Full Length Research Paper

ABSTRACT
Melaleuca oil has great medicinal properties. The objective is to develop a product based on Melaleuca armillaris to evaluate its antihistaminic action and to compare the antihistaminic effect and protective effect of M. armillaris oil and ointment. Pruritus intensity was assessed at sensitization points. Eighty volunteers, aged between 21 and 60 years (male and female) participated in the study, without contraindications to the Prick test. The left forearm was sensitized at four points: A: control (+) histamine, B: control (-) M. armillaris oil, C: histamine and after 2 min, drying and application of M. armillaris. D: M. armillaris and after 2 min the application of histamine. The right forearm was sensitized at four points. A: control (+) histamine; B: control (-) M. armillaris ointment. C: histamine and after 2 min, drying and application of M. armillaris. D: M. armillaris ointment and after 2 min, drying and application of histamine. Reading was taken after 15 min. Areas obtained were scanned and analyzed by Image J. The pruritus was evaluated through the Visual Analogue Scale. There were differences in the left and right forearm between the points A: control (+) and C: effect of post-chopped oil and post-chopped effect of ointment rearmillarisectively. The oil of M. armillaris, 100% and the ointment of M. armillaris, 50% presented antihistaminic action and did not influence the intensity of pruritus. There was no protective effect of the oil and ointment of M. armillaris.
Key words: Histamine antagonists, phytotherapy, Melaleuca, bites, stings.
INTRODUCTION
Reactions due to insects of the order Diptera are due to allergens in insect saliva and not due to toxin. Saliva contains active compounds that inhibit the body's immune responses causing coagulation, platelet formation, vasodilation and anti-inflammatory activities to be impaired (Singh and Mann, 2013).
Generally occurring in children 2 to 10 years old, papular urticaria occasionally affects adolescents and adults. Sensitization takes time, so it is not seen in newborns. The higher prevalence in children may result from immune mechanisms and / or behaviors that predispose them to contact with insects. Most children overcome the disease probably due to desensitization by repeated exposures. There are no racial or gender predilections (Singh and Mann, 2013). Insect bite reactions are common, but information on their prevalence is limited. Children under 14 at the Dermatology Outpatient Clinic in Pondicherry had a prevalence of papular urticaria of 5.3%. Children under 5 years old attending clinic in Calcutta had a prevalence of 10.6% papular urticaria, with seasonal variation (rainy season 16.7%, summer 6.7%, winter 5.8%) (Singh and Mann, 2013). Phytotherapy is the area of study that evaluates the drug action of active ingredients from plants used in the treatment and prevention of diseases. Phyton, in Greek, means plant and therapeia comes from the verb therapeuo, which means to treat, to take care of. According to Portaria 971, dated 05/05/2006, of the Ministry of Health, Phytotherapy is a therapy characterized by the use of medicinal plants in their different pharmaceutical forms, without the use of isolated active substances, although of vegetal origin (Panizza, 2016).
The genus Melaleuca belongs to the family Myrtaceae (Oliveira et al., 2011). It usually presents simple, coriaceous, acute-lanceolate leaves and, sometimes, in scythe format, 1 - 2.5 cm length, with oil glands (Monteiro et al., 2013). This genus is formed by several species standing out the Melaleuca alternifolia (Vieira et al., 2004). It is known as tea tree (Oliveira et al., 2011). The trees can reach seven meters in height, have thin bark and long pointed leaves that, when broken, emit a strong aroma. They can be cut after 15 months of cultivation and cropped each year (Simões et al., 2002).
Native to Australia and Indian Ocean Islands. Flowering mainly in marsh areas, near rivers (Oliveira et al., 2011). M. alternifolia belongs to the group of species of Melaleuca armillaris Sm. (Which also includes Melaleuca dissitiflora F. Muell, Melaleuca linophylla F. Muell., Melaleuca trichostachya Lindl), of wide distribution and occurrence in several climates. Terpinenol-4 chemotypes occur in species of the group. Species grown in Brazil (Monteiro et al., 2013). The oil of the tree is colorless or pale yellow in color and has a spicy earthy odor (Fahlbusch et al., 2003). Terpinenol-4 is mainly responsible for its medicinal properties, mainly antifungal and antibacterial (Garcia et al., 2009).
