Full Length Research Paper

ABSTRACT
Dual voices of women with human immunodeficiency virus (HIV) and acquired immune deficiency syndrome (AIDS) show the experiences of the HIV positive women who are ignored by the society at large. The study aims to showcase the voices of women living with HIV and AIDS at a micro-level to approach the disease in a more holistic way. Qualitative study was employed to explore and describe the experiences of women living with HIV and AIDS. The study area is a clinic in Gauteng Province of South Africa. A non-probability purposive sampling technique was used to select the study participants (n=12). In-depth, individual semi-structured interviews were conducted and thematic content approach was used for data analysis. Five themes were used to describe the women’s five experiences from being diagnosed with HIV: disclosing HIV positive status, signs and symptoms of HIV and AIDS, stigmatization, emotions and services being rendered. HIV and AIDS have negative effects on the women. They are looking for ways to cope with the disease. Women should be given enough support and health care. This can be done by providing enough consultation rooms, adequate waiting time, pre-counseling before given antiretroviral treatment (ART), engagement of male partners and relatives and addressing peer support and confidentiality.
Key words: Acquired immune deficiency syndrome (AIDS), experiences, human immunodeficiency virus (HIV), women.
INTRODUCTION
Worldwide, an estimated 17.8 million women were living with HIV in 2015 constituting 51% of all adults living with HIV (UNAIDS, 2015). To date, women constitute more than 50% of all people living with HIV (The Foundation for AIDS Research, 2015). In addition, AIDS-related conditions remain the leading causes of mortality for women of reproductive age (15-49 years), posing a huge public health threat that needs to be addressed.
There are many reported cases of harmful impacts and ‘socially complex’ outcomes, which resulted from the HIV/AIDS epidemic in South Africa. While some of these outcomes relate to structural issues, others stem from society’s attitudinal milieu and its attempts to cure the illness (Ogunmefun et al., 2011). A survey conducted by the Human Sciences Research Council (HSRC) of South Africa suggests that the incidence rates of HIV/AIDS among females remain a concern. In 2012, the number of new infections among adults of 15-49 years was 1.7 times higher in females than in men. The HIV incidence rate among female youths aged 15-24 is over four times greater than the incidence rate found in males of the same age group (Shisana et al., 2014).
Women living with HIV and AIDS (WLWHA) are at a particular high risk of living a painful, shameful life of exclusion. Their families, friends and partners have rejected them. In spite of the burden of disease, the world is paying less attention to issues raised by WLWHA. Their dual voices remain unheard and regarded as the latent sources of infections. They have captivated culpability and blame leading to a highly stigmatized and discriminated life. Despite this situation, women and their particular concerns in HIV/AIDS research literature are ignored (Paudel and Baral, 2015).
In 2016, South Africa had 270 000 (240 000-290 000) new HIV infections and 110 000 (88 000-140 000) AIDS-related deaths. The National Strategic Plan for HIV, tuberculosis (TB) and sexually transmitted infections (STIs) 2017-2022 aims to increase progress towards meeting the “Fast-Track” by decreasing new infections, improving treatment, care and support; reaching key and vulnerable populations; and addressing the social and structural drives of HIV, TB and STIs. Implementation plan throughout the nine provinces intervened. To address the high number of new HIV infections among young women and adolescent girls, a national prevention campaign called She Conquers was launched (UNAIDS, 2018). In 2017, an estimated 12.6% of the total population was HIV positive. Approximately one-fifth of South African women in their reproductive ages (15-49 years) were HIV positive (Statistics South Africa Mid-Year Population Estimates, 2017).
TB is one of the top causes of death worldwide caused by the bacterium (Mycobacterium tuberculosis) that most often affects the lungs. TB is curable and preventable. In 2017, 10 million people had TB, and 1.6 million died from the disease (including 0.3 million among people with HIV). TB is a leading killer of HIV positive people. Moreover, in 2017, 87% of new cases occurred in 30 high TB burden countries. Eight countries accounted for two thirds of the new TB cases namely: India, China, Indonesia, the Philippines, Pakistan, Nigeria, Bangladesh and South Africa (WHO Global Tuberculosis Report, 2018). The estimated overall HIV prevalence rate is approximately 13.15 among South African population. The total number of people living with HIV is estimated at approximately 7.52 million in 2018. For adult aged 15-49 years, an estimated 19.0% of the population is HIV positive (Statistics South Africa Mid-Year Population Estimates, 2018).
STIs are infections transmitted during unprotected sexual intercourse (both heterosexual and homosexual-anal, vaginal or oral). STIs, known since ancient times, remain major public health problems worldwide and were compounded by the appearance of HIV/AIDS around 1980. STIs may cause acute and chronic illness, infertility, long-term disability and death, with severe medical and psychological consequences for millions of men, women and children. Apart from being serious diseases in their own right, STIs increase the risk of contracting or transmitting HIV infection (WHO, 2018). This work aims to describe the experiences of women living with HIV and AIDS and make recommendations for policy makers to support women living with HIV and AIDS.
