Full Length Research Paper
ABSTRACT
Obesity has reached epidemic proportions globally, and is now prevalent in low-income and middle-income countries. This study sets out to determine the prevalence of obesity as well as its predictors in rural South-Western Nigeria. Cross-sectional descriptive survey of 416 participants aged 20 to 70 years in two rural communities in Remo North Local Government area of Ogun State, Nigeria was taken. Relevant clinical and demographic parameters were obtained. Participants were screened for generalized and central obesity, using standard protocol. The prevalence of overweight and generalized obesity was 21.4 and 10.5%, respectively in all the participants. Females had a higher frequency of generalized obesity than the males (p<0.001). Central obesity was significantly more prevalent among the female participants with three different criteria (p≤0.001). More participants were classified as centrally obese using waist-to-hip ratio (WHR) or waist-to-height ratio (WHtR) than waist circumference (WC). Predictors of central obesity were age, female gender, alcohol and cigarette smoking. The prevalence of obesity is high in rural communities of South-Western Nigeria. Compared to men, the chances of developing central obesity (defined as increased WC) increased by 11-fold among the women. Targeted aggressive healthy lifestyle intervention becomes necessary to prevent future cardiovascular disease.
Key words: Obesity, rural communities, cardiovascular disease.
INTRODUCTION
Obesity has reached epidemic proportions globally with its prevalence nearly doubled since 1980 (World Health Organization [WHO], 2014). WHO (2008), estimated that more than 1.4 billion adults, 20 years and above, were overweight. Of these, over 200 million men and nearly 300 million women were obese. In adults aged 20 years and above, the prevalence of overweight and obesity in 2008 were 35 and 11%, respectively (WHO, 2008).
Overweight and obesity are the fifth leading risk for global deaths, with at least 2.8 million death each year as a result of being overweight or obese (WHO, 2014). Obesity is a major risk factor for hypertension, as well as cardiovascular disease, diabetes, cancers, and musculoskeletal disorders (WHO, 2008; Nguyen and Lau, 2012). Measures of central obesity predict metabolic syndrome, type 2 diabetes, cardiovascular disease, and all-cause mortality better than body mass index (BMI) (Visscher et al., 2001; Goh et al., 2014).
Once associated with high-income countries, obesity is now prevalent in low- and middle-income countries. As more Nigerians adopt civilization or western lifestyle, the prevalence of obesity is expected to increase, with its attendant complications. According to the WHO, the prevalence of overweight and obesity in Nigeria in 2008 was 26.8 and 6.5%, respectively, while that of hypertension was 42.8% (WHO, 2008).
Increasing age, alcohol consumption and cigarette smoking are associated with obesity. Ageing is associated with changes in body composition resulting in increase in fat mass and a decrease in muscle mass (Hughes et al., 2002). Alcohol has an energy value of 7 kcal/g, second only to fat which is the most energy dense macronutrient at 9 kcal/g. Therefore, daily energy intake may rise considerably when alcohol is consumed (Dennis et al., 2009).
The relationship between smoking and obesity is complex. Compared to non-smokers, smokers have lower weight. This is because smoking improves satiety and reduces caloric intake (Wager-Srdar et al., 1984). See comment in PubMed Commons below Fat oxidation also increases with nicotine intake (Jensen et al., 1995). Conversely, smoking cessation is associated with weight gain (Williamson et al., 1991). However, among smokers, tobacco smoking is positively associated with BMI and waist-to-hip ratio (WHR) (Bamia et al., 2004).
There are many reports on obesity in rural Nigeria (Oladapo et al., 2010; Adediran et al., 2012; Iloh et al., 2012; Ahaneku et al., 2011). It is most reported that obesity was more prevalent among women; the magnitude of the problem among women compared to men was not stated. For every man with obesity, how many women are obese? Who should preventive measures target? These questions were not answered by previous studies. Current preventive measures appear to target urban communities. Most health institutions are also concentrated in the urban centres. Thus, many vulnerable rural dwellers are cut-off from curative services. Therefore, prevention is the answer to better health in rural setting, and since resources are scarce, we must identify those individuals at the highest risk of comorbidities in order to identify those who might benefit the most from aggressive weight management.
The aim of this study was to determine the prevalence of obesity, using indices of generalized and central obesity in two rural communities in South-Western Nigeria. The study also sought to determine the predictors of central obesity and the population that preventive measures should focus on.
