Full Length Research Paper

ABSTRACT
Chronic periodontitis is a prevalent condition, affecting nearly half of the adult US population aged 30 years or older. When left untreated, the condition can lead to debilitating tooth loss. While there are well established therapies for all degrees of disease, many are expensive and out of reach to those who lack access to care for medical, socio-economic, or geographic reasons. Scaling and root planing (SC/RP) is the recognized first level of care for periodontally affected teeth, but its overall efficacy is limited to about 1 mm of pocket depth reduction even with the introduction of antibiotic co-therapy. The next level of care requires more invasive surgical approaches and requires practitioners with surgical skills, thus added expense for the patient. The typical open surgical flap approaches will also expose the patient to associated risks and morbidities. To address the need for a minimally invasive approach to periodontal defect treatment with greater potential to reduce pocket depth than SC/RP, a novel nonsurgical approach was developed in a private practice setting. The approach avoids the formation of traditional flaps for access and instead uses adaptations of standard instrumentation for non-incisional debridement of the periodontal pocket lining and preparation of the root surface. This report is a dental chart review, a retrospective analysis of the 3 to 6-month post-treatment outcomes for 221 patients treated by the procedure in this private practice. While the data available was limited to “real world” clinical information available in the patient records, they do provide evidence that this procedure has the potential to address periodontal defects in a meaningful way with a mean pocket depth (PD) reduction of 3.44 ± 1.09 mm and with 75% of the treated sites having a final PD of 4 mm or less.
Key words: Periodontology, therapy, nonsurgical.
INTRODUCTION
Chronic periodontitis is a prevalent condition, affecting 45.9% of the adult US population aged 30 years or older (Eke et al., 2012, 2015). Chronic periodontitis results in the loss of tooth‑supporting connective tissue and alveolar bone and, if untreated, is a major cause of toothloss in adults (Dikbas et al., 2013). According to the Centers for Disease Control and Prevention and the American Academy of Periodontology case definitions, the prevalence of incipient/moderate and severe periodontitis is estimated as 37.1 and 8.9%, respectively, among US adults (Eke et al., 2012, 2015).
Periodontal therapy is often a multi-stage process that increases in invasiveness and cost to the patient as it progresses. Scaling and root planing alone or with adjuncts is understood to be important during initial stage periodontal therapy (Cobb, 2002)but results in a limited average reduction of 1 mm of pocket depth (PD), which is highly dependent on the severity of the periodontal disease (Smiley et al., 2015, 2015a). Additionally, any significant improvement of clinical attachment level (CAL) is limited, even when antimicrobials are added as an adjunct (Garcia Canas et al., 2015; Michalowicz et al., 2013), thus, few non-invasive therapies have been demonstrated to achieve pocket reduction to a greater degree. Next in the spectrum of increasing invasiveness, a range of surgical techniques have been employed to maintain or improve the gingival position as well as achieve pocket reduction. These more invasive techniques are employed to reduce pocket depth plus maintain or improve the gingival esthetics. Many of the surgical techniques, particularly those requiring the development of large areas of flap access, have associated risks and morbidities that cause discomfort for the patient and when they fail can result in esthetic failure and less than the desired gain of CAL (Muller et al., 2001; Tonetti et al., 2004; Zadeh and Daftary, 2004).
While adjuncts to initial therapy have been disappointing (Smiley et al., 2015, 2015a), the effort to reduce the negative sequelae of periodontal reflected flap surgeries has resulted in the development of minimally invasive surgical approaches (Cortellini, 2012; Cortellini and Tonetti, 2009; Harrel, 1998, 1999; Harrel et al., 1999, 2010; Tunnell and Harrel, 2017). The evidence supporting many of these methods is well developed and accepted. The move towards minimally invasive surgical periodontal techniques continues to evolve, driven on one side by patient demands on the practitioner, and on the other by the introduction of new instrumentation, biomaterials, and growth factors (Harrel et al., 2005, 2010; Kaigler et al., 2011). By eliminating the need for large flaps for access to periodontally damaged areas, minimally invasive approaches assist in the post-surgical preservation of gingival form, result in shorter healing times, minimize scarring, and result in less post-operative pain for the patient (Cortellini, 2012; Ribeiro et al., 2011). By preserving tissue, they also appear to ease a practitioner’s task of reconstructing lost bone support and elements of the periodontal attachment apparatus (Harrel, 2018). While many of the established minimally invasive surgical approaches have been shown to be successful in reconstructing damaged tissue, they require a high level of surgical skill, may require expensive magnification devices to perform properly (Cortellini and Tonetti, 2007, 2009; Harrel, 2018; Harrel et al., 2014), and are typically provided only by periodontists. When the use of biologic devices and biological modifiers such as growth factors are introduced, additional improvements in outcomes are possible, but the cost and complexity of treatment are also increased (Agudio et al., 2016; Cortellini and Tonetti, 2007, 2009).
