Full Length Research Paper

ABSTRACT
Clinic absence or lost to follow-up is still a big challenge in West Africa, especially in Guinea-Bissau, where retention in care is lower compared to all other low- or middle-income countries. The study aims to explore the reasons for clinic absence among HIV-infected patients in Guinea-Bissau, and to evaluate whether the telephone tracing is associated with patients returning to clinic follow-up. A prospective cohort analysis was conducted. Data were collected through telephone calls in which patients or their contact persons were asked for reasons for non-attendance. A total of 3,668 patients, who had been considered as clinic absent were enrolled in this study; 1,883 (51.3%) on antiretroviral treatment (ART) and 1,785 (48.7%) without ART. The median time between patients last clinic visit to time of calling was 203 days (interquartile range (IQR) 59 - 360 days). 748 (20.4%) patients and additional 364 (9.9%) contact persons were successfully reached. Reasons for clinic absence included traveling 346 (31.1%), death 211 (19.0%), and still having medicine 186 (16.7%). After tracing, 555 (49.9%) of the traced patients returned to the clinic. Nineteen percent of the absent HIV-infected patients had died by the time of calling, underscoring the need to improve patient follow-up in Guinea-Bissau. Telephone calls provide an important tool to address reasons for clinic absence and may lead to patients returning to clinical follow-up.
Key words: Clinic Absence, Loss to follow-up, Return, HIV, ART, Telephone, Sub Saharan Africa.
INTRODUCTION
It is estimated that 36.7 million people worldwide are infected with HIV (UNAIDS, 2017a) and the number is growing. Sub-Saharan Africa is the most affected region and in some parts of this region antiretroviral treatment (ART) is not available (UNAIDS, 2017a; Oliveira et al., 2012). ART has reduced mortality and improved life quality among HIV-infected individuals, but treatment success depends highly on patient retention and good adherence (Dyrehave et al., 2016; Rasmussen et al., 2013; Jespersen et al., 2015a). ART requires a large commitment from the patient as poor adherence leads to viral resistance, a subsequent risk of progression to AIDS with opportunistic infections, and a risk of further transmission of resistant viral strains (Dyrehave et al., 2016; Rasmussen et al., 2013; Onoka et al., 2012). Adherence to treatment may therefore be considered as important as any pharmacologic effect of the treatment regime (Jespersen et al., 2015b; Onoka et al., 2012). Loss to follow-up (LTFU) is closely related with poor adherence, lack of general knowledge of HIV natural history (Dyrehave et al., 2016; Rasmussen et al., 2013), and remains one of the biggest barriers to adequate HIV care delivery in sub-Saharan Africa (Fox, 2015).
In the West African country Guinea-Bissau, both HIV-1 and HIV-2 are prevalent (Olesen et al., 2018). According to the 2016 UNAIDS country factsheets, thirty-six–thousand people were living with HIV, and only 33% of them were on ART (UNAIDS, 2017b). In a study from the capital Bissau, 57.5% of all diagnosed patients had been lost to follow-up during a seven-year period (Hønge et al., 2013). A systematic review and meta-analysis from 2015 reported that patient retention was lower in Guinea-Bissau compared to other low- and middle-income countries (Fox, 2015). In order to address the issues of clinic absence, more studies are needed. Previous research has shown that LTFU from the HIV clinic in Bissau are associated with male sex, young age, low body mass index (BMI) and low CD4 cell count (Hønge et al., 2013; Jespersen et al., 2014), but the exact causes of absence from the clinic are insufficiently understood and described. While death is likely one of the main reasons of LTFU and clinical absence, many other factors may be considered, such as: travelling, unregistered transfer to another HIV clinic, seasonal work away from the clinic area, patients not feeling sick, and patients that decided to take traditional treatment (Nordentoft et al., 2017). The objective of this study was to describe the exact causes of clinic absence among HIV-infected patients, and to evaluate whether active follow-up by telephone contact tracing is associated with patients returning to the clinic.
MATERIALS AND METHODS
Study design
Prospective cohort data analysis.
