ABSTRACT
This study examined healthcare access and utilization among rural households in Ogun state, Southwestern Nigeria. Primary data were collected through the use of structured questionnaires. Multistage sampling technique was employed for the selection of 200 rural households. The data were analyzed using descriptive statistics and health care accessibility index. The results show that the mean age of the respondents was 46 years with an average household size of 8 members. Majority of the respondents (43.5%) had no formal education and farming is the main occupation of respondents. Fifty-eight percent of the respondents have access to health care services while only 42.50% utilized these services. Most of the respondents (40.5%) travel a distance of 5-9 km before accessing health care facilities. Accessibility indices reveal unequal access to modern health facilities in the study area. Therefore this study recommends that rural development policies should promote the creation of enabling environment to enhance participation and equitable accessibility in modern health care delivery across the rural areas in the country.
Key words: Healthcare, utilization, rural households, Nigeria.
Sound health is a fundamental requirement for living a socially and economically productive life. Poor health inflicts great hardships on households, including debilitation, substantial monetary expenditures, loss of labour and sometimes death. The health status of adults affects their ability to work, and thus underpins the welfare of the household, including the children’s development (Asenso-Okyere et al., 2011). Poor health affects agricultural production. Treatable conditions often go untreated because of lack of access to healthcare. Development in all its forms is only possible when there is access to healthcare service and in turn its effective utilization by individuals.
Access to healthcare services is a multidimensional process involving the quality of care, geographical accessibility, availability of the right type of care for those in need, financial accessibility, and acceptability of service (Peters et al., 2008). The utilization of healthcare services is related to the availability, quality and cost of services, as well as to social-economic structure, and personal characteristics of the users (Chakraborty et al., 2003; Manzoor et al., 2009; Onah et al., 2009).
In developing countries, the under-utilization of the health services in public sector has been a universal phenomenon (Zwi, 2001). The state of the Nigerian health system is dysfunctional and grossly under-funded with a per capita expenditure of US$ 9.44 (World Bank, 2010). As a result, Nigeria still has one of the worst health indices in the world and sadly accounts for 10 percent of the world’s maternal deaths. The National health management information system is weak, without an integrated system for disease surveillance, prevention and management. Research also indicates that there are high rates of absenteeism (about 40%) among medical doctors, especially in rural areas (Hamid et al., 2005). The high level of mortality, and morbidity which accounts for 157 deaths per 1000 live births (NDHS, 2008), non-attainment of international goals for health and survival, and the inequalities in access to health facilities are the challenges of rural populace.
According to the Federal Ministry of Health (2008), the total shares of public ownership in 2004 on health facilities were 14,607 while the private sector accounted for 9,029 in Nigeria. Consequently, various Nigerian governments have made numerous great efforts toward the provision of healthcare facilities to its populace. Notable among these efforts were the expansion of medical education, improvement of public health care systems, provision of primary health care (PHC) in many rural areas. However, overt attention has not been paid to equity in the planning and distribution of health care facilities over the years in the country. Public and private health care facilities are sparsely provided in many rural areas within the country. Such regions with difficult terrain and physical environment are often neglected (Onokerhoraye 1999). This makes the distance between the rural dwellers and the healthcare center far apart, given the transportation problems experienced in these areas, and its attendant cost. Many rural areas do not have clinics; the sick must be carried on the backs of young men or on bicycles to the nearest clinic. Moreover, clinics in rural areas often lack adequate equipment or trained health personnel, and they require payment before providing services. In the absence of health insurance, rural people are often unable to afford healthcare of any kind.
Healthcare access and utilization are of major interest to rural development, because they are vital elements of wellbeing and components of human capital (Aghion et al., 2010). In rural areas, where physical jobs tend to be more abundant, healthcare access and utilization stand to be more important than education in determining labour productivity. Furthermore, every individual sees good health as a need; this makes healthcare utilization an economic good. Good health is a need for all and the choice of a particular healthcare system respond to the laws of demand and supply, the demand for health care is a derived demand. Health care is not demanded for itself but for the advantages that can be derived from being healthy.
