Hospital, were randomly selected. The study took place from January to December, 2011. HIV/AIDS clients were selected according to their exposure status to antiretroviral treatment. Patients were divided into two groups: “ARV-exposed”, which included all HIV-positive individuals who were on HAART for at least three months, and “ARV naive”, HIV- positive individuals on pre-ART follow-up (who had not yet started HAART treatment) (WHO, 2013). The initiation of ART was based on the eligibility criteria based on CD4 cell counts. All HIV-infected individuals over the age of 15 years visiting the selected health institutions for HAART or pre-ART follow-up services were considered as the source population. HIV- infected individuals with less than three months follow- up and less than 15 years old were not included in the analysis
Sample size determination
The sample consisted of 760 HIV-infected individuals who visited the seven selected institutions during the data collection period. The sample size was calculated using two population proportion formulas based on the following assumptions: the proportion of HIV infected individuals receiving HAART with chronic HBV infection was 9% (Hoffmann and Thio, 2007); the proportion of HIV infected individuals not yet exposed to HAART with chronic HBV infection was 14% (Hoffmann and Thio, 2007); a standard score corres-ponding to 95% certainty, power of 80%, and the ratio of exposed to non- exposed was one to one.
Data collection
Socio-demographic data were collected from the study participants using a pretested structured questionnaire, supplemented by information gathered on patient intake forms and medical record review. All surveys and intake forms were administered by health professionals. Additional clinical data, including baseline and mean CD4 cell counts, mean alanine trans-aminase (ALT), aspartate transaminase (AST) values, type of first line regimens started, adverse reactions to antiretroviral (ARV) drug experienced, and duration of ART treatment were taken from follow-up forms included in the patients' clinical folders. Blood samples were collected from each study participant with standard operational procedure after informed consent was obtained. Serological tests for determining HBV infection were done using SD HBsAg rapid test kit (SD Company, Korea) at Debre Berhan Referral Hospital, and positive results were confirmed with HBV confirmatory reagent AxSYMHBsAg (Abbott AXSYM System, Abbot Diagnostic Division, Germany) according to the manufacturer’s instructions.
Data analysis
Data were checked for completeness and entered using Epi Info 3.5 software and analysed using SPSS version 18. Both descriptive and analytical statistical procedures were employed. Univariate, bivariate and multivariate logistic regressions with odds ratio along with the 95% confidence interval were used to examine the association between covariates and dependant variables. Pearson's chi- square tests and odds ratio (OR) were used to assess the relationship between HIV/AIDS patient characteristics and HBsAg sero status. The Cornfield Approximation was used for calculating the 95% confidence intervals (CI) for the OR. Logistic regression analysis was carried out to determine the adjusted effect of each factor on the HBsAg sero status. Variables with more than two categories were entered into the model in the form of two "indicator" contrasts comparing each category to the first group as reference. A backward stepwise procedure based on the likelihood ratio was used to select the variables included in the final model. The significance for variable removal and entry was set to 0.10 and 0.05, respectively. The Hosmer and Lemeshow test was used to check the goodness-of-fit of the model. Only covariates that were statistically significant at the bivariate level were included in the multivariate binary logistic regression to control confounding. Odds ratios and 95% confidence intervals were derived from each variable coefficient in the final model. The significance of each coefficient was tested by the Wald test.