Setting and patients
This study was conducted at the “Centro de Tratamento Ambulatório de Hospital Nacional Simao Mendes” (CTA-HNSM). CTA-HNSM is the largest HIV clinic in Guinea-Bissau in terms of the number of patients on follow-up, with about 10000 patients registered. The study population consisted of all HIV-infected individuals diagnosed at the HIV clinic between June 2005 - December 2016.
On the first day a patient visited the clinic, HIV testing was performed, and basic demographic information was collected by a doctor or a psychologist. Schooling was defined as attending school with the purpose of learning how to read and write; koranic school was excluded from this criterion. When a patient was diagnosed with HIV, the patient was given a requisition for laboratory analyses (which includes differentiation of HIV types, CD4 cell count, biochemistry, and hematology). The blood samples were collected routinely in the morning and patients were asked to come back to the clinic within 7 days when a doctor would decide whether to initiate ART, and in this case, which treatment regime was the most indicated, based primarily on HIV type, hemoglobin levels, and CD4 cell count. When the ART initiation decision was taken, the patient received ART the same day as the consultation, and information about how to take ART and possible side effects was given. All services including ART and laboratory analysis are free of charge for HIV-infected individuals in Guinea-Bissau. The cost is supported by Global Fund to fight AIDS, Tuberculosis, and Malaria (Jespersen et al., 2015a).
Active follow-up
Patients diagnosed with HIV were given a personal follow-up card with a unique registration number and the date of the next appointment at the clinic was noted. Patients were assigned to one primary doctor during follow-up and were asked to provide their own telephone number and/or the telephone number of the closest contact person, to be used during active follow-up in case of clinic absence. Every month the patient must return to the consultation for a clinical control, and to pick up medicine. A blood sample was drawn every third month for measurement of CD4 cell count and biochemistry. From January 2011 to December 2016, we considered all patients who had missed an appointment from the clinic for more than 7 days, after the date of their next planned visit, as clinic absence, and they were called and asked for reasons for non-attendance.
Statistical methods
The data were entered in an Access database (Microsoft), and analysed using Stata IC 13.0 (StataCorp, College Station, Texas, USA). Descriptive statistics were used to summarize patient data, and the variables were described by frequency distribution. Demographic, laboratory, and clinical variables were compared using χ2 test for category variables. For continuous variables, we used rank sum test and Student T-test as appropriate.
Ethical statement
The Bissau HIV cohort has ethical approval from the National Ethics Committee from Ministry of Health of Guinea-Bissau, reference no. 023/CNES/INASA/2014, which includes the use of all data from patient journals as long the patient confidentially was kept unbroken. At the time of enrolment, the patient provided informed oral and written consent. In case of illiteracy, the fingerprint is provided.
RESULTS
Between June 2005 and December 2016, 9,536 patients were diagnosed with HIV by CTA-HNSM (Figure 1). HIV typing revealed that 6,367 (66.8%) of the patients were infected with HIV-1, 1,198 (12.6%) of the patients were infected with HIV-2, and 772 (8.1%) of the patients were dually infected with both HIV-1 and HIV-2 (HIV-1/2). A total of 1,199 patients (12.6%) had not had HIV typing performed.