Many low-income countries, Nigeria inclusive, have not been able to meet the basic healthcare needs of their people, especially those in the rural areas. In Nigeria, there has been a growing recognition of the challenge of rural people’s health issues and the need for it to be addressed (Hamid et al., 2005). There is a huge shortage of qualified practitioners in the rural areas. Accessing health care in rural areas is confounded by problems such as insufficient health infrastructure, the presence of chronic diseases and disabilities, socioeconomic and physical barriers (Ricketts, 2009).
Over the years, Ogun State healthcare services and facilities have not achieved all its objectives of ensuring that everybody has access to adequate health care services at affordable costs. This study will extend prior literature such as: Sanusi and Awe (2009) who studied the level of awareness of National Health Insurance Scheme (NHIS) by health care consumers in the south west of Nigeria using chi-square and descriptive statistics. Ibiwoye and Adeleke (2009) examined the extent to which income of household heads, occupation of household heads, sex of household heads, age group, marital status and family size plays an explanatory role in the slow pace of usage of healthcare service in Lagos State; while Olugbenga-Bello and Adebimpe (2010) examined the knowledge and attitude of civil servants in Osun State towards its healthcare usage. However, this research work fills the huge knowledge gap examining the access and utilization of health care services among rural households in Ogun State. Specifically, this study intends:
(1) To identify rural household access and use of health care services in relation to their socio-economic characteristics.
(2) To determine the level of accessibility of rural households to healthcare facilities.
The study area is Ogun State, Southwest of Nigeria. The total land area is 16,409.26 km². It is bounded by Benin Republic to the West, Lagos State and the Atlantic Ocean to the south, Ondo State to the East, and on the North by Oyo and Osun States. It is situated between Latitude 6.2°N and 7.8°N and Longitude 3.0°E and 5.0°E. The main cash crops produced in the State are cocoa, cashew, kola nut, oil palm and palm kernels, rubber and coffee.
Primary data employed in this study were obtained with the aid of well-structured questionnaires. A multi-stage sampling technique was employed in the selection of respondents. The first stage involved the selection of the entire four Agricultural zones while the second stage involved the random selection of two Blocks (LGA) from the zones. In the third stage, five cells (Villages) each were randomly selected from the blocks (LGA) amounting to 10 cells across the zones. The fourth stage was the random selection of 210 households proportionate to size of the selected cells. However, a total of 200 questionnaires with consistent reports were used for analysis.
The analytical techniques used in this study include descriptive statistics and Healthcare Accessibility Index. Descriptive statistics such as frequencies, means, percentages and standard deviation were used to describe the sources and uses of healthcare facilities in relation to socio-economic characteristics as well as the level of utilization of health care services.
Healthcare Accessibility Index was used to analyze the second objective which is to determine the level of accessibility of the rural households to healthcare facilities. The data set was segregated based on the wards in the selected local government areas in the state. The segregation of the data generated the pattern of distribution of the health care facilities in the study area. The pattern evolved revealed the extent of inequality among the local government in terms of the provision of the health care facility by both government and private sector in the area. The index of accessibility to health care services was computed using three variables from the data set. The variables used are population ratio to bed space in each LGA: population ratio to medical doctor and population ratio to nurses/ mid-wife. The choice of these three variables is because doctors and nurses are directly involved in providing health care services to the people and bed spaces is a basic requirement in health care delivery.
The indices are household size per medical officer (I.A1); Household size per nurse (I.A2); number of people in households per community health workers (I.A3); and household size per hospital bed space (I.A4). These indices are expressed as:
RESULTS AND DISCUSSION
Where:
I.A4= index of accessibility for number of persons per hospital bed
Np = number of persons in the households
Nb= number of hospital beds
Socio-economic characteristics of respondents
The distribution of the respondents according to their socio-economic characteristics, access to health care services and utilization is as reported below:
Gender of household head
Table 1 show that 58% of the respondents have access to health care services while only 42.50% utilizes these services. 71% of the household heads were males while the remaining 29% were females. However, 41% of the male headed households have access to healthcare services while 17% of the female headed households have access to healthcare service. Out of these, about 78 and 61.76% of the male and female respectively, utilized healthcare service. This shows that the majority of the respondents were males. Male headed households have more access to healthcare services than female headed households which in turn makes them utilize healthcare services more in the study area.