MATERIALS AND METHODS
Study location
The study was conducted at Isara and Ode-Remo communities, in Remo North Local Government Area of Ogun State, Nigeria from December, 2006 to June, 2007. Ogun State is a state in Western Nigeria. It borders Lagos State to the South, Oyo and Osun States to the North, Ondo State to the East and the republic of Benin to the West. Remo North has an area of 199 km2 and population of 59,911 according to the 2006 census, and its headquarters are located at Isara.
Ethical approval
Approval for the study was obtained from the ethic and research committee of the Olabisi Onabanjo University Teaching Hospital, Sagamu, Ogun State. The consent of the king and community leaders was also sought. The consent of each participant was also obtained.
Study design
This is a cross-sectional descriptive survey.
Study participants/Sampling
The participants included market men and women, artisans, farmers, drivers, and few civil servants typical of the population of rural Nigeria and Africa. The communities were chosen because of the proximity to the researchers’ institution. Initial sensitization visits were paid to the communities, and the participants were told to meet at a designated point for the screening, including the King’s palace, market, town halls, and parks. Participants aged 20 to 70 years, were included in the study. Pregnant women, breastfeeding mothers, those that were unable to stand or who were wheelchair bound were excluded from the study.
All the people who met the inclusion criteria and who gave their consent were included in the study. With the aid of a pre-tested structured interview questionnaire, clinical and demographic parameters such as age, gender, marital status, occupation, history of tobacco use, consumption of alcohol and soft drinks were obtained. Participants who currently smoked cigarette or use tobacco snuffs were regarded as tobacco users. Blood pressure, height, weight, waist and hip circumferences were measured.
Procedure and measurements
Trained assistants helped with data collection and physical measurements. Gender matching was ensured as much as possible.
Anthropometric measurements
Height: The height was measured (in metres) to the nearest 0.1 m with a calibrated meter rule placed horizontally against the wall. The subjects were asked to be barefooted and wore light clothing. Subjects were asked to stand on a flat surface, with weight distributed evenly on both feet, heels together and the head positioned so that the line of vision is perpendicular to the body. The arms hung freely by the sides, and the head, back, buttocks and the heels were in contact with the vertical board. The movable headboard was brought onto the topmost point on the head with sufficient pressure to compress the hair (WHO, 1995).
Weight: The weight was measured (in kilograms) with a weighing scale without shoes and with the patient wearing light clothing, to the nearest 0.1 kg (WHO, 1995). BMI was taken as the ratio of weight (kg) to the square of the height (m2) (WHO, 1995). The BMI was classified as follows: ≤18.5 kg/m2, underweight; 18.5 to 24.9 kg/m2, normal; 25.0 to 29.9 kg/m2, overweight; 30.0 to 34.9 kg/m2, class 1 obesity; 35.0 to 39.9 kg/m2, class 2 obesity; ≥40.0 kg/m2, class 3 obesity (WHO, 1995).
Waist circumference (WC): With the aid of a tape rule, the waist circumference (in centimetres) was taken midway between the inferior margin of the last rib and the iliac crest in a horizontal plane. The subjects stood comfortably with their weight evenly distributed on both feet. Each landmark was palpated and marked and the midpoint determined with a tape measure .The circumferences were measured to the nearest centimetre at the end of normal expiration (WHO, 1995).
Hip circumference: This was measured to the nearest centimetres at the level of the greater trochanters with the subjects wearing underwear or light clothing. The subjects stood erect with arms at the sides and feet together. The greater trochanters were located, and the tape applied snugly against the skin without compressing the soft tissues (WHO, 1995).
WHR was calculated from the values of the waist divided by the hip circumferences. Waist-to-height ratio (WHtR) was calculated from the values of waist circumference divided by the height in centimetres.
Central obesity was defined as (1) WC >80 cm in females or WC >94 cm in males (International Diabetes Federation, 2005), (2) WHR >0.85 in females or >0.90 in males (WHO, 1995), (3) WHtR of 0.5 or more in both men and women (Browning et al., 2010).
Blood pressure measurement
Blood pressure was determined once with a standard mercury sphygmomanometer (Accosons, England) with the subjects in the sitting position and the left arm resting on a table at the same level of the heart. Systolic and diastolic blood pressures were taken as the appearance and disappearance of the Korotkoff’s sounds (Phases I and V), respectively.