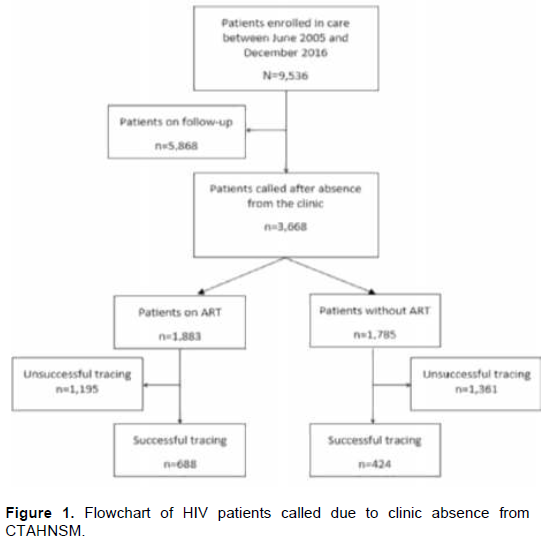
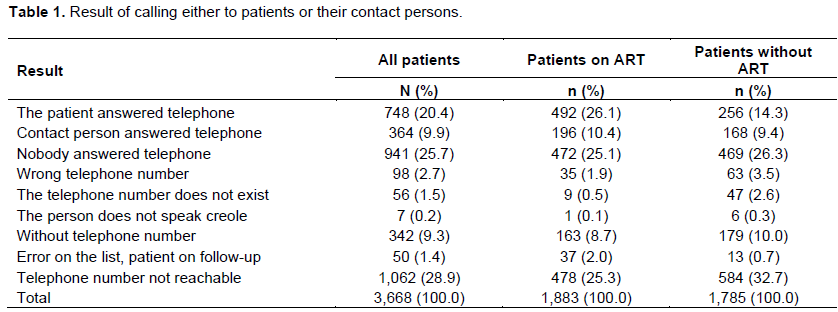
Five-thousand-eight-hundred-and-sixty-eight patients were excluded in this study; this comprised patients who remained on follow-up, patients who died, and those who were transferred to another ART center. While a total of 3,668 patients were included in the study, due to clinic absence (Figure 1). The median time between patients last clinic visit to the time of calling was 203 days interquartile range (IQR 59 - 360 days). During the active telephone tracing, we successfully reached 1,112 (30.3%) patients or their contact persons. A larger proportion of patients (or contact person) on ART answered the telephone, n=688 (36.5%) compared with those not receiving ART, n=424 (23.8%), p<0.01. Nobody answered the telephone in 941 (25.7%) of the cases, and 342 (9.3%) patients had not provided a telephone number. For 1,062 (28.9%) patients, the telephone number was not reachable (Table 1).
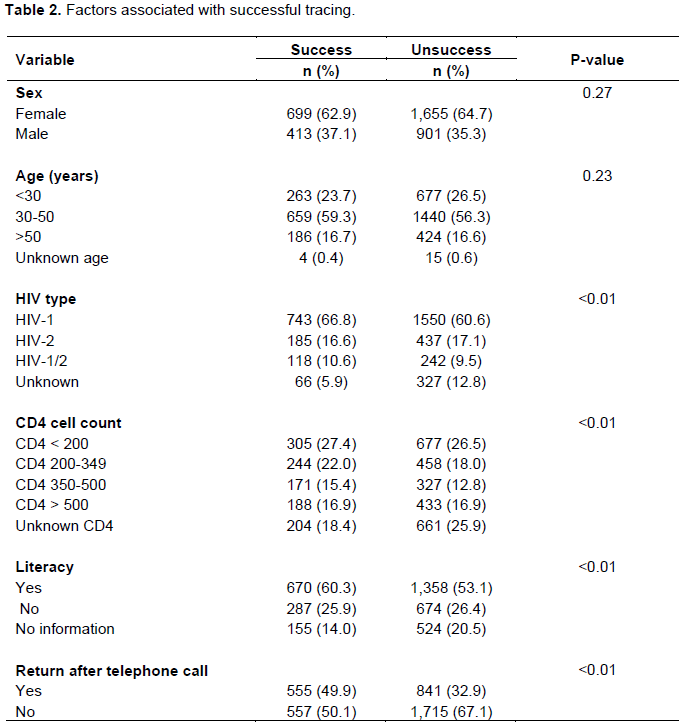
There was no difference in tracing success between the different age groups (p=0.23, Table 2). For HIV types, there are significant difference according to groups, with the lowest proportion of successful tracing among patients with unknown HIV type (p<0.01). When patients with unknown HIV type were excluded from the analysis, there was no difference between groups (p=0.43). Moreover, tracing success was associated with lack of CD4 cell count measurement (p<0.01), but median CD4 cell count was similar for patients with tracing success (294 cells/µL) compared to patients with tracing failure (280 cells/µl, p=0.74).