Age of household head
Table 2 reveals that 71% of the respondents are in their economic active age (≤ 50 years). About 75.55% of the respondents within this age bracket accesses and utilizes healthcare service more than the elderly ones because they still have more energy to travel a wide distance to access the healthcare facilities. The mean age is 46 years. Majority (34.4%) of the respondents are within ages 41 to 50 years, 20% have access to healthcare services while 77.5% with access utilized the health care services. The least are those above the age of 60 years.
Marital status of household head
Table 3 indicates that 69% of the respondents were married while 31% are unmarried/divorced. Out of the married, 40% have access to healthcare services while 77.5% of those with access utilized healthcare services provided in the rural area. Since most of the respondents were married, additional cost is incurred to maintain health of the wife during child birth as well as the upkeep of the children which may increase the participation of the respondents in health care use.
Educational status of household head
As shown in Table 4, 43.50% have no formal education while 6, 23.5, 11.5, and 15.5% had adult, primary, secondary and tertiary education respectively. Thirteen percent of those with primary education had access to health care services while 78.57% out of these, utilized the healthcare services. Furthermore, 24.5% of those with no formal education had access to healthcare service while 69.23% of the respondents utilized healthcare services. Hence, the level of education and literacy of a household will determine the kind of choices he takes especially in healthcare use. Most of the respondents in the study area are educated and this would have informed their healthcare choices.
Primary occupation of household head
Table 5 showed that 37% of the respondents are engaged in farming as their primary occupation while 7.5, 21.5, 23, 4% and 7% are artisans, traders, salary earners, wage earners and other forms of employment. This shows that farming is the predominant occupation in the study area. More so, farmers have the highest (26%) access to healthcare service with the lowest proportional (63.46%) uses of healthcare service. This is as a result of the fact that most households in the rural area depend mainly on agriculture, as their primary source of livelihood and cannot afford to pay for the high cost of healthcare services.
Distance of respondents to healthcare facilities
Table 6 shows that majority (40.5%) of the rural households lived 5 to 9 km to a public health center with 21% having access to healthcare facilities and 85.7% utilizing the facilities. Eleven percent of respondents living 4 km from the healthcare service provider have access to healthcare facilities while 90.09% of the respondents utilized it. 13% of the respondent who lives 10 to 14 km from healthcare service had access while 61.11% utilized the services. Forty-three percent of respondents living more than 14 km to their healthcare providers makes use of the available healthcare facilities. The result, therefore, indicates that utilization of available health facilities increases with proximity to the health centers.
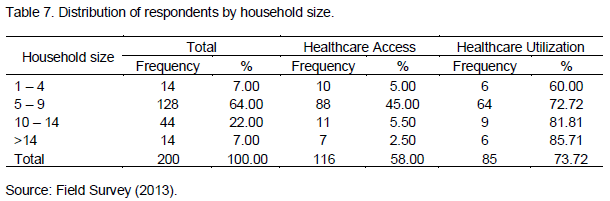
Household size
The mean household size was 8 members. Table 7 reveals that 7% of respondents have family size of 1-4 members per household, whereas only 60% of the respondents within this group with access to healthcare facilities utilized it. Furthermore, those with household size above 14 members have the highest health service utilization with 85.71%.
Healthcare utilization pattern of the household
From the result, 11.50, 17.05, 5.50 and 24.0% have access to self-care, government, private and traditional healthcare provider respectively (Table 8). Traditional healthcare was the most frequently utilized by the respondents, followed by self-care while private healthcare was the least. Out of those with access to traditional health care, 83.33% utilized it while 78.26, 61.76 and 54% utilized self-medication, government and private hospitals respectively. Traditional healthcare is mostly utilized because of its easy accessibility and low cost of treatment compared with the other forms of healthcare providers.