RESULTS
Socio-demographic and clinical characteristics of study population
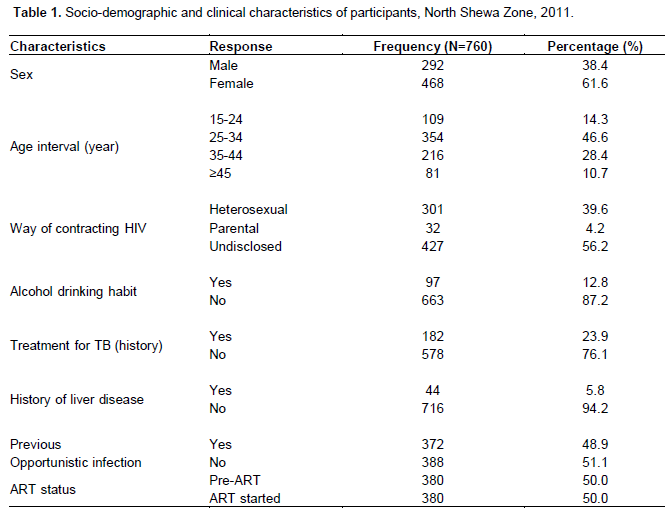
A total of 760 HIV-positive adults were included in this study. From the sample, 468 (61.6%) were women, 605 (79.6%) were considered urban, and 354 (46.6%) of participants were between the ages of 25 to 34 years. 40% of the participants did not have a secure source of income. Only 16.1% were employed and working at the time of the study (Table 1). 93% of study participants lived with HIV for up to five years, and 56.2% refused to disclose how they contracted HIV. From those who disclosed the mode of infection, hetero-sexual intercourse was reported by 301 (39.6%) individuals. Nearly a fourth (182, 23.9%) had been treated for TB after being enrolled in the care and treatment follow- up meaning one out of five HIV-infected individuals developed pulmonary tuberculosis. According to their medical history, 372 (48.9%) individuals developed opportunistic infections of which 132 (35.1%) cases were pulmonary tuberculosis; 44.9% of the patients developed oral candidiasis, herpes zoster and/or diarrhoea.
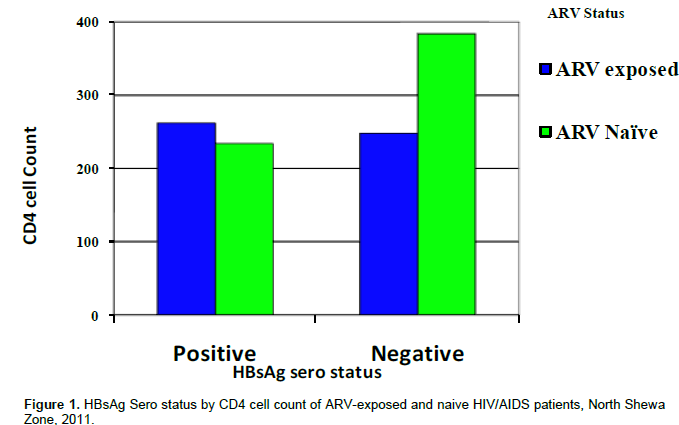
Clinical characteristics of ARV-naive and experienced HIV infected individuals
Of the 380 (50%) ARV-naive HIV infected individuals included in this study, 359 had CD4 cell count records. Of these 172 (46.6%) had CD4 cell counts ≥350 cells/mm3 (Figure 1). On average, 206 (54.2%) of them were enrolled in chronic care for up to 6 months, 42 (11.1%) for 7 to 12 months, 60 (15.7%) for 13 to 24 months and 72 (18.9%) for more than 24 months. In the ARV-exposed group, we included 380 patients who were on treatment, on average, for 28 months (SD±17.4). Two-hundred (52.6%) had been on ART for ≥24 months and 17.6% of individuals started ART at a very low baseline CD4 cell count (<50cells/mm3), while 40% started at the right time with a baseline CD4 cell count of 101 to 200 cells/mm3. The CD4 cell counts of the respective participants for the duration of initiated ART showed that 151 (39.7%) had a CD4 cell count ranging from 201 to 350 cells/mm3 (Figure 1). At the beginning of the study, 99 (26.0%), 89 (23.4%), 168 (44.2%), and 24 (6.3%) individuals were at WHO HIV/AIDS stages I, II, III, and IV, respectively. Three-hundred-forty-seven (91.3%) were actively working in their usual occupations (mostly farming and other physical labor). The follow-up records showed that 93.2% of them had good adherence to their respective prescribed ARV regimen. Of the 380 ARV-exposed individuals, liver function test results were found for only 119 (31.3%) patients. ALT/AST measurements were used to evaluate liver function. Accordingly, ALT/AST levels for the patients were 11 to 40 U/L (64.4 %), 41 to 7 0U/L (28%), and ≥7 1U/L (7.6%). All 380 ART-exposed patients had been on first line antiretroviral regimens; 29.7% started with 1a regimen, a combined ARV containing stavudine (d4t), lamivudine (3TC), NRTIs and nevirapine (NVP), a NNRTI, and 88 (23.2%) had started with 1c regimen, which differs from 1a by including zidovudin (AZT) instead of d4t. During their course of treatment, 52 (13.7%) patients had been forced to substitute the first regimen drug, mainly due to toxicity or side effects (82.7%).
