Full Length Research Paper

ABSTRACT
The use of plants for medicine has constituted an important aspect of primary healthcare delivery system of people throughout the world for many centuries. Nonetheless, information on medicinal plants and their conservation are still lacking in some areas, including the Togo Plateau Forest Reserve in Ghana. This paper investigates the ethnobotany of the Togo Plateau Forest Reserve, Ghana, to document the traditional knowledge, uses and conservation of medicinal plants. Information on these plants was sought through a structured questionnaire administered to 384 registered members of the Ghana Federation of Traditional Medicine Practitioners’ Association including certified traditional healers, traditional birth attendants (TBAs), vendors of herbal remedies, managers of herbal medicine centers, and local plant collectors from six communities within the catchment area of the Togo Plateau Forest Reserve. The study recorded 114 medicinal plant species, including 14 herbs, 6 lianas, 21 shrubs and 74 trees that are mostly collected from the wild. The most commonly cited medicinal plant species were Azadirachta indica, Alstonia boonei, Morinda lucidaand Nauclea latifolia, mostly used to treat human conditions such as malaria, jaundice, rheumatism, andcough. Mostof the herbal medicines were prepared as decoctions and administered by drinking. Majority of the informants (75%) were within the age bracket of 41-60 years, with males (39%) out numbering the females (36%). Barks, roots and leaves were the most commonly used plant parts, and these were mostly collected by destructive methods. The unregulated collection of plant parts and harvesting methods may reduce plant species richness and abundance in the area, requiring sustained conservation efforts in order to benefit from them medicinally.
Key words: Medicinal plants, Togo Plateau forest reserve, plant diversity.
INTRODUCTION
The use of plants for medicine has constituted animportant aspect of primary healthcare delivery system of people throughout the world for many centuries (Agbovie et al., 2002; Jeruto et al., 2008; WHO, 2015).
Currently, over 80% of the world’s human populations rely on medicinal plants for their daily fight for better health (WHO, 2015). In Africa, in particular, medicinal plants are extensively (ca. 90%) used due to limited access to modern medical treatment, either resulting from lack of facilities or unavailability of hospital services (Satpong, 2000; Fyhrquist, 2007; Jeruto et al., 2008; Koduru et al., 2007). Studies show that about 46% of Ghanaians, for example, live in rural communities and depend largely on locally available plant resources for their health care needs (Fyhrquist, 2007).
The high demand for and dependence on traditional medicine (TM) for health care delivery in developing countries have resulted in the proliferation of traditional medicine dealers. According to the Ghana Federation of Traditional Medicine Practitioners Association (GHAFTRAM), there are more than 100,000 TM practitioners in Ghana of which 45,000 are registered. These practitioners are uniformly distributed throughout Ghana, resulting in approximately one TM practitioner for every 400 people, compared to one allopathic doctor for every 12000 people (WHO, 2015).
Several studies have documented the wide spectrum of application of medicinal plants among people (Abbiw, 1990; Addo-Fordjour et al., 2013; Jeyaprakash et al., 2011). Medicinal plants are commonly used to treat human conditions such asmalaria, jaundice, migraine, cough, rheumatism and gastrointestinal pain, among others (Addo-Fordjour et al., 2013; Jeyaprakash et al., 2011). These human conditions are treated using diverse plant parts ranging from whole plant, roots, leaves and bark, with the latter being the most commonly used in herbal medicine preparation in Ghana (Addo-Fordjour et al., 2013; Asase et al., 2005; Ziblim et al., 2013) and elsewhere (Kakudidi, 2000; Kala, 2005; Kamatenesi-Mugisha et al., 2008).
Ecologists and conservationists have established that the harvesting methods often used for medicinal plants are critical to their survival (Balemie et al., 2004; Megersa et al., 2013). Destructive methods such as harvesting of the whole plant and roots, coupled with steady decline in customary laws that regulate the commercial collection of medicinal plant resources from the wild, are reportedly to cause the depletion of medicinal plant diversity as well as the indigenous knowledge associated with their conservation and use (Jeruto et al., 2008; Kamatenesi-Mugisha et al., 2008; Schippmann, 2001).
In this light, non-destructive methods of plant harvesting including consideration of the frequency, time, and season of harvesting which could affect natural regeneration (Abbiw 1990) are increasingly being encouraged. Researchers have also recommended harvesting of fruits and other aerial parts instead of the root, stem or the whole plant which could cause defoliation, debarking, root destruction and wounds (Abbiw, 1990; Jeruto, 2008). Extracting plant leaves also provides a more sustainable use strategy through rapid replacement by re-growt (Dold and Cocks, 2002).