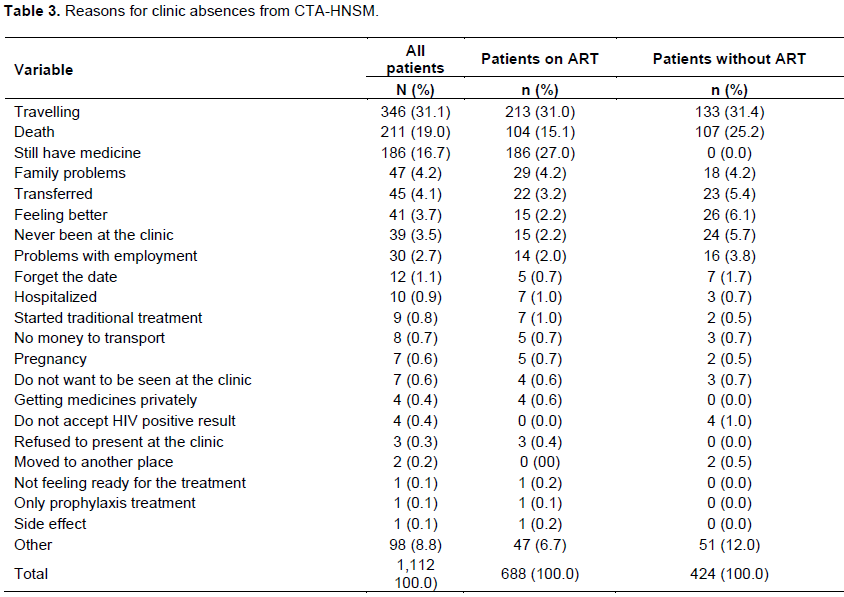
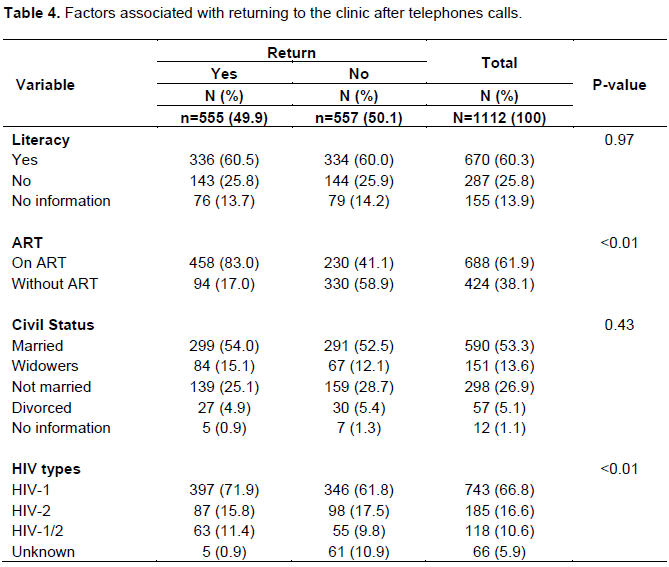
Our results showed that the most common reason of clinic absence from the HIV clinic in Bissau was travelling (31.1%), followed by death (19.0%) and patients that claimed that they still had medicine (16.7%) (Table 3). After the active telephone tracing, a total of 555/1112 (49.9%) of the traced patients returned to the clinic. The median time between date of the last clinic visit and the date of calling patients was lower for patients who returned to the clinic (104 days, interquartile range (IQR) 69-190 days) compared to patients that did not return (252 days, IQR 182-528 days, p<0.01). The success rate for patients who returned to the clinic after telephone calls (Table 4) was significantly higher among patients who had started ART (83.0%) compared with those without ART (17.0%, p<0.01) (Table 4). After excluding patients with unknown HIV type, we found no association between HIV type and proportion of patients returning (p=0.29). According to returning to the clinic after the telephone trace, we found no significant differences when we looked at the patient`s literacy (p=0.97) or civil status (p=0.43).
DISCUSSION
In this study, we explored the reasons for clinic absence among HIV-infected patients, and whether an active follow-up by telephone contact tracing was associated with patients returning to follow-up at the largest ART clinic in Bissau, Guinea-Bissau. Our findings show that the most common reasons for clinic absence were traveling and death. Furthermore, we found that it was possible, through active telephone tracing, to assess the reason for clinic absence among a minority of the HIV-infected patients, and that the telephone call was associated with half of the traced patients returning to the clinic to continue their follow-up.