Chemically terpenes can be divided into two major groups: terpene derivatives (menthol and citronellol) and phenylpropane derivatives (anethole and eugenol). The main pharmacological characteristics of terpenes are related to the use as antiseptic, anti-inflammatory and antipyretic agents (Lima et al., 2005). The main product of the Melaleuca plant is TTO tea tree oil, of great medicinal importance because it has a proven bactericidal and antifungal action against several human pathogens, being used in topical formulations (Oliveira et al., 2011).
Among their great properties, they emphasize their bactericidal, healing, expectorant, fungicidal, anti-infective, balsamic, anti-inflammatory, antiseptic, antiviral, febrifuge, insecticide, immunostimulant, diaphoretic and parasiticide actions (Maluf, 2009). However, this oil has interesting therapeutic characteristics against certain pathologies, such as antiacne action, onychomycosis, dermatitis, eczema, toothache, bad breath, among others
(Garcia et al., 2009). It can also be incorporated into formulations such as the intima liquid soaps, where it seeks the prevention of diseases of the female genito-urinary tract, as against candidiasis (Garcia et al., 2009). Melaleuca oil has wide applicability in products such as disinfectants, capillary products, oral and personal hygiene, deodorants, burns, insect bites, post-sun, veterinary products, aromatherapy and flavoring (Souza, 2009).
Topical use of Melaleuca oil is considered safe for most adults. It is commonly indicated for skin infections, cuts and abrasions, boils, recurrent cold sores, infections of the mouth and nose, sore throat and ear infections such as otitis media and otitis externa, cough additive, bronchial congestion and the pulmonary inflammation (Oliveira et al., 2011). There are no reports of health hazards if given in an appropriate therapeutic manner. However, contact dermatitis may occur. In pediatric use, the oil can not be applied around the nose of infants and children, because of the risk of glottal edema (Monteiro et al., 2013). In view of the need for further studies and research on the medicinal importance and applicability of M. armillaris. The objective of this study was to evaluate the antihistaminic effectiveness of this oil in order to provide an adequate treatment for allergic reactions and subsequent development of a new pharmaceutical formulation.
MATERIALS AND METHODS
Clinical, analytical, observational, transversal and controlled study. The research was carried out in the city of Pouso Alegre, MG, at the Universidade do Vale do Sapucaí, Fátima Unit, from June to September 2016. The study population consisted of eighty volunteers of both sexes who agreed to participate in the study and signed the Free and Informed Consent Term (FICT). Inclusion criteria: individuals who signed the FICT, aged between 18 and 60 years old and who did not present contraindications to the Prick Test (history of previous anaphylaxis, extensive dermatitis using antihistamine) (Mendonça et al., 2014).
Exclusion criteria: Individuals who have had a negative reaction to histamine or who withdraw their consent at any stage of the study.
Oil of M. armillaris
Melaleuca oil was obtained from leaves taken from M. armillaris, using a hydrodistillation extracted methods. The leaves were dried at room temperature in a rustic solar dryer with clear plastic cover for six days. 150 g of dried leaves was transferred to a volumetric flask with 400 ml of distilled water. The flask was then fitted to the condenser and connected to the refrigeration system. The heating mantle was switched on and set at the boiling temperature of the water at 100°C until it reached boiling and then reduced to 75°C in admixture with the biomass, initiating the extraction process for a period of 50 min.