Available records showed that intensive gathering of plants from the wild for medicinal purposes poses serious threat to Ghana’s biodiversity (Addo-Fordjour et al., 2013; Asase et al., 2005; Bussmann et al., 2011; Megersa et al., 2013; Ziblim et al., 2013) as it increases the risk of local extinction of plant species in general (Ita and Offiong, 2013) and the scarcity of commonly used medicinal plants in particular (Bussmann et al., 2011; Kamatenesi-Mugisha and Bukenya-Ziraba, 2002; Megersa et al., 2013). Consequently, increasing commitment toward efficient controls and better conservation practices can help preserve medicinal plant diversity in Ghana.
The Togo Plateau Forest Reserve, covering a total land area of 14.763 hectares is the largest forest reserve in the Volta Region of Ghana. This reserve has been recognized as a biodiversity significant area due to its wide topographic range and high elevation (Abbiw, 1990; Agbovie et al., 2002) and thus provides a variety of medicinal plants to the surrounding communities.This has resulted in a high demand for and dependence on TM by the people for their healthcare needs leading to a proliferation of practitioners in the area, whose activities could pose a threat to the medicinal plants biodiversity on the plateau. Moreover, given the diverse plant species reportedly used for medicinal purposes in the area, targeting them for conservation can positively impact biodiversity conservation in the reserve generally. There is, therefore, an urgent need for information on medicinal plant usage and conservation practices by communities fringing the Togo Plateau Forest Reserve, but this is yet to be documented. The objective of this study is to document the traditional knowledge, uses and conservation of medicinal plants among the fringed communities in the Togo Plateau Forest Reserve.
MATERIALS AND METHODS
Study area
The Togo Plateau Forest Reserve was established by the British Colonial Administration in 1929, in the then Trans-Volta-Togoland and gazetted in 1931 as a forest reserve in Ghana. The reserve occupies an area of 14.763 ha, making it the largest reserve in the Volta Region of the country. It lies within longitudes 0°15¢E and 0° 45¢E and latitudes 6° 45¢N and 7° 15¢ N with elevation between 250 and 2680 m.a.s.l (Figure 1). The reserve is surrounded by several communities, most of which depend on medicinal plant resources mostly from the reserve for their healthcare needs. These communities include Hohoe, Alavanyo, Santrokofi and Akpafu, which are located within the HohoeMunicipality, as well as Bowiri and Nkonya both in the Biakoye District.

The Hohoe municipality has a total land area of 1,172 km2, representing 5.6% of the land area of the Volta Region, and has Hohoe as its capital. The municipality lies in the wet semi-equatorial climatic zone, with annual rainfall of 1016-1210 mm and 4-5-month dry season between November and April. Temperatures are high throughout the year and range from 26 to about 32°C. The population of the Municipality in 2010 was 172.950 (Ghana Statistical Service, 2010). Major economic activities include agriculture, forestry and fishery. The Biakoye District, on the other hand, has a total land area of 738.20 km2, representing about 4.1% of the total land area of the region. The district capital is Nkonya Ahenkro.The district experiences the wet equatorial rainfall regime with its peak in July and September, respectively. The mean annual rainfall is about 1500 mm. There is a rather short dry season, which is characterized by the cool dry North-East trade winds from early December to mid-March. Temperatures vary between 22 and 34°C.The district is estimated to have 63,645 people (GSS, 2010). Major economic activities of the inhabitants include fishing, lumbering, carpentry, blacksmithing, distilling, palm oil extraction and gari processing.
Ethnobotanical study
Information on medicinal plant knowledge, use and their conservation status was sought through a structured questionnaire (Viertler, 2002) administered to a total of 384 people from six communities around the Togo Plateau Forest Reserve, Ghana. These informants (aged 30-70 years) were purposively and proportionately selected from each community in the order Hohoe (234 informant), Nkonya (42), Santrokofi (40), Bowiri (35), Alavanyo (23) and, Akpafu (10). The selection was done following consultation with opinion leaders, from the following category of medicinal plant dealers: certified traditional healers, traditional birth attendants (TBAs), vendors of herbal remedies, managers of herbal medicine centers, and local plant collectors. The selected informants were confirmed by GHAFTRAM as registered members. Information on respondents and medicinal plants of the study area including demographics (age, gender and education), growth form and plant parts used, condition before use and major uses constituted the checklist. Other data gathered included preparation methods, mode of administration, location and mode of plant collection, domestication status, and conservation status of these plants. Both local and scientific names of the plants were recorded with the help of experienced taxonomists. Scientific names were verified from the online resource “The Plant List” (2013, v1.1). The survey was conducted between September, 2017and June, 2018.
Data analysis
All medicinal plants encounted were compiled in a checklist including species same (local name, family, growth form, parts used, condition, and major uses). Descriptive statistics on the human conditions treated with the medicinal plants, the preparation methods, mode of administration and condition before use, availability, harvesting methods, and conservation status or efforts were also presented. The analyses were performed using MS Excel.