Statistical analysis
Data were analysed using the Statistical Package for Social Sciences (SPSS) version 16.0 (Chicago, Illinois, USA). Pearson’s chi-square (c2) test was used to find the association between categorical variables. Student’s t-test was used to compare continuous variables. Categorical variables were expressed as percentages, while continuous variables were expressed as means. Binary logistic regression was used to analyse the predictors of central obesity. The level of significance was set at p<0.05.
RESULTS
Four hundred and thirty three people were screened out of which 412 people with complete data (206 males and 206 females) were analysed, giving a response rate of 95.2%.
Table 1 shows the mean age and the clinical characteristics of the participants. The mean age of all the participants was 44.5±15.6 years. Female participants were significantly older than the male participants (50.7±14.9 versus 38.4±13.8 years, p<0.001). All the obesity-related indices were greater in the female participants. Significantly, the MBI and the WHtR were greater in the female participants (p<0.001). Similarly, the female participants had greater WC and WHR than their male counterparts (p=0.001). The mean blood pressures were similar between the two genders.
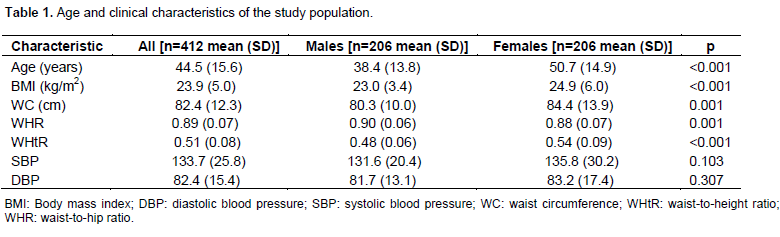
Table 2 shows the prevalence of obesity using different criteria. 21.4% of all the participants were overweight, while 10.5% had generalized obesity. Significantly, generalized obesity was more prevalent among the females participants (p<0.001). Among the females, classes 2 and 3 generalized obesity was found in 4.4 and 1.5%, respectively. Among the males, class 2 general obesity was present in 1.0% and none had class 3 obesity. Central obesity was significantly more prevalent among the female participants with the three different criteria. More participants were classified as centrally obese using WHR than WC (50% versus 12.6% in males and 65.5% versus 56.8% in females). Similarly, more participants were classified as centrally obese using WHtR than WC (29.1% versus 12.6% in males and 62.1% versus 56.8% in females).
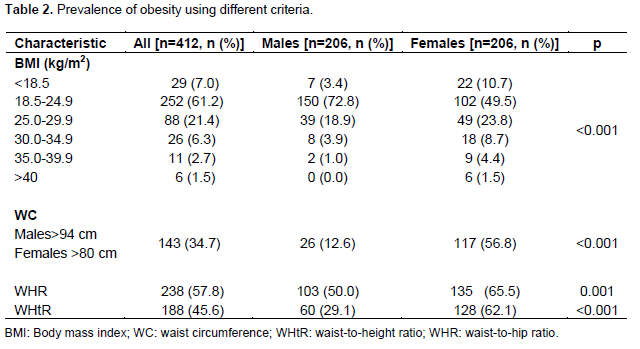
Table 3 shows the prevalence of central obesity in relation to age and gender. Significantly, the prevalence of central obesity using three different criteria increases with age (p<0.001).
