Full Length Research Paper
ABSTRACT
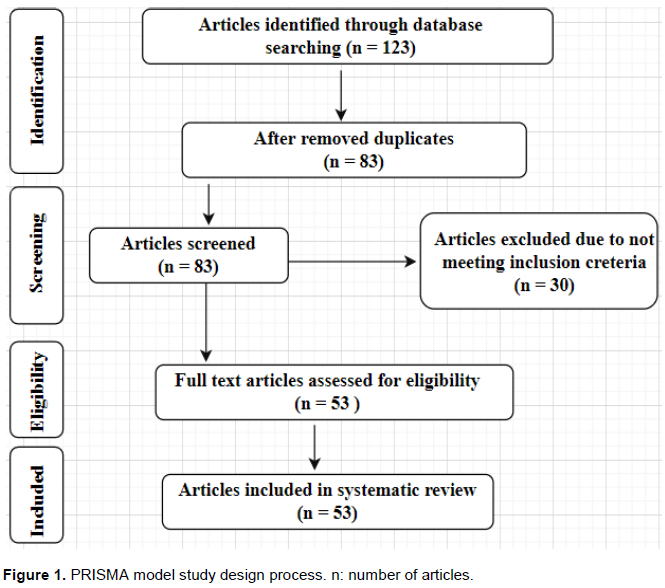
Cholera is an epidemic disease and a real public health problem throughout the world, particularly in West Africa. This study provides a comprehensive overview of the pathogenicity, epidemiology and Vibrio cholerae strains’s antibiotics resistance in West Africa. A literature review was conducted online in English using the keywords “Cholera”, “Vibrio cholerae” “West Africa”, “Epidemiology”, “Antibiotic resistance”. These keywords were entered into using electronic databases such as PubMed, Google Scholar, Scopus and Elsevier and articles were used according to the reliability of their sources, study areas, and subjects. This review was based on the collected data from different databases. One hundred and twenty-three articles were identified. After the initial and final sorting of the collected data in order to eliminate duplicate copies, eighty-three were retained while seventy articles were selected, respectively, for this review. Though some studies had recommended for a system of monitoring cholera in West African countries, nevertheless, there is the need to create more awareness. Furthermore, hygienic practices and environmental wastes management in these countries need to be improved.
Key words: Cholera, epidemiology, Vibrio cholerae, antibiotic resistance, West Africa.
INTRODUCTION
METHODOLOGY
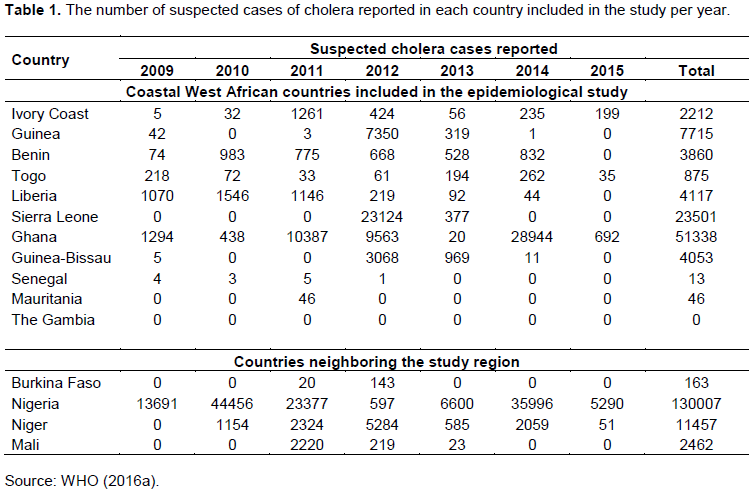
RESULTS

DISCUSSION
CONCLUSION
CONFLICT OF INTERESTS
REFERENCES
|
Abana D, Gyamfi E, Dogbe M, Opoku G, Opare D, Boateng G and Mosi L (2019). Investigating the virulence genes and antibiotic susceptibility patterns of Vibrio cholerae O1 in environmental and clinical isolates in Accra, Ghana. BMC Infectious Diseases 19(76). |
|
|
Adewale AK, Pazhani GP, Abiodun IB, Afolabi O, Kolawole OD, Mukhopadhyay AK, Ramamurthy T (2016). Unique Clones of Vibrio cholerae O1 El Tor with Haitian Type ctxB Allele Implicated in the Recent Cholera Epidemics from Nigeria, Africa. PLoS ONE 11(8):e0159794. |
|
|
Aidara A, Koblavi S, Boye CS, Raphenon G, Gassama A, Grimont F, Grimont PA (1998). Phenotypic and genotypic characterization of Vibrio cholerae isolates from a recent cholera outbreak in Senegal: comparison with isolates from Guinea-Bissau. The American Journal of Tropical Medicine and Hygiene 58(2):163-167. |
|
|
Ali M, Lopez AL, Ae You Y, Eun Kim Y, Sah B, Maskery B, Clemens J (2012). The global burden of cholera. Bulletin of the World Health Organization 90(3):209-218. |
|
|
Amedome A, Kpodzro H, Nabede N, Vovor VM (1971). Initial 40 cases of bacteriologically confirmed cholera treated at the National Hospital Center of Lomé (Togo). Bulletin de la Société Médicale d'Afrique Noire de Langue Française 16(2):219-23. |
|
|
Banerjee R, Das B, Nair BG, Basak S (2014). Dynamics in genome evolution of Vibrio cholerae. Infection, Genetics and Evolution 23:32-41. |
|
|