MATERIALS AND METHODS
Research design is the overall plan for addressing a research question (Appendix), including specifications to enhance the study’s integrity (Polit and Beck, 2012). Exploratory and descriptive research design based on qualitative approach was used. Experiences of women living with HIV and AIDS were explored and described to have a detailed picture of the extent of the problem and contribute to the body of knowledge in this important area of public health.
Study setting
The research was conducted at a clinic in Gauteng Province of South Africa. The researchers selected the health facility because it was the most convenient and accessible site to them. One of the researchers used facilities at the clinic occasionally and came across a number of women receiving HIV and AIDS treatment. This sparked the researchers’ interests to find more about the experiences of women living with HIV and AIDS. Moreover, the clinic has a well-established antiretroviral therapy (ART) site which serves many women living with HIV and AIDS.
Study population and sampling strategy
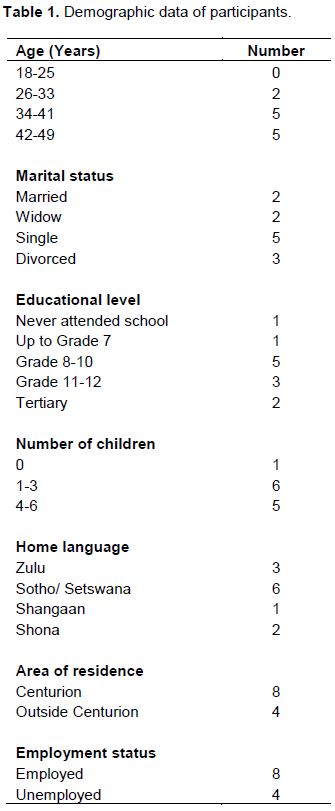
The research engaged a non-probability purposive sampling technique. The researchers selected a sample of HIV positive women between the ages of 18 and 49 years, who attend, get help and treatment at the clinic (Larry et al., 2011). Twelve participants were selected for intensive exploration and description of their experiences of living with HIV and AIDS. Gerish and Lacey (2010) state that the whole total population that forms the focus for the study is known as target population. HIV positive women attending the clinic constituted the study population. A sample was drawn as it was not possible to study the entire population of women living with HIV and AIDS. The final number of twelve participants interviewed was determined by the criterion called saturation of information, whereby a sense of closure was attained because new data yielded redundant information (Polit and Beck, 2012). The interviews lasted for 30 min to an h for each participant (Table 1).
Data collection and analysis
A pilot study was conducted one week prior to the main study. The purpose of the pilot study was to find out if participants would understand the purpose of the study, the interview questions, and if there were any amendments to be made prior to the data collection process. Two trial participants with the same inclusion characteristics were interviewed at the research area. The same participants were not included in the main study.
The researchers conducted in-depth individual semi-structured interviews as means of data collection. Green and Thorogood (2009) assert that in- depth interviews allow the interviewees enough time to develop their own accounts of the issues important to them. The in-depth interviews allowed the participants to express their experiences of living with HIV and AIDS. One researcher took the position of a facilitator to help participants talk freely. Open questions to seek clarification, illustration and further exploration were used (Balls, 2009). Interviews were recorded with a digital voice recorder exactly the same way it was done in the pilot study.
Follow-up prompts based on the initial response were used to generate further discussion. The interviews were conducted in a flexible and open-minded inquiry. One researcher took some field notes and at the same time recorded the interviews to refer to later during data analysis. Field notes were written in English, the same language used during the interviews. Data records were kept in a locked cabinet to which only the researchers had entry.
Data analysis is the description of what is done with data during and after data collection to obtain a clearer picture of what the information conveys to us (McNee and McCabe, 2008). The researchers used a thematic content analysis approach for data analysis. The process involved searching through data about the experiences of women living with HIV and AIDS as given by the study participants to identify any recurrent patterns. The process was done through data coding. Data coding is a process that involves reading, thinking about and labelling every piece of data in order to find it easily later in the analysis. Coding was undertaken so that portions of data about similar topics, ideas, actions or communication could be easily identified and compared (Griffiths, 2009).
The data were saved and labelled in accordance with each separate interview by indicating the participant and assigning them number as Clinic Participant 1 (CP-1). Participants’ details were anonymised at the data collection stage; therefore a specific participant could not be identified by name; only their label, CP-1 and their number were identifiable. The same way was used in labelling and saving the fields notes. Content thematic analysis consists of breaking down the messages in simple elements in order to code them according to thematic categories and to register their frequency (Krippendorff, 1980). Furthermore, Krippendorf defined content analysis as a technique that draws valid and repeatable inferences from the data to their context. The following are six phases of thematic analysis utilized by the researchers:
1. Familiarization with the data.
2. Generating initial codes.
3. Searching for themes.
4. Reviewing themes.
5. Defining and naming themes.
6. Producing the report.
The data collected from the participants were carefully transcribed. An iterative process of close reading and re-reading of data led to the development of themes and categories. The researchers carefully read the transcribed data line by line, underlined words and phrases representative of participants’ experiences of living with HIV and AIDS and divided the data into meaningful analytical units. After locating the meaningful segments, category names were assigned. The researchers continued with the process until initial coding was completed on all data. Checking of themes on the experiences of women living with HIV and AIDS as reported by the participants was then conducted.