This long case series report describes the use and results of a novel device consisting of a “non-incisional” method and combination of materials to treat periodontal defects. A series of patients were followed through and after the treatment in a private practice office over a five-year period. The approach has been named Periodontal Structural Repair™ (PSR™). The intent of this procedure is to provide a less involved treatment method that has the potential to stabilize periodontal defects and improve anatomical outcomes. The PSR method avoids the formation of traditional flaps for access and instead uses adaptations of standard instrumentation for non-incisional debridement of the periodontal pocket lining and preparation of the root surface. In this approach, an initial therapy step is followed by defect treatment using formulated biomaterial and sealing of the gingival portion of the defect with a surgical cyanoacrylate adhesive. No sutures are required for closure. The PSR technique may serve as a step between scaling and root planing and more involved minimally invasive surgical approaches in its ability to improve PD and reduce tooth mobility while potentially obviating the need for more extensive forms of periodontal surgery.
The purpose of this retrospective chart review case series is to report office-based results of the PSR procedure in terms of the clinical improvement of probing depth and mobility over a widely varying period between treatment and outcome observation. While the clinical records available do not provide the rigorous measurements needed in a clinical trial, they do provide evidence that this procedure has the potential to address periodontal defects in a meaningful way. This “real-world” data has proven useful in the design of the prospective PSR clinical study currently underway – the utility of such data supported by the FDA’s Draft Guidance on the “Use of Real-World Evidence to Support Regulatory Decision-Making for Medical Devices” (Administration, U.S. Food and Drug, 2017). Additionally, this point is supported by the cautions about hard criteria data interpretation in the American Statistical Association statement on p-values (Wasserstein and Lazar, 2016).
MATERIALS AND METHODS
Prior to the start of data collection in this retrospective chart review, Institutional Review Board (IRB) approval for the study plan and a waiver of informed consent was obtained. The IRB for the study was Sterling IRB, 6300 Powers Ferry Road, Suite 600-351, Atlanta, GA 30339.
The charts reviewed were for a series of 221 patients with periodontal defects of varying severity who were treated over an approximate five‑year period from November 2000 to July 2005 and returned later for a general recall visit. Treatment was performed by one practitioner (DWS) and one dental assistant (JY) in a solo private periodontal practice. Nine patients were treated in separate areas of the mouth during a second treatment session. As a result, a total of 231 procedures were performed. The follow‑up times widely varied between treatment and outcome observation; however, the average follow-up time was 168.5 days (median, 77 days). Pre‑ and post‑surgical probing values were made using a Williams periodontal probe at four points around each tooth and immediately recorded in the patient record along with furcation (Grade I, II, III), and tooth mobility (Class 0, 1, 2, 3). All clinical observations and measurements were made by the same practitioner as customary in this solo private practice. No intra-examiner calibration was performed in this practice environment.
Gross debridement was carried out at an appointment prior to the PSR treatment. This initial cleaning was performed using ultrasonic scaling to remove all supragingival calculus in a similar process to that used in a standard dental hygiene tooth cleaning. All calculus deposits were then removed from the subgingival tooth surfaces with an ultrasonic scaler until undetectable visually or with a probe.
At the treatment appointment, commercially available long shank burs (1157R, 1158R, and 56R) were used to plane root surfaces and to remove the inner lining of the pocket epithelium, creating a 1-1.5 mm space. The burs used in the bur planing step were modified in the office to change the bur tips to a rounded shape. Long shank length burs were specifically chosen to maximize access to periodontal pockets in all areas of the oral cavity. In the treatment step that followed, small strips of gauze sponge were placed to aid hemostasis and create a slight distension of the pocket. Warmed PSR compound, a carefully formulated mixture of crystalline hydroxyapatite, fibrillar bovine type I collagen, and medical grade calcium sulfate, was introduced to fill the periodontal defect as the gauze strips were removed, following which the gingival tissue was sealed in the desired position with medical grade cyanoacrylate tissue adhesive to resist displacement of the paste. The bur planing did not require the creation of a gingival flap and as the pocket was sealed with cyanoacrylate tissue sealant, the PSR method eliminated the placement of sutures and the need for suture care.
