Full Length Research Paper

ABSTRACT
Effect of healthcare accessibility on cocoa farmers’ food security explored latest research from the economic, medical and food security literature concerning the eminence of care, physical accessibility, cost, availability of the right type of care for those in need, and its significances on food security, with a focus on healthcare personnel availability. A multistage (five-stage) sampling procedure was employed to select 200 farmers and data were collected using structured questionnaire. Accessibility Index (AI), Food Security Index (FSI) and Tobit regression model were used for the analysis. The accessibility index shows that Owo LGA has 5 patients per doctor, Idanre LGA has 9 patients per doctor and Ile Oluji LGA has 8 patients per doctor while Ondo West LGA has 7 patients per doctor. Consultation cost, service cost and diagnosis cost were found to have negative effect on farmers’ income while medicine and surgical cost were found significant to farmers’ income. Although 65.50% of the respondents were food secured, the number of patient per different health personnel and facility as well as family size (0.000) have a significant relationship with farmers' food security status. Thus, it is suggested that more deployment of health care officers and facilities are needed in the study areas.
Key words: Food security, farmers, healthcare, accessibility, income, cocoa.
INTRODUCTION
The notion of food security has been enlightened differently based on diverse conceptualizations and punitive approaches (Pinstrup-Andersen, 2009). There has been different postulation such as if more food is not made available by 2030, a perfect food insecurity is inevitable (Poppy et al., 2014). Food security has been studied based on three pillars, which are: availability, accessibility and utilization (Pinstrup-Andersen, 2009; Barrett, 2010; Maxwell, 1996). Barrett (2010) added that these pillars follow a process as access can only occur after food availability is fulfilled. The main goal of food security is for people to be able to acquire satisfactory food required at all times and to be able to utilize the food to meet the body’s needs.
Being healthy is not just the absence of sickness or infirmity but a state of ample bodily, mental and social comfort. Health raises physical capacities like strength and endurance, mental capacities and reasoning abilities. These enhance workers’ productivity (FAO/WHO, 1992), and have a great impact on the number of hours worked by humans everywhere (Currie and Madrian, 1999). Sound health is an ultimate prerequisite for living a socially and frugally active prolific life (Titus et al., 2015).
Health care is the deterrence, management and treatment of illness and the safeguarding of mental and physical comfort through the services offered by the medical and allied health professionals (Farlex, 2018). Healthcare access is of major interest to rural development, because it is a vital element of wellbeing and component of human capital (Aghion et al., 2010). Rural areas are known to be a place where physical jobs tend to be more abundant, therefore among the needed vital basic amenities for proper delivery of the primary occupation is healthcare accessibility. Additionally, all individuals understand good health as a need; this makes healthcare accessibility an economic good. It was reported that the effects of ill health on farmers' households include three broad impacts: absenteeism from work due to morbidity (and eventual death) (Asenso-Okyere et al., 2011); diversion of farming time to caring for the sick; and the loss of savings and assets in the course of dealing with diseases and its consequences. The ultimate impact of this ill health can be narrowed down to a decline in household income. When the farmers, family members or employees are unable to work because of health problems or the whole income or larger percentage of it is spent on the treatment, both viability and quality of life are negatively affected (Gillespie and Johnson, 2010). The ability of farm families to manage health problems is dependent on access to care that is made more affordable and accessible.
Access to healthcare services was described as a multidimensional process involving the quality of care, geographical accessibility, availability of the right type of care for those in need, financial accessibility, and acceptability of service (Peters et al., 2008). Geographical accessibility to healthcare services means the timely use of personal health services to achieve the best health outcomes. It relates to the quality of being able to reach a facility easily and it has come to be popular especially in the distribution of services and amenities among a given population. Accessibility was also viewed not only in the physical sense but it has in addition economic, cultural and functional connotations (Nwaru, 1993). Economic accessibility refers to whether the cost is affordable while cultural accessibility implies that the technology and administrative standard must be compatible with the social values, habits, cultural patterns and customs of the community served. World Health Organization also describes physical accessibility as the obtainability of good health services within realistic reach of those who need them, economic accessibility is however described as the people’s ability to pay for services without financial destitution (it takes both the direct and indirect cost into consideration [WHO, 2013]).