Patients who had initiated ART were more likely to return to the clinic to continue their follow-up. Findings from Gambia have shown that a high proportion of ART eligible HIV infected patients were not able to initiate ART and they accounted for a high pre-treatment mortality rate (Togun et al., 2011). Our results found no differences in tracing success rate according to literacy. This could be explained by a general lack of information and knowledge about the chronicity of HIV infection, and the aim of lifelong treatment previously described (Dyrehave et al., 2016; Rasmussen et al., 2013). There is an urgent need to improve information about HIV lifelong treatment for all patients at the time of inclusion, so that we can improve patients understanding about the aim of the treatment and improve retention and avoid clinic absences.
Our data has demonstrated that the most common reason of absence was travelling, followed by death and patients that claimed that they still had medicine. A previous study from Bissau published in 2017 had also reported that the most common reason of becoming lost to follow-up was moving/travelling (Nordentoft et al., 2017). Travelling can be associated with the purpose of patients deciding to take a traditional treatment from the capital Bissau, and with seasonal work (Nordentoft et al., 2017). These findings can support results from a previous similar study carried out in Nairobi, Kenya, that also reported that the most common reason for losing to follow-up among HIV-infected patients was moving, and the majority of these moving is related to job loss or change in employment (Marson et al., 2013).
The second and most worrisome reason for clinic absence among all traced patients in this study was death. These findings correspond to similar studies from West Africa (Cameroon and Togo) that also reported high mortality among HIV-infected patients that have been considered as LTFU (Bekolo et al., 2013; Saka et al., 2013). Thus, there is a big challenge for doctors to identify the most severely ill patients and those at risk of LTFU. A possible intervention could, for example, be the development and implementation of national HIV clinic-score, based on patients´ clinical presentation and laboratory results, which would be able to guide the clinicians to identify which patients are at a high risk of dying, and thereby an absolute indication of acute hospitalisation and intensive treatment. Our findings support a previous study with a published report that indicated that telephones call can be used to assess the vital status among HIV-infected patients who have been LTFU in sub-Saharan Africa (Semeere et al., 2017). Future studies could look at the time of patients´ death, so we can be aware if they have had some period without taking ART or died due to treatment failure.
Some patients reported their absence from the clinic was because they still had medicine. This is worrisome because patients are only called after the registered dispersed number of pills have expired, suggesting drug holidays, or poor compliance. As we described before, findings from previous research conducted in Bissau have indicated that the general knowledge of HIV chronic infections, and the aim of lifelong treatment is poor (Dyrehave et al., 2016; Rasmussen et al., 2013), and patients can skip their medicine doses when they do not have food (Rasmussen et al., 2013), that can explain why some patients still have medicines at home despite having not attended the clinic for a long period of time. In this case, telephone call reminders can be used as an important tool to improve treatment adherence (Kinyua et al., 2013).
Telephone tracing can be used to address reasons for clinic absence in settings where patients retention rates are known to be low, as in Guinea-Bissau and many other countries in sub-Saharan Africa (Fox, 2015; Hønge et al., 2013). It has been published before that one of the most important aspects of any health care intervention is to assess its feasibility and intervention in the real world (Belzer et al., 2015). Our data has demonstrated that with an active telephone trace it is possible to address reasons for clinic absence among HIV-infected individuals and tracing success was associated with increased number of patients returning to the clinic. A recent study from 2017 showed that the use of mobile phone trace was an effective tool to reach young people and achieve knowledge and behavior change (Ippoliti and L’Engle, 2017). Another study from Kenya with public report has also indicated that the use of Short Message Service (SMS) through mobile phones may be a very important tool to achieve high retention and a better treatment response among HIV infected individuals in resource limited settings (Pop-Eleches et al., 2011).
LIMITATIONS OF THE STUDY
The main limitation of this study is that we could not talk to a total of 54.3% of patients or contact persons we tried to phone call. That could be because they may already have died by the time of calling, which implies there is an underestimated death rate.