The patients were then instructed not to brush the cyanoacrylate-sealed areas for two weeks to avoid disrupting the tissue seal and displacing the paste; however, they were told that areas that were not treated with PSR could be cleaned gently.
Statistical methods
The goal of the analysis of the data was to describe the patients in the study and to determine any factors that were related to the success or failure of the procedure. A challenge in the analysis of the data was the number of subjects (221), with a few to these subjects having more than one procedure done at different times resulting in 231 procedures. The question was whether to summarize the results by subject or by the procedure. Due to the structure of the data set and the few subjects with multiple procedures, the analysis was summarized by procedure. ANOVA was used to evaluate effects related to the primary outcome variable, which was change in PD by procedure. For effects related to the procedure, a mean change in PD was the response variable and each procedure was modeled as a random effect, to preserve the procedure as the unit of analysis. If the effect in the model was categorical in nature (site type, tooth type, classification of furcation type, classification of mobility), Tukey’s test was used to adjust for multiple comparisons. Continuous data was summarized by means and standard deviation; categorical data were described by frequency. Note that the PD measured in this case series was measured at four sites per tooth (M, D, B, L) and the areas being treated were sites of pocket depth 5 mm or greater.
RESULTS
Demographics
This is a large case series with 221 patients. Five subjects had the procedure done in two different places in the mouth at different times and one subject had three procedures for a total 231 procedures. There were slightly more female subjects (59%) than males (Table 1). The patients had a mean age of 56 and ranged in age from 30 to 90 years of age (Figure 1). Thus, there was a wide range of ages with representation from both genders.


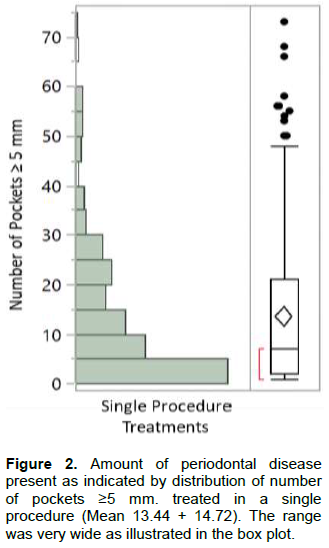
There was detectable periodontal disease in the patients having a mean number of pockets ≥ 5 mm of 13.4, but varied a great deal, ranging from 1 to 70 sites (Figure 2). The mean depth of the pockets ≥ 5 mm per procedure ranged from 5 to 10 mm per procedure with an overall mean of 6.75 ± 1.03 mm for the group (Figure 3). The location of the sites was predominantly at the mesial and distal of teeth (74% of sites) and was relatively evenly distributed among different tooth types (ranging from lower bicuspid 8% of sites to lower second molar 15% of sites) except for third molars where there were fewer treated deep pockets. Most of the sites treated were on the mesial and distal sides of teeth (74% of sites). However, the depth of pockets was greater at the molars. Thus, the periodontal disease varied amongst the subjects in location and severity across the 231 procedures that were performed.

The overall mean effect for the group of procedures was 3.31 ± 1.14 mm and on a procedure level, the mean ranged from -1 to 7 mm (Figure 4). On a procedure level, mean change was not related to the time since the procedure, but there was a strong linear relationship with the initial pocket depth as demonstrated in Figure 5. Thus, the effect was larger for areas that had more severe defects and was not related to the observation period.


The therapeutic effect was evaluated for multiple anatomical features using the ANOVA model. The following effects were evaluated mobility (0, 1, 2) (note that class 3 mobility teeth were an exclusion criteria), furcation involvement (I, II, III), initial pocket depth, site type and tooth type. The largest effect (as noted, the log effect) was the initial pocket depth (Figure 5, Table 2).

The next largest relationship was between change in pocket depth and furcation grade. There was a large reduction in efficacy for grade II furcations (and essentially no therapeutic effect (0.61 mm) for sites with a furcation grade of III (Table 3).

Molars had the smallest change due to therapy (Table 4), but as noted earlier, the initial depth of the pockets was greater. This suggests that the therapy is more effective in non-molar teeth but the procedure is still effective in molar teeth, with the exception of those sites that had grade II or III involvement. In the model, site type, adjusted for the other effects, had a modest effect and mobility had no effect on efficacy of the therapy.