Ethical considerations
Prior to the study, researchers obtained ethical clearance from the Ethics Review Committee to respect the rights and dignity of participants as human beings and for the institution, University of South Africa (UNISA). Permissions from the Gauteng Provincial Health Department, District Health Services Support and Tshwane Research Committee were sought to conduct the study at the clinic.
After obtaining permission to conduct the study, researchers made it clear to the potential participants that participation was voluntary. Participants were informed that they were free to withdraw at any point without penalty. The decision whether or not to participate did not influence the way they received treatment at the Clinic. Beneficence was also taken into consideration to ensure that there was neither physical nor mental distress harm nor any danger to the study participants. The research is expected to benefit both the individual participants and society in general for a positive contribution towards the welfare of people. There was also a duty to protect the weak, vulnerable and incompetent by adopting procedures and processes to take into account their vulnerabilities. The researchers also applied the principle of justice, which is about being fair to all participants and not giving preference to some participants over others (Moule and Goodman, 2009).
RESULTS
Experiences of being diagnosed with HIV
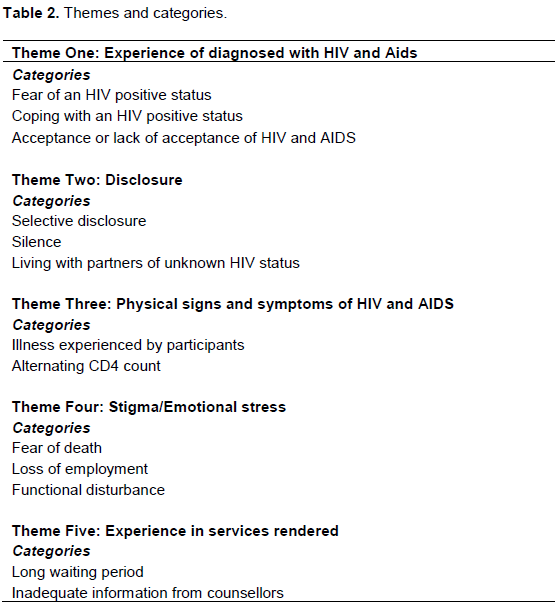
Data analysis revealed that experience of being diagnosed with HIV was the first theme that emerged. Two categories namely, fear of HIV positive status and coping with HIV positive status fell under this theme. The news of being diagnosed with HIV positive came with various stressful experiences. These stressful experiences ranged from the time of being tested for HIV and AIDS to the time the participants waited for the outcome of their results. HIV was considered by some participants as a threat to their lives and seen as a death sentence (Table 2).
The people living with HIV and AIDS (PLWHA) coped with their situation by depending on God and other PLWHA (Setlhare et al., 2014). Furthermore, relatives, friends, church, as well as non-governmental organizations (NGOs) and the government were used by PLWHA to cater for their emotional, physical and other needs. Religion, relatives and community structures are known coping mechanisms for PLWHA and these interventions need to be encouraged (Setlhare et al., 2014).
Fear of HIV positive status
The fear of being found positive for HIV itself was stressful among some of the participants. Furthermore, they reported having felt disturbed emotionally and stressed upon realizing their HIV status to the extent that a car hit one due to confusion. The participants interviewed had different reactions to the diagnosis of HIV and AIDS. The news of being diagnosed HIV positive, or having AIDS was a traumatic event for other participants. However, despite the disruption caused by HIV infection, the participants sought to put their lives together by applying different strategies to cope with the disease.
Setlhare et al. (2014) found in their study on experiences of people living with HIV/AIDS in Gaborone that women hesitate and fear to receive the care and treatment given to them. Secondly, they themselves become the victims of stress, depression, inferiority feeling, guilt and suicidal feelings.
Coping with HIV positive status
The participants had their different experiences and reactions upon the discovery of their HIV positive status, with most of them getting stressful. One of the participants revealed that T she looked after her late two brothers who were HIV positive. According to the participant, she had discovered some rashes developing on her private parts and suspected HIV. The participant reported that she refused to take medication and went for HIV and AIDS test. She applied a more positive copying mechanism because she had experienced and learnt more about HIV and AIDS through her siblings. She learnt to accept that HIV and Aids is something that one can live with instead of thinking of dying of it.
