Full Length Research Paper
ABSTRACT
Diabetes is a common disease in sub-Saharan Africa. Complications associated with type 2 diabetes mellitus are due to macro-vascular and micro-vascular lesions. One of the less known complications of diabetes is impaired respiratory function. The objective of this study was to evaluate the ventilatory function of Senegalese type 2 diabetics. A total of Sixty-four women composed to 32 diabetic subjects and 32 healthy control individuals were included in this study. Spirographic recording was realized for the two groups. The HbAc1of diabetic patients was measured and duration of diabetic status was estimated and the diabetic groups were sub-divided according to HbA1C level (group -a>7.5%, group- b ≤ to 7.5%) and diabetic duration (group a> to 10 years and group< to 10 years). It was observed that 59% of diabetic patients had an obstructive bronchial which was localized in the distal bronchi. For the restrictive syndrome it was found in 31% of population with diabetic. Diabetes could cause a restrictive and obstructive ventilatory disorder. This phenomonea might probably be due to glycosylation abnormalities linked to type 2 diabetes.
Key words: Type 2 diabetes, spirometry, obstructive ventilatory disorder, restrictive ventilatory disorder.
INTRODUCTION
Diabetes mellitus (DM) is a principal cause of cardiac ischemia considered as major public health problem. DM affects a large part of the world's population and its incidence is increasing significantly. The World Health Organization estimates that more than 180 million people worldwide are reported to have diabetes and this number is expected to double by 2030 (WHO, 2008). There is an alarming increase in the incidence and prevalence of diabetes mellitus, particularly in sub-Saharan Africa. According to data from the International Diabetes Federation (Tao et al., 2015), Africa is among the most affected areas with 27.5 million people with diabetes. In Senegal, although the prevalence of type 2 diabetes varies according to localities and sources, several studies indicate rates ranging from 6 to 10% of the general population (Mbanya et al., 2014). Chronic hyperglycemia is responsible for protein glycation which leads to thickening of the basement membrane, particularly that of capillaries, with weakening of the capillaries leading to microangiopathy. These lesions cause complications in several organs, mainly the kidney, retina and peripheral nervous system (American Diabetes Association, 2014). The presence of abundant connective tissue and significant microvascular circulation in the lung suggests that the lung is not immune to diabetes. There is growing evidence that the lungs are also one of the target organs for diabetic microangiopathy in patients with type 2 diabetes (Pitocco et al., 2012; Sandler, 1990). Autopsy results in human diabetic subjects included thickening of the alveolar epithelium and pulmonary capillary basal membranes, centrilobular emphysema and pulmonary microangiopathy (Vracko et al., 1979; Kodolova et al., 1982).
However, due to its high reserve, a substantial loss of the pulmonary microvascular layer can be tolerated and often ignored by patients and physicians. Thus, diabetic pulmonary microangiopathy may be clinically under-diagnosed. The pulmonary complications of diabetes have been poorly characterized and have given contradictory results.
Pre-existing ventilatory function disorders are now suspected to be one of the risk factors for respiratory infections in diabetics (Asanuma et al., 1985). In this regard, studies on the reduction of forced vital capacity and maximum expiratory volume in one second (FEV1) have been reported (Schuyler et al., 1976). Clinical studies have observed a restrictive syndrome and damage of the alveolar-capillary membrane due to microangiopathy (Chance et al., 2008 ; Guverner et al., 2003). Mannino et al. (2003, 2006) showed that ventilatory disorders were associated with an increased risk of death. In addition, impaired ventilatory function related to diabetes could compromise new insulin delivery systems such as inhaled insulin.
The purpose of our study was to evaluate the ventilatory function of subjects with type 2 non-smoking diabetes under medical follow-up in the Thies region.
MATERIALS AND METHODS
Study design
This study was conducted at the department of functional explorations and the various diabetes care centres in Thies, Senegal. This is a descriptive and comparative cross-sectional study that took place over the period from 1 March 2015 to 30 September2018. The protocol was designed in accordance with the guidelines set out in the Helsinki Declaration and approved by the Ethics Committee of the Faculty of Health Sciences of the University of Cheikh Anta Diop (0411/2018/CER/UCAD). All subjects had agreed to voluntarily participate in the study by signing a free and informed consent form.