UTILIZATION OF HEALTHCARE FACILITIES
Utilization of health facilities by age
Age is expected to be positively related to utilization of health facilities (Dias et al., 2008). However, as depicted in Table 9, majority of household heads in their active and economic age seek health care from government hospitals with a few of them utilizing self-care and traditional care. Private hospitals are least utilized across the various age groups probably because of the high cost associated with their services since private health providers are out to maximize profit. The table further show that a higher proportion of the household heads within the age brackets of 20 to 30 years (40.74%) and 31 to 40 years (43.48%) utilized government hospitals, while those in age groups of 41 to 50 years (39.13%) sought healthcare from traditional sources. However, self-medication and traditional care are mostly utilized among household heads above 50 years of age.
Utilization of healthcare facilities by gender
The highest proportion of male-headed households (33.90%) utilized traditional health care facilities while 41.38% of female-headed households used self-medication (Table 10). However, a higher proportion of male-headed households (30.99%) seek modern health care services than female-headed households (27.59%). This implies that the level of utilization of modern health facilities is lower among female-headed households than among their male counterparts. This is consistent with the findings of Dias et al. (2008). This might be as a result of low level of access to productive assets among rural female-headed households.
Utilization of healthcare facilities by household size
The result shows that while utilization of modern health facilities decreases with household size, utilization of traditional health care facilities increases with household size (Table 11). Most of the households with 1 to 4 members utilized government hospitals while 28.57 and 35.71% of households with more than 14 members utilized self-care and traditional care respectively. The result further shows that private hospitals are least utilized in the rural area probably because of high cost of consultation. It can be deduced that larger sized households may not be able to afford modern health facilities and thus turn to the utilization of self-medication and traditional health care services, which they consider relatively cheaper as a larger share of household expenditure will be spent on food.
Healthcare utilization by educational status
Education has an important effect on utilization of health care facilities. The result in Table 12 shows that the highest proportion (24%) of the rural household heads has primary education. The result also reveals that a larger percentage (67.69%) of households whose heads have tertiary education utilized modern health care facilities (government and private hospitals) while a higher percentage (68.96%) of households heads with no formal education do not utilize modern healthcare facilities. Likewise, 75% of households whose heads undergo adult literacy education do not utilize modern healthcare facilities. The result follows the findings of Mekonnen and Mekonnen (2002) that utilization of modern health care facilities increases with educational attainment.
Distance on the utilization of health facilities
Table 13 shows that only 39 households which represent 19.5% of the rural households live close (≤ 4 km) to a public health centre. Majority (35.9%) of the rural households within this distance seek healthcare services from government hospitals while a higher proportion (41.67%) of rural households living farther than 14 km utilized the traditional health centers. The result, therefore, indicates that utilization of available public health facilities increases with proximity to the health centers, thus, rural households utilize self-medication and traditional care closer to their residence. This is expected to reduce their cost of transportation and rigour of accessibility to distant modern healthcare services.
Accessibility to healthcare services
Accessibility of health services has been shown to be an important determinant of utilization of health services in developing countries (Mekonnen and Mekonnen 2002). The result of the indices of accessibility to Public Health care facilities show that there is an average 111, 20, 61 and 6 patient to a doctor, a nurse, a community health worker and a hospital bed respectively (Table 14). This suggests that there is inadequate supply of health workers in the rural public health centers. This might reduce the level of utilization of such centers due to much time spent in accessing health care. The result further shows that there is inadequate supply of public health care facilities (both human and infrastructural) in rural Ogun State. Furthermore, there is unequal access to modern healthcare by the respondents in the study area. The patient ratio per health personnel goes a long way to determine the workload of the personnel and their efficiencies on the job. The number of patients to attend to per health personnel determine the waiting time of the patient, thereby measure the accessibility of patient to medical facilities. The lower the number of patients per health personnel, the better the accessibility of health care facilities. Bhattia and Cleland (2001) in their study have noted that the high use of private health care is due to easy access, shorter waiting time, longer or flexible opening hours, better availability of staff and drugs, and better attitude of staff.

