ABSTRACT
This purpose of this study was to investigate the effects of sodium bicarbonate ingestion on lactate steady state responses (blood lactate and heart rate) in female futsal players. 30 female futsal players volunteered to participate in this investigation. Participants were randomly assigned to either experimental group or placebo group. While the experimental group was ingested sodium bicarbonate supplementation (NaHCO3), the placebo group was ingested sodium chloride (NaCl). Participants were first tested using a standard incremental treadmill test to define the blood lactate profile. Running speeds corresponding to fixed blood lactate concentrations of 4.0 mmol.l-1 were calculated using linear interpolation. The maximal lactate steady state was determined from 30-min constant-speed treadmill runs. The maximal lactate steady state was defined as fastest running speed that produced no more than a 1.0 mmol.l-1 increase in blood lactate concentration between 10 and 30 min of exercise. Paired Samples T test was used to determine whether there are significant blood lactate and heart rate differences in before and after sodium bicarbonate ingestion. Test results showed a significant decrease in the post-supplement heart rate responses given by the sodium bicarbonate group at the 10th, 20th and 30th min of the lactate steady state exercise (p<0.05). Although an increase was recorded in the lactate responses of the experimental group, the only significant difference was recorded at the 20th min of the exercise after the sodium bicarbonate ingestion (p<0.05). In the control group, on the other hand, no significant difference was recorded in the pre-test and post-test values of any variables (p>0.05).
Key words: Lactate steady state, sodium bicarbonate, heart rate, blood lactate.
Futsal is a sports branch played for two equal periods of 20 min, during which clock is stopped whenever the ball is out of play, between two teams of five players each, one being a goalkeeper (ÇaÄŸlayan and Mehtap, 2010). It is played in a much narrower area (20 × 40 m) and at a tempo much higher than football (Barbero et al., 2008). Futsal is a high intensity, intermittent sport within structure where accelerations and short sprints are performed at
maximal or almost maximal intensity, interspersed by brief recovery periods during a relatively long period of time (Berdejo-del-Fresno, 2012).
It is well documented that blood lactate concentration is a result of the production in the working muscle and removal of lactate in the blood (Moxnes and Sandbakk, 2012). Lactate is produced by tissues during exercise or even at rest and formation and removal of the lactate is highly related to metabolic rate (Myers and Ashley, 1997; Stanley et al., 1988; Connett et al., 1984). For moderate constant work rates, the aerobic power increases towards a steady state condition. The concept of maximal lactate steady state (MLSS), that is the highest intensity where a steady state lactate can be obtained, has been regarded as important for endurance performance (Moxnes and Sandbakk, 2012; Billat et al., 2003; Margariaet et al., 1963).
Acids are molecules (such as lactic acid, carbonic acid, and similar molecules) that release hydrogen ions (H+). Inorganic acid is produced as a result of carbohydrate, fat, and protein metabolism. Dissociation of these acids increases the H+ ion concentration in body fluids (Sönmez, 2002). Moderate to high intensity exercise causes the formation of ionic changes within contracting muscles that contribute to development of acidosis (Putmanet et al., 2003; Lindinger et al., 1999; Kowalchuk et al., 1984). Production of lactic acid in the muscles causes a drop in muscle and blood pH due to the dissociation of lactic acid into lactate and hydrogen ions (Abbiss and Laursen, 2005; Juel, 1998; Bogdanis et al., 1994). Keeping pH within a normal range is obtained by buffering or excreting acids (Jones, 2010; Sönmez, 2002). To reduce the effect of free H+ ions, there are some alkaline substances in blood and muscles which combine with the H+ ion to buffer or neutralize them. These alkaline substances are called buffering substances (Sönmez, 2002). There are several buffer systems to clear hydrogen ions and, in turn, lactic acid concentrating in the body which enables one to continue exercise at the same intensity level (CicioÄŸlu and Onay, 2002; Fox et al., 1988).