The resultant effect of inadequate access to healthcare facilities can be best exemplified by the number of man hour loss to illness. The consequence is lower productivity which in a way upset the farmers’ income. Access to healthcare services is critical to good health, yet rural dwellers face varieties of access barriers. Ideally, they should be able to expediently and assuredly access services such as primary health care, emergency care and public health services. This is important for overall physical, social and mental health status, diseases prevention and quality of life. Barriers such as financial means to pay for services, transportation means to reach the services and other factors limit their ability to access healthcare services and obtain the care they need [WHO, 2013]. In general, they waste a lot of time getting to the nearest healthcare service center, of which they either have to trek long distance or spend money on motorcycle. Farmers easily resign to purchase of medication over the counter as there is no surety of neither qualified medical personnel or medicine availability even after incurring transportation cost.
The scenario portrays the situation in many states of the federation. Despite the slogan of “health for all by year 2000” (WHO, 1978) and even the proclaimed free health policy, the accessibility to health care services are still far from being adequate (Ajala et al., 2005). Study on healthcare expenditure, healthcare status and national productivity in Nigeria by Eneji (2013) found that health spending in Nigeria is low and as such there is inequality in health care access in Nigeria. Poor health status in Nigeria was attributed to poverty, unemployment, poor living conditions, ignorance, poor health behaviors, scarce health resources, infrastructure and low government expenditure on health(Ajala et al.,2005; Eneji, 2013). Narrowing down this research work to Ondo State Nigeria, this work focused on healthcare expenditure, healthcare status, income and food security of the cocoa farmers’ household in Ondo State.
A large body of research shows that the primary cause of food insecurity is low income (Kreider et al., 2011; Oladapo & Olajide, 2015). A constrained or limited income may force household to make difficult decisions that can result to a less adequate supply of food. This is conceivably best illustrated in Edin and Laura (1997) making ends meet’s qualitative study; the report shows how some poor urban mothers chose to go without food rather than forgo other essentials, such as medical care.
Despite numerous studies on household food insecurity and health (Alaimo et al., 2001; Shannon, 2014; Siefert et al., 2001; Olajide, 2014), knowledge of the relationship between food security and accessibility to healthcare services is limited, and food security policies tend to miss this (Sipsma et al., 2013). Thus, this research sought to fill this gap by focusing on the healthcare service accessibility and food security of cocoa farmers to provide answers to the following research question:
(1) What is the level of healthcare services accessibility to cocoa farmers in the study area?
(2) What are the effects of the healthcare cost on the farmer's income?
(3) What is the relationship between the farmers’ healthcare accessibility and food security?
This paper is based on the theory and application of demand for health. Demand for health model has been argued to be one of the major achievements in theoretical health economics (Hartwig and Sturm, 2018). It is structured around three concepts: the indifference map, health production function and budget constraints. The indifference map is a means of representing diagrammatically the assumption that people value health and other things in life but do not place an overriding value on their health. The health production function expresses the idea that people "produce" their health by accessing "health inputs", such as healthcare services. The budget constraint indicates that individuals have only limited incomes to finance their health production and other activities, and that neither their health production nor their other activities are costless. The basic proposition of this model is that healthcare services can be viewed as a capital stock that produces an output of healthy being over time (Jason, 2019).
MATERIALS AND METHODS
Study area
This study was conducted in Ondo State, Southwestern region of Nigeria located between latitude 50° 451 and 80° 151 North and longitude 40° 451 and 6° East which means that the state lies entirely in the tropics. Ondo State has 18 Local Government Areas (LGAS) with Akure as the state capital and a teeming population of 3,441,024 persons (NPC, 2007). The vegetation comprises coastal and mangrove marsh forest in the south, humid lowland forest, and the forest grassland in the north. Dampness is high during the rainy season and low during the harmattan period of the dry season (Akindele, 2013). Agriculture was reported to be the main occupation of the people in the state and it provides income and employment for over 75% of the population in the state. It also contributes well over 70% of the state’s Gross Domestic Product (GDP) (Ministry of Agriculture, Fisheries and Forest Resources Annual Reports, 2006).