Some of the participants did not just cope but reported that their belief in God helped them to carry on with a positive mind. They believed that death is from God and that everyone has his or her time to die. Some of the participants received support from their partners and family members including their children and this helped them cope with their status. One participant highlighted that her son who is 17 years old often reminds her of the time to take her treatment. As the participants disclosed HIV and AIDS report, they received love, care and support from their family members. Support is particularly important for women living with HIV and AIDS as it assists them in building a positive life.
Acceptance or lack of acceptance of HIV and AIDS
As some of the respondents gained knowledge of HIV and AIDS, through encouragement and acquisition of more knowledge they later on accepted their status and viewed HIV and Aids like any other disease. For example, a participant reported that she had accepted her status after revealing it to her sister, although initially she struggled to accept. She went on and mentioned later in the interview how she was ready and willing to tell anyone about her HIV positive status and that she was at a stage of assisting other HIV positive people. Moreover, she managed to come to terms with her status and embarked on a mission to aid others in a similar situation. The participant developed a sense of purpose in using her experience to help others.
However, some participants revealed a sense of partial denial, not only during the initial stages of diagnosis, but also from time to time later on. They struggled to accept their HIV positive status. One participant reported that it was very hard for her to accept that she was HIV positive; the participant revealed that she could not take her treatment that time. This was a sign of denial. Although the participant later on decided to take her medication a year later after the diagnosis, she felt she was doing it for her children and not for herself.
Disclosing HIV positive status
This theme mainly deals with the participants’ decision to disclose their HIV status to other people. Almost all participants except for one managed to disclose their HIV status to at least one person or more. High rate of disclosure in the study may be attributed to the presence of peer counsellors who encouraged disclosure and adherence to ART at the clinic.
Selective disclosure
Although almost all participants managed to disclose their HIV status to at least one person or more, some of them were selective as to whom they told. One participant reported that she told her mother and her mother’s reaction was not very encouraging. Majority of the respondents disclosed their status to a family member, typically their mothers and/ or their current partners.
Silence
Out of the twelve participants who were interviewed, only one participant indicated that she had not told anyone about her HIV positive status. As the interview went on, the researcher discovered that the participant had lost most of her family members due to HIV and AIDS as she reported that she was alone at home. However, the participant revealed that she was in a relationship and still did not disclose her HIV status to her partner. Since she reported that she lost most of her family members and was alone at home, she might have feared that disclosing her status to her partner might chase him away.
Living with partners of unknown HIV status
The study findings also revealed that participants experienced having to live with their partners whose HIV statuses are unknown. Some reported that they were married and therefore revealed their status to their partners; they however, both struggled with the fact that their partners refused to test for HIV. As women living with HIV and AIDS, the participants were therefore faced with different challenges in living with partners whose HIV statuses were unknown. The situation presented additional anxiety and stress regarding exposure to re-infection, hence affecting their progress with their ART.
Signs and symptoms of HIV AND AIDS
The participants reported to have experienced some physical signs and symptoms of HIV and AIDS, which include TB related cough, loss of weight, vaginal rush and black spots, sweating, headaches, stomach pains, fever and tiredness. Due to these reported signs and symptoms, participants therefore fell ill from time to time. These changes had a great impact on their lives.
Illness
Some participants experienced HIV and AIDS related illnesses soon after testing positive for HIV. For example, one participant reported an experience of flulike symptom. The physical appearance of many women changed after they were infected with HIV.
Alternating CD4 count
The beginning of bodily changes related to HIV and AIDS, which often reveal deterioration due to illness, brings forth stigmatization because these changes are seen as “imminent death”. In addition, all too often job loss is a consequence (Liaputtong et al., 2009). According to Ramdas et al. (2015), women had a higher CD4+count at the time of being lost to follow-up. This could be expected as previous studies from sub-Saharan Africa have shown that women usually have a higher CD4+ count at ART initiation and a better median CD4+ count increase from baseline across all time periods after ART initiation than men (Meloni et al., 2014).
Stigmatization and emotions
People living with HIV and AIDS are inevitably affected by the symbolic meanings attached to the disease. The social stigma attached to HIV and AIDS often presents obstacles to the lives of people living with it. The women interviewed indicated having experienced some stress at some stage because of an HIV positive status. Participants were faced with having to deal with stressful experiences, which included the fear of death attached to HIV and AIDS, loss of employment, and functional disturbances upon being diagnosed with HIV positive. Another factor attributed to emotional stress was the delay in services rendered at the clinic.
Fear of death
One of the most likely sources of stigma of HIV and AIDS is its association with death and it illuminates many people’s responses to HIV and AIDS. According to some of the participants, the possibility of dying came into their minds after discovering that they were HIV positive. Some participants revealed their fear of death and reacted as if they have been diagnosed with a fatal and untreatable disease. They were exposed to the reality of death and scared that they would die. One participant related to death as something that happens to everyone, whether HIV positive or not. The participant was so confident and relaxed. Although she seemed to accept the possibility of her own death, it is almost inconceivable for her to imagine an actual ending of her own life here on earth
Loss of employment
Loss of employment was among some of the stressors faced by women living with HIV and AIDS. One participant gave a narration of how she was employed and fell ill on and off until she was forced to leave work due to her illness.