The biggest buffering capacity is provided by HCO3/CO2 system in the blood and extracellular fluid. Bicarbonate ion is an effective natural buffer which prevents damage to intracellular and extracellular as well as blood and skeleton muscle acid-base equilibrium. Ergogenic supplements are substances used generally for improving sports performance and are expressed as techniques. In theory, the use of sodium bicarbonate improves buffering capacity of the body by absorbing hydrogen ions (CicioÄŸlu and Onay, 2002). But,the studies that examined the effect of sodium bicarbonate supplementation on sport performance were contradictory (Matson and Tran, 1993). While some studies have stated significant performance enhancement after the sodium bicarbonate ingestion (McNaughton et al., 1999; Verbitsky et al., 1997; Wilkes et al., 1983;Jones et al., 1977), others report no effect on exercise performance (Ball et al., 1996, Brien and McKenzie, 1989, Potteiger et al., 1996).
These discrepancies may explain duration and intensity of exercise, the dosage and duration of sodium bicarbonate implemented and the time delay between implementation (Jourkeshet et al., 2011). Therefore, the purpose of this study was to investigate the effects of sodium bicarbonate ingestion on blood lactate and heart rate responses during running velocity at maximal lactate steady state.
Study group
Thirty (30) female futsal players

playing sports actively for minimum 4 years volunteered to participate in this investigation. Participants were randomly assigned to two equal groups of experimental group and control group.Two hours before the experiment, experimental group was ingested sodium bicarbonate (NaHCO
3) supplementation (0.3 g/kg body mass) with an amount of water, while sodium chloride (NaCl) was received the placebo groups (PG) into the same amounts. Measurements were made at the end of team’s preparation training period. All measurements were done in the morning (between 9 and 12 am).
Measurement tools
Height measurements
Height measurements of the athletes were measured by using a wall-mounted stadiometer (Holtain Ltd. U.K.) at anatomic standing structure, barefoot, head at frontal plane position to the nearest 1 mm.
Body mass measurements
Body mass measurements of athletes were measured using digital weighing scale (Tanita TBF 401 A Japan) in standard sportswear (shorts and t-shirts) to the nearest 0.1 kg.
Heart rate measurements
Heart rate values of the athletes were measured continuously beat by beat during exercise and recovery using a Polar RS800CX heart rate monitor (Polar Electro Oy, Kempele, Finland).
Blood lactate measurements
Pre-exercise and immediately after each exercise stage, capillary blood samples from the fingertip were measured with the use of Eco Twenty Care Diagnostica lactate analyzer. Firstly, fingertip was pricked by lancet and 20 µl of blood samples was placed into capillary tubes. Afterwards, capillary samples were collected into the 2.0 ml plastic solution tube that included a lysing stabilizing agent for the measurement process. 2.0 ml of plastic solution tubes were shaken by hand and placed into removable sample trays on lactate analyzer. Before blood analysis, the blood lactate analyzer was calibrated with 12 mmol.l-1 standard solution provided by the manufacturer.
Data collection
Athletes involved in this study were asked not to take any ergogenic substance or any drug in the last two weeks and not to make any physical activity in the last 24 h before the measurements. Athletes to have had an inflammatory disease or any disability were excluded from the study. Before the study, each athlete signed an informed consent form including detailed information on study, possible risks and disturbances. Measurements were made in the following order.
Detection of physical properties
Firstly, athletes were informed about the test procedures. Physical properties of the athletes (age, height and body mass) were measured and recorded in measurement form.
Preparations prior to the treadmill protocol
The gradual preparations made before the treadmill protocol are as follows:
1. In the first preparation stage for the treadmill protocol: in order to monitor the signals transmitted by the heart rate monitors, the monitors were fixed around the chests of the athletes using elastic straps and polar watches were given to the athletes to wear on their wrists. Resting heart rate was obtained with the subjects lying supine after 15 min of rest.
2. In the second stage: blood samples were collected from capillaries to detect resting blood lactate values of the athletes. To this end, fingertips of the athletes were pricked by a lancet and the obtained blood samples were filled in 20 µl capillary tubes. Capillary blood samples were collected into the 2.0 ml plastic solution tube that included a lysing stabilizing agent. To determine resting blood lactate values, the plastic solution tubes were placed into removable sample trays on Eco Twenty Care Diagnostica lactate analyzer.