The farmers in the state grow food such as cassava, yam, rice, among other crops and cash crops such as cocoa, cashew, palm, timber for both domestic consumption and export (Oseni and Adams, 2013), but cocoa still remains the major cash crop in the state. The southern zone of the state is where agricultural tree crops like cocoa, rubber, oil palm, and cashew are planted in abundance. As far as cocoa is concerned, about 60% of the nation’s output is produced in Ondo State (IITA, 2007).
Data collection
Primary data were collected through the use of a well-structured questionnaire and personal interviews from cocoa farmers. The questionnaire was structured to collect socio-economic information of cocoa farmers in the study area as well as production activities, food security, healthcare accessibility, assets, income and expenditure.
The multi-stage sampling technique was employed in the selection of farming household in the study area. Four local governments (Idanre, Ile-Oluji, Owo and Ondo) were purposively selected from eighteen local government in Ondo State because they are the largest cocoa producers in the state. From each of the four local governments, five villages were randomly selected (to make a total of 20 villages). From each of the twenty villages ten farmers were randomly selected which brought the total number of selected farmers to 200.
The administration of the survey questionnaire followed extensive preparatory qualitative inquiries. First, many villages were visited to conduct a series of informal discussions, next, questionnaire was administered to farmers individually to get information on various aspects. These included agricultural practices, healthcare services, food security, income flow and medical personnel and facilities availability and accessibility.
Data analysis
Selection of healthcare cost and food security indicators
The costs incurred in accessing healthcare services associated with food insecurity included direct and indirect costs. Examples of direct costs are health expenses for diagnosis, treatment, continuing care, therapy, and so forth while non-medical expenditures included costs of transportation to healthcare providers, expenses related to changes in diet, housing, and other similar changes necessary for disease management (Hodgson and Meiners, 1982; Jeph et al., 2000; Perkins et al., 2009). Indirect costs include the loss of resources and/or productivity incurred. It is simply the income or earning lost by farmers in seeking healthcare (Perkins et al., 2009). The idea of a good health, therefore, means healthcare facilities as well as personnel should be made accessible to people at minimum cost.
To operationalize the concept, the direct cost of accessing healthcare was captured in monetary value and the effect of these costs on farmers’ income was analyzed. Healthcare services accessibility was operationalized by generating accessibility index of number of personnel per patient and facility per patient which defines availability and accessibility. Food security indicators on the other hand, in this concept, were captured as the ability to purchase needed food per time which is accessibility/affordability.
Calculation of accessibility index (I.A) and food security status
Four indices of accessibilities (I.A) were computed for this study to determine the accessibility of healthcare services to the respondents (Opaluwa et al., 2010). They are number of patient per medical officer, number of patient per nurse, number of patient per community health workers and number of patient per hospital bed space.
These indices (I.A) can be written as:
I.A1 = Np/Nd (1)
where I.A1 = index of accessibility for number of patient per doctor, Np = number of patients, Nd = number of doctors,
I.A2 = Np/Ns (2)
where I.A2 = index of accessibility for number of patient per nurse, Np = number of patients, and Nn = Number of nurses.
I.A3 = Np/Nc (3)
where I.A3 = index of accessibility for number of patient per community health worker, Np = number of patients, and Nc = number of community health workers.
I.A4 = Np/Nb (4)
where I.A4 = index of accessibility for number of patient per hospital bed, Np = number of patients and Nb= number of hospital beds
Calculation of food security status
Food security index was used to analyze food insecurity status (indices) of the household. The expenditure on food per household was converted to per capita food expenditure for each household. This was achieved by dividing the expenditure of the whole household with the household size giving us the equivalent spending of each member of the household on food per year. This was summed up to get the total per capital food expenditure which was further simplified to obtain the mean of per capita food expenditure of all household members. To calculate the food security index, two-third of the mean per capita food expenditure of all households was obtained, then the per capita food expenditure for each household was divided by two-thirds of the mean per capita food expenditure of all household members.
According to Iorlamen et al. (2014), a households is considered food secured if at least its monthly food expenditure is above or equal to two-third of the mean per capita monthly food expenditure of all the households.
Food Security Index (Fi) = Per capita food expenditure for each of the household (N) (5)
2/3 mean per capita food expenditure of all households (N)
where Fi = food security index, Fi ≥ 1… Food secured and Fi < 1… Food unsecured.