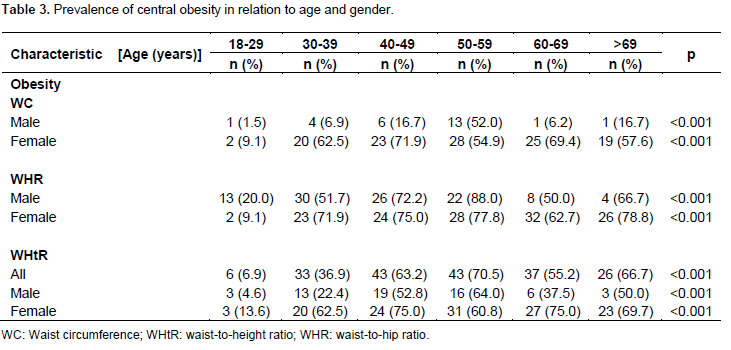
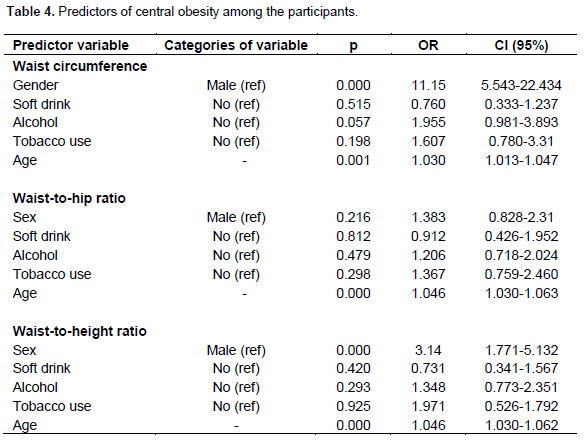
Table 4 shows the predictors of central obesity in the population studied. Age and gender predicted central obesity. The female gender increases the odd of developing abnormal WC and WHtR by 11-fold (p<0.001, 95% confidence interval (CI)=5.543 to 22.434) and 3-fold, respectively (p<0.001, 95% CI=1.771 to 5.132). The models correctly predicted the chances of developing central obesity better than when no predictor variable was built into the model ({WC, prediction increased from 66.0 to 72%, p<0.001, c2=110.4, df=5} {WHR, prediction increased from 57.5 to 69.2%, p<0.001, c2=52.5, df=5} {WHtR, prediction increased from 54.4 to 68.7%, p<0.001, X2=84.4, df=5}). Alcohol and tobacco use also increases the odds of developing increased WC (odd ratio (OR)=1.96, CI=0.98-3.89 with alcohol; OR=1.61, CI=0.78 to 3.31 with tobacco use).
DISCUSSION
Prevalence of obesity
The prevalence of overweight and generalised obesity in this study was 21.4 and 10.5%, respectively. This is higher than a reported prevalence of 1.9 and 2.0% for overweight and obesity, respectively from a study in rural community of a neighbouring state in South-Western Nigeria (Oladapo et al., 2010). It is also higher than a prevalence of global obesity of 4.3% from rural Northern Nigeria (Adediran et al., 2012) and 6.0% from Eastern Nigeria (Iloh et al., 2012). However, it is similar to the findings from other studies with prevalence of obesity between 11.7 and 13.3% in rural communities in South. Eastern Nigeria (Ahaneku et al., 2011; Ulasi et al., 2010).
The prevalence of overweight and global obesity in this study is lower than the findings among the Kalabaris from the South-South Nigeria (22.95 and 47.26%, res-pectively) (Adienbo et al., 2012). The higher prevalence in their study, despite the lower mean age was due to the cultural practice of fattening room visits by the women. In their study, this practice accounted for about 20% increase in the obesity burden in the females, whose obesity prevalence doubled that of the male participants.
The overall prevalence of central obesity in this study ranged from 34.7 to 57.8% depending on the criteria used. It was the highest with WHR (65.5%), followed by WHtR (62.1%), and lowest with WC (56.8%). This is higher than the findings from an earlier study from rural South Western Nigeria and rural Northern Nigeria (Oladapo et al., 2010; Adediran et al., 2012). This study finding is however similar to findings from rural communities in South Eastern Nigeria (Ahaneku et al., 2011; Ulasi et al., 2010). The rising prevalence of obesity in rural areas is due to nutritional transition, coupled with transition away from agricultural (both for production and subsistence) to wage labour that has decreased the physical activity of people (McGarvey, 1991; Snodgrass et al., 2006). Among both men and women, the change in occupation leading to a subsequent decrease in daily physical activity is greater in rural areas.
The higher prevalence of obesity from this study as compared to the Northern Nigeria may be because the residents from South Western Nigeria are likely to more readily adopt western lifestyle, which predisposes to obesity than those from Northern Nigeria. The mean age of this study population was also higher than theirs. Additionally, genetic and environmental factors may also contribute to this disparity in obesity prevalence.
Similar to previous local studies, both generalized and central obesity were more prevalent among the female population in the current study (Oladapo et al., 2010; Adediran et al., 2012; Iloh et al., 2012; Ahaneku et al., 2011; Adienbo et al., 2012; Desalu et al., 2008; Chukwuonye et al., 2013). A similar trend was reported by WHO (2008). Women are usually less active than men who engaged more in farming and other physical activities. The female participants were also significantly older than their male counterparts, and this affects obesity prevalence as discussed subsequently. Sociocultural beliefs may also play a role in the gender difference in obesity prevalence. Obesity, especially among women in some parts of Nigeria is ascribed to affluence and good nutrition. The practice of fattening room visits by women in South-South Nigeria is due to the belief that it enhances fertility (Adienbo et al., 2012). Futhermore, the nutritional transition that is on-going in developing world has greater impact on obesity among women. This is due to differences in carbohydrate metabolism between males and females (Knopp et al., 2005). Finally, biological factor such as menopause may contribute to higher prevalence of obesity in the females in this study. Although question relating to this was not specifically asked, we believe that many of the female participants were postmenopausal, judging by their mean age.