Study population
Sixty-four 64 Senegalese women participated in this study. Thirty-two subjects have type 2 diabetes and 32 subjects do not have diabetes (control group). Controls were matched by age, weight, height and came from the same community with the same socio-economic status as type 2 diabetes patients.
A patient was considered diabetic if she or he had at least one of the following two criteria: a blood glucose level higher than 126 mg/dl (7.0 mmol/l) after an 8-h fast and checked twice, or the presence of diabetes symptoms (polyuria, polydipsia, weight loss) associated with a blood glucose level (on venous plasma) higher than or equal to 200 mg/dl (11.1 mmol/L) (Baynest, 2015).
Subjects with pregnancy, spinal column or ribcage abnormalities, neuromuscular diseases, chronic progressive cardiopulmonary pathology known at the time of the study were excluded. Besides, subjects with current or previous drug or tobacco addictions and patients with diabetes complications such as neuropathy, nephropathy and retinopathy were also excluded.
Anthropometric and cardiovascular parameters
All participants underwent a full clinical examination and completed a standard questionnaire on smoking habits, alcohol consumption, detailed medical history, including medication, and family history of diabetes. The existence of micro and macro vascular complications such as the presence of vision disorders, paresthesia of the limbs or high blood pressure (HBP) was also investigated.
Anthropometric data such as age, weight and height were determined. The weight of our subjects was measured using a SECA-type weighing scale. The body mass index (BMI) of our subjects expressed in kg/m² was calculated by the Quetelet formula: BMI= weight (kg)/height (m²). Weight was assessed in the morning at 8 a.m. in subjects with barefoot and light clothing. Systolic (SBP) and diastolic (DBP) blood pressures were measured manually using a validated sphygmomanometer (Spengler CE, 0459; France). Blood pressure measurements were performed according to the recommendations of the American Heart Association (AHA) (Pickering et al., 2005). The patients were comfortably seated in a quiet room at ambient temperature and had been at rest for more than 15 min. In a sitting position, the arms were relaxed with the forearms supported; blood pressure was taken with a cuff placed on the plane of the heart and taking 2/3 of the left arm.
Biochemical parameters
Blood samples were taken from each subject who was fasting. Fasting blood glucose and lipid profile (triglycerides, LDL-cholesterol, HDL-cholesterol and total cholesterol) were measured in the morning in fasting subjects using the standard enzymatic method. The determination of glycated hemoglobin (HbA1c) was performed using high-performance liquid chromatography (HPLC) on freshly collected whole blood.
Spirographic recording
The spirometry was performed using a Jaeger PNEUMO care Fusion electronic spirometer coupled to a computer in which a data analysis software is installed. All the tests were performed at a specific time of day (10:00 am - 2:00 pm) to minimize daytime variations. The device was calibrated daily and operated in the ambient temperature range of 25 to 40 degrees Celsius. Explanations and supporting illustrations were provided in advance regarding the conduct of the examination. The tests were performed according to American Thoracic Society / European Respiratory Society guidelines (ATS / ERS guidelines) (Miller et al., 2005) in a quiet room seated with a soft nose clip. Subjects performed the spirometric tests three times at 15-min intervals and the best of the three was taken into account. The parameters recorded were: forced vital capacity (FVC) in litre, maximum expiratory volume in 1 second (FEV1) in litre, Tiffeneau ratio FEV1 / FVC expressed as a percentage, maximum expiratory flow at 25% of the FVC (FEF25%), maximum expiratory flow at 50% of the FVC (FEF50%), maximum expiratory flow at 75% of the FVC (FEF75%), maximum expiratory flow between 25 to 75% of the FVC (FEF25-75%). We defined the obstructive syndrome based on a decrease in the FEV1/CVF ratio (less than 70%) and an FEV1 < 80% of the predicted value with FEV1 < FEV1 and the restrictive syndrome on the basis of a decrease in FEV1 < 80% of the predicted value and a normal FEV1/CVF ratio (>70%).
Statistical analysis
The statistical analyses were carried out using Graph Pad Version 5 software. The data were expressed as percentages, averages and standard deviations. The student test made it possible to compare the averages. The Pearson test was used to look for the correlation between the different variables studied. The significance threshold was set at p<0.05, a p-value of less than 0.05.