Bockemühl J, Meinicke D (1976). Value of phage typing of Vibrio cholerae biotype eltor in West Africa. Bulletin of the World Health Organization 54(2):187-92. |
|
|
Bockemühl J, Schröter G (1975). The El Tor cholera epidemic in Togo (West Africa) 1970-1972. Tropenmedizin Parasitologie 26(3):312-22. |
|
|
Boeckmann M, Roux T, Robinson M, Areal A, Durusu D, Wernecke B, Chersich MF (2019). Climate Change and Heat-Health Stu M F. Climate change and control of diarrhoeal diseases in South Africa: Priorities for action. South African Medical Journal 109(6):359-361. |
|
|
Cholera Annual Report (2011). Weekly Epidemiological Record, Volume 87. WHO Press, Geneva: World Health Organisation, pp. 289-304. |
|
|
Constantin de Magny G, Guegan JF, Petit M, Cazelles B (2007). Regional-scale climate variability synchrony of cholera epidemics in West Africa. BMC Infectious Diseases 7(20):1-9. |
|
|
Dalhat MM, Isa AN, Nguku P, Nasir SG, Urban K, Abdulaziz M, Dankoli RS, Nsubuga P, Poggensee G (2014). Descriptive characterization of the 2010 cholera outbreak in Nigeria. BMC Public Health 14(1):1167. |
|
|
Dalsgaard A, Forslund A, Petersen A, Brown DJ, Dias F, Monteiro S, Molbak K, Aaby P, Rodrigues A, Sandström A (2000). Class 1 Integron-borne, multiple antibiotic resistance encoded by a 150-kilobase conjugative plasmid in epidemic Vibrio cholerae O1 strains isolated in Guinea-Bissau. Journal of Clinical Microbiology 38(10):3774-3777. |
|
|
Dalsgaard D, Mortensen HF, Mølbak K, Dias F, Serichantalergs O, Echeverria P (1996). Molecular Characterization of Vibrio cholerae O1 Strains Isolated during Cholera Outbreaks in Guinea-Bissau. Journal of Clinical Microbiology 34(5):1189-1192. |
|
|
Danso EK, Asare P, Otchere ID, Akyeh LM, Asante-Poku A, Aboagye SY, Osei-Wusu S, Opare D, Ntoumi F, Zumla A, Duodu S, Yeboah-Manu D (2020). A molecular and epidemiological study of Vibrio cholerae isolates from cholera outbreaks in southern Ghana. PLOS ONE 15(7):e0236016. |
|
|
Echenberg M (2011). Africa in the Time of Cholera: A History of Pandemics from 1817 to the Present (Vol. 114). Cambridge University Press. Cambridge, UK. |
|
|
Ekra KD, Attoh-Toure H, Benie BV, Coulibaly D, Koutouan MG, Aka LN, Dagnan SN, Coulibaly A, Douba A, Tiembré I, Odéhouri-Koudou P, Tagliante-Saracino J (2009). Five years of cholera surveillance in Ivory Coast during social and political crisis, 2001 to 2005 [Article in French]. Bulletin de la Société de Pathologie Exotique 102(2):107-109. |
|
|
Gbary AR, Dossou JP, Sossou RA, Mongbo V, Massougbodji A (2011). Epidemiologic and medico-clinical aspects of the cholera outbreak in the Littoral department of Benin in 2008 [in French]. Médecine Tropicale 71(2):157-61. |
|
|
Ghana Health Service/Ministry of Health (2013). Report: End of 2012 cholera outbreak in Ghana.Ghana weekly epidemiological bulletin [Internet] (2015) [cited 2018/11/2]. View |
|
|
Gidado S, Awosanya E, Haladu S, Ayanleke HB, Idris S, Mamuda I, Mohammed A, Michael CA, Waziri NE, Nguku P (2018). Cholera outbreak in a naïve rural community in Northern Nigeria: the importance of hand washing with soap, September 2010. The Pan African Medical Journal 30:5. |