In this study, the prevalence of obesity increases with age as reported by other workers (Oladapo et al., 2010; Iloh et al., 2012; Ahaneku et al., 2011). However, in a study by Adediran et al. (2012), no association was found between obesity and age (Adediran et al., 2012). Ageing is associated with changes in body composition resulting in increase in fat mass and a decrease in muscle mass (Hughes et al., 2002). The amount of fat significantly increases with age despite stable weight (Prentice and Jebb, 2001). Ageing is associated with osteoporosis and spinal deformity, with consequent decline in height. These changes may lead to false increase in BMI which may range from 1.5 to 2.5 kg/m2 depending on the gender (Sorkin et al., 1999).
Predictors of central obesity
In this study, logistic regression revealed that age, female gender, alcohol and cigarette smoking were predictors of central or abdominal obesity. This study showed that increasing age was associated with greater odds of being obese, a finding that is consistent with a previous study in Nigeria, (Chukwuonye et al., 2013). This is also in keeping with the fact that central obesity increases with age as indicated in this study. Ageing is associated with changes in body composition resulting in increase in fat mass and a decrease in muscle mass (Hughes et al., 2002). While many studies (Oladapo et al., 2010; Adediran et al., 2012; Iloh et al., 2012; Ahaneku et al., 2011; Adienbo et al., 2012; Desalu et al., 2008; Chukwuonye et al., 2013) found that central obesity is more prevalent among women; this study further revealed that as compared to men, the chances of developing central obesity (defined as increased WC) increased by 11-fold among women. Gender differences in physical activity may account for this. As pointed out earlier, the women in the community studied tend to indulge in sedentary lifestyle since many of them either engage in petty trading in the market or are housewives. Furthermore, sociocultural beliefs, nutritional transition and biological factor mentioned earlier may also explain the higher prevalence of obesity among the women as compared to men.
Alcohol consumption increases the risk of central obesity in this study. This is similar to findings by other workers that high alcohol intake is associated with abdominal obesity (Schroder et al., 2007), although an earlier study in Nigeria did not find such association (Chukwuonye et al., 2013). The high energy content of alcohol makes its consumption a potential contributor to the obesity epidemic. Furthermore, both light and heavy drinking have been shown to be associated with increase in food intake (Lloyd-Richardson et al., 2008; Yeomans et al., 2010). These eventually, will lead to weight gain.
This study also showed that tobacco use was associated with increased risk of obesity. As stated earlier, the relationship between smoking and obesity is complex. As compared to non-smokers, smokers have lower weight. Conversely, smoking cessation is associated with weight gain (Williamson et al., 1991). Nevertheless, smoking has been shown to increase the risk of abdominal obesity by previous workers (Visser et al., 1999; Canoy et al., 2005; Saarni et al., 2009). Although smokers have lower mean BMI when compared with non-smokers, they have a more metabolically adverse fat distribution profile, with higher central adiposity. Indeed, a dose-response relation of increasing WHR with increasing number of cigarettes smoked has been observed, independent of BMI (Barrett-Connor and Khaw, 1989).
CONCLUSION
The prevalence of obesity is high in these rural communities. Compared to men, the chances of developing central obesity (defined as increased WC) increased by 11-fold among the women, and this is a source of concern because of the potential CVD in the future. Aggressive education targeted at the women is necessary for the communities to adopt a healthy lifestyle.
LIMITATIONS
The cross-sectional design of this study makes it difficult to establish causal relationship between obesity and its predictors. The volumes of ethanol consumed by the participants were not quantified. Comparing light and heavy drinkers could have yielded different results.
RECOMMENDATIONS
Health education on healthy lifestyle ought to be incorporated into the primary health care system in order to capture the rural communities. The media should be encouraged to participate actively in the dissemination of appropriate information to the community. While both genders are important, emphasis should be placed on women.
CONFLICT OF INTEREST
The authors declare that there are no conflicts of interests regarding the publication of this paper.