RESULTS
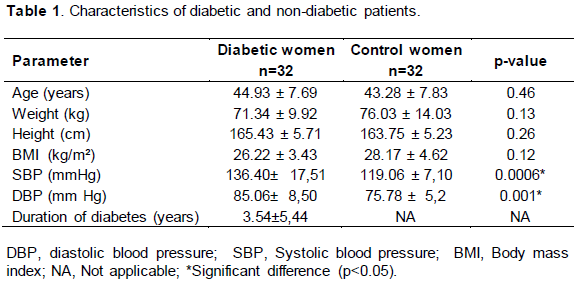
Anthropometric data such as age, height, weight and body mass index have been represented in Table 1. Our results showed that there was no statistically significant difference between the two groups in age and BMI. The average age of diabetic subjects was 44.93±7.69 years compared to 43.28±7.83 years for controls (p<0.46). The average BMI was 26.22±3.43 kg/m² in the diabetic group and 28.17±4.62 kg/m² for female controls. The average duration of T2D in our population was estimated at 3.54 years for a seniority ranging from 1 month to 13 years.
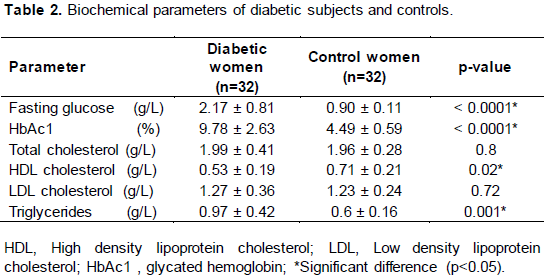
The biochemical profile data are presented in Table 2. The average fasting blood glucose level was 2.17 ± 0.81 g/l in diabetic patients and 0.90 ± 0.11g/l in control subjects with a significant difference noted (p = 0.0001). The average percentage of glycated hemoglobin in diabetic patients was high compared to the control group (9.78±2.63% vs. 4.49±0.59%). Concerning the lipid profile, a significantly higher level of triglycerides was noted in type 2 diabetics (0.97 ± 0.42 g/l vs 0.6 ± 0.16g/l; p = 0.001).
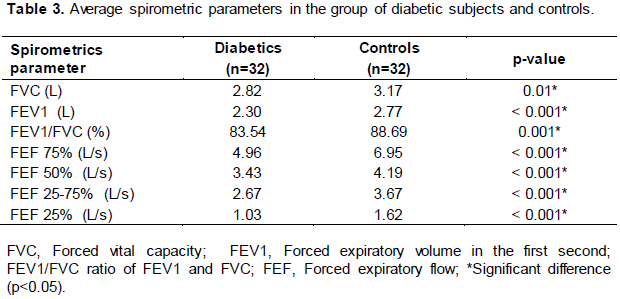
When comparing the diabetics and non-diabetic women, the average of spirometric parameters including forced vital capacity (FVC), forced first-second expiratory volume (FEV1), maximum expiratory flow rates (FEF25%, FEF50%, FEF75% and FEF25-75%) were significantly lower (p<0.05) in patients with type 2 diabetes compared to those without diabetes (Table 3).
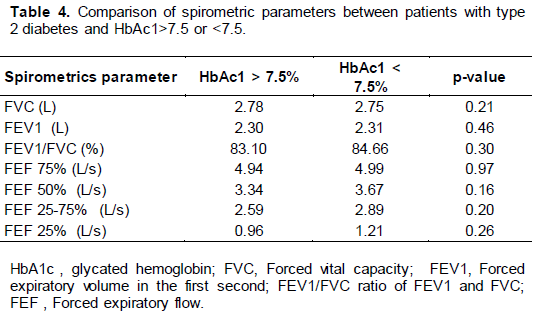
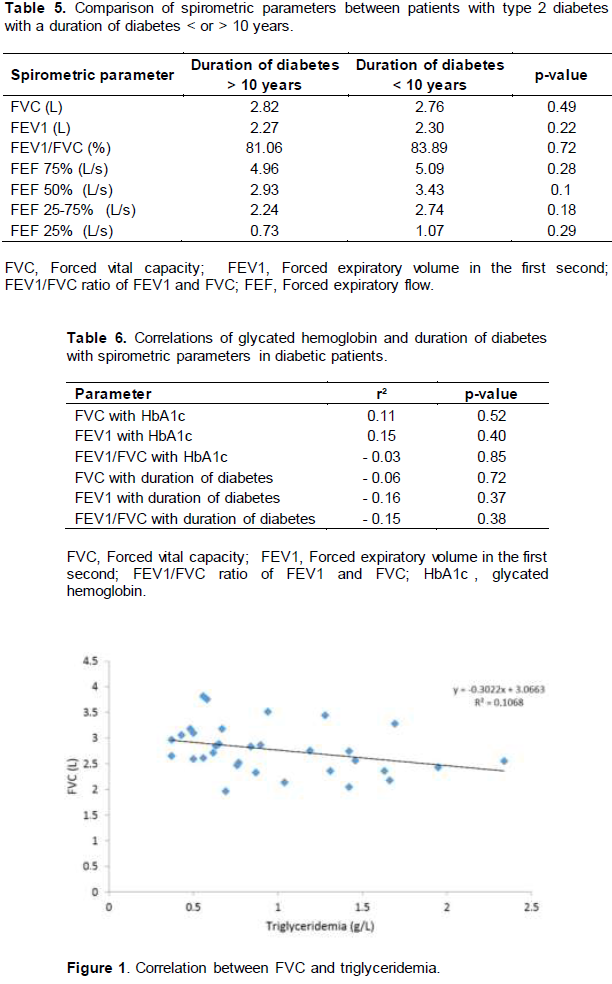
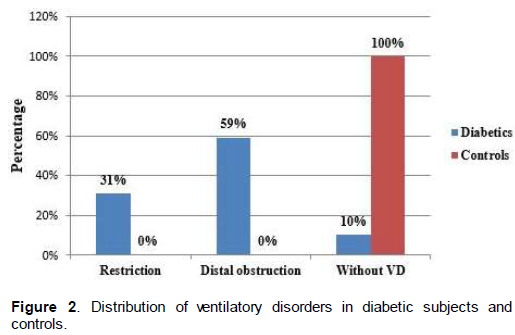