Treadmill protocols
Two different test protocols were administered to the athletes. Firstly, running speeds of the athletes corresponding to 4 mmol.l-1 lactate threshold were determined. For this, athletes were subjected to incremental intermittent treadmill test starting at the speed of 7 km/h-1 which is increased by 1 km/h-1 at every 3 min stage until volitional exhaustion21. Fingertip capillary blood samples were taken within 30 s. Running speeds corresponding to fixed blood lactate concentrations of 4.0 mmol.l-1 were calculated using linear interpolation. Tests were conducted on the treadmill (Star Trac, U.S.A) at 1% inclination. At the second stage, athletes were performed 30 minutes constant-speed run at running speed corresponding to 4 mmol.l-1 blood lactate for the determination of the maximal lactate steady state. Blood samples were collected from fingertips of the athletes while resting and following each 10 minute of exercise. The maximal lactate steady state was defined as the running speed that produced no more than a 1.0 mmol.l-1 increase in blood lactate between 10 and 30 min of exercise (Billat et al., 2003). In case of a lactate difference below 1 mmol.l-1 between the 10th and 30th min of the exercise, athletes were required to complete another constant-speed run at a speed that was 1 km.h-1 faster than the running speed at 4 mmol.l-1 lactate threshold 48 h later. Similarly, in cases of blood lactate difference above 1 mmol.l-1, 1 km.h-1 speed less was applied.
Statistical analysis
Paired Samples T test was used to determine whether there are significant blood lactate and heart rate differences in before and after the sodium bicarbonate ingestion. Measurements were statistically analyzed using SPSS 17.0 for Windows and statistical significance was set at P<0.05.
Physical characteristics of the female futsal players
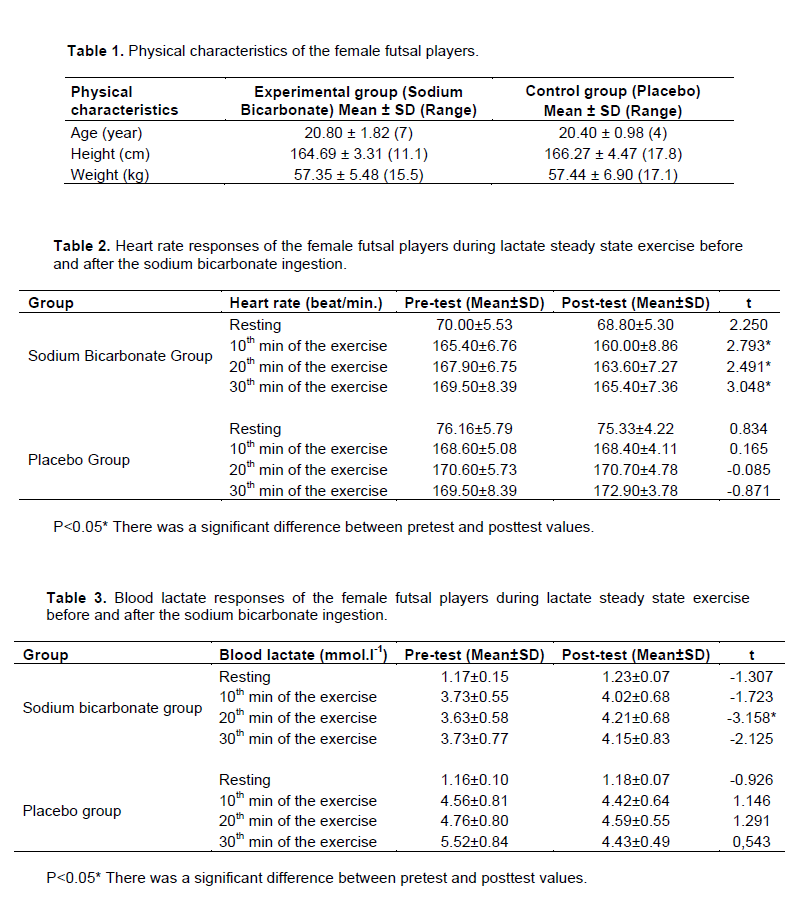
Physical characteristics of the female futsal players are presented in Table 1. The mean age, height and weight of the experimental group (NaHCO3) athletes were 20.80 years, 164.69 cm. and 57.35 kg respectively, while mean age, height and weight of placebo group (NaCl) were 20.40 years, 166.27 cm and 57.44 kg., respectively.
