Full Length Research Paper

ABSTRACT
The study aimed to characterize the influence of Mansonella perstans co-infection on immunity. This research was carried out in November, 2021 in the neighboring villages of Saint Camille de Davougon in the Abomey Commune. Blood samples were collected from both genders of all ages. Buruli ulcer was diagnosed by polymerase chain reaction (PCR), using specific IS2404 repeat sequence for Mycobacterium ulcerans. Microfilaria detection was done with the help of the counting chamber technique. Using 100 white blood cells, the proportion of eosinophils was determined. Minividas® Biomerieux was used to quantify the IgE titers in the patients' serum using an immuno-enzymatic sandwich enzyme linked immunosorbent assay (ELISA). This study shows an overall co-infection of Buruli ulcers with M. perstans as 23.86%. In the age group of fewer than 16 years, the co-infection prevalence was 28.57% (n=6), while in patients of age greater than 16, the co-infection prevalence was 71.42% (n=15). The Buruli ulcer patients co-infected with M. perstans had the highest median eosinophil level, whereas the control group had the lowest. The lowest median total IgE titer was observed in the control, while the maximum was observed in the Buruli ulcer patients co-infected with M. perstans. This study concludes that Buruli ulcer co-infection with M. perstans prevails in some rural villages in Benin. Therefore, this pathogen must be considered in the treatment of Buruli ulcer. The findings imply that IgE could be used to assess the patient's immunological response during Buruli ulcer and M. perstans.
Key words: Mansonella perstans, co-infection, immunity, Buruli ulcer.
INTRODUCTION
Buruli ulcer is a tropical illness caused by Mycobacterium ulcerans that is frequent in rural areas of West Africa. M. ulcerans disease causes disfiguring skin ulcers, most common in children. The disease is relatively localized, with cases reported in Ghana’s humid and tropical southern regions, including Ashanti and Greater Accra (Wansbrough-Jones and Phillips, 2006). Although actual transmission paths for M. ulcerans remain unknown, recent research shows that marine species act as reservoirs for this parasite (Salomao et al., 2017). Aquatic insects infected with M. ulcerans can infect mice by biting (Ray and Maunsell, 2011), but it is unclear if this is the source of infectious disease in humans (Benbow et al., 2008). Information relating infected mosquitoes to cases reported in humans has been discovered in southern Australia (Lavender et al., 2011), but transmission assurance is inadequate. A previous study reported that Buruli ulcer is endemic in Benin (Williamson et al., 2012). Inhabitants in Buruli ulcer-endemic areas are regularly exposed to parasitic illnesses like Filariasis. Lymphatic Filariasis induced by Wuchereria bancrofti worms has been discovered in Ghana in numerous areas where Buruli ulcer is endemic, including the Upper Denkyira district in the central region (Hoerauf et al., 2008). Mansonella perstans, a filarial nematode indigenous to Central and Western Africa, has a range that overlaps with that of other filarial nematodes. Infection caused by M. perstans is not related to a definite set of clinical signs and symptoms, although those connected with it comprised acute swelling (forearms, hands, and face) that subsides in a few days but often returns; itchiness both with and without rash, arthralgia, and eosinophilia are all symptoms (Simonsen et al., 2011).
M. perstans is prevalent in 33 African countries, with an estimated 100 million people infected (Simonsen et al., 2011). M. perstans, which was previously thought to be incapable of causing infection, is now suspected of causing severe clinical signs, particularly allergic reactions. This illness can also cause hypereosinophilia (Bregani et al., 2006).
Despite the fact that the pathophysiology of helminth infections is unknown, the immune system is the primary cause of signs and symptoms. Filariasis patients' IgG4 and IgE patterns are considered immune response indicators. Antigen-specific IgE expression has also been linked to allergic responses and parasite clearance related to total IgE production (Blackwell et al., 2011). IgE levels are higher during infection of loiasis than IgG4 levels, and they have been proven to diminish after treatment (Mitre and Nutman, 2006). Furthermore, a correlation was discovered between elevated IgE titers and patent infection, parasitemia, and medical manifestation (Arndts et al., 2012).
Moreover, it has been proposed that throughout Mansonella infection, immune-regulatory responses are altered (Simonsen et al., 2012). Clarifying the symptomatic and immunological implications of dual infection would help researchers better comprehend the underlying problem. Examining the range of IgE levels during single or co-infection might help explain this issue and determine the use of IgE levels in detecting individuals with multiple infections and evaluating post-treatment techniques to cure chronic infections. The purpose of this study was to examine how substantial an immune response, such as IgE titers, was during Buruli ulcer and M. perstans infections in Benin, whether they were single or co-infections.