The best parameter to assess the level of metabolic control of diabetes is the HbA1c level. To assess the effect of diabetes metabolic control on ventilatory disorders, patients were divided into two subgroups based on their HbA1c levels: well controlled [n =9; HbAc1 ≤7.5%] with an average HbAc1 of 6.32 ± 0.98 and poorly controlled (n = 23; HbAc1 > 7.5%) with an average HbA1c of 11.20 ± .73. There was no significant difference in the average of the spirometric parameters according to the percentage of HbAc1 higher than or equal to 7.5% in diabetic patients. To determine the effect of diabetes duration on spirometric parameters, diabetic patients were divided into two subgroups: one with diabetes duration <10 years (n =28) with an average duration of 2.30 ± 1.71 years and the other with a diabetes duration longer than 10 years (n =4) with an average of 12 ± 0.81 (Table 4). There was significant difference between the averages of the spirometric parameters between the groups (Table 5). By correlating FVC and FEV1 with the duration of diabetes and HbA1, there were no significant correlations between them (Table 6). On the other hand, CVF was significantly correlated with triglyceridemia (Figure 1). We found a restriction in 31% of our diabetic subjects and 59% had distal obstruction. Our control subjects did not have any ventilatory disorders (Figure 2).
DISCUSSION
Our study showed that the ventilatory function of diabetic subjects was significantly impaired compared to control subjects. In fact, there is a significant decrease in FVC, FEV1, FEV1/FVC ratio and instantaneous and median maximum expiratory flow rates at 75, 50, 25 and 25-75% in the diabetic group compared to the Senegalese reference values of healthy subjects. Recent studies (Röhling et al., 2018) have even shown that this ventilatory impairment is present even in patients with newly diagnosed type 2 diabetes mellitus compared to a matched glucose tolerant control group for age, sex, BMI and smoking status. Although it is well described that deterioration respiratory function is related to obesity or overweight, in our study there was no difference between the groups for the BMI (26.22 ±3.43 kgm2 for diabetics and 28.17 ± 4.62 kgm2 for control subjects) .