When the mixture of water and leaves (biomass) was boiled, the water vapors and volatiles were conducted towards the condenser, where the heat exchange was carried out, condensing the vapors with the cooling water. At this stage, this mixture of oil and hydrolyzate (by-product) was cooled and returned to the liquid phase. The mixture reached the last stage of the process, separating the oil from the hydrolate by means of the polarity and density differences of these substances through the separating funnel. To determine the yield of the essential oil, the empty 1000 ml flask (320 g) was weighed in analytical balance and the flask was then charged with the sheets (470 g). At each extraction of 150 g of M.armillaris, 6.5 ml of oil was extracted. The oil was then transferred to an amber glass vial and stored in a cool place without the direct incidence of light.
Preparation of M. armillaris ointment.
The semi-solid pharmaceutical form was made according to Table 1.
Procedures for data collection
The Prick Test is the safest and easiest to perform, has good reproducibility and is considered the best for use in clinical allergy practice (Motta et al., 2005). The skin test is very important for the verification of IgE-mediated hypersensitivity reactions, which are attributed to mediators, including histamine. For this reason, the method chosen, based on this test, was used in humans to compare the antihistaminic effect of M. armillaris and the oil of M. armillaris incorporated in ointment. Each individual was their own control (paired sample). And the place for the test used the ventral midface (volar) of the forearms of the participants. Antisepsis of the skin was carried out with cotton soaked in 70% alcohol. The region to be applied the test could not present any type of tissue injury. After cleaning, the points (A, B, C and D) were marked with a watermark on the left and right forearms. In the left forearm the antihistaminic action of the oil was evaluated and in the right forearm the antihistaminic action of the Melaleuca ointment. Each point had a distance of approximately 2 cm in a predetermined sequence:
i) Point A (positive control) application of histamine at the concentration of 10 mg / ml acquired from the Laboratory Alergolatina. In order to simulate an allergic reaction to the insect bite.
ii) Point B (negative control) had the objective of verifying that the oil of M. armillaris. (left forearm) and ointment (right forearm) would have an irritating effect on the skin.
iii) Point C simulated the antihistaminic effect of M. armillaris (left forearm) and the ointment (right forearm) after the insect sting. The oil of M. armillaris. and ointment were applied 2 min after histamine application.
iv) Point D simulated the protective antihistaminic effect of M. armillaris (left forearm) and ointment (right forearm) for the insect bite. The oil of M. armillaris and the ointment were applied 2 min before histamine application.
The left forearm was sensitized at four points (A, B, C and D). Point A: Positive control (+) sensitized with a drop of histamine, causing redness, papule (swelling) and pruritus, point B: negative control
(-) sensitized with only one drop of M. armillaris. Point C was sensitized with one drop of histamine and after 2 minutes, drying of the histamine with paper napkin and application of one drop of the oil of M. armillaris. Point D was sensitized with one drop of the M. armillaris oil and after 2 minutes the application of one drop of histamine.
The right forearm was sensitized at four points (A, B, C and D). Point A: Positive (+) control sensitized with a drop of histamine, which may cause redness, papules (swelling) and pruritus; point B: negative control (-) sensitized only with the ointment of M. armillaris. Point C was sensitized with a drop of histamine and after 2 minutes, drying with paper napkin and application of the ointment of M. armillaris. The D spot was sensitized with M. armillaris ointment and after 2 min, paper napkin drying and application of a drop of histamine. The application of M. armillaris and histamine were performed with the bead dropper from each vial. And the ointment of M. armillaris was applied with wooden spatula.
A puncture (plastic device that limited the degree of skin penetration) was used and allowed the penetration of histamine through the skin of the participant for each point. The reading was performed after 15 min after puncture. The papules obtained were delimited with a fine-tipped dermographic pen and covered by transparent adhesive tape, forming a mold of the areas. These areas were scanned and analyzed by the Image J program which is a scientific image processor available in a virtual environment. The pruritus was evaluated through the Visual Analogue Scale to measure the degree of intensity at each point on the forearms of the participants. The Visual Analogue Scale consisted of a 10 cm line, marked the numbers from 0 to 10. And the participants reported their note for pruritus. From 0 to 3 it was considered mild pruritus, between 4 and 8 moderate pruritus and between 9 and 10 severe pruritus (Welter et al., 2008).