Prevalence of HBV and associated factors among ARV-naive and experienced HIV infected individuals
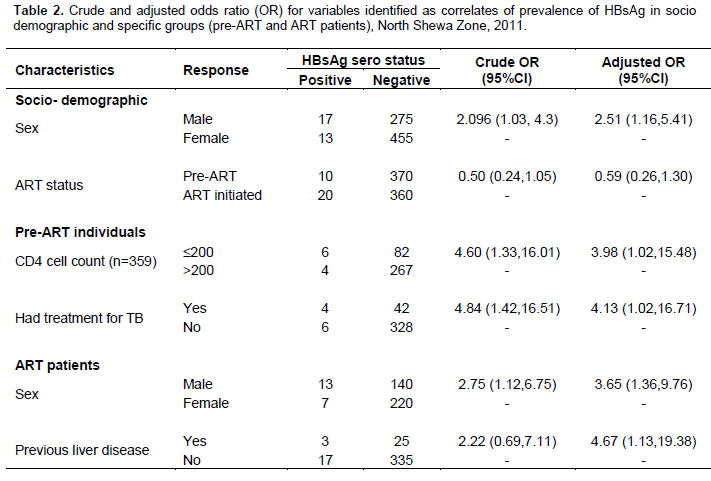
The cumulative prevalence of HBsAg was found to be 3.9% (5.8% in men, 2.8% in women, P=0.02) The prevalence among men was different, 7.1 and 9.5% in the age groups of 25 to 34 years and 35 to 45years, respectively (P<0.05) For women in the same age group the prevalence rates were 2.9 and 3.8%, respectively. HBsAg positivity in ARV-naive and exposed individuals were 5.3 and 2.6%, respectively, but the difference was not significant (P=0.06).
Factors associated with the prevalence of HBV among ARV-naive and experienced individuals
The multivariate analysis for ARV-naive participants showed that only previous treatment for tuberculosis (AOR=4.13;95%CI: 1.02, 16.71) and immune recovery (CD4 count ) (AOR=3.98;95%CI: 1.02, 15.48) were associated with HBsAg sero-prevalence. In cases of ARV-exposed individuals, the odds of having HBV were 2.5 times more common among men than women (AOR=2.5; 95%CI: 11.2, 5.4), and 4.6 times higher in patients with previous history of liver disease (AOR=4.67; 95%CI:1.13,19.38). However, there was no association by WHO stage classification (OR=2.00; 95%CI: 0.74, 5.46), INH prophylaxis and treatment for TB (Table 2).
DISCUSSION
In this study, half of the participants developed opportunistic infections, and pulmonary tuberculosis (23.9%) was the most common of these infections. This is consistent with previous studies and government reports for Ethiopia, which reflect a 20 to 50% HIV/TB coinfection prevalence in the country (Datiko et al., 2008; MOH, 2008). After 12 months of follow- up, 46.6% of ARV-naive HIV infected participants had an average CD4 cell count of ≥350 cells/mm3, while half of the individuals were ARV-exposed for more than two years. According to the WHO, two years is considered an adequate period of follow-up for evaluating anti viral responses and factors related with ARV treatments including immune recovery and hepatotoxicity. WHO considers the first six months on ART as critical during which time clinical and immunological improvement are expected and should manifest (WHO, 2006). In this study, 38% of the individuals started ART at CD4 cell counts below 100 cells/mm3, of which 18% started below a critical level of 50 cells/mm3. It is reported that starting ART at a low CD4 cell count, less than 50cells/mm3, impairs effectiveness of treatment and results in poor immune recovery, and in most cases even in treatment of failure and death (WHO, 2006; Mascolini, 2010; Wilkin, 2010).