RESULTS
Socio-demographic characteristics of the studied communities
Majority of the informants (75%) were within the age bracket of 41-60 years, with males (39%) outnumbering the females (36%) (Table 1). Although all respondents had received formal education, only (17%) had reached the secondary school level or beyond. Results also indicated that all the respondents had knowledge of medicinal plants and their uses in the area, with (84%) of them claiming at least 6 years of experience as TM practitioners. Certified traditional healers constituted the largest category (30%) of practitioners identified in the study, followed by vendors of herbal medicine (27%), certified managers of herbal medicine centers (25%) and certified TBAs (14%). A small number of the respondents (4%) were classified as local plant collectors.

Medicinal plants identifiedin the study area
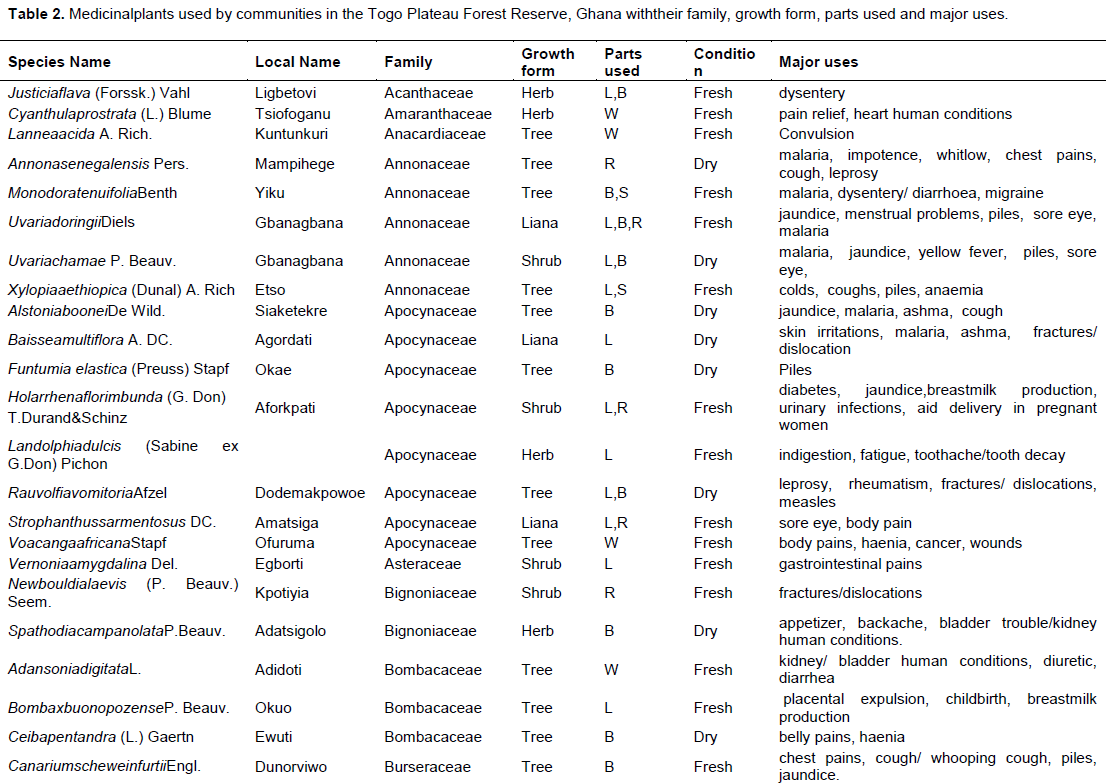
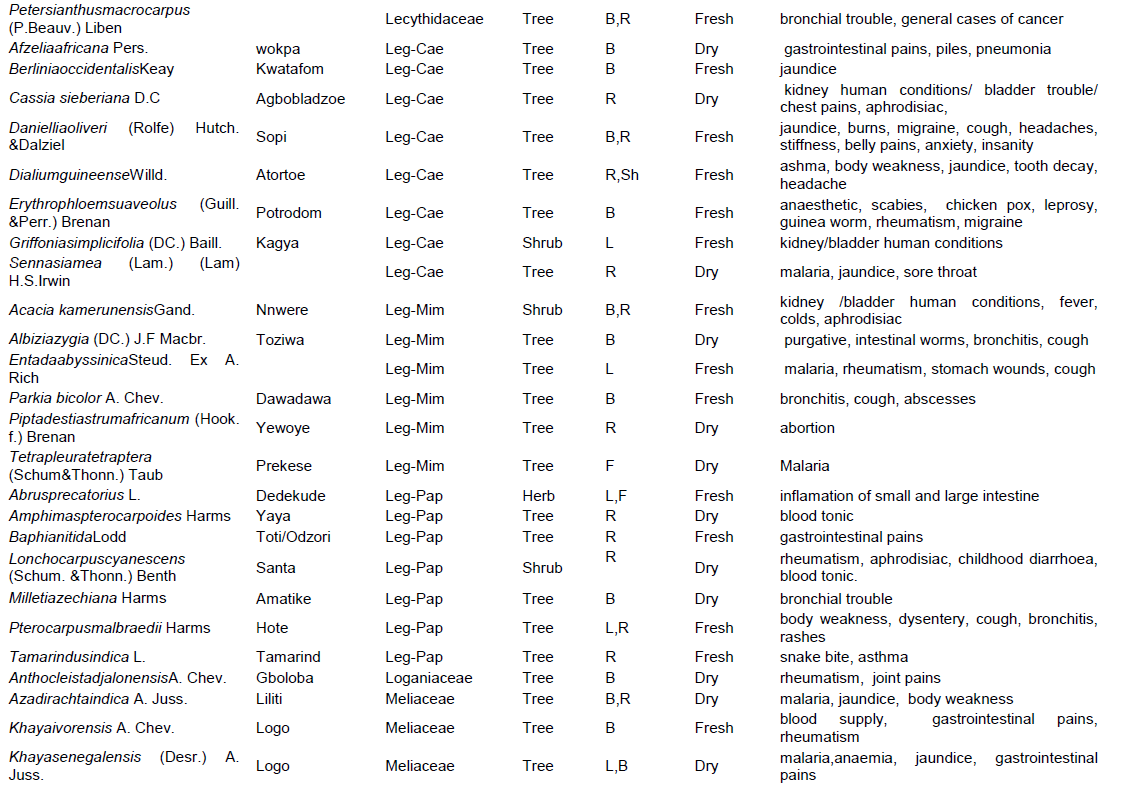
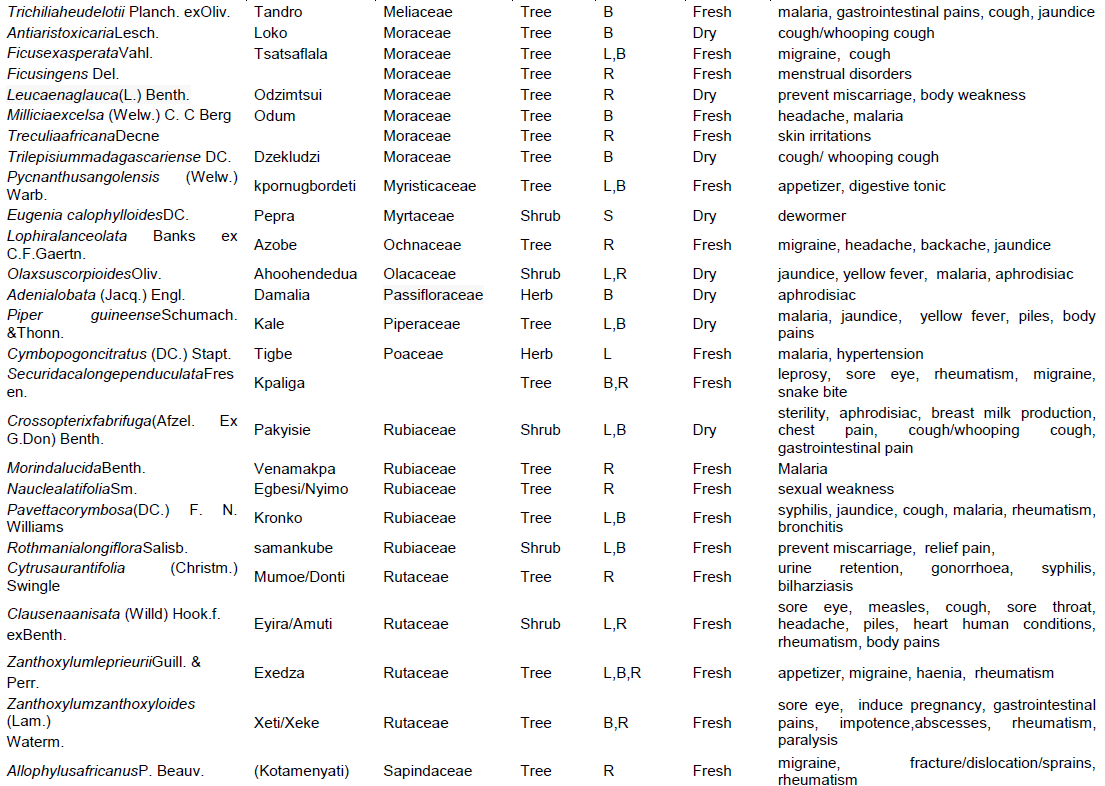
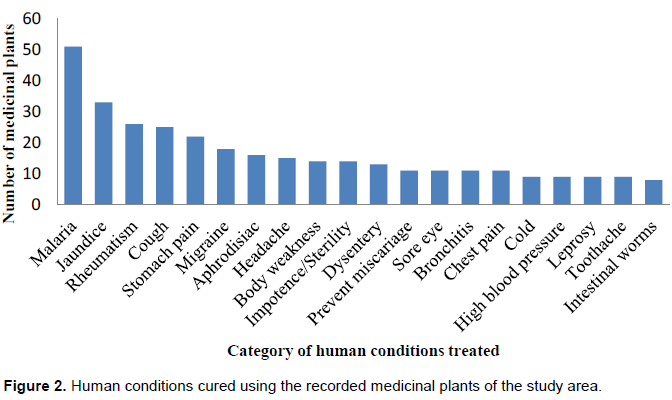
The study recorded 114 medicinal plant species, belonging to 42 families and distributed in four growth forms (14 herbs, six lianas, 21 shrubs and 74 trees) in the six communities surveyed (Table 2). Of the 42 families recorded, Leguminosae and Euphorbiaceae emerged as the most important medicinal plant families with 21 and 10 species, respectively, followed by Apocynaceae and Moraceae with seven species each. The remaining 38 families combined contributed 69 species. The medicinal plants identified in the study were reportedly used to treat about 75 human-related conditions (Table 2). Majority of the plants (51 species) were used to treat malaria, followed by jaundice (33), rheumatism (26), cough (25) and stomach pain (22) (Figure 2). Each of the remaining 70 conditions had 1-18 medicinal plant species cited as potential cure for it. The most commonly cited medicinal plant species were Azadirachta indica (256), Alstonia boonei (230), Morinda lucida (212) and Nauclea latifolia (193) (Figure 3).