|
|
Goita A (2014). Waterborne pathogenic bacteria from epidemiology to prevention. Bibliographical study. Thesis for the doctoral degree in Pharmacy. University Mohamed V- Souissi. Faculty of Medicine and Pharmacy. |
|
|
Landoh DE, Gessner BD, Badziklou K, Tamekloe T, Ibrahim ND, Dagnra A, Abiba BK (2013). National surveillance data on the epidemiology of cholera in Togo. The Journal of Infectious Diseases 208(1):115-119. |
|
|
Luquero FJ, Banga CN, Remartínez D, Palma PP, Baron E, Grais RF (2011). Cholera Epidemic in Guinea-Bissau (2008): The Importance of Place. PLoS ONE 6(5):e19005. |
|
|
Manga NM, Ndour CT, Diop SA, Dia NM, Ka-Sall R, Diop BM, Sow AI, Sow PS (2018). Cholera in Senegal from 2004 to 2006: lessons learned from successive outbreaks. Journal of Medicine in the Tropics 68(6):589-592. |
|
|
Marin MA, Thompson CC, Freitas FS, Fonseca EL, Aboderin AO, Zailani SB, Quartey NKE, Okeke IN, Vicente ACP (2013). Cholera Outbreaks in Nigeria Are Associated with Multidrug Resistant Atypical El Tor and Non-O1/Non-O139 Vibrio cholerae. PLOS Neglected Tropical Diseases 7(2):e2049. |
|
|
Mengel MA, Delrieu I, Heyerdahl L, Gessner BD (2014). Cholera Outbreaks in Africa. Current Topics of Microbiology and Immunology 379:117-44. |
|
|
Moore S, Dongdem AZ, Opare D, Cottavoz P, Fookes M, Sadji AY, Piarroux R (2018). Dynamics of cholera epidemics from Benin to Mauritania. PLOS Neglected Tropical Diseases 12(4):e0006379. |
|
|
Munita JM, Arias CA (2016). Mechanisms of Antibiotic Resistance. Microbiology Spectrum 4(2). |
|
|
Okeke IN, Abudu AB, Lamikanra A (2001). Microbiological investigation of an outbreak of acute gastroenteritis in Niger State, Nigeria. Clinical Microbiology and Infection 7(9):514-516. |
|
|
Opajobi SO, Kandakai-Olukemi YT, Mawak JD, Olukemi MA, Bello CSS (2004). Vibrio cholerae O1 infections in Jos, Nigeria. African Journal of Clinical and Experimental Microbiology 5(3):260-264. |
|
|
Quilici ML, Denis M, Bouba G, Barem B, David MO (2010). Vibrio cholerae O1 variant with reduced susceptibility to ciprofloxacin, Western Africa. Emerging Infectious Diseases 16(11):1804-1805. |
|
|
Ramamurthy T, Mutreja A, Weill FX, Das B, Ghosh A, Nair GB (2019). Revisiting the global epidemiology of cholera in conjunction with Vibrio cholerae genomics. Frontiers in Public Health 7:237. |
|
|
Rebaudet BS, Sudre B, Faucher R, Piarroux J (2013). Cholera Outbreaks in Nigeria Are Associated with Multidrug Resistant Atypical El Tor and Non-O1/NonO139 Vibrio cholerae. Infectious Diseases 208(1):S46-S54. |
|
|
Rebaudet S, Mengel MA, Koivogui L, Moore S, Ankur Mutreja, Kande Y, Yattara O, Keita VS, Njanpop-Lafourcade BM, Fournier PE, Garnotel E, Keita S, Piarroux R (2014). Deciphering the Origin of the 2012 Cholera Epidemic in Guinea by Integrating Epidemiological and Molecular Analyses. PLoS Neglected Tropical Diseases 8(6):e2898. |