Heart rate values of the female futsal players during lactate steady state exercise before and after sodium bicarbonate ingestion
Heart rate responses given by the participant athletes during lactate steady state exercise before and after the sodium bicarbonate ingestion are presented in Table 2. Test results show a significant decrease in the post-supplement heart rate responses given by the bicarbonate group at the 10th, 20th and 30th min of the exercise (p<0.05), but no significant difference was observed in the control group in terms of the pre-test and post-test values of any variable (p>0.05).
Blood lactate values of the female futsal players during lactate steady state exercise before and after bicarbonate ingestion
Blood lactate responses given by the participant athletes during lactate steady state exercise before and after sodium bicarbonate ingestion is presented in Table 3. According to test results, although a numerical increase was recorded in the lactate responses of the experimental group, a significant difference in the lactate responses of the same group after supplement was detected only at the 20th min of the exercise (p<0.05). On the other hand, no significant difference was recorded in the control group in terms of pre-test and post-test values of any variable (p>0.05).
The present study examined the effects of sodium bicarbonate ingestion on the lactate steady state responses of female futsal players during a treadmill test. There was a significant decrease in the post-bicarbonate heart rate responses at the 10th, 20th and 30th min of the lactate steady state exercise. Although an increase in the lactate responses of the experimental group was observed, the only significant increase was recorded at the 20th min of the exercise after the sodium bicarbonate ingestion.
The point where blood lactate begins to accumulate reflects transition from aerobic to anaerobic metabolism due to a change in the use of energy pathways (Anderson and Rhodes, 1991). This point appears to represent a critical intensity above which endurance performance is severely limited (Rhodes and McKenzie, 1984) and transition between aerobic and anaerobic metabolism (Anderson and Rhodes, 1991). Lactic acid production and the dissociation into hydrogen ions (H+) and lactate increases with enhanced glycolytic metabolism (Campos et al., 2012; Midgley et al., 2007; Kowalchuk et al., 1984), leading to a decrease in muscle and blood pH (Mero et al., 2004; Medbo and Sejersted, 1985), impairing energy production, and inhibiting the contractile function by interfering with calcium release from the endoplasmic reticulum (Donaldson and Hermansen, 1978; Fabiato and Fabiato, 1978). Consequently, deterioration in athletic performance occurs following the increase in hydrogen ion concentration (George and MacLaren, 1988).
The bicarbonate ion (HCO3) is an effective intracellular buffer, and the efflux of H+ ions from cells is accelerated by augmenting the extracellular buffer (McNaughton, 1992). It has been suggested that bicarbonate stores in the blood and the buffering capacity is increased by sodium bicarbonate supplementation (Jourkeshet et al., 2011). Zajac et al. (2009) stated that acid-base balance and lactate concentration can be affected significantly by the intake of sodium bicarbonate. An increase in extracellular bicarbonate can cause higher efflux of lactate output from skeletal muscle by the mono-carboxylate co-transporter, a symport carrier of lactate and H+ (Wu et al., 2010; Nielsen et al., 2002). As a result, blood lactate concentration is significantly increased after sodium bicarbonate ingestion (Wue et al., 2010). This is consistent with the observed increase in lactate during lactate steady state exercise following sodium bicarbonate ingestion.