MATERIALS AND METHODS
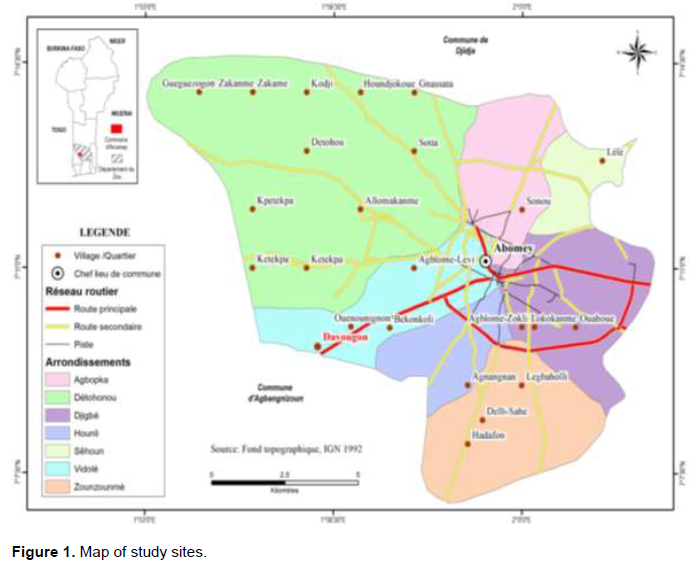
The sampling was carried out from two weeks of November 2021 in the neighboring villages of Saint Camille de Davougon in the Abomey Commune (Figure 1). In previous studies, this area was observed to be endemic for Buruli ulcers. Blood samples were collected from all the patients admitted to the hospital for health checkups. All age patients of both genders were included in the study. The research and ethical committee (Ref: IRB00006860) approved the research study before collecting samples. The research goal was thoroughly discussed in numerous meetings with local health officials and members of the study population. In a pre-designed Performa, age, sex, name, and other characteristics were recorded. To participate in the study, all patients over the age of 12 signed an informed consent form, while younger patients required parental approval. In this study, a total of 120 blood samples were collected. Buruli ulcer was diagnosed by polymerase chain reaction, using specific IS2404 repeat sequence for M. ulcerans as described in the previous study (Hoerauf etb al., 2008). The research included both test and control groups. The control groups were made up of single infected individuals as opposed to co-infected individuals, which described the test group.
Microfilaria detection was done with the help of the counting chamber technique. In heparinized capillary tubes, 100 ml blood samples were taken from all the patients included in the study. Later in the laboratory, the blood samples were examined under the microscope at 100× magnifications in a counting chamber (Sedgewick Rafter). The microfilariae were allowed to settle for 1 h before being examined and counted. Macgregor's solution was employed to repair the M. perstans microfilaria, as it is generally done.
The thick blood film was prepared, dried, de-hemoglobinized, ethanol-fixed, and stained with Giemsa stain. After that, the slides were examined under a microscope. Eosinophils were counted after blood was spread out on Giemsa-stained slides. The eosinophil fraction was calculated using 100 white blood cells. Hyper-eosinophilia was defined as an eosinophil count of more than 10% of WBC. The Minividas® Biomerieux was used to quantify the IgE titers in the patients' serum using an immuno-enzymatic sandwich ELISA. All the data was entered in SPSS version 23. For comparing different results, Fisher's exact test was applied. A P-value of less than 0.05 was considered statistically significant.
RESULTS
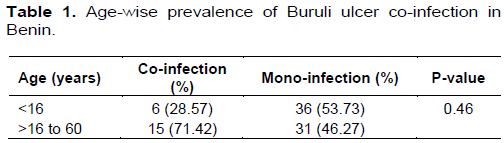
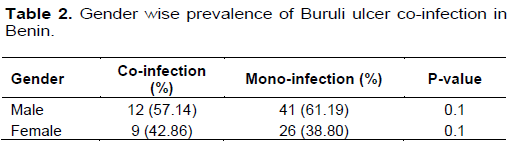
In this study, 120 patients attending the hospital were included. There were 90 (75%) females and 30 (25%) males in the study. Out of 120 suspected patients, Buruli ulcer was confirmed in 88 patients by PCR. This shows a prevalence of 73.33% of Buruli ulcers in Benin. Out of 88 Buruli ulcer-positive patients, 32 were control group, 53 (60.22%) were male, and 35 (39.77%) were female. Microscopically by counting chamber technique, M. perstans was observed in 21 samples of patients positive for Buruli ulcer while 67 samples were negative for M. perstans. This shows an overall co-infection of 23.86%. Out of 21 co-infected patients, 12 (57.14%) were male and 9 (42.86%) were female. The gender-wise prevalence was statistically non-significant (p=0.1) (Table 1). In the age group of fewer than 16 years, the co-infection prevalence was 28.57% (n=6), while in patients of age greater than 16, the co-infection prevalence was 71.42% (n=15). This age-wise prevalence was not significant as the p-value was 0.46 (Table 2). The patients with Buruli ulcers who were also infected with M. perstans had the highest median eosinophil level, while the control group had the lowest. Everyone in the co-infected and single infection groups had a high eosinophil level, but no one in the control group did. This comparison was statistically significant (p=0.01). The lowest median total IgE titer was 141 (55-231) KUI/L in control, while the maximum was 6225 (4111-17,513) KUI/L in the Buruli ulcer patients co-infected with M. perstans. In comparison to single-infected individuals, co-infected individuals showed greater IgE levels. The single infected Buruli ulcer patients and the control group had similar titers. The single infection titer of M. perstans was 3241 (1216-7022) KUI/L. This comparison was also significant statistically (p=0.01) (Table 3).