Functional disturbance
Participants narrated having suffered some discomforts such as psychological distress, depression, hopelessness and confusion. From these facts, it was clear that HIV and AIDS were perceived as destructive especially at the initial phase of diagnosis. The participants were faced with the stress of finding out that they were HIV positive. In such a situation the anxiety of what will happen next is inevitable. Questions related to possibility of treatment, sickness, disclosure and the future of the affected people can run through one’s mind causing stress and a feeling of hopelessness. Consistently worrying about what people might or are saying can mean a turnaround of the lives of women living with HIV and AIDS. Participants experienced a life full of social constructions around HIV and AIDS.
Experiences in provision of services
When asked about the services and treatment that they receive at the clinic, most women indicated that they were happy and that the nurses treated them well. However, some women were not happy with the long waiting period they had to endure before getting into the consultation room. On the other hand, some expressed disappointment with the lack of information given regarding their medication.
Long waiting period
Some of the participants reported that they would come to the clinic at 07H00 only to leave in the afternoon around 14H00. This meant an average of seven hours of waiting in the long queues to get assistance. The facts show that participants wait for a long time in the queues to get treatment and this can be frustrating to them. In addition, they felt that the delays in receiving services could be because they are HIV positive and hence may be regarded as less important than other patients did. This adds on the stress of living with HIV and AIDS that they already endure. As gathered from the participants’ notions, getting time to visit the clinic while one is employed can be a problem. One participant reported that it was very difficult to get time from work to go to the clinic every month. According to her, being a worker and having HIV was a challenge. Frequent visits to the clinic can be disruptive since one has to be absent from work.
Inadequate information from counsellors
It is also very necessary for health care providers to explain all the medication to be taken by their patients so that they understand the reasons why they are taking them. When asked about what information they needed from the VCT session, one participant reported that she did not get enough information regarding her medication and the type of food to eat and avoid. Drinking drugs and following a good diet is one of the most important things to do when one is HIV positive and it is therefore necessary that health care providers take the issue of information giving as a serious matter.
DISCUSSION
This study explored the experiences of women diagnosed as HIV positive and how this news affected their senses of self. As seen from the responses given, being diagnosed with HIV and AIDS came with various feelings such as fear of HIV positive status, struggling to cope with the disease as well as difficulty in accepting the disease. However, despite being faced with such a difficult moment of having one’s status being disclosed, most women, during the interviews, revealed how they realised the need to become strong and accept the painful news to be able to get on with their lives. The researchers felt the need to reinforce the message to PLWHA that HIV is not necessarily an early life sentence. People with HIV and AIDS can live normal lives if the resources to help are properly in place.
The aforementioned findings concur with the findings reported by Evans and Becker (2009) who suggest that diagnosis represents the moment at which HIV, AIDS is officially “named”, and this can produce a range of contradictory reactions. The writers further contend that many women describe their discovery of their HIV status as a traumatic experience that had a major impact on their emotional well-being and sense of identity. However, on the contrary, findings of a study conducted by Kajura (2010) maintain that accepting to be tested meant accepting everything that would come out. According to the author, people tend to feel better and at ease when told of their HIV positive status because at least they know the cause of their illnesses and hence freely accept the results. These findings are however, not supported in this research paper as only one participant in this study felt at ease with the fact that she was HIV positive; the rest of the participants experienced some emotional stress and were disrupted upon finding out they were HIV positive.
The findings revealed that women’s decisions related to disclosure are likely influenced by their evaluation of the consequences of disclosure. There is, therefore, a need for greater support to encourage women undergoing voluntary counselling and testing (VCT) to disclose their HIV status as this reduces the stigma associated with HIV. The findings reflected that participants were selective in deciding whom to tell and one of the reasons had to do with the fear of reactions from different people. Participants responded differently in terms of disclosing their HIV status. Some decided to be silent about their status and not telling a single soul apart from the health care providers.
Congruent study findings have been reported by Preau et al. (2008) who concluded that all individuals who learn about their HIV antibody status face an important decision regarding whom to share this information with. The decision of disclosure of one’s HIV sero-positivity to others is often perceived as a double-edged sword. According to the authors, opening up about one’s status may open up the opportunity of receiving social support; however, it may also lead to added stress due to stigmatisation, discrimination and disruption of interpersonal relationships.