Ethical aspects
Before starting any procedure, the present study was submitted to the Research Ethics Committee of the Universidade do Vale do Sapucaí and approved on 12/16/15. Under the Supported Opinion: 1,372,740, CAAE: 50703515.1.0000.5102. Performed in accordance with the precepts established by Resolution 466/12 of 12/12/12 of the Ministry of Health in Brazil.
Data analysis
The obtained data were arranged in tables of Microsoft Office Excel 2007 and analyzed quantitatively. The program used for Statistical Analysis was PASW Statistics 18. Descriptive procedures for quantitative variables through measures of central tendency (mean and median) and by measures of dispersion (standard deviation). Qualitative variables were described by proportions. Inferential analysis was conducted for parametric continuous variables by paired T tests (for two samples). For the non-parametric variables Wilcoxon and Friedman tests were used. The level of significance was set at 5% (p <0.05).
RESULTS
Characterization of the sample
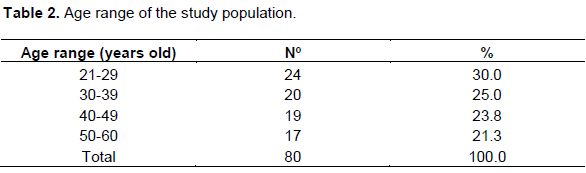
Of the eighty participants, six had a negative reaction to histamine (positive control) at point A of the right forearm and were excluded from the sample. Thus the sample for the left forearm was n: 80 and for the right forearm n: 74. Regarding gender, 49 were females and 31 were males. Age was divided into age groups in four subgroups: 21-29 years, 30-39 years, 40-49 years and 50-60 years, with a predominance of young adults (Table 2).
Comparison of application and effect of oil and ointment of M. armillaris
In Table 3 it is possible verify the averages of the areas of the papules in cm² formed at the points of application on the left and right forearms.
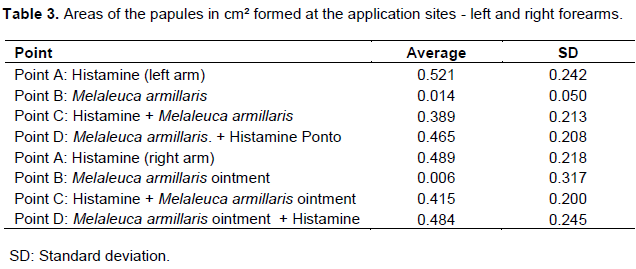
Standard deviation
It was observed in points B: negative controls that the oil of M. armillaris and the ointment of M. armillaris did not cause any irritating effect on the skin. At points A and C (left forearm) there was a difference between the positive control: histamine and the effect of post-chopped oil (p: 0.000), demonstrating the antihistaminic effect of M. armillaris and suggesting its post-pricking insect use. At points A and D (left forearm) there was no difference between the positive control: histamine and the protective antihistaminic effect of oil (p: 0.057). At points A and C (right forearm) there was a difference between the positive control: histamine and the post-pricked effect of the ointment (p: 0.003), proving the antihistaminic effect of M. armillaris and suggesting its post-pricking insect use. At points A and D (right arm) there was no significant difference between the positive control: histamine and the protective antihistamine effect of the ointment (p: 0.887). At points C and D (right arm), the post-pricked and protective effect of the ointment was compared (p: 0.017) and there was a significant difference evidencing the antihistaminic effect of M. armillaris post-chopped. Comparing point C (left arm) and point C (right arm), it was verified that there was no difference in the post-chopped effect between oil and ointment (p: 0.496). Comparing D (left arm) and D (right arm), there was no difference in the protective effect between oil and ointment (p: 0.497).