DISCUSSION
Buruli ulcer and M. perstans infections are two conditions that can occur together. M. perstans filariasis is prevalent mainly in rural areas, and infection typically starts in childhood; the most significant infection rates are reported in children aged 10 to 14 years (Asio et al., 2009), which are comparable to those seen in children who are at risk for M. ulcerans infection. M. perstans infection is found in Ghana and was first discovered in the Volta area near Hohoe in the 1990s, but its occurrence is unclear (Awadzi et al., 1991), and no data on the average value of worms per infection is known. The frequency of M. perstans infection in Uganda has been estimated to be between 0.4 and 50% (Onapa et al., 2005). The bites of Culicoides midges transfer M. perstans nematodes, but it is unclear if M. perstans-infected midges may also carry M. ulcerans. Skin penetration was necessary for the formation of M. ulcerans illness in a guinea pig experiment (Marsollier et al., 2007).
Microscopically by counting chamber technique, M. perstans was observed in patients positive for Buruli ulcer while some negative for M. perstans. This shows an overall co-infection of 23.86%. The gender-wise prevalence was statistically non-significant (p=0.1). In the age group of fewer than 16 years, the co-infection prevalence was 28.57%, while in patients of age greater than 16 the co-infection prevalence was 71.42%. This age-wise prevalence was not significant. Similar results were observed in a previous study that reported Buruli ulcer co-infection with M. perstans (Phillips et al., 2014). The majority of infected individuals reside in rural locations where molecular methods and ELISA are not available. Specific immunological indicators will aid in identifying dual-infected individuals, at most by associating the existence of clinical symptoms with the presence of microfilaria, mainly when parasitic numbers are below the detection limit for microscopic examination. The Buruli ulcer patients co-infected with M. perstans had the highest median eosinophil level, whereas the control group had the lowest. No one in the control group had a high eosinophil level, while everyone in the co-infected and single infection groups did. This comparison was significant statistically.
In comparison with single-infected individuals, co-infected individuals showed greater IgE levels. The single infected Buruli ulcer patients and the control group had similar titers. This comparison was also significant statistically (p=0.01). A previous study reported that total IgE levels in infected individuals were higher than in the control group (Arndts et al., 2012). Compared to patients with a single infection, co-infected individuals had higher IgE titers. This discrepancy shows that during co-infection, there is a significant hyper-responsiveness. The reduced microfilaraemia in M. perstans patients explains the lower IgE titers detected in M. perstans patients than others. IgG4 levels are elevated in both situations, with a low IgG4/IgE ratio since IgG4 balances out higher IgE concentrations (Arndts et al., 2012). Mansonella infection has been hypothesized to influence infected individuals' regulatory responses, potentially interfering with the outcomes of other endemic illnesses like HIV and malaria in regions where they co-exist. In a malaria-endemic environment, the two filarial may be linked to anaemia (Dolo et al., 2012). The lack of antigen-specific IgE testing was a crucial flaw in this study. However, the correlations identified between total IgE titers and Filariasis are robust and statistically significant (Blackwell et al., 2011).