Sodium bicarbonate may be an effective intervention to decrease heart rate responses during endurance exercise. Mueller et al. (2013) explained that plasma osmolality of blood increases with sodium bicarbonate supplementation, counteracted by an expansion in plasma volume, and thereby a decrease in heart rate.Effects of sodium bicarbonate supplementation on exercise performance have been contradictory. Some studies have reported an ergogenic effect (Mueller et al., 2013; Jourkesh et al., 2011; Wu et al., 2010; Mero et al., 2004; George and Maclaren, 1988; MacLaren and Mellor 1985; Wilkes et al., 1983; Sutton et al., 1981; Jones et al., 1977), but other studies have reported that bicarbonate does not affect exercise performance (Horswillet et al., 1988; Kindermann et al., 1977; Poulus et al., 1974; Margaria et al., 1971). Discrepancies may have been caused by the intensity and duration of the exercise tests, the dosage and duration of sodium bicarbonate administered, and the time delay between administration and the beginning of the exercise test (Jourkesh et al., 2011).
In conclusion, blood lactate levels and heart rate are an important indicator of endurance capacity. Endurance capacity is expressed by lower heart rate and muscle lactate levels. After the sodium bicarbonate ingestion, we found an important change in the heart rate and blood lactate values during the lactate steady state test. Reduction of heart rate and occurring changes in lactate levels may contribute to change of the individual endurance performance.
The authors have not declared any conflict of interests.
REFERENCES
|
Abbiss CR, Laursen PB (2005). Models to explain fatigue during prolonged endurance cycling. Sports Med. 35(10):865-898.
Crossref
|
|
|
|
Anderson GS, Rhodes EC (1991). Relationship between blood lactate and excess CO2 in elite cyclists. J. Sports Sci. 9:173-181.
Crossref
|
|
|
|
|
Ball D, Greenhaff PL, Maughan RJ (1996). The acute reversal of a diet-induced metabolic acidosis does not restore endurance capacity during high-intensity exercise in man. Eur. J. Appl. Physiol. 73:105-112.
Crossref
|
|
|
|
|
Barbero-Alvarez JC, Soto VM, Barbero-Alvarez V, Granda-Vera J (2008). Match analysis and heart rate of futsal players during competition. J. Sports Sci. 26(1):63-73.
Crossref
|
|
|
|
|
Berdejo-del-Fresno D (2012). Fitness Seasonal Changes in a First Division English Futsal Team. Afr. J. Basic Appl. Sci. 4(2):49-54.
|
|
|
|
|
Billat VL, Sirvent P, Py G, Koralsztein JP, Mercier J (2003). The concept of maximal lactate steady state. Sports Med. 33:407-426.
Crossref
|
|
|
|
|
Bogdanis GC, Nevilla ME, Lakomya HKA (1994). Effects of previous dynamic arm exercise on power output during repeated maximal sprint cycling. J. Sports Sci. 12(4):363-370.
Crossref
|
|
|
|
|
Brien DM, McKenzie DC (1989). The effect of induced alkalosis and acidosis on plasma lactate and work output in elite oarsmen. Eur. J. Appl. Physiol. 58:797-802.
Crossref
|
|
|
|
|
ÇaÄŸlayan HS, Mehtap B (2010). The Investıgatıon Of Epıstemologıcal Belıefs Of Female Unıversıty Futsal Team Players In Terms Of Some Varıables. Nigde University J. Phys. Educ. Sport Sci. 4:1.
|
|
|
|
|
Campos EZ, Sangali EB, Gerosa NJ, Gobbi RB, Freitas JIF, Papoti M (2012). Effects of Sodium Bicarbonate Ingestion during an Intermittent Exercise on Blood Lactate, Stroke Parameters, and Performance of Swimmers. J. Exercise Physiol. 15(6):84-92.
|
|
|
|
|
CicioÄŸlu Ä°, Onay M (2002). The Effects Of High Intensity Exercise on Blood Gases and Some Blood Parameters Related with Glucose Consumption. J. Phys. Educ. Sport Sci. 4:3.
|
|
|
|
|
Connett RJ, Gayeski TEJ, Honig GR (1984). Lactate accumulation in fully aerobic, working dog gracilis muscle. Am. J. Physiol. 246:120-128.
|
|
|
|
|
Donaldson SKB, Hermansen L (1978). Differential direct effects of H+ and Ca2+-activated force of skinned fibres from the soleus, cardiac, adductor magnus muscle of rabbits. Eur. J. Physiol. 376: 55-65.