Disclosure is another important issue with WLWHA. It has been an obstacle for WLWHA as not disclosing might deprive them of the opportunity of getting proper attention, care and access to facilities from family and health institutions (Paudel and Baral, 2015). Haffejee et al. (2016) indicated that only one respondent disclosed her status to anyone whilst two disclosed to everyone that they knew. Ramdas et al. (2015) reported that women preferred to disclose to a relative (82.1%) rather than a partner (28.6%). Disclosure of HIV status to one’s spouse is known to be associated with good adherence (Maskew et al., 2012). Cotemporary literary sources show that there is limited disclosure of one’s HIV status to a sexual partner (Gari et al., 2010). HIV positive partners usually disclose their status to other family members such as parents and siblings, but rarely to their sexual partners (Horn, 2010).
In addition, even though some participants managed to disclose their sero-positive status to their partners, they were faced with a difficult situation of having to live with their partners who refused to do HIV test. The results of the study are in agreement with a study by Deribe et al. (2008) on disclosure, experience and associated factors among HIV positive men and women clinical users in South West Ethiopia. In their study, a significant proportion of the women interviewed did not know their partners’ HIV status despite having disclosed their own status to them.
According to Paudel and Baral (2015), silence, secrecy and fear of disclosure were killing women with HIV and AIDS faster than the disease. Despite numerous benefits associated with HIV disclosure such as increased social support and kindness and easy access to health care treatment, there are also numbers of potential risks especially for women. These include abandonment and relationship termination, stigma and discrimination and emotional abuse. This had kept women in dilemma whether to disclose their status or not. Moreover, Kajura (2010) asserts that most women fear that they would be rejected, detested by their family members if they realised that they were HIV positive. The author further contends that disclosing one’s status would upset family members and lead to individuals been scorned by family members.
According to Patel et al. (2012), albeit HIV disclosure offers benefits, there are several barriers for HIV positive individuals to disclose which include being blamed for having HIV, fear of stigma and discrimination as well as potential disruption of relationships.
Participants narrated their different experiences of HIV related illness, which included headaches, stomach pains, fever, sweating and a lot more. A study by Willard et al. (2009) reveals the same findings that people living with HIV and AIDS experience several common but controllable symptoms throughout their illness trajectory. The frequently reported physical symptoms in their study include pain, fatigue, drowsiness, headaches and fever to mention a few.
Gonzale et al. (2012) found in their study that as a result of HIV and AIDS, including medication regimens used, persons living with the disease often experience a wide range of bodily sensations and the common symptoms include fatigue, nausea, chill or sweats and dizziness.
Along with physical illness other traumatic conditions came up like depression and anxiety. Some women were scared that been diagnosed meant that death was around the corner, some lost their jobs; while on the other hand some endured functional disturbances. Similar findings have being reported in a study conducted by Rief (2011) on highly stressful and traumatic experiences among individuals with HIV and AIDS in South Africa; the study participants were also faced with stressful experiences, loss of employment, stigma and functional disturbance.
HIV stigma in women is associated with rejection from friends and family, society, feelings of uncertainty and loss, low self-esteem, fear, anxiety, depression and even suicidal ideation (Paudel and Baral, 2015). In a study on assessment of awareness level and sources of information on HIV and AIDS among market women in Nigeria, Olubunmi and Aishat (2017) found that screening for HIV and AIDS was low among women. This was based on many reasons, but the major reasons were fear of death and stigmatization. This may suggest that discrimination of people living with HIV and AIDS still exists among the market women. Although HIV prevention programmes are expanding, they have not kept pace with the epidemic. Therefore, a lot still needs to be done to achieve the 90-90-90 target end the AIDS epidemic by 2030.
Although some PLWHAs are likely to maintain their jobs until serious physical dysfunction occurs, their occupational abilities and performances maybe restricted by periodic crisis of symptoms and pain. Women living with HIV and AIDS often encounter occupational difficulties due to on-going challenges of adjusting to the illness and social stigma.
Losing their jobs made the PLWHA to depend on relatives, hospice, church and government for sustenance and shelter. They could no longer support themselves or their children, and they suffered from hunger. Most lost their homes and lived with relatives (Setlhare et al., 2014). In a study conducted by Campbell et al. (2013) on the role of community groups in managing HIV/AIDS in rural Zimbabawe, job losses and disease progression made participants and their children dependent on relatives as has been found in other studies.
Setlhare et al. (2014) found that illness and stigmatisation led to job losses for PLWHA and may have worsened their anxiety and depression. Haffejee et al. (2016) further agreed that two (13%) of the respondents reported losing their jobs. Personal worries reported by HIV infected women were about death and leaving their children behind (Haffejee et al., 2016).
The study conducted by Ramdas et al. (2015) on factors associated with retention of HIV care at a medical centre, patient waiting time was kept to a minimum as appointments were made according to a time schedule. Appointments were booked electronically according to a time schedule, which, according to the staff, minimised patient waiting time. A large ART programme in Malawi also considered time-specific appointments for each patient as an option to reduce waiting time (Tweya et al., 2013).