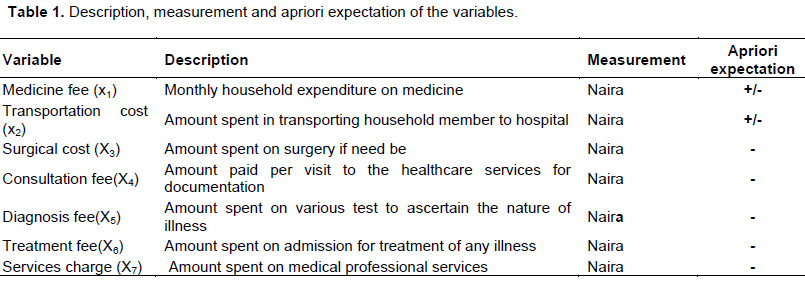
The effect of the cost incurred by farmers to seek healthcare on the farmer's income and the relationship between the healthcare accessibility and food security was analyzed using Tobit model. The Tobit model is developed to estimate linear correlations between variables when there is either left- or right-censoring in the dependent variable. It is used when the dependent variable is continuous although bounded but not limited to binary and also permits analyzing dependent variables with zero as their lowest value (Luo & Bu, 2018). This was one of the reasons it was considered here against Probit or Logit. Some of the selected cost included the farmers’ health status. This is to examine the frequency of visiting the health care centers, consultation fee, medicine cost, treatment charges, and diagnostic fee, transportation cost to measure the direct and indirect cost of accessing healthcare services incurred by the farmers. Majority of these costs were expected to have negative effect on farmers’ income. Also the relationship between the farmers’ healthcare accessibility index and their food security was expected to be statistically significant (Table 1).
Tobit model was represented as:
Y = Sqx + e (6)
where Y = vector of dependent variable, x = vector of explanatory variables predictors, q = Tobit coefficients, and e = random error term.
Implicit form of the model was specified as follows:
Y= f (X1, X2, X3, X4, X5, X6, X7, e), (7)
where the explanatory variables included in the model are Y = Food security (Dependent variable), X1 = Medicine cost (in #), X2 = Transportation cost, X3 = Surgical cost, X4 = Consultation fee (in #), X5 = Diagnostic fee (in #), X6 = Treatment charges (in #), X7 = Service charges (in #), and e = error term.
RESULTS AND DISCUSSION
Access to healthcare services
The index of accessibility was used to ascertain if healthcare was accessible to them in the study area using the number of health personnel and facility available to a patient and the result is shown. Table 2 reveals that Ondo West LGA has the lowest number of patients per doctor, which is at ratio 5 to 1, Idanre LGA has approximately 9 patients per doctor which is the highest ratio, Ile Oluji LGA has approximately 8 patients per doctor while Owo LGA has about 7 patients per doctor.
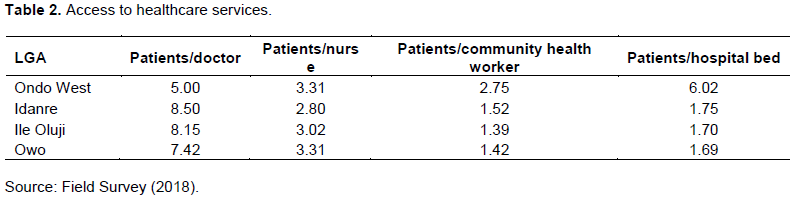
Also, each of the four LGAs (Owo, Idanre, Ile Oluji and Ondo west) has approximately 3 patients per nurse, which implies that Ondo State employed the services of nurses as healthcare personnel than doctors or we can say that nurses were mostly deployed to rural area as healthcare personnel discharging or administering healthcare services to cocoa farmers in Ondo State. Furthermore, Owo and Ile Oluji LGAs have approximately 1 patient per community health workers, which means community health workers are highly sufficient in the local government area. Idanre LGA has approximately 2 patients per community health workers while Ondo west has approximately 3 patients per community health. Lastly, all the 4 LGAs sampled in Ondo State have approximately 2 patients per hospital bed except Ondo west local government that has 6 patients per hospital bed which means there is insufficient distribution of hospital beds especially in the rural areas.