CONCLUSION AND RECOMMENDATION
This study has shown that there is unequal distribution of health facilities as well as low level of accessibility of household to medical facilities in the study area. To this end, governments at all tiers should ensure equitable accessibility to health care delivery across the rural areas by deploying more medical and para-medical staffs to the rural areas. Rural development policies should promote the creation of enabling environment to enhance participation in modern health care delivery. Household heads should be encouraged to utilize modern healthcare facilities by organizing a sensitization programme to create awareness about the importance of using modern healthcare facilities. There should be establishment of public health centers in the core rural areas. This will increase the proximity and accessibility of rural people to public health facilities.
The authors have declared that no conflicting interest exists.
REFERENCES
Aghion P, Peter H, Fabrice M (2010). "The Relationship Between Health and Growth: When Lucas Meets Nelson-Phelps." National Bureau Econ. Res. (NBER) Working Paper No. 15813.
CrossRef |
|
|
|
Asenso-Okyere K, Chiang C, Thangata P, Andam KS (2011). Interactions between health and farm-labour productivity. International Food Policy Research Institute, Washington, DC. |
|
|
Bhattia JC, Cleland J (2001). Health care seeking and expenditure by young Indian mothers in the public and private sectors. Health Pol. Plan 16:55–61.
CrossRef |
|
|
Chakraborty N, Islam MA, Chowdhury RI, Bari WW, Akhter HH (2003). Determinants of the use of maternal health services in rural Bangladesh. Health Prom. Int. 18(4): 327-337.
CrossRef |
|
|
Dias SF, Severo M, Barros H (2008). Determinants of health care utilization by immigrants in Portugal. BMC Health Serv. Res. 8:207.
CrossRef |
|
|
|
Federal Ministry of Health (2008). The Nigerian Health Financing Policy, Federal Ministry of Health (FMOH), Abuja, Nigeria. |
|
|
|
Hamid SA, Sadique Z, Ahmed S, Molla AA (2005). Determinants of choice of healthcare providers: Evidence from selected rural areas of Bangladesh. Pak. J. Soc. Sci. 3(3):437-444 |
|
|
|
Ibiwoye A, Adeleke TA (2009). A log-Linear Analysis of Factors Affecting the Usage of Nigeria's national Health Insurance Scheme. Soc. Sci. 4(6):587-592. |
|
|
Manzoor I, Hashmi NR, Mukhtar F (2009). Determinants and pattern of health care services utilization in post graduate students. J. Ayub Med. Coll. Abbottabad 21(3):100-105.
CrossRef |
|
|
|
Mekonnen Y, Mekonnen A (2002). Utilization of Health Care Services in Ethiopia. Calverton, Maryland, USA: ORC Macro. |
|
|
|
NDHS (National Demographic Health Survey) (2008). Regent Park. Retrieved August 20 1009 from http://www.ndhs.ca/regentpark. |
|
|
Olugbenga-Bello AI, Adebimpe WO (2010). Knowledge and Attitude of Civil Servants in Ogun State South Western Nigeria Towards the National Health Insurance. Nig. J. Clin. Pract. 13(4):421-426.
CrossRef |
|
|
Onah H, Ikeako L, Iloabachie G, (2009). Factors associated with the use of elasticity of healthcare services in Enugu, Southeastern Nigeria. Soc. Sci. Med. 63(7):1870-1878.
CrossRef |
|
|
|
Onokerhoraye AG (1999). Access and utilization of modern health care facilities in the petroleumproducing region of Nigeria: The case of Bayelsa State. Research Paper No. 162. Takemi Program in International Health Harvard School of Public Health. |
|
|
Peters DH, Garg A, Bloom G, Walker DG, Brieger WR, Rahman MH (2008). Poverty and access to healthcare in developing countries. Ann. N Y Acad. Sci. 1136:161-171.
CrossRef |
|
|
|
Ricketts TC (2009). Rural health in the United States. New York: Oxford University Press. |
|
|
|
Sanusi RA, Awe AT (2009). An Assessment Level of National Health Insurance Scheme (NHIS) Among Health Care Consumers in Ogun State, Nigeria. Soc. Sci. 4(2):143-148. |
|
|
|
World Bank (2010). The millennium development goals for health: rising to the challenges. Washington DC: World Bank. |
|
|
Zwi AB (2001). Private health care in developing countries. Br. Med. J. 323:464–466.
CrossRef |