According to Setlhare et al. (2014), the company and support of other PLWHA was valued considerably more than counselling by health workers. Ramdas et al. (2015) argue that adherence to ART at the medical centre was monitored at each visit by means of pill counts conducted by the social worker or counsellor and recorded as descriptive notes in the patients’ files and on the system. Furthermore, Ramdas et al. (2015) indicated that having a stable staff complement at the clinic meant that patients saw the same counsellor or social worker at every visit, which facilitated good relationships between staff and patients.
Health care workers are often community role models for conveying any health related concepts and ideas. Their attitudes and behaviours can shape the way members of the community treat persons suffering from health problems by challenging stereotypes and discriminatory attitudes. Health care workers must be educated about their responsibility so they do not perpetuate negative attitudes towards persons living with HV. Similarly, health care personnel at all levels need to be equipped with intensive training to sensitize them on the need to treat WLWHA without discrimination and provide them quality care (Paudel and Baral, 2015).
However, Haffejee et al. (2016), in their study on knowledge of and attitudes towards HIV infection and PMTCT of HIV in an urban, low-income community of South Africa, three respondents (5%) reported that their CD4 T cell count was above the required level for receiving ART. All women on ART reported that the medication had a positive effect on their health. Furthermore, women commented that they worried about becoming sick when their CD4 T cell count dropped.
Limitations
No attempts were made to generalize the findings of this article to a larger population as the research was limited to HIV positive women only. The study is also about the experiences of women living with HIV and AIDS in one clinic of Gauteng Province. In addition, due to the complexity of a positive status, not every participant gave detailed information as some participants withheld information that was sensitive to them.
CONCLUSION
The findings revealed that the experiences of women living with HIV and AIDS are to some extent related to the stigma that is associated with HIV and AIDS which led to fear of being diagnosed HIV positive, fear of death as well as issues related to disclosure and who to trust with one’s HIV positive status. However, apart from issues related to stigma, there was no discrimination experience amongst those who revealed their status to their partners and family. Furthermore, the findings indicated the benefits of disclosure as support and acceptance. However, illness was found inevitable at some stage in the women living with HIV and AIDS; therefore highlighting the importance of having a good health system with all the necessary medication available.
RECOMMENDATIONS
Practice
(1) There should be a well-established health system to assist women living with HIV and AIDS on how to cope and to raise awareness of the pandemic.
(2) There should be implementation and development of informative, structured support groups for women living with HIV and AIDS not having family in order to facilitate the acceptance of their HIV positive status and disclose to others.
(3) There should be strengthened testing of couples to avoid issues of living with a partner whose HIV status is unknown.
(4) There should be promotion of access to HIV and AIDS healthcare resources such as introducing mobile clinics and more staff to reduce pressure on the already existing fixed clinics and hospitals.
(5) Offering of support groups for women living with HIV and AIDS should be advocated as a fundamental part of HIV service as an effective and useful intervention.
Research
(1) Research to be conducted on a larger scale with women living with HIV and AIDS from different settings such as both urban and rural areas to get experiences of women living with HIV and AIDS from all spheres of life.
(2) Further research on how women living with HIV and AIDS cope with the pressure of having to be at work and having to find time off to visit their health care providers for treatment and check-up.
(3) A follow-up study to be conducted on the role of partners and workplace support amongst HIV positive women who are sole breadwinners in the household.
(4) Guidelines and policies are required in South Africa to reduce the AIDS stigma and to assist women diagnosed with HIV and AIDS to make effective decisions about disclosing their status to others.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Balls P (2009). Phenomenology in nursing research: methodology, interviewing and transcribing. Nortfolk and Norwich University Hospitals. NHS Foundation Trust. |
|
|
Campbell C, Scott K, Nhamo M (2012). Aids Care (25)1:114-122. F |
|
|
Deribe K, Woldemichael K, Wondafrash M (2008). Disclosure, experience and associated factors among HIV positive men and women clinical users in South West Ethiopia. Ethiopia: Biomed Central. |
|
|
Evans R, Becker S (2009). Children Caring for Parents with HIV and AIDS: Global Issues and Policy Responses. The Policy Press. |