ACKNOWLEDGEMENTS
The authors appreciate the assistance of Mrs. Adekanbi, Dr. Adebayo P., Dr. Shobayo F., Dr. Oluwemimo A., Dr. Asumon A., Dr. Okunowo B., Dr. Sokan L., Dr. Vitowanu J., Dr. Onaseso O., Dr. Ilori O. and Dr Samuel A., in data acquisition.
REFERENCES
| Adediran OS, Okpara IC, Adeniyi OS, Jimoh AK (2012). Obesity prevalence and its associated factors in an urban and rural area of Abuja, Nigeria. Glo Adv. Res. J. Med. Med. Sci. 1(8):237-241. | ||||
| Adienbo OM, Hart VO, Oyeyemi WA (2012). High prevalence of obesity among indigenous residents of a Nigerian ethnic group: The Kalabaris in the Niger Delta region of south-south Nigeria. Greener J. Med. Sci. 2:152-156. | ||||
|
Ahaneku GI, Osuji CU, Anisiuba BC, Ikeh VO, Oguejiofor OC, Ahaneku JE (2011). Evaluation of blood pressure and indices of obesity in a typical rural community in eastern Nigeria. Ann. Afr. Med. 10:120-126. Crossref |
||||
|
Bamia C, Trichopoulou A, Lenas D, Trichopoulou D (2004). Tobacco smoking in relation to body fat mass and distribution in a general population sample. Int. J. Obes. Relat. Metab. Disord. 28(8):1091-1096. Crossref |
||||
| Barrett-Connor E, Khaw KT (1989). Cigarette smoking and increased central adiposity. Ann. Intern. Med. 5;111(10):783-787. | ||||
|
Browning LM, Hsieh SD, Ashwell M (2010). A systematic review of waist-to-height ratio as a screening tool for the prediction of cardiovascular disease and diabetes: 0.5 could be a suitable global boundary value. Nutr. Res. Rev. 23(2):247-269. Crossref |
||||
|
Canoy D, Wareham N, Luben R, Welch A, Bingham S, Day N, Khaw KT (2005). Cigarette smoking and fat distribution in 21,828 British men and women: a population-based study. Obes. Res. 13(8):1466-1475. Crossref |
||||
|
Chukwuonye II, Chuku A, Onyeonoro UU, Okpechi IG, Madukwe TI, Ogah OS (2013). Prevalence of abdominal obesity in Abia State, Nigeria: results of a population-based house-to-house survey. Diabetes Metab. Syndr. Obes. 6:285-291 Crossref |
||||
|
Dennis EA, Flack KD, Davy BM (2009). Beverage consumption and adult weight management: A review. Eating Behav. 10(4):237–246. Crossref |
||||
| Desalu OO, Salami AK, Oluboyo PO, Olarinoye JK (2008). Prevalence and socio-demographic determinants of obesity among adults in an urban Nigerain population. Sahel Med. J. 11:61-64. | ||||
|
Goh LGH, Dhaliwal SS, Welborn TA, Lee AH, Della PR (2014). Anthropometric measurements of general and central obesity and the prediction of cardiovascular disease risk in women: a cross-sectional study. BMJ Open 4(2):e004138. Crossref |
||||
|
Hughes VA, Frontera WR, Roubenoff R, Evan WJ, Singh MA (2002). Longitudinal changes in body composition in older men and women: role of body weight change and physical activity. Am. J. Clin. Nutr. 76(2):473-481 Pubmed |
||||
|
Iloh G, Amadi AN, Nwankwo BO, Ugwu VC (2011). Obesity in adult Nigerians: A study of its pattern and common primary co-morbidities in a rural Mission General Hospital in Imo state, south-eastern Nigeria. Niger. J. Clin. Pract. 14:212-218. Crossref |
||||
| International Diabetes Federation (2005). The IDF consensus worldwide definition of the metabolic syndrome. Available at: http://www.idf.org/webdata/docs/MetS_def_update2006.pdf | ||||
|
Jensen EX, Fusch C, Jaeger P, Peheim E, Horber FF (1995). Impact of chronic cigarette smoking on body composition and fuel metabolism. J. Clin. Endocrinol. Metab. 80(7):2181-2185. Crossref |
||||
|
Knopp RH, Paramsothy P, Retzlaff BM, Fish B, Walden C, Dowdy A, Tsunehara C, Aikawa K, Cheung MC (2005) . Gender differences in lipoprotein metabolism and dietary response: basis in hormonal differences and implications for cardiovascular disease. Curr. Atheroscler. Rep. 7(6):472-479. Crossref |