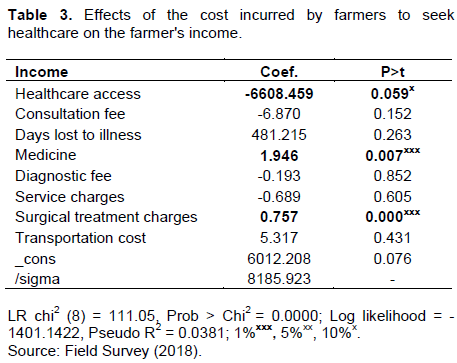
Effects of the cost incurred by farmers to seek healthcare on the farmer's income
Income exhibits a direct relationship with healthcare service accessibility. Therefore, farmers’ incomes are drastically negatively affected if the cost incurred in accessing the healthcare services is high. Medicine and surgical cost was found significant to the farmer’s income and also Prob > Chi2 of 0.000 confirms the model is statistically significant. Some notable variables for accessing healthcare facility such as service cost, diagnostic cost, consultation fee and healthcare access has a negative effect on income. As shown in Table 3, the negative value of coefficients implies that higher value of the variables could decrease the farmers income in such a way that as little as a consultation fee is, a unit increase in the consultation fee could lead to 6.87 decrease in farmers income. A unit increase in service fee could lead to 0.69 decrease on the farmers’ income, a unit increase in diagnostic cost could lead to 0.19 decrease in income and a unit increase in the usage of healthcare services will lead to huge decrease in farmers’ income. This makes consultation fee, diagnostic fee, service fee, health status conform to the apriori expectation of negative relationship implying that an increase in any of these costs could lead to a decrease in the farmers income level which will therefore pose a negative effect on the household food affordability.
Households’ food security status
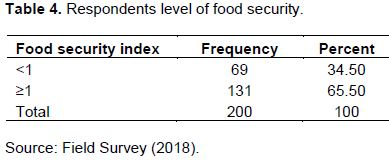
The respondents’ food security level was first profiled before the relationship can be determined. In order to measure the farmers’ food security level, a Food Security Index (FSI) was constructed. Information on household expenditure on food was collected and converted to per capita food expenditure per household and the sum total of the mean of per capita food expenditure of all household was obtained. Further, to calculate the food security index, two-third of the mean per capita food expenditure of all household was obtained and then divided by the per capita food expenditure for each household by two-third of the mean per capita food expenditure of all household. Households whose per capita monthly food expenditure fell above or was equal to two-third of the mean per capita monthly food expenditure of all the households were considered food secure while those below were regarded as food insecure. The result in Table 4 shows that about 65.50% of the respondents were food secured living well at or above two-third of the mean per capita monthly food expenditure of all the household while 69 of the 200 farmers sampled, representing 34.50% were found to be food insecure. The mean of Food Security Indices for the insecure and secure households were given as 0.58 and 1.98, respectively.
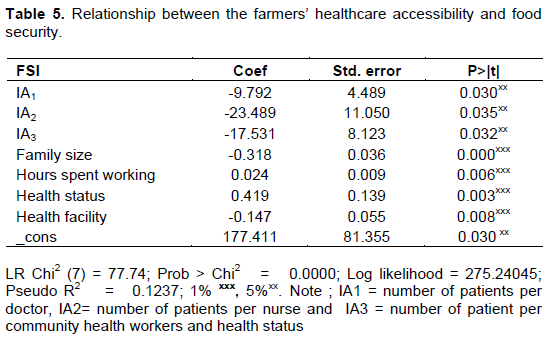
Relationship between the farmers’ healthcare accessibility and food security
The relationship between healthcare accessibility and food security index was analyzed using Tobit. The result as presented in Table 5 shows that sigma (standard deviation) was 0.11, the model has a high negative Log pseudo likelihood = -275.24, altogether describing a model displaying a good fit and normal distribution of the error term. Variables that had expected signs were number of patients per doctor, number of patients per nurse, number of patient per community health workers and health status, family size, hours spent working and health facility that are significant at either 1 or 5% level of significance. Some of the coefficients were positive while some were negative. A positive coefficient indicates that a higher value of the variables tends to increase the likelihood of being food secured. Similarly, a negative value of coefficients implies that higher value of the variables could decrease the probability of food security. Household/Family size has long been noted to be a determinant of food security status. Variable’s negative coefficients of -0.32 and its p-value significance at all level of significance shows the relevance of how the variable determined food security status. This result follows a priori expectation that with more mouth to feed, more hospital bills to foot, less number of health personnel and facility, health status and fixed means of production, the chances of worsening food security status is high.