Measurement of pruritus degree
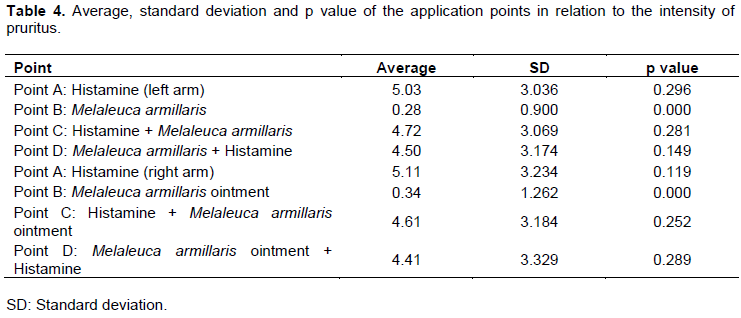
The results in relation to the intensity of pruritus (Table 4) showed that the majority of participants reported moderate itching in the application of oil and ointment of M. armillaris. There were no differences between the points of the left and right forearms. It was also verified in points B: negative controls that the oil of M. armillaris and the ointment of M. armillaris did not cause itching on the skin.
DISCUSSION
In the present study there were differences between the A points (positive control: histamine) and the C points that simulated the post-prickly antihistamine effect of the insect of M.armillaris to 100% (left forearm) and M. armillaris to 50% (right forearm). The C points showed a decrease in the size of the papule area formed in relation to point A. The antihistaminic effect of the oil and ointment of M. armillaris and their post-pricking insect use was suggested.
Comparisons were also made between the C-points that simulated the post-chopped antihistamine effect and the D-points that simulated the protective effect of M. armillaris to 100% (left forearm) and M. armillaris to 50% (right forearm) and there were differences. The antihistaminic effect of the oil and ointment of M. armillaris post-chopped. The effect of topically applied tea tree oil (TTO) reduced histamine-induced edema in the ears of mice. Topical application of TTO, and in particular terpinenol-4, may be effective in controlling the histamine-induced edema frequently associated with Type I immediate hypersensitivity allergic reactions (Brand et al., 2002).
Topical application of 100% TTO may have therapeutic benefit in nickel-induced contact hypersensitivity on human skin. The mode of action of TTO requires additional investigation (Pearce et al., 2005). When applied 20 min after histamine injection into the skin of the human forearm, tea tree oil (TTO) reduces the developing cutaneous vascular response (Khalil et al., 2004). It was verified in points B: negative controls that the oil of M. armillaris to 100% and M. armillaris to 50% did not cause any irritation after topical use. The topical use of Melaleuca oil is relatively safe and adverse effects are minor and occasional (Hammer et al., 2006). Both 100% M. armillaris oil and 50% M. armillaris ointment cause any pruritus on the skin through evaluation. It is fundamental to attenuate or eliminate pruritus, since it is the act of scratching one of the factors, not only of increasing the duration of the lesions but also the one responsible for possible secondary infections and residual hyperpigmentation. Anti-histamines (cetirizine, ebastine) have been shown to be associated with a 50% reduction in the maculae caused by the immediate reaction after mosquito bites and a 70% decrease in pruritus accompanying the bites. The use of emollients / moisturizers with additional pruritic and healing action may also be useful in some patients (Moreira et al., 2014).
In an experimental study on contact dermatitis and urticaria, the efficacy of traditional topical therapeutic agents and tea tree oil was compared. The effects of 10% ictamol, 20% zinc oxide, 20% camphor, 10% levomenthol, 20 or 50% tea tree oil and 0.05% clobetasone were studied in the following experimental models: nickel allergic contact dermatitis, irritative contact dermatitis of benzalkonium chloride, and in immediate reactions to histamine and benzoic acid), respectively. Tea tree oil reduced allergic contact dermatitis by 40.5%, zinc oxide by 17.4% and clobetasone by 23.5%. Zinc oxide reduced histamine-induced enlargement by 18.5%, ictamol by 19.2% and clobetasone by 44.1%. The histamine-induced pruritus was assessed using Visual Analog Scale and also remained unchanged. In this study, the author states that tea tree oil appears to be a more effective anti-eczematous agent than zinc oxide and clobetasone in the topical treatment of urticaria reactions (Wallengren, 2011).