Prevalence of HBV/HIV coinfection among HIV/AIDS patients
Based on this study, the cumulative prevalence of HBV in HIV-infected adults was 3.9%. This implied that 3.9% of HIV infected adults have persistence of HBsAg with or without replicative hepatitis B, which is consistent with the findings of previous studies on HBV infection rates in Addis Ababa, Ethiopia (Duncan et al., 1995; Awole and Gebre, 2005; Techalew et al., 2008), and pregnant women in Jimma, Ethiopia (3.7% HBsAg) (Awole and Gebre, 2005). However, this prevalence was different from a cross-sectional household study done in Addis Ababa, which reflected a 6.2% coinfection rate in the general population (Abebe et al., 2003). The higher occurrence of occult HBV infection in HIV-positive people may be attributed to the slightly lower rate of HBsAg in HIV-infected populations in general and ARV-naive individuals in particular (Burnett et al., 2005). In addition to differences in methodological approaches, in the above household study, 38% of the prevalence was attributed to the age group less than 15 years old, an age cohort excluded from the current study. HIV/HBV coinfection was associated with gender and age.
Gender
Men were 2.5 times more likely to be exposed to HBV infected than women; similar to studies in the United States and Addis Ababa, which reported six-times and 1.5-times higher risk in men, respectively (Martinez et al., 2001; Techalew et al., 2008 ). Although, the reason for higher risk among men is unclear, it may be due in part to greater exposure to HBV during childhood (Abebe et al., 2003; Techalew et al., 2008), among men or genetic predisposition, which warrants further studies.
Age
The rate of HBsAg sero-positivity increased with age, and was higher in the age groups 25 to 34 (4.3%) and 35 to 45 (6.3%), which accounted for 93% of the HBV infected patients and were higher than the cumulative prevalence of all study participants. Similar research from Kenya also identified increased age as a significant predictor of HIV/HBV coinfection (P<0.04) (Puoti et al., 2002). This may be due to the increased risk of exposure or presentation of HBV infection and HBsAg with time. In addition, infection contracted at an early age may lie dormant initially, and become active at a later age (due to immune suppression in HIV/AIDS or immuno-suppressive drugs) (Mauss et al., 2013).
HIV/HBV coinfection among specific groups; ARV-naive and exposed participants
In the current study, the prevalence of HBsAg was 5.3% in ARV-exposed and 2.6% in ARV-naive individuals. The prevalence among ARV-exposed individuals was comparable with the general population (6.2%) (Abebe et al., 2003). The finding was consistent with a study done in Thailand, where a chronic HBV prevalence of 8.7 and 5 to 10% were reported among patients receiving ART and in the general population, respectively (Hoffmann and Thio, 2007).
The HBV prevalence reported here was higher among the ARV-exposed group than naive ones. HBsAg positivity rate was lower among ARV-naive HIV-infected participants as compared to those exposed to treatment, which contrasted with rates reported in another study done in Addis Ababa (2.9 versus 4.5%) (Techalew et al., 2008). The difference might be attributed to the small sample size (N=305) as well as involvement of patients who were on ART for short duration in the previous study (Techalew et al., 2008). In the other way, we believe that the high prevalence observed in the ARV-exposed group could suggest presence or occurrence of drug resistance against lamivudine, a dually effective drug included in all ART regimens currently being given for all eligible individuals. As we discussed elsewhere, high HBsAg positivity across older age (25 to 34 years and 35 to 45years) and among patients on lamivudine-tenofovir (3TC-TDF) combination regimen than in any other regimen strengthens such claims. It is well known that the presence of lamivudine as part of the combination therapy in HAART halts multiplication of HBV (WHO, 2006; Techalew et al., 2008; Mauss et al., 2013).
However, previous studies showed that a nucleoside anti-HBV drug like lamivudine requires long-term treatment to achieve HBsAg clearance or sero conver-sion to anti- HBsAg. After a short term, treatment clearance could be achieved only in <5% of patients (Mauss et al., 2013). So if complete, suppression was not achieved during treatment, resistance commences rather quickly. Furthermore, within the first year of treatment, 20% of patients on lamivudine may develop mutation resulting in loss of effectiveness against HBV (Chang et al., 2005) and virologic breakthrough (Mauss et al., 2009; Kim et al., 2011). HIV might also reduce efficacy of anti-HBV therapy, including the risk of lamivudine resistance and decreased response to interferon α (Peters, 2007). In the current study, ARV-exposed participants had been taking treatment for an average of 28 months (more than two years) during which time mutant strains might emerge. Another study also reported the incidence of HBV resistance to be 24 to 30%, after lamivudine based treatment for two years (Puoti et al., 2002; Mauss et al., 2009; Plaza et al., 2013). In contrast, the increased prevalence we reported could be the result of HBeAg sero-conversion to anti-HBeAg and the subsequent suppression of HBV replication by anti-retroviral like lamivudine. In these patients, HBsAg remains detectable and transaminases are within normal range (Mauss et al., 2013). For this reason, the levels of HBV DNA and HBeAg should be determined to identify the actual cause.