CONCLUSION
Accessibility is a vital component of the health services. The study revealed that healthcare personnel and facility were unequally and inadequately accessed among cocoa farmers of Ondo State, Nigeria. This was evident from the number of personnel available to patients from one local government to another. The local government with reasonable personnel does not have needed facility as simple as hospital bed which says proper examination may be a difficult task in such area. Some cost incurred in accessing available healthcare facilities had negative effect on the income of the respondents in the study area thus depriving most of them the access to improved health facilities because with high cost, farmers with lower income might not be able to access it. And those that access because they have no alternative did with huge minus to their income which invariably will have effect on the food security. Family or household size, medicine expenditure, service charges on health, surgical treatment cost, number of patients per doctor, number of patients per nurse and number of patients per community health workers, health facility, hours spent working and health status, were found to be the influencing factors of household food security.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGMENTS
This research received partial funding from Agricultural Policy Research in Africa (APRA) and unknown reviewers. Therefore we would like to acknowledge and extend our sincere gratitude.
REFERENCES
|
Akindele SO (2013). Tree Species Diversity and Structure of a Nigerian Strict Nature Reserve. Tropical Ecology 54(3):275-288. |
|
|
Aghion P, Peter H, Fabrice M (2010). The Relationship between Health and Growth: When Lucas Meets Nelson-Phelps. National Bureau Economics Research (NBER) Working Paper No. 15813. |
|
|
Ajala OA, Lekan S, Adeyinka SA (2005). Accessibility to Health Care Facilities: A Panacea for Sustainable Rural Development in Osun State Southwestern, Nigeria: Journal of Human Ecology 18(2):121-128. |
|
|
Alaimo K, Olson CM, Frongillo EAJ, Briefel RR (2001). Food insufficiency, family income, and health in US preschool and school-aged children. American Journal of Public Health 91(5):781-786. |
|
|
Asenso-Okyere K, Chiang C, Thangata P, Andam KS (2011). Interactions between Health and Farm-Labour Productivity IFPRI food policy reports". |
|
|
Barrett CB (2010). Measuring Food Insecurity. Science 327(5967):825-828. |
|
|
Currie J, Madrian BC (1999). Health insurance and The Labor Market. New York: Elsevier Science. |
|
|
Edin K, Laura L (1997). Making Ends Meet. Russell Sage Foundation. JSTOR, |
|
|
Eneji MA, Dickson VJ, Onabe BJ (2013). Health care Expenditure, Health Status and National Productivity in Nigeria (1999-2012). Journal of Economics and International Finance 5:258-272. |
|
|
Farlex (2018). Healthcare, Online Dictionary. |
|
|
Food and Agricultural Organization/World Health Organization, (FAO/WHO) (1992). International Conference on Nutrition and Development. A Global Assessment 3:46. |
|
|
Gillespie GW, Johnson SE (2010). Success in farm start-ups in the Northeastern United States. Journal of Agriculture, Food Systems, and Community Development 1(1):31-48. |
|
|
Hartwig J, Sturm JE (2018). Testing the Grossman model of medical spending determinants with macroeconomic panel data. European Journal Health Economics 19(8):1067-1086. Epub 2018 Feb 16. PMID: 29453763. |
|
|
Hodgson TA, Meiners MR (1982). Cost-of-illness methodology: a guide to current practices and procedures. The Milbank Memorial Fund Quarterly Health Society 60:429-462. |
|
|
IITA (2007). Towards a Sustainable Cocoa Economy: Managing rural transformation in West Africa cocoa producing communities. |
|
|
Iorlamen TR, Abu GA, Lawal WL (2014). Assessment of expenditure on food among urban household and its implication for food security: Evidence from Benue State, Nigeria. African Journal of Food, Agriculture, Nutrition and Development. 14(2). |