Crossref
|
|
|
|
|
Fabiato A, Fabiato F (1978). Effects of pH on the myofilaments and the sarcoplasmic reticulum of skinned cells from cardiac and skeletal muscles. J. Physiol. 276:233-255.
Crossref
|
|
|
|
|
Fox EL, Bowers RW, Foss ML (1988). The Physiological Basis of Physical Education and Athletics, 4th Ed., Sounders College Publishing. New York.
|
|
|
|
|
George KP, Maclaren DPM (1988). The effect of induced alkalosis and acidosis on endurance running at an intensity corresponding to 4 mM blood lactate. Ergonomic 31(11):1639-1645.
Crossref
|
|
|
|
|
Horswill CA, Costill DL, Fink WJ, Flynn M, Kirwan J, Mitchell J, Houmard J (1988). Influence of sodium bicarbonate on sprint performance: Relationship to dosage. Med. Sci. Sports Exerc. 20:566-569.
Crossref
|
|
|
|
|
Jones MB (2010). Basic Interpretation of Metabolic Acidosis. Crit. Care Nurse 30:63-69.
Crossref
|
|
|
|
|
Jones NL, Sutton JR, Taylor R, Toews CJ (1977). Effect of pH on cardiorespiratory and metabolic responses to exercise. J. Appl. Physiol. 43: 959-964.
|
|
|
|
|
Jourkesh M, Ahmaidi S, Keikha BM, Sadri I, Ojagi A (2011). Effects of six weeks sodium bicarbonate supplementation and high-intensity interval training on endurance performance and body composition. Ann. Biol. Res. 2(2):403-413.
|
|
|
|
|
Juel C (1998). Skeletal muscle Na+/H+ exchange in rats: Ph dependency and the effect of training. Acta Physiologica Scandinavica 164:135-140.
Crossref
|
|
|
|
|
Kindermann W, Keul J, Huber G (1977). Physical exercise after induced alkalosis (bicarbonate or Tris-buffer). Eur. J. Appl. Physiol. 29:215-223.
Crossref
|
|
|
|
|
Kowalchuk JM, Heigenhauser GJF, Jones NL (1984). Effect of ph on metabolic and cardiorespiratory responses during progressive exercise. J. Appl. Physiol. 57:1558-1563.
|
|
|
|
|
Lindinger, MI, Horn PL, Grudzien SP (1999). Exercise-induced stimulation of K+ transport in human erythrocytes. J. Appl. Physiol. 87:2157-2167.
|
|
|
|
|
Maclaren D, Mellors S, (1985). The Effect of induced alkalosis and acidosis on the lactate threshold and performance at 95% VO2 max. Brit. J. Sports Med. 19:237.
|
|
|
|
|
Margaria R, Aghemo P Sassi G (1971). Effects of alkalosis on performance and lactate formation in supramaximal exercise. Internationale Zeitschrift für Angewandte Physiologie. 29:215-223.
Crossref
|
|
|
|
|
Margaria R, Cerretelli P, Mangili F (1963). Balance and kinetics of anaerobic energy release during strenuous exercise in man. J. Appl. Physiol. 19: 623-628.
|
|
|
|
|
Matson LG, Tran ZV (1993). Effects of sodium bicarbonate ingestion on anaerobic performance: A meta-analytic review. Int. J. Sport Nutr. 3:2-28.
|
|
|
|
|
McNaughton L, Backx K, Palmer G, Strange N (1999). Effects of chronic bicarbonate ingestion on the performance of high-intensity work. Eur. J. Appl. Physiol. 80:333-336.
Crossref
|
|
|
|
|
Mcnaughton LR (1992). Bicarbonate ingestion: Effects of dosage on 60 s cycle ergometry. J. Sports Sci. 10:415-423.
Crossref
|
|
|
|
|
Medbo JI, Sejersted OM (1985). Acid base and electrolyte balance after exhausting exercise in endurance and sprint trained subjects. Acta Physiologica Scandinavica 125:97-109.