This is supported by results from a research conducted in a west African country Gambia (Togun et al., 2011). Results from a metanalysis that used data from five different treatment programs from sub-Saharan Africa reported that, patients lost to follow-up are at substantially higher risk of death compared with patients who remain in health care (Brinkhof et al., 2010). Another possible explanation could be logistic problems with lack of electricity in the country and patients being unable to charge their telephones. Guinea-Bissau is known to be one of the poorest countries in the world, where 67% of the population lives below the poverty line (World Factbook, 2018). People in Guinea-Bissau often change their telephone number after some period, for example, when they lack money to buy telephone credits, which could prove a challenge and make a telephone trace impossible, and it can be a risk factor for increasing the rate of clinic absence. Another possible explanation could be that some people do not want to talk with the health care workers from the HIV clinic, because they are afraid of being stigmatized in the society if someone else gets to know that they are HIV-infected. A previous qualitative study from Bissau published in 2013 has reported that HIV stigmatization is one of the strongest barriers for treatment adherence and retention in care among HIV-infected patients in Guinea-Bissau (Rasmussen et al., 2013), and that can be a strong risk factor for unattendance.
CONCLUSION
Travelling was the most common reason for clinic absence in this study, emphasizing the need for better universal access to HIV treatment and more coordination between national HIV clinics. Furthermore, the information about lifelong HIV treatment should be improved by the time of a patient’s enrolment. Almost every fifth patient that has been absent from the clinic had died by the time of telephone calls, which could indicate that it was challenging for the doctors to clinically identify the most severely ill patients and most often it was not possible. Active telephone tracing can be used as an important tool to address the reason for clinic absence and vital status among HIV-infected individuals, and it is associated with the patients returning to the clinic.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGEMENT
This study was financially supported by DANIDA Fellowship Centre, Copenhagen, Denmark.
REFERENCES
|
Bekolo C, Jayne W, Moses B, Gerald S, Basile K (2013). Trends in Mortality and Loss to Follow-up in HIV Care at the Nkongsamba Regional Hospital, Cameroon. BMC Research Notes 6(1):512. |
|
|
Belzer ME, Kolmodin MK, Clark LF, Huang J, Olson J, Kahana SY, Adolescent Medicine Trials Network for HIV/AIDS Interventions. (2015). Acceptability and feasibility of a cell phone support intervention for youth living with HIV with nonadherence to antiretroviral therapy. AIDS Patient Care and STDs 29(6):338-345. |
|
|
Nordentoft PB, Engell-Sørensen T, Jespersen S, Correia FG, Medina C, da Silva TD, Bissau HIV Cohort study group (2017). Assessing factors for loss to follow-up of HIV infected patients in Guinea-Bissau. Infection 45(2):187-197. |
|
|
Brinkhof MW, Spycher BD, Yiannoutsos C, Weigel R, Wood R, Messou E, International epidemiological Database to Evaluate AIDS (IeDEA) (2010). Adjusting mortality for loss to follow-up: analysis of five ART programmes in sub-Saharan Africa. Plos One 5(11):e14149. |
|
|
Dyrehave C, Rasmussen DN, Hønge BL, Jespersen S, Correia FG, Medina C, Bissau HIV Cohort Study Group (2016). Nonadherence is associated with lack of HIV-related knowledge: a cross-sectional study among HIV-infected individuals in Guinea-Bissau. Journal of the International Association of Providers of AIDS Care (JIAPAC) 15(4):350-358. |
|
|
Fox MP (2015). Retention of Adult Patients on Antiretroviral Therapy in Low-and Middle-Income Countries: Systematic Review and Meta-Analysis 2008-2013. Journal of Acquired Immune Deficiency Syndromes (1999) 69(1):98. |
|
|