The decrease in FVC and FEV1 observed in diabetic patients in our study is consistent with the results of the analysis by van den Borst et al. (2010) on ventilatory function in diabetic subjects, which showed a 5.1% decrease in FEV1 in diabetic patients compared to the predicted value and a 6.3% decrease in vital capacity. Their results are consistent with those of Davis et al. who showed an average decrease of 9.5% in average FVC values in diabetics (Davis et al., 2000) and may be due to a decrease in defenses against environmental pollution such as smoking and diabetes-related respiratory tract infections (Sreeja et al., 2003; Lange et al., 2002). Similar results have been reported by Asanuma et al. (1985) and Lange et al. (1989). There was a decrease in FVC and FEV1 in type 2 diabetic subjects compared to control subjects. However, other studies have shown that FVC and FEV1 are within the predicted values for type 2 diabetes (Lange et al., 2002; Litonjua et al., 2005; Benbassat 2001). These inconsistencies could be due to the limitations of these studies, including the definition of diabetes, methodological differences, generally small sample sizes and heterogeneity of the populations studied in terms of age, race, duration of disease, degree of metabolic control and presence of complications. Some studies have even included patients with a history of smoking or previous lung damage (Buckingham et al., 1986; Lujbic et al., 1998).
In addition, our study also showed an obstructive syndrome objective by a decrease in the FEV1 and FEV1/FVC ratio in diabetic subjects compared to non-diabetic subjects. These data confirm the hypothesis that the respiratory function of the diabetes subject is associated with airway obstruction. A study conducted by the Framingham Research Centre evaluated respiratory function in individuals with type 2 diabetes without antidiabetic treatment. The results showed that the FEV1 reduction was greater than the FVC reduction resulting in a reduction in FEV1/FVC (Walter et al., 2003).
Our results confirm those of the previous studies showing that restrictive lung disease occurs in diabetes. Similar results have been observed by other researchers (Sinha et al., 2004; Davis et al., 2004; Sonoda et al., 2018). Impaired lung function with restrictive ventilatory disorder type in patients with T2DM has been demonstrated in a meta-analysis (Van Den Borst et al., 2010). Furthermore, a small cross-sectional study (n = 60 patients) also suggests an association between T2DM and a restrictive respiratory profile (Anadhalakshmi et al., 2013). Non-enzymatic glycation of lung tissues, in particular collagen and elastin damage (Lecube et al., 2010), but also damage to thoracic neuro-muscular function (Van Den Borst et al., 2010; Yeh et al., 2008) are thought to be responsible for restrictive ventilation disorders.
Data on obstructive pulmonary disease in diabetic patients are sometimes inconsistent, probably due to population heterogeneity (type 1 and 2 diabetes, smoking status, age, BMI). A distal obstructive pulmonary disease pattern with reduced values of FEF25-75% has been found in our patients with type 2 diabetes mellitus that may be due to their inflammatory status (Yeh et al., 2008). The study by Mario Cazzola et al. (2012) on bronchial tubes isolated in humans elucidated the character of obstructive pulmonary pathology in diabetics at the molecular level. Thus, hyperglycemia can independently contribute to airway obstruction in a similar way to peripheral airway inflammation leading to airway obstruction in asthma (Barnes, 2002). Moreover, in patients with T2DM, the pulmonary surfactant is insufficient, which may affect the stability of air flow and the alteration of airway calibres (Pellegrino et al., 2005). In our study, diabetic patients had significant hypertriglyceridemia compared to controls and a negative correlation was found between triglyceridemia and CFV. In other respects, Sinha et al. (2004) showed in their study a significant correlation between DLCO decrease and cholesterol levels. Dyslipidemia may play a non-contributory role in the pathogenesis of decreased lung function in diabetic patients.
CONCLUSION
Respiratory function is impaired during diabetes. The results of this study are in line with those of other authors, who strongly suggest that type 2 diabetes mellitus affects lung function and that impaired respiratory function is restrictive and obstructive, although the studies suggest an essentially restrictive pathology. The changes mentioned are probably due to non-enzymatic glycosylation of tissue proteins induced by hyperglycemia and chronic diabetic microangiopathy causing thickening of the basement membrane resulting in a reduction in tissue strength and elasticity.