|
|
Jason S (2019). The Grossman model. Healthcare Economist,Unbiased Analysis of Today's Healthcare Issues |
|
|
Jeph H, Charles CB, Boccuzzi SJ, Weintraub WS, Ballard DJ (2000). Household income losses associated with Ischaemic heart disease for US employees. Pharmaeconomics 17(3):304-314. |
|
|
Oseni JO, Adams AQ (2013). Cost Benefit Analysis of Certified Cocoa Production in Ondo State, Nigeria. No 161631, 2013 Fourth International Conference, September 22-25, 2013, Hammamet, Tunisia from African Association of Agricultural Economists (AAAE). |
|
|
Kreider B, Gundersen C, Pepper J (2011). The Economics of Food Insecurity in the United States. Applied Economic Perspectives and Policy 33(3):281-303. |
|
|
Luo Y, Bu J (2018). When are emerging market multinationals more risk-taking? Global Strategy Journal 8(4):635-664. Maddala GS (1983). Limited-dependent and qualitative |
|
|
Maxwell DG (1996). Measuring Food Insecurity: The Frequency and Severity of 'Coping Strategies." Food Policy 21(3):291-303. |
|
|
Ministry of Agriculture, Fisheries and Forest Resources, Annual Reports, 2006. |
|
|
National Population Commission (NPC) (2007). Population Figure. Federal Republic of Nigeria, Abuja. Retrieved from http://www.npc.gov |
|
|
Nwaru JC (1993). A Comparison of the Allocative Efficiency of Cooperative and Non- Cooperative Farms in Food Crop Production in Imo State, Nigeria. Nigerian Journal of Agricultural Teacher Education VI (1 & 2): 239 -248. |
|
|
Olajide OA (2014). Household-food market relations and its implications for food security of farm families in Imo state Nigeria. African Journal of Food, Agriculture, Nutrition and Development. |
|
|
Olusesan O, Olajide OA (2015). Land-Income-Nutrition Nexus: Implication for Food Security of Rural Households in Nigeria. Journal of Agriculture and Sustainability 8(2):29-42. |
|
|
Opaluwa H, Otitolaiye J, Onuche U (2010). Accessibility to Improved Health Care as a Means to Economic Empowerment in Rural Kogi State, North Central, Nigeria. Research Journal of Agriculture and Biological Sciences 6(6):1036-1041. |
|
|
Perkins M, Ellen B, Themmen E, Bassane B, Djeneba D, Angeline M, Tuntufye M, Olipa N (2009) Out-of-pocket costs for fertility based maternity care in three African countries. Health policy planning 24(4):289-300. Epub 2009 April 3. |
|
|
Peters DH, Garg A, Bloom G, Walker DG, Brieger WR, Rahman MH (2008). Poverty and access to healthcare in developing countries. Annals of the New York Academy Sciences 1136(1):161-171. |
|
|
Pinstrup-Andersen P (2009). Food security: definition and measurement. Food Security 1(1):5-7. |
|
|
Poppy GM, Chiotha S, Eigenbrod F, Harvey C, Honzák M, Hudson M, Jarvis A, Madise N, Schreckenberg K, Shackleton C, Villa F, Dawson T (2014). Food security in a perfect storm: Using the ecosystem services framework to increase understanding. Philosophical transactions of the Royal Society of London. Series B, Biological sciences 369(1639) 20120288. 10.1098/rstb.2012.0288. |
|
|
Shannon J (2014). Food deserts: Governing obesity in the neoliberal city." Progress in Human Geography 38(2):248-266. doi:10.1177/030913251348437 |
|
|
Siefert K, Heflin CM, Corcoran ME, Williams DR (2001). Food insufficiency and the physical and mental health of low-income women. Women and Health 32(1-2):159-177. |
|
|
Sipsma H, Ofori-Atta A, Canavan M, Osei-Akoto I, Udry C, Bradley EH (2013). Poor mental health in Ghana: who is at risk? BMC Public Health 13(1):288. |
|
|
Titus OB, Adebisola OA, Adeniji AO (2015). Health-care access and utilization among rural households in Nigeria. Journal of Development and Agricultural Economics 7(5):195-203. |
|
|
World Health Organization (WHO) (1978). International Conference on Primary Health Care, Alma Ata. |
|
|
World Health Organization (WHO) (2013). Universal health coverage and universal access bulletin. 91:546-546A. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