The medicinal plants in the study area were collected from three sources, namely; forest reserve, garden and farmlands. Analysis revealed that (61%) of trees were collected from the forest reserve, (26%) from the farmland and 13% from the gardens. The distribution of shrubs and herbs followed a similar pattern as the trees, with majority collected from forests. Medicinal lianas were collected from two sources, namely; forest (80%) and farmland (20%) (Table 3).

Considering the domestication status, 65% of the tree species was collected from the wild while 35% was cultivated. From the shrubs, 68% were wild species whilst 32% were cultivated; 53% of the herbs were wild species whilst 47% were cultivated (Table 3). Different plant parts were used for the preparation of the traditional medicines (e.g., barks, roots, leaves, seeds and fruits). Of these, the bark (54 species) was more widely used than the roots (48) and leaves (44), but a few species however, the medicines are derived from the whole plant (6), seeds (5), fruits (3) and shoots (2) respectively (Figure 4).

Methods of preparation and modes of administration of medicinal plants
The most prevalent methods of medicinal plants preparation among thecommunities in the study area were decoction (51%), pounded (14%), powder (12%) and boil (10%). Other medicicines were seldomly prepared as infusion (4%), concoction (3%), crushed/mashed (2%), balm/ ointment (1%) and with juice, tea, tincture and poultice all accounting forless than (1%) (Table 4). With respect to the mode of administration of the drugs, 59% of the respondents reported that the medicines are taken orally. Other modes of administration include rubbing (10%), bathing (7%) and vapour bathing (6%). Few remedy preparations were applied through inhale vapour, drop on eye, ear, nose, sniffed, massage, chewed/swallowed and sit-bath (1–5%) (Table 4).

Medicinal plants and conservation practices
Most of the medicinal plants harvesting methods adopted by the respondents in the study area are destructive (81%) (Table 5). Most people collected the plant parts (59%) for medicine instead of the whole plant (11%) or individual plants (30%). On the availability of medicinal plants, 64% of the people noted that the plants were difficult or very difficult to find these days (Table 5). On whether the reserve was neccessary or not, majority of the people (45%) responded in the affirmative (Table 5). On the feasibility of conserving the medicinal plants, only 36% of the respondents agreed this was possible. The rest either did not agree (43%) or did not even appreciate the benefit associated with it (21%). Half (50%) of the respondent could not tell whether or not any conservation efforts had been made to save the Plateau from total degradation, although 31% acknowledged the initiation of such efforts either by the government or the community.

DISCUSSION
Demographic characteristics of the respondents
The study results confirmed the view that knowledge on medicinal uses of plants is often confined to the elderly (Abbiw, 1990; Addo-Fordjour et al., 2013; Jeyaprakash et al., 2011). This observation might be due to the fact that majority of the people in the study communities mostly spend their early years schooling and only resort to traditional medicine practice if they do not find jobs after school. The younger generation may also be ignorant about the vast medicinal resources available in their surroundings and/or are typically more inclined toward market resources (Addo-Fordjour et al., 2013).
The male dominance in the traditional medicinal practice over their female counterparts in this study could be linked to gender roles. The hectic nature of medicinal plants collection and processing appears to discourage many women from the practice. The few women encountered were mostly into vendorship (Abbiw, 1990; Addo-Fordjour et al., 2013).The educational status of respondents helps to ascertain their mindset towards conservation of medicinal plant species. People who have higher/tertiary education are believed to have a potential knowledge of conservation of medicinal plants and their use in curing human ailments than those with no or low level of education (Abbiw, 1990; Addo-Fordjour et al., 2013). Thus, the generally low level of education in the area (with 73% ending at the basic level) might have accounted for the limited knowledge on conservation of the medicinal plant species (Abbiw, 1990).