It is therefore recommended that periodic respiratory functional investigations be performed in diabetic patients to assess the severity of impaired lung function. These measures will help prevent lung damage in the early stages and thus contribute to reducing morbidity and mortality in patients with type 2 diabetes.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
American Diabetes Association (2014). Standards of medical care in diabetes. Diabetes Care 37:14-80. |
|
|
Anadhalakshmi S, Manikandan S, Ganeshkumar P, Ramachandran C (2013). Alveolar gas exchange and pulmonary functions in patients with type II diabetes mellitus. Journal of Clinical and Diagnostic Research 7(9):1874-1877. |
|
|
Asanuma Y, Fujiya S, Ide H, Agishi Y (1985). Characteristics of pulmonary function in patients with diabetes mellitus. Diabetes Research and Clinical Practice 1(2):95-10 |
|
|
Barnes PJ (2002). The role of inflammation and anti-inflammatory medication in asthma. Respiratory Medecine 96(Suppl. A):9-15. |
|
|
Baynest HW (2015). Classification, Pathophysiology, Diagnosis and Management of Diabetes Mellitus. Journal of Diabetes and Metabolism 6 (5):1-9. |
|
|
Buckingham B, Perejda AJ, Sandborg C, Kershnar AK, Uitto J (1986). Skin, joint, and pulmonary changes in type 1 diabetes mellitus. American Journal of Diseases of Children 140 (5):420-423. |
|
|
Chance WW, Rhee C, Yilmaz C, Dane DM, Pruneda ML, Raskin P, Hsia CCW (2008). Diminished alveolar microvascular reserves in type 2 diabetes reflect systemic microangiopathy. Diabetes Care 31(8):1596-1601. |
|
|
Cazzola M, Calzetta L, Rogliani P, Lauro D, Novelli L, Clive P, Kanavar V, Matera MG (2012). High Glucose Enhances Responsiveness of Human Airways Smooth Muscle via the Rho/ROCK Pathway. American Journal Respiratory Cell and Molecular Biology 47 (4):509-516. |
|
|
Davis TM, Knuimann M, Kendall P. Davis WA (2000). Reduced pulmonary function and its association in type-2 Diabetes: the Fremantle Diabetes Study. Diabetes Research and Clinical Practice 50(2):153-159. |
|
|
Davis WA, Knuiman M, Kendall P, Grange V, Davis TM (2004). Glycemic exposure is associated with reduced pulmonary function in type 2 diabetes: the Fremantle Diabetes Study. Diabetes Care 27(3):752-57. |
|
|
Guverner N, Tucuncu NB, Akcay S, Eyuboglu F, Gokcel A (2003). Alveolar gas exchange in patients with type 2 diabetes mellitus. Endocrine Journal 50(6):663-667. |
|
|
Kodolova IM, Lysenko LV, Saltykov BB (1982). Changes in the lungs in diabetes mellitus. Arkhiv Patologii 44 (7):35-40. |
|
|
Lange P, Parner J, Schnohr P, Jensen G (2002). Copenhagen City Heart Study: longitudinal analysis of ventilatory capacity in diabetic and non-diabetic adults. European Respiratory Journal 20:1406-1412. |
|
|
Lange P, Groth S, Kastrup J, Mortensen J, Appleyard M, Nyboe J, Jensen G, Schnohr P (1989). Diabetes mellitus, plasma glucose and lung function in a cross-sectional population study. European Respiratory Journal 2 (1):14-19. |
|
|
Lecube A, Sampol G, Munoz X, Hernandez C, Mesa J, Simo R (2010). Type 2 diabetes impairs pulmonary function in morbidly obese women: A case-control study. Diabetologia 53(6):1210-1216 |
|
|
Litonjua AA, Lazarus R, Sparrow D, Demolles D, Weiss ST (2005). Lung function in type 2 diabetes: the Normative Aging Study. Respiratory Medecine 99 (12):1583-1590. |
|
|
Lujbic S, Metelko Z, Car N, Roglic G, Drazic Z (1998). Reduction of diffusion capacity for carbon monoxide in diabetic patients Chest 114 (4):1033-5 |
|
|
Mannino DM, Doherty DE, Sonia Buist A (2006). Global Initiative on Obstructive Lung Disease (GOLD) classification of lung disease and mortality: findings from the Atherosclerosis Risk in Communities (ARIC) study. Respiratory Medecine 100(1):115-122. |
|
|