Hønge BL, Jespersen S, Nordentoft PB, Medina C, da Silva D, da Silva ZJ, Bissau HIV cohort study group (2013). Loss to Follow-up Occurs at All Stages in the Diagnostic and Follow-up Period among HIV-Infected Patients in Guinea-Bissau: A 7-Year Retrospective Cohort Study. BMJ Open 3(10): e003499. |
|
|
Ippoliti NB, Kelly E (2017). "Meet Us on the Phone: Mobile Phone Programs for Adolescent Sexual and Reproductive Health in Low-to-Middle Income Countries. Reproductive Health 14(1). |
|
|
Jespersen S, Hønge BL, Oliveira I, Medina C, Té DDS, Correia FG, Wejse C (2014). Challenges facing HIV treatment in Guinea-Bissau: the benefits of international research collaborations. Bulletin of the World Health Organization 92:909-914. |
|
|
Jespersen S, Hønge BL, Oliveira I, Medina C, da Silva TD, Correira FG, Bissau HIV Cohort study group (2015a). Cohort profile: the Bissau HIV cohort-a cohort of HIV-1, HIV-2 and co-infected patients. International Journal of Epidemiology 44(3):756-763. |
|
|
Jespersen S, Martin T, Hønge Bo, Candida M, David T, Svend Ellermann-E, Lars O, Christian W, Alex L, Bissau HIV cohort study group (2015b). High Level of HIV-1 Drug Resistance among Patients with HIV-1 and HIV-1/2 Dual Infections in Guinea-Bissau." Virology Journal 12(1):41. |
|
|
Kinyua F, Michael K, Gideon K, Joseph M, Adrienne FAM, Peter M, Elijah S (2013). Perceptions of HIV Infected Patients on the Use of Cell Phone as a Tool to Support Their Antiretroviral Adherence; a Cross-Sectional Study in a Large Referral Hospital in Kenya. BMC Public Health 13(1). |
|
|
Marson KG, Tapia K, Kohler P, McGrath CJ, John-Stewart GC, Richardson BA, Chung MH (2013). Male, mobile, and moneyed: loss to follow-up vs. transfer of care in an urban African antiretroviral treatment clinic. PloS ONE 8(10):e78900. |
|
|
Olesen JS, Jespersen S, Da Silva ZJ, Rodrigues A, Erikstrup C, Aaby P, Hønge, BL (2018). HIV-2 continues to decrease, whereas HIV-1 is stabilizing in Guinea-Bissau. Aids 32(9):1193-1198. |
|
|
Oliveira I, Andersen A, Furtado A, Medina C, da Silva D, da Silva ZJ, Bissau HIV cohort study group (2012). Assessment of simple risk markers for early mortality among HIV-infected patients in Guinea-Bissau: a cohort study. BMJ Open 2(6):e001587. |
|
|
Onoka CA, Uzochukwu BS, Onwujekwe OE, Chukwuka C, Ilozumba J, Onyedum C, Nwobi EA, Onwasigwe C (2012). Retention and Loss to Follow-up in Antiretroviral Treatment Programmes in Southeast Nigeria. Pathogens and Global Health 106(1):46-54. |
|
|
Pop-Eleches C, Thirumurthy H, Habyarimana JP, Zivin JG, Goldstein MP, De Walque D, Bangsberg DR. (2011). Mobile phone technologies improve adherence to antiretroviral treatment in a resource-limited setting: a randomized controlled trial of text message reminders. AIDS (London, England) 25(6):825-34. |
|
|
Rasmussen DN, da Silva Té, D, Rodkjaer L, Oliveira I, Medina C, Barfod T, Wejse C (2013). Barriers and facilitators to antiretroviral therapy adherence among patients with HIV in Bissau, Guinea-Bissau: a qualitative study. African Journal of AIDS Research 12(1):1-8. |
|
|
Saka B, Landoh DE, Patassi A, d'Almeida S, Singo A, Gessner BD, Pitché PV (2013). Loss of HIV-infected patients on potent antiretroviral therapy programs in Togo: risk factors and the fate of these patients. Pan African Medical Journal 15(1). |
|
|
Semeere A, Freeman E, Wenger M, Glidden D, Bwana M, Kanyesigye M, Martin J (2017). Updating vital status by tracking in the community among patients with epidemic Kaposi sarcoma who are lost to follow-up in sub-Saharan Africa. BMC Cancer 17(1):1-11. |
|
|
Togun T, Ingrid P, Shabbar J, Francis O, Uduak O, Kevin P, Assan J (2011). "Pre-Treatment Mortality and Loss-to-Follow-up in HIV-1, HIV-2 and HIV-1/HIV-2 Dually Infected Patients Eligible for Antiretroviral Therapy in The Gambia, West Africa. AIDS Research and Therapy 8(1):24. |
|
|
UNAIDS (2017a). Fact Sheet - Latest Statistics on the Status of the AIDS Epidemic | UNAIDS. 2017. |
|
|
UNAIDS (2017b). Guinea-Bissau Country Factsheets." (2017). |
|
|
World Factbook (2018). The World Factbook - Central Intelligence Agency. 2018. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