|
|
Roquet D, Diallo A, Kodio B, Daff BM, Fenech C, Etard JF (1998). The senegalese cholera epidemic of 1995 to 1996, an example of the geographic approach to health studies [Article in French]'. Sante 8(6):421-428. |
|
|
Ruenchit P, Reamtong O, Siripanichgon K, Chaicumpa W, Diraphat P (2019). New facet of non-O1/non-O139 Vibrio cholerae hemolysin A: a competitive factor in the ecological niche. FEMS Microbiology Ecology 94(1). |
|
|
Safa A, Nair GB, Kong RY (2010). Evolution of new variants of Vibrio cholerae O1. Trends Microbiology 18(1):46-54. |
|
|
Sambe-Ba B, Diallo MH, Seck A, Wane AA, Constantin de Magny G, Boye CSB, Sow AI, Gassama-Sow A (2017). Identification of Atypical El Tor V. cholerae O1 Ogawa Hosting SXT Element in Senegal, Africa. Frontiers in Microbiology 8:748. |
|
|
Somayyeh H, Amir YN, Atefeh MF (2018). Colonization and Investigation of Vibrio Cholera Recombination Protein in E-coli. International Journal of Engineering and Technology 7(4.7):32-35. |
|
|
Sule IB, Yahaya M, Aisha AA, Zainab AD, Ummulkhulthum B, Nguku P (2017). Descriptive epidemiology of a cholera outbreak in Kaduna State, Northwest Nigeria, 2014. Pan African Medical Journal 27. |
|
|
UNICEF (2011). UNICEF responds to cholera epidemic in Ivory Coast. |
|
|
UNICEF (2016). UNICEF Ghana-water, sanitation and hygiene-WASH in communities. |
|
|
Webb Jr JLA (2019) "Disease and Epidemiology of Humans and Animals: Methods." In Oxford Research Encyclopedia of African History. |
|
|
Weill FX, Domman D, Njamkepo E, Tarr C, Rauzier J, Fawal, Karen H, Keddy HS, Moore S, Mukhopadhyay AK, Bercion R, Luquero FJ, Ngandjio A, Dosso M, Monakhova E, Garin B, Bouchier C, Pazzani C, Mutreja A, Grunow R, Sidikou F, Bonte L, Breurec S, Damian M, Njanpop-Lafourcade BM, Sapriel G, Page AL, Hamze M, Henkens M, Chowdhury G, Mengel M, Koeck JL, Fournier JM, Dougan G, Grimont PAD, Parkhill J, Holt KE, Piarroux R, Ramamurthy T, Quilici M-L, Thomson NR (2017). Genomic history of the seventh pandemic of cholera in Africa. Science 358(6364):785-789. |
|
|
World Health Organization (WHO) (2016b). Weekly epidemiological record. cholera articles. WHO-Cholera (2016). |
|
|
World Health Organization (WHO) (1987). Cholera in 1986. The Weekly Epidemiological Record 62:141-142. |
|
|
World Health Organization (WHO) (2010). Global Task Force on Cholera Control. In Weekly Epidemiological Record: Cholera Articles. |
|
|
World Health Organization (WHO) (2013). Weekly epidemiological record 88(31):321-36. Available from: View. Accessed 18 Feb 2016. |
|
|
World Health Organization (WHO) (2014). Cholera-Fact Sheet. P 107. |
|
|
World Health Organization (WHO) (2016a). Antimicrobial resistance. Fact Sheet 194 (World Health Organization, World Health Organization, WHO, 2016. Cheers, Ed.). Geneva (Switzerland). |
|
|
World Health Organization (WHO) (2019). [cited 2019/11/02]. Cholera Facts Sheet [Internet]. View. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