|
|
Gari T, Habte D, Markos E (2010). HIV positive status disclosure among women attending ART clinic at Hawassa University Referral Hospital, South Ethiopia. East African Journal of Public Health 7(1). |
|
|
Gerish K, Lacey A (2010). The nursing research process in nursing, 6th edition, Wiley: Blackwell Publishing Ltd. |
|
|
Green J, Thorogood N (2009). Qualitative methods for health research. (2 edition). London: Sage. |
|
|
Griffiths F (2009). Research methods for health care practice. 1st edition. Sage Publications Ltd. |
|
|
Haffejee F, Ports KA, Mosavel M (2016). Knowledge and attitudes about HIV infection and prevention of mother to child transmission of HIV in an urban, low-income community in Durban, South Africa: Perspectives of residents and health care volunteers. Health and Gesondheid 21:171-178. |
|
|
Horn TJ (2010). Global Survey: Stigma, isolation and discrimination, Paper presented at XV111 International AIDS conference, July 18-23. [Cited 2018 March 08]. |
|
|
Kajura NN (2010). The perceived and experienced barriers and reported consequences of HIV positive status disclosure by people living with HIV to their partners and family members in Djibouti. University of Western Cape. |
|
|
Krippendorff K (1980). Content analysis an introduction to its Methodology. London: Sage. |
|
|
Liaputtong P, Haritavorn N, Kiatying-Angusulee N (2009). HIV and AIDS, stigma and AIDS support groups: Perspectives from women living with HIV and AIDS in central Thailand. Social Science and Medicine (69):862-868. |
|
|
Maskew M, Brennan AT, Westreich D (2012). Journal of Women's Health 1:113-120. |
|
|
Meloni SM, Chang C, Chaplin B, Rawiza H, Jolayemi, O, Banigbe B, Okonkwo P, Konki P (2014). Time –Dependent Predictors of Loss to Follow-up in a large HIV Treatment Cohort in Nigeria. From: |
|
|
Moule P, Goodman M (2009). Nursing Research, an introduction. 1st edition. Sage Publications Ltd. |
|
|
Ogunmefun C, Gilbert L, Schartz E (2011). Older female caregivers and HIV/AIDS-Related secondary stigma in Rural South Africa. 2011. Journal of Cross-Cultural Gerontology 26(1):85-102. |
|
|
Olubunmi A, Aishat U (2017). An assessment of awareness level and sources of information on HIV/AIDS among women in Ibadan, Oyo State, Nigeria. Journal of AIDS and HIV Research 9(9):179-186. |
|
|
Patel SV, Patel SN, Baxi RK, Colin CE, Mehta M, Shringarpure K, Bakshi H, Modi E, Coonor P, Mehta K (2012). HIV sero-status disclosure: Experiences and perceptions of people living with HIV/AIDS and their service providers in Gujarat, India. Industrial Psychiatry Journal 21:130-136. |
|
|
Paudel V, Baral K (2015). Women living with HIV/AIDS (WLHA) battling stigma, discrimination and denial and the role of support groups as a coping strategy: a review of literature. Reproductive Health.12-53. |
|
|
Polit DF, Beck CT (2012). Essentials of Nursing: Appraising Evidence for Nursing Practice. Wolters Kluwer, Lippincott, Williams & Wilkins. |
|
|
Preau M, Bouhnik AD, Roussiau N, Lert F, Spire B (2008). Disclosure and Religion among people living with HIV and Aids in France. Aids Care 5:521-526. |
|
|
Ramdas N, Meyer JC, Cameron D (2015). Factors associated with retention in HIV care at Sediba Hope Medical Centre. South African Journal of HIV Medicine 16(1):1-6. From: |
|
|
Rief S, Mugavero M, Raper J, Thielman N, Leserman J, Whetten K, Pence WB (2011). Highly Stressed; Stressful and traumatic experiences among individuals with HIV and Aids in Deep South. Aids Care 23(2):152-162. |
|
|
Setlhare V, Wright A, Couper I (2014). The experiences of people living with HIV/AIDS in Gaborone, Botswana: stigma, its consequences and coping mechanisms, South African Family Practice, 56:6, 309-313, |
|
|
Shisana O, Rehle T, Simbayi LC, Zuma K, Jooste S, Zungu N, Labadarios D, Onoya D (2014). South African National HIV Prevalence Incidence and Behaviour Survey. 2014. Cape Town, HSRC Press. |
|
|
Statistics South Africa: Mid-year Population Estimates (2017). Government Printer. South Africa. |
|
|
Statistics South Africa: Mid-Year Population Estimates (2018). Government Printer. South Africa. |
|
|
The Foundation for AIDS Research (amfAR) (2015). 'Statistics: Women and HIV/AIDS'. |
|
|
Tweya H, Feldacker C, Estill J, Janh A, Ngambi W, Ben-Smith A, Keiser O, Bokosi M, Egger M, Speight C, Gumulira, J, Phiri S (2013). Are They Really Lost? "True" Status and Reasons for Treatment Discontinuation among HIV Infected Patients on Antiretroviral Therapy Considered Lost to Follow Up in Urban Malawi. PLOS ONE/ www.Plosone.org September 2013 8 (9):e75761. |
|
|
UNAIDS (2015). Estimates from the AIDS info online database. Additional desegregations correspond to unpublished estimates for 2015 provided by UNAIDS, obtained from country-specific models of their AIDS epidemics. |
|
|
UNAIDS (2018). Country South Africa |
|
|
Willard S, Holzemer WL, Wantland DJ (2009). Does asymptomatic mean without symptoms for those living with HIV infection? Aids Care 21(3):322-328. |
|
|
World Health Organization (WHO) (2018). WHO/HIVAIDS and other sexually transmitted infections. International travel and health. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