In the other way, the low prevalence seen in ARV-naive HIV infected individuals may also be due to presence of occult HBV infection in which simultaneous infection with HIV reduces immune control of previous HBV infection, facilitating inactive HBV reactivation and HBV DNA replication without presence of detectable HBsAg (Soriano et al., 2008).
Risk factors for HBV infection in specific groups; ARV-Naive and experienced participants previous history of liver disease
In ARV-exposed individuals, previous liver disease was found to be a strong predictor of HBsAg positivity (AOR=4.67; 95%CI: 1.13, 19.38). This implied that such individuals could be chronic carriers of HBV with increased risk of HBV replication and progression to end stage liver disease, liver cirrhosis and hepatocellular carcinoma if immune recovery by ARVs becomes in-complete (Mauss et al., 2013). Male sex was another risk factor for increased HBsAg positivity (AOR=3.65; 95%CI: 1.36, 9.76) in this group. Possible reasons for this have been described above.
CD4 cell count
In this study, the relationship between CD4 cell count and HBsAg sero-positivity was also assessed in the two specific study groups. In ARV-naive individuals, a lower rate of CD4 cell recovery was recorded for HBsAg-positive individuals (P=0.04). In those individuals, poor immune recovery was risk factor HBsAg positivity (AOR=3.98; 95%CI: 1.02, 15.48). Previous studies also reported that HBV infection independently reduced CD4 cell recovery (Puoti et al., 2002; Peters, 2007). In ART-initiated individuals, though a slight increase in mean CD4 cell count was observed in HBsAg sero-positive individuals, the difference was not significant (P>0.05). The result was similar to the study of Chang and colleagues who found HBV to have no effect on CD4 cell loss after initiation of ART (Chang et al., 2005). Other cohort studies in Thailand and Nigeria also showed that CD4 lymphocyte increments were similar regardless of hepatitis B status (Puoti et al., 2002; Hoffmann and Thio, 2007; Crane et al., 2010). The repression of HBV effect on CD4 recovery after initiation of ART could be the result of treatment boosting immunity and consequently activation by the HBV suppressive action.
In the current study, contrary to previous thoughts on the effect of lamivudine on HBV clearance, the type of first line regimen (with or without tenofovir) lacked association with HBsAg positivity (P=0.28), another evidence for possible development of HBV drug resistance among study participants. In addition, though only 25 (6%) of the ART-exposed patients were taking a tenofovir-lamivudine combined regimen, they accounted for 10% of HBsAg-positive individuals, a higher proportion than any other regimen. As we noted previously, this combination therapy containing tenofovir and lamivudine as part of combination anti-retroviral treatment is superior in terms of HBV DNA suppression to tenofovir or lamivudine administered separately (Nunez et al., 2001; Levy and Robert, 2006; Hoffmann and Thio, 2007; Crane et al., 2010).
In summary, the development of viral resistance to polymerase inhibitors like lamivudine and tenofovir may result in rapid replication of HBV and development of end stage liver disease in ART- exposed HIV/HBV co-infected individuals. In accordance with this, we reported high HBV infection among ARV-experienced individuals; across older ages and regimens containing combination drugs as well as similar rates in regimens with and without tenofovir. This suggests that unless alternative treatment options are introduced, continuation of lamivudine may lead to the development of compensatory mutations that could potentially limit future treatment options
CONCLUSION
This study showed that in ARV-naive individuals, poor immune recovery and previous treatment for tuberculosis were correlated with HBsAg sero prevalence. Moreover, male sex and previous liver disease were independent predictors of HBsAg positivity in ART-initiated individuals. Based on the findings of this study, all HIV infected individuals need to be screened for HBV before initiating ART and Ethiopia ministry of health should incorporate routine HBV screening in ART treatment guidelines. Eligible HBsAg-positive patients (HBeAg positive, HBV DNA>2000IU/ml and positive liver fibrosis and elevated ALT level) should be treated according to WHO guidelines and screened for drug-resistant HBV mutant strains every six months. Non-eligible ones should also be checked every six months as part of the routine HIV follow-up. Furthermore, prospective studies should be conducted to determine the different factors associated with HIV/HBV co-infection and emergence of drug-resistant strains for currently available treatment regimens.