Medicinal plants use in the study area
Medicinal plant species richness (114) recorded by the communities around the Togo Plateau Forest Reserve is within the range recorded by severalsimilar studies. For example, Jeruto et al. (2008) recorded 115 species in the Nandi Forest in Kenya, Okello et al. (2009) recorded 107 species as used by the Sabaot people around Mt. Elgon, Ndegwa (2012) recorded 119 species as used by the Ogiek people in the East Mau forest, and Megersa et al. (2013) also recorded 126 species in WayuTuka District, West Ethiopia. Other studies, however, recorded less than 100 species. For example, e.g., Amri and Kisangau (2012) recorded 82 species in Kimboza Forest Reserve in Morogoro, Tanzania, Ziblim et al. (2013) recorded 47 species in the Northern Region, Ghana whereas Addo-Fordjour et al. (2013) had 52 species in the Aparapi Forest Reserve also in Ghana. The generally high number of medicinal plants species listed in this study confirms the vast knowledge of the peopleon medicinal plants in the area and their applications to treat human conditions.
The herbal preparations made from these medicinal plants were mostly used to treat malaria (51 species), jaundice (33), rheumatism (26), cough (25) and stomach pain (22), among others. This is evidenced in most of the informants citing plant species like Azadirachta indica, Alstonia boonei, Morinda lucida, Nauclea latifolia, etc. for the treatment of malaria, consistent with a number of previous studies (Addo-Fordjour et al., 2013; Asase et al., 2005; Jeyaprakash et al., 2011).
The greater contribution of the families Leguminosae, Euphorbiaceae, Apocynaceae and Moraceae to the medicinal plant species in this study confirms many similar studies (Abbiw, 1990; Asase et al., 2005). The more frequent use of trees for medicinal purpose by these communities relative to lianas, herbs and shrubs is also well documented by many studies (Amri and Kisangau, 2012; Jeruto et al., 2008; Megersa et al., 2013; Ndegwa, 2012; Okello et al., 2009).
Leguminosae happened to have most abundant and widely distributed component species on the plateau from the inventory study, probably explaining why the people are more familiar with plants from this family and their uses.
The study communities are very close to the reserve and this makes assessing it for medicinal plants an easy task. This has accounted for most of the plants listed being wild species (Abbiw, 1990; Addo-Fordjour et al., 2013; Datta et al., 2014; Ziblim et al., 2013). This practice of collecting most of the medicinal plants from the reserve by these communities is a threat to the survival of the reserve as it is now visibly seen that the wild stock of the reserve is eroded at the base. The practice is against the recommendations made by WHO (2015) that medicinal plant materials should be cultivated in farmlands and gardens to ensure their continual supply and therefore reduce the pressure on wild species. Countries like China have cultivated between 100–250 species of medicinal plants (Schippmann et al., 2002). In Africa, however, South Africa is the only country with records ofcultivation of medicinal plants, and even that an estimated 99% of the 400–550 species currently sold for use in traditional medicine originate from wild sources and only 1% are cultivated (Kakudidi et al., 2000).
The collection and use of plant barks and roots for medicinal purposes by the communities are not compatible with international conservation policies (Bussmann et al., 2011; Kamatenesi-Mugisha et al., 2000; Kamatenesi-Mugisha and Bukenya-Ziraba, 2002; Ziblim et al., 2013), as such practices can affect the survival of plants or may even remove their gene pool from the population. For that matter, harvesting of these plant parts would require careful monitoring to allow sufficient time for regeneration of the medicinal plants. The low level of education of the informants might be the reason why most of them are not adhering to the basic scientific principles of medicinal plants harvesting in a sustainable way.
Method of preparation and mode ofadministrationof medicinal plants
The use of different preparation methods of medicinal plants (e.g., decoction, pounded, powder, boil, infusion, concoction) and modes of administration (either internally or externally) to cure human conditions agree with many similar studies around forest-fringed communities (Abbiw, 1990).
The decoction was obtained by boiling the plant parts in water until the volume of the water reduced to minimum or required amount. The powder was prepared by grinding or pounding of the dried plant parts. The inhalation was done by burning of plant parts and inhaling the smoke through the nose or mouth. Poultices were done by crushing the plant part and mixing with a little hot water and apply directly over the area. Rubbing was done by crushing the plant part andmixing with water or processed as ointment/liniment and rubbed on body.
Tincture was prepared by placing the plant part into alcohol and leaving it to steep for a few days in a tightly sealed container. Infusion was done by steeping the plant part in cold water/hot water often overnight, the mixture is then strained.