Mannino DM, Buist AS, Petty TL, Enright PL, Redd SC (2003). Lung function and mortality in the United States: data from the First National Health and Nutrition Examination Survey follow up study. Thorax 58(5):388-393. |
|
|
Mbanya JC, Assah FK, Saji J, Atanga EN (2014). Obesity and type 2 diabetes in Sub-Sahara Africa. Current diabetes reports 14(7):501. |
|
|
Miller MR, Hankinson J, Brusasco V, Burgos F, Casaburi R, Coates A, Crapo R, Enright P, Van Der Grinten CP, Gustafsson P, Jensen R, Johnson DC, MacIntyre N, McKay R, Navajas D, Pedersen OF, Pellegrino R, Viegi G, Wanger J (2005). Standardization of spirometry. European Respiratory Journal 26(2):319‑38. |
|
|
Pellegrino R, Viegi G, Brusasco V, Crapo RO, .Burgos F, Casaburi R, Coates A, Van Der Grinten CPM, Gustafsson P, Hankinson J, Jensen R, Johnson DC, MacIntyre N, McKay R, Miller MR, Navajas D, Pedersen OF, Wanger J (2005). Interpretative strategies for lung function tests. European Respiratory Journal 26:948-968. |
|
|
Pickering TG, Hall JE, Appel LJ, Falkner BE, Graves JW, Hill MN, Jones DH, Kurtz T, Sheps SG, Roccella EJ (2005). Recommendations for blood pressure measurement in humans: an AHA scientific statement from the Council on High Blood Pressure Research Professional and Public Education Subcommittee. Journal of clinical Hypertension 7(2):102-109. |
|
|
Pitocco D, Fuso L, Conte EG, Zaccardi F, Condoluci C, Scavone G, Incalzi RA, Ghirlanda G (2012). The diabetic lung--a new target organ? Review of Diabetic Studies 9(1):23-35. |
|
|
Röhling M, Pesta D, Markgraf DF, Strassburger K, Knebel B, Burkart V, Julia Szendroedi, Karsten Müssig, Michael Roden, for the GDS study group. Metabolic (2018) Determinants of Impaired Pulmonary Function in Patients with Newly Diagnosed Type 2 Diabetes Mellitus. Experimental and Clinical Endocrinology and Diabetes 126(9):584-589. |
|
|
Sandler M (1990). Is the lung a 'target organ' in diabetes mellitus? Archives Internal Medecine 150 (7):1385-1388. |
|
|
Schuyler MR, Niewoehner DE, Inkley SR, Kohn R (1976). Abnormal lung elasticity in juvenile diabetes mellitus. American Review of Respiratory Disease 113(1):37-41. |
|
|
Sinha S, Guleria R, Misra A, Pandey RM, Yadev R, Tiwari S (2004). Pulmonary functions in patients with type 2 diabetes mellitus and correlation with anthropometry and microvascular complications. Indian Journal of Medical Research 119 (2):66-71. |
|
|
Sonoda N, Morimoto A, Tatsumi Y, Asayama K, Ohkubo T, Izawa S, Ohno Y (2018). The association between glycemic control and lung function impairment in individuals with diabetes: the Saku study. Diabetology International 19:10(3):213-218. |
|
|
Sreeja CK, Elizabeth Samuel, C Kesavachandran C, Shrusti Shashidhar (2003). Pulmonary function in patients with Diabetes Mellitus. Indian Journal of Physiology and Pharmacology 47(1):87-93. |
|
|
Tao Z, Shi A, Zhao J (2015). Epidemiological Perspectives of Diabetes. Cell Biochemistry and Biophysics 73(1):181-5. |
|
|
Van Den Borst B, Gosker HR, Zeegers MP, Schols AM (2010). Pulmonary function in diabetes a metaanalysis. Chest 138 (2):393-406. |
|
|
Vracko R, Thorning D, Huang TW (1979). Basal lamina of alveolar epithelial and capillaries. Quantitative changes with aging and with diabetes mellitus. American Review Respiratory Disease 120(5):973-83. |
|
|
Walter RE, Beiser A, Givelber RJ, O'Connor GT, Gottlieb DJ (2003). Association between glycemic state and lung function the Framingham Heart Study. American Journal of Respiratory and Critical Care Medicine 167(6):911-916. |
|
|
World Health Organization, WHO (2008) Fact sheet: Diabetes. No. 312, November. |
|
|
Yeh HC, Punjabi NM, Wang NY, Pankow JS, Duncan BB, Cox CE, Selvin E, Brancati FL (2008). Cross-sectional and prospective study of lung function in adults with type 2 diabetes: the Atherosclerosis Risk in Communities (ARIC) Study. Diabetes Care 31(4):741-746. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