Crossref
|
|
|
|
|
Mero AA, Keskinen KL, Malvela MT, Sallinen JM (2004). Combined creatine and sodium bicarbonate supplementation enhances interval swimming. J. Strength Condition. Res. 18(2):306-310.
Crossref
|
|
|
|
|
Midgley AW, McNaughton LR, Carrol S (2007). Physiological determinants of time to exhaustion during intermittent treadmill running at vVO2max. Int. J. Sports Med. 28(4):273-280.
Crossref
|
|
|
|
|
Moxnes JF, Sandbakk Ø (2012). The kinetics of lactate production and removal during whole-body exercise. Theor. Biol. Med. Model. 9(7):1-14.
Crossref
|
|
|
|
|
Mueller SM, Gehrig SM, Frese S, Wagner CA, Boutellier U, Toigo M (2013). Multiday acute sodium bicarbonate intake improves endurance capacity and reduces acidosis in men. J. Int. Soc. Sports Nutr. 10(16):2-9.
Crossref
|
|
|
|
|
Myers J, Ashley E (1997). Dangerous Curves: A perspective on Exercise, lactate and the anaerobic threshold. Chest J. 111:787-795.
Crossref
|
|
|
|
|
Nielsen HB, Bredmose PP, Stromstad M, Volianitis S, Quistorff B, Secher NH (2002). Bicarbonate attenuates arterial desaturation during maximal exercise in humans. J. Appl. Physiol. 93(7):24-31.
Crossref
|
|
|
|
|
Potteiger JA, Webster MJ, Nickel GL, Haub MD, Palmer RJ (1996). The effects of buffer ingestion on metabolic factors related to distance running performance. Eur. J. Appl. Physiol. 72:365-371.
Crossref
|
|
|
|
|
Poulus AJ, Doctor HJ. Westra HG (1974). Acid-base balance and subjective feelings of fatigue during physical exercise. Eur. J. Appl. Physiol. Occup. Physiol. 33:207-213.
Crossref
|
|
|
|
|
Putman CT, Jones NL, Heigenhauser GJF (2003). Effects of short-term training on plasma acid–base balance during incremental exercise in man. J. Physiol. 550(2):585-603.
Crossref
|
|
|
|
|
Rhodes EC, McKenzie DC (1984). Predicting marathon time from anaerobic threshold measurements. Phys. Sports Med. 12:95-98.
|
|
|
|
|
Sönmez GT (2002). Egzersiz ve Spor Fizyolojisi, Birlik Matbaacılık, Ankara.
|
|
|
|
|
Stanley WC, Gertz EW, Wisneski JA, Morris DL, Neese RA, Brooks GA (1988). Lactate kinetics during submaximal exercise in humans: Studies with isotopic tracers. J. Cardiopulmonary Rehabil. 9:331-340.
Crossref
|
|
|
|
|
Sutton JR, Jones NL, Peters EJ, Schmidt EF, Wolfe RR (1981). Effect of pH on muscle glycolysis during exercise. Clin. Sci. 61:331-338.
Crossref
|
|
|
|
|
Verbitsky O, Mizrahi J, Levin M, Isakov E (1997). Effect of ingested sodium bicarbonate on muscle force, fatigue, and recovery. J. Appl. Physiol. 83:333-337.
|
|
|
|
|
Wilkes D, Gledhill N, Smyth, R (1983). Effect of acute induced metabolic alkalosis on 800 m racing time. Med. Sci. Sports Exerc. 15:277-280.
Crossref
|
|
|
|
|
Wu C, Shih M, Yang C, Huang M, Chang C (2010). Sodium bicarbonate supplementation prevents skilled tennis performance decline after a simulated match. J. Int. Soc. Sports Nutr. 7(33):2-8.
Crossref
|
|
|
|
|
Zajac A, Cholewa J, Poprzecki S, Waskiewicz Z, Langfort J (2009). Effects of sodium bicarbonate ingestion on swim performance in youth athletes. J. Sports Sci. Med. 8(1):45-50.
|
|