||||
|
Lloyd-Richardson EE, Lucero ML, DiBello JR, Jacobson AE, Wing RR (2008). The relationship between alcohol use, eating habits and weight change in college freshmen. Eating Behav. 9(4):504-508. Crossref |
||||
|
McGarvey ST (1991). Obesity in Samoans and a perspective on its etiology in Polynesians. Am. J. Clin. Nutr. 53(6 Suppl):1586S-1594S. Pubmed |
||||
|
Nguyen T, Lau DC (2012). The obesity epidemic and its impact on hypertension. Can. J. Cardiol. 28:326-333 Crossref |
||||
|
Oladapo OO, Falase AO, Salako L, Sodiq O, Soyinka K, Adedapo K (2010). Prevalence of cardiometabolic risk factore among a rural Yoruba south-western Nigerian population: a population- based survey. Cardiovasc. J. Afr. 21:26-31. Pubmed |
||||
|
Prentice AM, Jebb SA (2001). Beyond body mass index. Obes. Rev. 2(3):141-147. Crossref |
||||
|
Saarni SE, Pietilainen K, Kantonen S, Rissanen A, Kaprio J (2009). Association of Smoking in Adolescence With Abdominal Obesity in Adulthood: A Follow-Up Study of 5 Birth Cohorts of Finnish Twins. Am. J. Public Health 99(2):348–354. Crossref |
||||
|
Schroder H, Morales-Molina JA, Bermejo S, Barral D, Mándoli ES, Grau M, Guxens M, de Jaime Gil E, Alvarez MD, Marrugat J (2007) Relationship of abdominal obesity with alcohol consumption at population scale. Eur. J. Nutr. 46(7):369-376. Crossref |
||||
|
Sorkin JD, Muller DC, Andres R (1999). Longitudinal change in height of men and women: implications for interpretation of the body mass index. The Baltimore Longitudinal Study of Aging. Am. J. Epidemiol. 150:969−977. Crossref |
||||
|
Snodgrass JJ, Leonard WR, Sorensen MV, Tarskaia LA, Alekseev VP, Krivoshapkin V (2006). The emergence of obesity among indigenous Siberians. J. Physiol. Anthropol. 25(1):75-84. Crossref |
||||
|
Ulasi II, Ijoma CK, Onodugo OD (2010). A community-based study of hypetension and cardiometabolic syndrome in semi-urban and rural communities Nigeria. BMC Health Serv. Res. 10:71. Crossref |
||||
|
Visscher TL, Seidell JC, Molarius A, Van der Kuip D, Hofman A, Witteman JC (2001). A comparison of body mass index, waist-hip ratio and waist circumference as predictors of all-cause mortality among the elderly: the Rotterdam study. Int. J. Obes. Relat. Metab. Disord. 25(11):1730-1735. Crossref |
||||
|
Visser M, Launer LJ, Deurenberg P, Deeg DJ (1999). Past and current smoking in relation to body fat distribution in older men and women. J. Gerontol. A Biol. Sci. Med. Sci. 54(6):M293-M298. Crossref |
||||
|
Williamson D, Madans J, Anda R, Kleinman J, Giovino G, Byers T (1991). Smoking cessation and severity of weight gain in a national cohort. N. Engl. J. Med. 324:739-745. Crossref |
||||
| World Health Organization (1995). Technical Report Series-854. Physical Status: The use and interpretation of Anthropometry. WHO Geneva. | ||||
| WHO Non-communicable disease country profiles (WHO, 2008). WHO African Region: Nigeria. Available at: www.who.int/countries/nga/en/ | ||||
| World Health Organization Fact Sheet (WHO, 2014). Obesity and overweight Fact sheet N°311. Available at: www.who.int/mediacentre/factsheets/fs311/en/ | ||||
|
Wager-Srdar SA, Levine AS, Morley JE, Hoidal JR, Niewoehner DE (1984). Effects of cigarette smoke and nicotine on feeding and energy. Physiol. Behav. 32(3):389-395. Crossref |
||||
|
Yeomans MR (2010). Alcohol, appetite and energy balance: Is alcohol intake a risk factor for obesity? Physiol. Behav. 100(1):82-89. Crossref |
||||
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