In summary, the patients started out with a mean PD of untreated periodontal disease (all sites equal to or greater than 5 mm) of 6.75 ± 1.03 mm and ended up with a mean of 3.44 ± 1.09 mm with 75% of the treated sites having a final PD of 4 mm or less. Photographs in Figures 6 to 8 show typical results for patients who receive PSR treatment: much improved pocket depths and less bleeding on probing.



DISCUSSION
In this retrospective case series, the therapeutic effect, reduction of PD was greater than has been reported for scaling and root planing alone in the literature (Smiley et al., 2015, 2015a). The PSR device and method appears to be effective at reducing PD of periodontal defects from a pre‑treatment mean of 6.75 mm by a mean of 3.3 mm, returning most patients to a desirable PD of 4 mm or less. In previous systematic reviews (Cobb, 2002; John et al., 2017; Smiley et al., 2015, 2015a), pocket depth reduction from scaling and root planing was reported to average about 1 mm. Thus, PSR appears to have added therapeutic benefit. Two additional effects were noted :
1) A significant reduction in both the number of mobile teeth and the class of mobility occurred by the time of the final post-treatment observation. Due to the limitations of the data set, this report makes no comparison of effect on tooth mobility to historical reports of the effect of other therapies that have been reported in the literature.
2) All grade I furcations were improved to no detectable furcation and 64.7% of grade II furcations were improved, with 47.3% to no detectable furcations and the remainder to grade I. Again, due to the limitations of the data set, this report makes no comparison of the effect of PSR treatment on furcation reduction or closure to historical reports of the effect of other therapies that have been reported in the literature.
Thus, the overall periodontal health of the treated sites showed clinically important improvement. One point that the data made clear is that as with other non-grafting approaches, PSR was not as effective in posterior teeth with deep and/or through and through furcation defects. The limitations in the data set do not permit assessment of the degree of effect the use of PSR has in varying kinds of defect morphology. However, it is possible to say that the technique appears effective when used on defects around single-rooted teeth and multirooted teeth with shallow furcations and the degree of that effect appears to be better than the amount of improvement afforded by scaling and root planing as reported in systematic reviews (Smiley et al., 2015, 2015a). PSR may offer an alternative to traditional nonsurgical therapy to consider prior to resorting to the use of minimally invasive surgical techniques. Most minimally invasive surgical methods require a fairly high level of clinical skill and often, expensive equipment such as clinical microscopes, LASERS and costly biomaterials including growth factors (Burkhardt and Hurzeler, 2000, Burkhardt and Lang, 2014; Cortellini, 2012; Cortellini and Tonetti, 2007, Cortellini et al., 2008, 2009; Miron et al., 2016). By contrast, PSR is a relatively simple technique that uses familiar equipment, common dental skills, and easy to handle materials, making it accessible to more practitioners including general practitioners, and likely more affordable to patients. Pressures on practitioners to use less invasive, less painful methods to address periodontal disease have driven development of minimally invasive methods, that have been shown to be as effective as more extensive surgical techniques with less sequelae and pain (Cortellini, 2012). When applied to the right target defects, PSR may have similar abilities, with a similar promise of minimal pain and discomfort while improving three key prognostic factors for tooth loss: pocket depth, furcation extent, and mobility delivered via a less complex and costly process.
CONCLUSION
This study has shown that long clinical case series are limited but are enticing. Probing depth, mobility, and reduction of furcation involvement were recorded and overall were seen to improve in a clinically meaningful way. Since it is not routine in clinical practice to measure clinical attachment level (CAL), lack of that data limited the observation set. Therefore, the data cannot speak to an improvement in CAL that also might be occurring. The practitioner who performed the procedure was also the examiner as is typical in solo private practice settings. This study is therefore limited by lack of an independent masked or calibrated examiner which potentially could bias the clinical evaluation of the result. Also, unlike a formal clinical trial, there was no comparison group or control group data available from the chart review. Thus, other factors such as improvement of oral hygiene or a placebo effect might have had an additional influence on the result.
The clinical validity of these findings along with additional measures including CAL and gingival indices are currently under investigation in a multicenter, randomized, controlled clinical trial which examines the efficacy of PSR relative to scaling and root planing as the standard of care control.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests. Dr. Spitznagel and Dr. Gunsolley are paid clinical study design and analysis consultants to Periovance, Inc.