CONFLICT OF INTEREST
The authors have no conflicts of interest.
ACKNOWLEDGEMENT
The authors thank Debre Berhan Referral Hospital and International clinical laboratory staff for actively participating in data collection and Erin and Tony Portolio for reviewing the manuscript. This work was financially supported by Debre Berhan University.
REFERENCES
|
Abebe A, Nokes J, Dejene A, Enquselassie F, Messele T, Cutts FT (2003). Sero epidemiology of hepatitis B virus in Addis Ababa, Ethiopia: transmission patterns and vaccine control. Epidemiol. Infect. 131: 757-770. Crossref |
||||
|
Alter M (2006). Epidemiology of hepatitis virus and HIV co-infection. J. Hepatol. 44:56-59. Crossref |
||||
|
Awole M, Gebre SS (2005). Seroprevalence of HBsAg and its risk factors among pregnant women in Jimma, Southwest Ethiopia. Ethiop. J. Health Dev. 19:45-50. Crossref |
||||
| BoFED (2009). The population report of Amhara region by zone: Reports for North ShoaZone. Amhara National Regional State Bureau of Finance and Economic Development, Bahirdar. | ||||
|
Burnett RJ, Francois G, Kew M (2005). Hepatitis B virus and human immunodeficiency virus co-infection in sub-Saharan Africa: a call for further investigation. Liver Int. 25:201-24. Crossref |
||||
|
Chang JJ, Wightman F, Bartholomeusz A (2005). Reduced hepatitis B virus (HBV)-specific CD4-T-cell responses in Human Immunodeficiency Virus type 1-HBV- co infected individuals receiving HBV-active antiretroviral therapy. J. Virol. 79(5):3038-3051. Crossref |
||||
|
Crane M, Sirivichayakul S, Chang JJ (2010). No increase in hepatitis B virus (HBV) specific CD8-T cells in patients with HIV-1-HBV co-infections following HBV-active HAART. J. Virol. 84(6):2657-2665. Crossref |
||||
|
Datiko DG, Yassin MA, Chekol LT, Kabeto LE, Lindtjorn B (2008). The rate of TB-HIV co-infection depends on the prevalence of HIV infection in a community. BMC Public Health 8:266. Crossref |
||||
| Duncan M, Tibaus G, Pelzer A (1995). Prevalence and significance of sexually transmitted diseases among women attending clinics in Addis Ababa. Ethiop. J. Health Dev. 9:31-40. | ||||
| Easterbrook P, Sands A, Harmanci H (2013). Challenges and priorities in the management of HIV/HBV and HIV/HCV co-infection in resource-limited areas. Semin. Liver Dis. 32:147-157. | ||||
|
Hoffmann CJ, Thio CL (2007). Clinical implications of HIV and hepatitis B co-infection in Asia and Africa. Lancet Infect. Dis. 7(6):402-409. Crossref |
||||
|
Kenneth S, Marion P, Margaret K (2007). HIV and Liver Disease Forum: Conference Proceedings. Hepatology 45:1566-1577. Crossref |
||||
|
Kim HN, Scott J, Cent A, Cook L, Morrow RA, Richardson B, Tapia K, Jerome KR, Lule G, John-Stewart G, Chung MH (2011). HBV lamivudine resistance among hepatitis B and HIV co-infected patients starting lamivudine, stavudine and nevirapine in Kenya. J. Viral Hepat. 18:e447-e452. Crossref |
||||
|
Lacombe K, Bottero J, Lemoine M, Boyd A, Girard PM (2010). HIV/HBV co-infection: current challenges and new strategies. J. Antimicrob. Chemother. 65:10-17. Crossref |
||||
|
Lacombe K, Rockstroh J (2012). HIV and viral hepatitis co-infections: advances and challenges. Gut:i47-i48 Crossref |
||||
|