The herbal remedies commonly used by the studied communities including drinking, rubbing, bathing,vapour bathing and inhalation are in keeping with findings of previous studies in Ghana (Abbiw, 1990; Addo-Fordjour et al., 2013; Asase et al., 2005; Ziblim et al., 2013). The frequent citation of malaria as the human conditions mostly treated with the medicinal plants in this study points to the widespread nature of these human conditions in the country and the urgent need to reverse this trend not only in the study area but also in other rural areas.
Medicinal plants and conservation practices
The unsustainable harvesting method employed by the respondents in the study area is a major concern as these activities can cause genetic erosion from the population and a general decline of biodiversity (Balemie et al., 2004; Megersa et al., 2013). Other threats to medicinal plants availability reported by the informants include drought, deforestation and firewood collection. Addressing some of these issues would require the domestication of some medicinal plant species which the indigenous people can easily fall on for their traditional remedies. This will reduce the pressure on the wild species. However, opinion on the need for the reserve by the people of the study area was very high. This is good because such reserves provide numerous benefits to man, including the maintenance of global and regional temperatures within appreciable range through the sequestration of carbon, protection of endangered species by serving as habitats, provision of food, supply of oxygen, etc. (Akerele et al., 1991; Balemie et al., 2004; Bodeker, 2002; Bussmann et al., 2011; Kamatenesi-Mugisha et al., 2000; Kamatenesi-Mugisha and Bukenya-Ziraba, 2002; Megersa et al., 2013).
The negative view of conservation of the reserve by some of the informants, citing restricted access to forest products, which serve as the source of their livelihood sustainance and restricted access to medicinal plants leading to loss of traditional botanical/medicinal knowledge is quite a serious issue (Akerele et al., 1991; Balemie et al., 2004; Bodeker, 2002; Kamatenesi-Mugisha et al., 2000; Megersa et al., 2013).
In this regard, the establishment of by-laws by the Ghana Wildlife Society to regulate collection of medicinal plants from the reserve is a step in the right direction. There should be conscious effort by both the government and the community towards the conservation of biodiversity of the plateau.
CONCLUSION
The study results demonstrated a rich diversity of medicinal plants used to treat a variety of ailments by communities around the Togo Plateau Forest Reserve. Leguminosae is the most represented medicinal plant family in the study area. This is evident from the floristic inventory, which recorded most of the tree species from this family on the landscape. The component species should therefore be targetedand managed sustainably. Crucially, most of the medicinal plants were collected from the reserve, exposing it to the danger of deforestation. Domestication (cultivation of medicinal plants in farmlands and gardens) therefore is the obvious management choice as it could help reduce the pressure on the wild species stock (Bodeker, 2002). The local people have very little knowledge on conservation issues; hence there is an urgent need to include them in resources utilization and management of the reserve. Also there is the need for workshops to be organised periodically by resource persons from either the Ghana Federation of Traditional Medicine Practitioners’ Association or Ghana Forestry Services Division to educate these plant poachers on appropriate conservation measures for plant exploitation.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Abbiw D (1990). Useful plants of Ghana. London: Intermediate Technology Publications Ltd. and the Royal Botanic Gardens, Kew. |
|
|
Addo-Fordjour P, Anning AK, Belford EJD, Akonnor D (2013). Diversity and conservation of medicinal plants in the Bomaa community of the BrongAhafo region, Ghana. Journal of Medicinal Plants Research 2 (9):226-233. |
|
|
Agbovie T, Amponsah K, Crentsil OR, Dennis F, Odamtten GT, Ofusohene-Djan W (2002). Conservation and sustainable use of medicinal plants in Ghana: Ethnobotanical survey. |
|
|
Akerele O, Heywood V, Synge H (1991). The conservation of medicinal plants: proceedings of an International Consultations 21-27 march 1988 held at Chiang Mai, Thailand. |
|
|
Amri E, Kisangau DP (2012). Ethnobotanical study of plants used in villagesaround Kimboza forest reserve in Morogoro, Tanzania.Journal of Ethnobiology and Ethnomedicine, 8:1 |
|
|
Asase A, Oteng- Yeboah AA, Odamtten GT, Simmonds MS(2005). Ethnobotanical study of some Ghanaian antimalarial plants. Journal of Ethnopharmacology Department of Botany University of Ghana. 99 (2):273-279. |