REFERENCES
|
Agudio G, Cortellini P, Buti J, Pini Prato G (2016). Periodontal Conditions of Sites Treated With Gingival Augmentation Surgery Compared With Untreated Contralateral Homologous Sites: An 18- to 35-Year Long-Term Study. Journal Periodontology 87(12):1371-1378. |
|
|
Burkhardt R, Hurzeler MB (2000). Utilization of the surgical microscope for advanced plastic periodontal surgery. Practise Periodontics Aesthet Dentisty 12(2):171-80; quiz 182. PMid:11404959 |
|
|
Burkhardt R, Lang NP (2014). Fundamental principles in periodontal plastic surgery and mucosal augmentation - a narrative review. Journal Clinical Periodontology 41(S98-S107. |
|
|
Cobb CM (2002). Clinical significance of non-surgical periodontal therapy: an evidence-based perspective of scaling and root planing. Journal Clinical Periodontology 29 Suppl 2(6-16. PMid:12010523 |
|
|
Cortellini P (2012). Minimally invasive surgical techniques in periodontal regeneration. Journal Evid Based Dentisty Practise 12(3 Suppl):89-100. |
|
|
Cortellini P, Nieri M, Prato GP, Tonetti MS (2008). Single minimally invasive surgical technique with an enamel matrix derivative to treat multiple adjacent intra-bony defects: clinical outcomes and patient morbidity. Journal Clinical Periodontology 35(7):605-13. |
|
|
Cortellini P, Pini-Prato G, Nieri M, Tonetti MS (2009). Minimally invasive surgical technique and enamel matrix derivative in intrabony defects: 2. Factors associated with healing outcomes. International Journal Periodontics Restorative Dentisty 29(3):257-65. PMid:19537465 |
|
|
Cortellini P, Tonetti MS (2007). Minimally invasive surgical technique and enamel matrix derivative in intra-bony defects. I: Clinical outcomes and morbidity. Journal Clinical Periodontology 34(12):1082-1088. |
|
|
Cortellini P, Tonetti MS (2007). A minimally invasive surgical technique with an enamel matrix derivative in the regenerative treatment of intra-bony defects: a novel approach to limit morbidity. Journal Clinical Periodontology 34(1):87-93. |
|
|
Cortellini P, Tonetti MS (2009). Improved wound stability with a modified minimally invasive surgical technique in the regenerative treatment of isolated interdental intrabony defects. Journal Clinical Periodontology 36(2):157-63. |
|
|
Dikbas I, Tanalp J, Tomruk CO, Koksal T (2013). Evaluation of reasons for extraction of crowned teeth: a prospective study at a university clinic. Acta Odontol Scand 71(3-4):848-56. |
|
|
Eke PI, Dye BA, Wei L, Slade GD, Thornton-Evans GO, Borgnakke WS, Taylor GW, Page RC, Beck JD, Genco RJ (2015). Update on Prevalence of Periodontitis in Adults in the United States: NHANES 2009 to 2012. Journal of Periodontology 86(5):611-22. |
|
|
Eke PI, Dye BA, Wei L, Thornton-Evans GO, Genco RJ, Cdc Periodontal Disease Surveillance workgroup: James Beck GDRP (2012). Prevalence of periodontitis in adults in the United States: 2009 and 2010. Journal of Dental Research 91(10):914-20. |
|
|
Garcia Canas P, Khouly I, Sanz J, Loomer PM (2015). Effectiveness of systemic antimicrobial therapy in combination with scaling and root planing in the treatment of periodontitis: a systematic review. Journal American Dentisty Assocation 146(3):150-63. |
|
|
Harrel SK (1998). A minimally invasive surgical approach for periodontal bone grafting. International Journal Periodontics Restorative Dentisty 18(2):161-9. PMid:9663094 |
|
|
Harrel SK (1999). A minimally invasive surgical approach for periodontal regeneration: surgical technique and observations. Journal of Periodontology 70(12):1547-57. |
|
|
Harrel SK (2018). Videoscope-Assisted Minimally Invasive Surgery (VMIS) for Bone Regeneration around Teeth and Implants: A Literature Review and Technique Update. Dentisty Journal (Basel) 6(3): |
|
|
Harrel SK, Abraham CM, Rivera-Hidalgo F, Shulman JD, Nunn ME (2014). Videoscope-assisted minimally invasive periodontal surgery (V-MIS). Journal of Clinical Periodontology 41(9):900-7. |