Levy V, Robert M (2006). Antiretroviral therapy for hepatitis B virus-HIV co-infected patients: promises and pitfalls. Clin. Infect. Dis. 43:904-910. Crossref |
||||
|
Martinez E, Blanco G, Arnaiz A (2001). Hepatotoxicity in HIV1 infected patients receiving nevirapine-containing antiretroviral therapy. AIDS 15:1261-8. Crossref |
||||
| Mascolini M (2010). Older age, lower CD4 nadir, NNRTI uses predict slow CD4 recovery in Athena. 17th Conference on Retroviruses and Opportunistic Infections, San Francisco CA. | ||||
|
Mauss S, Berg T, Rockstroh J, Sarrazin C, Wedemeyer H (2009). Hepatology: A clinical textbook. 1st ed. Flying Publisher: Dűsseldorf, Germany. p. 467. Crossref |
||||
|
Mauss S, Thomas B, Juergen R, Christoph S, Heiner W (2013). Hepatology: A Clinical Textbook. 4th ed. Flying Publisher: Düsseldorf, Germany. p. 467. Crossref |
||||
| MOH (2008). Guidelines for management of opportunistic infections in adults and adolescents in Ethiopia. Federal HAPCO. Available: www.who.int/hiv/pub/guidelines/ethiopia_art.pdf | ||||
|
Nunez M, Lana R, Mendoza J (2001). Risk factors for severe hepatic injury after introduction of highly active antiretroviral therapy. J. AIDS 27:426-31. Crossref |
||||
|
Peters MG (2007). Diagnosis and management of hepatitis B virus and HIV co-infection. Top. HIV Med. 15(5):163-166. Pubmed |
||||
|
Plaza Z, Aguilera A, Mena A, Vispo E, Sierra-Enguita R, Tomé S, Pedreira J, Rodriguez C, Barreiro P, del Romero J, Soriano V, Poveda E (2013). Influence of HIV infection on response to tenofovir in patients with chronic hepatitis B. AIDS 27(14):2219-2224. Crossref |
||||
|
Puoti M, Airoldi M, Bruno R, Zanini B, Spinetti A, Pezzoli C, Patroni A, Castelli F, Sacchi P, Filice G, Carosi G (2002). Hepatitis B Virus co-infection in human immunodeficiency virus-infected subjects. AIDS Rev. 4:27-35. Pubmed |
||||
|
Soriano V, Puoti M, Peters M, Benhamou Y, Sulkowski M, Zoulim F, Mauss S, Rockstroh J (2008). Care of HIV patients with chronic hepatitis B: updated recommendations from the HIV-Hepatitis B Virus International Panel. AIDS 22(12):1399-1410. Crossref |
||||
| Tesga E, Mengesha B, Hanson BG (1986). Hepatitis A, B, and Delta infection in Ethiopia: a serologic survey with demographic data. Am. J. Epidemiol. 123:345-351. | ||||
| UNAIDS (2013). Access to Antiretroviral therapy in Africa: Status Report on Progress towards the 2015 targets. UNAIDS, Geneva. Available: http://www.unaids.org/sites/default/files/media_asset/20131219_AccessARTAfricaStatusReportProgresstowards2015Targets_en_0.pdf. | ||||
| Wilkin T (2010). What causes poor CD4-cell recovery in the setting of suppressive antiretroviral therapy? Journals Watch HIV/AIDS Clinical Care. Available from: http://www.jwatch.org/ac201004260000001/2010/04/26/what-causes-poor-cd4-cell-recovery-setting. | ||||
| World Health Organization (WHO) (2006). Antiretroviral Therapy for HIV Infection in Adults and Adolescents Recommendations for Public Health Approach: 2006-Revision. WHO, Geneva. 26. | ||||
| World Health Organization (WHO) (2013). Consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection: recommendations for a public health approach. Available: http://www.who.int/hiv/pub/guidelines/arv2013/en/index.html. | ||||
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