Popular knowledge has brought great contribution to the dissemination of the use of plants in the treatment of diseases. In recent decades, there has been an increase in interest in alternative medicines, mostly from natural extracts, triggering the search for validation of the use of these drugs, given the favorable therapeutic effects in vitro and in vivo (Oliveira et al., 2011). Preparations based on Melaleuca essential oil obtained by steam distillation of foliage are indicated for the treatment of small surface wounds and insect bites. Semi-solid dosage forms are suitable for cutaneous use (European Medicines Agency, 2013).
In addition to being vectors of infectious diseases, insects can be a cause of discomfort for their bites. Some species of mosquitoes may cause local irritation, pruritus, secondary infection, cellulitis, pain and sleep disturbances (Stefani et al., 2009). One of the reactions to insect bites is the pruritus that occurs in the region of the papules. When immunological sensitization to these bites occurs a more extensive picture called estropole (papular urticaria) (Rodrigues et al., 2010).
Although the exact prevalence of papular urticaria is unknown, it is a frequent dermatosis (estimated if it occurs in about 10% of the population) and is characteristic of children, appearing mainly from 2 years of age, with spontaneous disappearance, in most cases, up to 7 10 years. However, it can also affect adolescents and adults and can cause considerable impact on the quality of life of affected patients. Its diagnosis implies a high clinical suspicion and it is carried out based on the clinical history and identification of the characteristic cutaneous lesions. Regarding its treatment, this is mainly based on symptomatic relief, control of hypersensitivity reaction and measures of eradication and prophylaxis of bites by causative agents. In this context, antihistamines play a determining role, as the main drugs to be used (Moreira et al., 2014). The aim of this study is to study the medicinal plant M. armillaris and evaluating the antihistaminic effect of M. armillaris oil and compare it with M. armillaris ointment and thus to develop a herbal medicine for the treatment of patients suffering from allergies to insect bites.
In view of the limitations encountered during the manipulation in the incorporation of M. armillaris and obtaining the stability of the pharmaceutical form. Taking into account children with hypersensitivity to insect bites and information from the European Medicines Agency (EMA), 2013 that the use of oil in children under 12 years of age has not been established due to lack of adequate data. The future prospects of in-depth studies on the absorption, toxicity of this active principle and pharmaceutical technology aimed at obtaining a stable and appropriate formulation for pediatric topical use are highlighted.
CONCLUSION
The oil of M. armillaris, 100% and M. armillaris ointment, 50% presented antihistaminic action and did not influence the severity of pruritus. There was no protective effect of the oil and ointment of M. armillaris.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Brand C, Townley SL, Finlay-Jones JJ, Hart HP (2002). Tea tree oil reduces histamine-induced o edema in mirine ears. Inflammation Research 51(6):283-289. |
|
|
European Medicines Agency (2013). Committee on herbal medicinal products. Community herbal monograph on Melaleuca alternifolia (Maiden and Betch). Cheel, M. armillaris Smith, M. dissitiflora F. Mueller and/or other species of Melaleuca, aetheroleum. |
|
|
Fahlbusch KG, Hammerschmidt FJ, Panten J, Picknhagen W, Schatkowski D, Bauer K, Garbe D, Surburg H (2003). Flabors and fragrances. Ullmann's Encyclopedia of Industrial Chemistry. |