|
|
Harrel SK, Nunn M, Belling CM (1999). Long-term results of a minimally invasive surgical approach for bone grafting. Journal of Periodontology 70(12):1558-63. |
|
|
Harrel SK, Wilson TG Jr, Nunn ME (2010). Prospective assessment of the use of enamel matrix derivative with minimally invasive surgery: 6-year results. Journal of Periodontology 81(3):435-41. |
|
|
Harrel SK, Wilson TG, Nunn ME (2005). Prospective assessment of the use of enamel matrix proteins with minimally invasive surgery. Journal Periodontology 76(3):380-4. |
|
|
John MT, Michalowicz BS, Kotsakis GA, Chu H (2017). Network meta-analysis of studies included in the Clinical Practice Guideline on the nonsurgical treatment of chronic periodontitis. Journal Clinical Periodontology 44(6):603-611. |
|
|
Kaigler D, Avila G, Wisner-Lynch L, Nevins ML, Nevins M, Rasperini G, Lynch SE, Giannobile WV (2011). Platelet-derived growth factor applications in periodontal and peri-implant bone regeneration. Expert Opinion on Biological Therapy 11(3):375-85. |
|
|
Michalowicz BS, Hodges JS, Pihlstrom BL (2013). Is change in probing depth a reliable predictor of change in clinical attachment loss? Journal American Dentisty Assocation 144(2):171-8. PMid:23372133 |
|
|
Miron RJ, Sculean A, Cochran DL, Froum S, Zucchelli G, Nemcovsky C, Donos N, Lyngstadaas SP, Deschner J, Dard M, Stavropoulos A, Zhang Y, Trombelli L, Kasaj A, Shirakata Y, Cortellini P, Tonetti M, Rasperini G, Jepsen S, Bosshardt DD, (2016). Twenty years of enamel matrix derivative: the past, the present and the future. Journal Clinical Periodontology 43(8):668-83. |
|
|
Muller HP, Stahl M, Eger T (2001). Failure of root coverage of shallow gingival recessions employing GTR and a bioresorbable membrane. International Journal of Periodontics and Restorative Dentistry 21(2):171-81. PMid:11829391. |
|
|
Ribeiro FV, Casarin RC, Palma MA, Junior FH, Sallum EA, Casati MZ (2011). Clinical and patient-centered outcomes after minimally invasive non-surgical or surgical approaches for the treatment of intrabony defects: a randomized clinical trial. Journal Periodontology 82(9):1256-66. |
|
|
Smiley CJ, Tracy S L, Abt E, Michalowicz BS, John MT, Gunsolley J, Cobb CM, Rossmann J, Harrel SK, Forrest JL, Hujoel PP, Noraian KW, Greenwell H, Frantsve-Hawley J, Estrich C, Hanson N (2015). Evidence-based clinical practice guideline on the nonsurgical treatment of chronic periodontitis by means of scaling and root planing with or without adjuncts. Journal American Dentisty Assocation 146(7):525-35. |
|
|
Smiley CJ, Tracy SL, Abt E, Michalowicz BS, John MT, Gunsolley J, Cobb CM, Rossmann J, Harrel SK, Forrest JL, Hujoel PP, Noraian KW, Greenwell H, Frantsve-Hawley J, Estrich C, Hanson N (2015a). Systematic review and meta-analysis on the nonsurgical treatment of chronic periodontitis by means of scaling and root planing with or without adjuncts. Journal American Dentisty Assocation 146(7):508-24 e5. |
|
|
Tonetti MS, Fourmousis I, Suvan J, Cortellini P, Bragger U, Lang NP, European Research Group on P (2004). Healing, post-operative morbidity and patient perception of outcomes following regenerative therapy of deep intrabony defects. Journal Clinical Periodontology 31(12):1092-8. |
|
|
Tunnell JC, Harrel SK (2017). Minimally Invasive Surgery in Periodontal Regeneration: A Review of the Literature. Compend Continuous Education Dentisty 38(4):e13-e16. PMid:28368128 |
|
|
Wasserstein RL, Lazar NA (2016). The ASA Statement on p-Values: Context, Process, and Purpose. The American Statistician 70(2):129-133. |
|
|
Zadeh HH, Daftary F (2004). Minimally invasive surgery: an alternative approach for periodontal and implant reconstruction. The Journal of the California Dental Association 32(12):1022-30. PMid:15715379. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