CONCLUSION
The study concludes that Buruli ulcer can have co-infection with M. perstans prevalent in Benin. Therefore, this pathogen must be considered during the treatment of Buruli ulcers. The findings suggest that eosinophil and IgE titer increased in the case of co-infection as compared to the single infection and thus IgE and eosinophil count might be used to measure the patient's immunological response during Buruli ulcer and M. perstans. Chronic filarial infections can cause immunological modulation and affect the host's response to intracellular pathogens. Initiatives must be undertaken to discover low-cost sensitive approaches to help identify and classify infected individuals and assess treatment efficacy and elucidate immunological relationships between numerous filarial infections and other diseases.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Arndts K, Deininger S, Specht S, Klarmann U, Mand S, Adjobimey T, Alexander Y, Debrah AY, Batsa L, Kwarteng A, Epp C, Taylor M (2012). Elevated adaptive immune responses are associated with latent infections of Wuchereria bancrofti. PLoS Neglected Tropical Diseases 6(4):e1611. |
|
|
Asio SM, Simonsen PE, Onapa AW (2009). Mansonella perstans Filariasis in Uganda: patterns of microfilaraemia and clinical manifestations in two endemic communities. Transactions of the Royal Society of Tropical Medicine and Hygiene 103(3):266-273. |
|
|
Awadzi K, Hero M, Opoku O, Büttner D, Gilles H (1991). The chemotherapy of onchocerciasis. XV. Studies with albendazole. Tropical Medicine and Parasitology 42(4):356-360. |
|
|
Benbow M, Williamson H, Kimbirauskus R, McIntosh M, Kolar R, Quaye C, Small PLC, Boakye D, Merritt RW (2008). A large-scale field study on aquatic invertebrates associated with Buruli ulcer disease: are biting water bugs likely vectors. Emerging Infectious Diseases 5(4):e 10675. |
|
|
Blackwell AD, Gurven MD, Sugiyama LS, Madimenos FC, Liebert MA, Martin MA, Kaplan HS, Snodgrass JJ (2011). Evidence for a peak shift in a humoral response to helminths: age profiles of IgE in the Shuar of Ecuador, the Tsimane of Bolivia, and the US NHANES. PLoS Neglected Tropical Diseases 5(6):e1218 |
|
|
Bregani ER, Rovellini A, Mbaidoum N, Magnini MG (2006). Comparison of different anthelminthic drug regimens against Mansonella perstans Filariasis. Transactions of the Royal Society of Tropical Medicine and Hygiene 100(5):458-463. |
|
|
Dolo H, Coulibaly YI, Dembele B, Konate S, Coulibaly SY, Doumbia SS, Diallo AA, Soumaoro L, Coulibaly ME, Diakite SA, Guindo A (2012) Filariasis attenuates anemia and proinflammatory responses associated with clinical malaria: a matched prospective study in children and young adults. PLoS Neglected Tropical Diseases 6(11):e1890. |
|
|
Hoerauf A, Specht S, Büttner M, Pfarr K, Mand S, Fimmers R, Marfo-Debrekyei Y, Konadu P, Debrah AY, Bandi C, Brattig N (2008). Wolbachia endobacteria depletion by doxycycline as antifilarial therapy has macrofilaricidal activity in onchocerciasis: a randomized placebo-controlled study. Medical microbiology immunology 197(3):295-311. |
|
|
Lavender CJ, Fyfe JA, Azuolas J, Brown K, Evans RN, Ray LR, Johnson PD (2011). Risk of Buruli ulcer and detection of Mycobacterium ulcerans in mosquitoes in southeastern Australia. PLoS Neglected Tropical Diseases 5(9):e1305. |
|
|
Marsollier L, Aubry J, Milon G, Brodin P (2007) Punaises aquatiques et transmission de Mycobacterium ulcerans. médecine/sciences 23(6-7):572-575 |
|
|
Mitre E, Nutman TB (2006). IgE memory: persistence of antigen-specific IgE responses years after treatment of human filarial infections. Journal of Allergy Clinical Immunology 117(4):939-945. |
|
|
Onapa A, Simonsen P, Baehr I, Pedersen E (2005). Rapid assessment of the geographical distribution of Mansonella perstans infections in Uganda, by screening schoolchildren for microfilariae. Annals of Tropical Medicine and Parasitology 99(4):383-393. |
|
|
Phillips RO, Frimpong M, Sarfo FS, Kretschmer B, Beissner M, Debrah A, Ampem-Amoako Y, Abass KM, Thompson W, Duah MS, Abotsi J (2014). Infection with Mansonella perstans nematodes in Buruli ulcer patients, Ghana. Emerging Infectious Diseases 20(6):1000. |
|
|
Ray S, Maunsell JH (2011). Different origins of gamma rhythm and high-gamma activity in macaque visual cortex. PLoS Biology 9(4):e1000610. |
|
|
Salomao C, Nacima A, Cuamba L, Gujral L, Amiel O, Baltazar C, Cliff J, Gudo ES (2017). Epidemiology, clinical features and risk factors for human rabies and animal bites during an outbreak of rabies in Maputo and Matola cities, Mozambique, 2014: Implications for public health interventions for rabies control. PLoS Neglected Tropical Diseases 11(7):e0005787. |
|
|
Simonsen PE, Onapa AW, Asio SM (2011) Mansonella perstans filariasis in Africa. Acta Troprica 120:S109-S120. |
|
|
Wansbrough-Jones M, Phillips R (2006). Buruli ulcer: emerging from obscurity. The Lancet 367(9525):1849-1858. |
|
|
Williamson HR, Benbow ME, Campbell LP, Johnson CR, Sopoh G, Barogui Y, Merritt RW, Small PL (2012). Detection of Mycobacterium ulcerans in the environment predicts prevalence of Buruli ulcer in Benin. PLoS Neglected Tropical Diseases 6(1):e1506. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