|
|
Garcia CC, Germano C, Osti NM, Chorilli M (2009). Desenvolvimento e avaliação da estabilidade físico-química de formulações de sabonete líquido íntimo acrescidas de óleo de Melaleuca. Revista Brasileira de Farmácia 90(3):236-240. |
|
|
Hammer KA, Carson CF, Riley TV, Nielsen JB (2006). A review of the toxicity of Melaleuca alternifolia (tea tree) oil. Food and Chemical Toxicology 44(5):616-625. |
|
|
Khalil Z, Pearce AL, Satkunanathan N, Storer E, Finlay-Jones JJ, Hart PH (2004). Regulation of wheal and flare by tea tree oil: complementary human and rodent studies. Journal of Investigative Dermatology 123(4):683-690. |
|
|
Lima JF Jr, Vieira LB, Leite MJVF, Lima KC (2005). O uso de fitoterápicos e a saúde bucal. Rev Saúde em Revista 16:11-17. |
|
|
Maluf S (2009). Aromaterapia uma abordagem sistêmica. São Paulo: do autor. |
|
|
Mendonça ARA, Paschoal GRM, Barbosa S, Santos WJ (2014). Efeito anti-histamínico do óleo de Melaleuca (Melaleuca alternifolia) em testes imunológicos em humanos. Trabalho de conclusão de curso. Pouso Alegre: Universidade do Vale do Sapucaí, Curso de Ciências Biológicas. |
|
|
Monteiro MHDA, Macedo HW, Silva AJr, Paumgartten FJR (2013). Óleos essenciais terapêuticos obtidos de espécies de Melaleuca L.(Myrtaceae Juss.). Revista Fitos 8(1). |
|
|
Moreira A, Rosmaninho I, Silva JPM (2014). Urticária papular: Revisão da literatura. Revista Portuguesa de Imunoalergologia 22(4):279-287. |
|
|
Motta AA, Kalil J, Barros MT (2005). Testes cutâneos. Brazilian Journal of Allergy and Immunology 28(2):73-83. |
|
|
Oliveira ACM, Fontana A, Negrini TC, Nogueira, MNM, Bedran TBL, Andrade CR, Spolidorio LC, Spolidorio DMP (2011). Emprego do óleo de Melaleuca alternifolia Cheel (Myrtaceae) na odontologia: perspectivas quanto à utilização como antimicrobiano alternativo às doenças infecciosas de origem bucal. Revista Brasileira de Plantas Medicinais,pp. 492-499. |
|
|
Panizza ST (2016). Fitoterapia e terapias complementares: plantas medicinais e fitoterápicos. |
|
|
Pearce G, Finlay-Jones JJ, Hart HP (2005). Reduction of nickel-induced contact hypersensitivity reactions by topical tea tree oil in humans. Inflammation Research 54(1):22-30. |
|
|
Rodrigues DA, Tomimori J, Floriano MC, Mendonça S (2010). Atlas de dermatologia em povos indígenas. SciELO-Editora Fap-Unifesp. |
|
|
Simões RP, Groppo FC, Sartorato A, Del Fiol FS, Mattos Filho TR, Ramacciato JC, Rodrigues MVN (2002). Efeito do óleo de Melaleuca alternifolia sobre a infecção estafilocócica. Lecta-USF 20(2):143-152. |
|
|
Singh S, Mann BK (2013). Insect bite reactions. Indian Journal of Dermatology, Venereology and Leprology 79(2):151. |
|
|
Souza VM (2009). Ativos dermatológicos, volumes 1 a 4: guia de ativos dermatológicos utilizados na farmácia de manipulação para médicos e farmacêuticos. São Paulo: Pharmabooks Editora, pp. 402-403. |
|
|
Stefani GP, Pastorino AC, Castro APBM, Fomin ABF, Jacob CMA (2009). Repelentes de insetos: recomendações para uso em crianças. Revista Paulista de Pediatria 27(1):81-89. |
|
|
Vieira TR, Barbosa LCA, Maltha CRA, Paula VF, Nascimento EA (2004). Constituintes químicos de Melaleuca alternifolia (Myrtaceae). Química Nova 27(4):536-539. |
|
|
Wallengren J (2011). Tea tree oil attenuates experimental contact dermatitis. Archives of Dermatological Research 303(5):333-338. |
|
|
Welter EQ, Bonfá R, Petry W, Moreira LL, Weber MB (2008). Relação entre grau de prurido e qualidade de vida de pacientes em hemodiálise Relationship between pruritus and quality of life in patients on hemodialysis. Brazilian Annals of Dermatology 83(2):137-40 |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