|
|
Balemie K, Kelbessa E, Asfaw Z (2004). Indigenous medicinal plant utilization, management and threats in Fentalle area, Eastern Shewa, Ethiopia.Ethiop Journal Biology Science 3(1):37058. |
|
|
Bodeker G (2002). Medicinal Plants: Towards Sustainability and Security. Green College, Oxford, UK. |
|
|
Bussmann RW, Swartzinsky P, Worede A, Evangelista P (2011). Plantuse in Odo-Bulu and Demaro, Bale region, Ethiopia J. Ethnobiol.Ethnomed. 7:28 University Press pp. 337-358. |
|
|
Datta T, PatraAK, DastidarSG (2014). Medicinal plants used by tribal population of Coochbehar district, WestBengal, India.Department of Zoology, Ananda Chandra College, Jalpaiguri-735101, West Bengal, India. |
|
|
Dold T, Cocks M (2001). The trade in medicinal plants in the Eastern Cape Province, South Africa.TRAFFIC Bulletin 18: 11-13. |
|
|
Fyhrquist P (2007) Traditional Medicinal uses and biological activities of some extracts of African Combretum, Terminalia and Pteleopsisspecies 183 p. |
|
|
Ghana Statistical Service (GSS)(2010). Population and Housing Census (PHC). |
|
|
Ita PB, Offiong EE (2013). Medicinal Plants Used in Traditional Medicine by RuralCommunities in Cross River State, NigeriaDepartment of Forestry and Wildlife Resources Management, University of Calabar, Calabar |
|
|
Jeyaprakash K, Ayyanar M, Geetha KN, Sekar T (2011). Traditional uses of medicinal plants among the tribal people in Theni District (Western Ghats), Southern India. Asian Pacific Journal of Tropical Biomedicine 1(1):S20-S25. |
|
|
Jeruto P, Lukhoba C, Ouma G (2008). An ethnobotanical study of medicinal plants used by the Nandi people in Kenya. Journal of Ethnopharmacology 116(2):370-376. |
|
|
Kakudidi EKZ, Bukenya-Ziraba R, Kasenene JM (2000). The medicinal plants in and around Kibale National Park in Western Uganda A Norwegian Journal of Botany (Lidia) 5:109-124. |
|
|
Kala CP (2005). Current status of medicinal plants used by traditional vaidyas in Uttaranchal State of India.Ethnobotany Research Applied 3:267-278. |
|
|
Kamatenesi-Mugisha M, Bukenya-Ziraba R (2002). Ethnobotanicalsurvey methods to monitor and assess the sustainable harvesting ofmedicinal plants in Uganda. In Maunder et al. (eds)Plant Conservation in the Tropics.Perspectives and practice.RoyalBotanical Gardens, Kew.The Cromwell Press Ltd, UK, pp. 467-482. |
|
|
Kamatenesi-Mugisha M, Oryem-Origa H, Odyek O, Makawiti DW (2008). Medicinal plants used in the treatment of fungal and bacterial infections in and around Queen Elizabeth Biosphere Reserve, Western Uganda.African Journal of Ecology 46:90-97. |
|
|
Koduru S, Grierson DS, Afolayan AJ (2007). Ethnobotanical information of medicinal plants used for treatment of cancer in the Eastern Cape Province, South Africa. Current Science 92(7):906-908. |
|
|
Megersa M, Asfaw Z, Kelbessa E, Beyene A, Woldeab B (2013). An ethnobotanical study of medicinal plants in WayuTuka District, East Welega Zone of OromiaRegional State, West Ethiopia. |
|
|
Ndegwa FK (2012). Use, conservation and harvesting of medicinal plants by the Ogiek people of East Mau forest, Nakuru district, Kenya. Kenyatta University. |
|
|
Okello J, Ssegawa P (2007). Medicinal plants used by communities of Ngaisubcounty, Apac district, Northern Uganda. African Journal of Ecology 45:76-83. |
|
|
Okello SV, Nyunja RO, Netondo GW, Onyango JC (2009). Ethnobotanical study of medicinal plants used by Sabaots of Mt. Elgon Kenya. African Journal of Traditional, Complementary and Alternative Medicines 7(1):1-10. |
|
|
Schippmann U, Leaman DJ, Cunningham AB (2002). Impact of Cultivation and Gathering ofMedicinal Plants on Biodiversity: Global Trends and Issues. Inter-Department Working Group onBiology Diversity for Food and Agriculture, FAO, Rome, Italy. |
|
|
Satpong K (2000). Traditional medicine for the 21st century in Ghana- The role of the scientist/researcher. Commonwealth Lecture Theatre, University of Ghana, as part of traditional medicine week celebrations for the year 2000. |
|
|
Viertler RB (2002). Métodosantropológicoscomoferramentaparaestudoemetnobiologia e etnoecologia. pp. 12-29. In: M.C.M. Amorozo; L.C. Ming & S.M.P. Silva (orgs.). Métodosdecoleta e análise de dados emetnobiologia, etnoecologia e disciplinascorrelatas. Rio Claro, UNESP/CNPq. |
|
|
World Health Organization (WHO) (2015) Traditional medicine – growing needs and potential. WHOPolicy Perspectives Medecine 2:1-6. |
|
|
Ziblim IA, Khan AT, Eledi JD (2013). Exploitation and use of medicinal plants, Northern Region, GhanaUniversity for Development Studies, Department of Range and Wildlife Management, Nyankpala Campus. Tamale, Ghana. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


