Full Length Research Paper
ABSTRACT
Poor compliance with standard radiation protection procedures induces risk to the safety and the health of the population and the medical staff. This study aims to assess compliance with standard radiation protection processes in medical imaging (MI) units in the Atlantique and Littoral departments of Benin in 2019. This was a cross-sectional, descriptive, evaluative study led from March to April 2019 in the functional MI divisions of hospitals in the Atlantique and Littoral departments. Imaging technicians or handlers were included for convenience and the managers of medical imaging units by reasoned choice. The compliance with standard radiation protection processes in MI units (main component) was assessed by assigning an overall score resulting from the appreciation of the sub-components (radiation protection means, radiation protection processes, the working environment, and the knowledge of the staff). There were 89 respondents in 18 MI units included in the study. The mean age of the staff was 36.5 ± 9.5 years, with a male domination of 56.34%. Compliance with standard radiation protection processes was low, with an overall score of 41.41%, mainly due to a weakness in the sub-components "Radiation protection means", "Radiation protection processes", "Working environment" and "Handler knowledge", which scores were of 33.01, 44.24 and 11.67%, respectively. Only the sub-component related to technicians was medium, with a score of 60.50%. The implementation of radiation protection measures in the medical imaging units of the Atlantique and Littoral departments in Benin is insufficient. The establishment of a regulatory and nuclear safety authority could help to meet the challenge of radiation protection in Benin's imaging units.
Key words: Evaluation, standard processes, radiation protection, Benin.
INTRODUCTION
Radiation protection is the set of means used to protect people exposed to ionizing radiation. It provides a baseline for the protection of the population and the environment without unduly limiting beneficial practices leading to radiation exposure (Collection of IRSN scientific books, 2007). All these means allow the detection of certain major risks for which action is possible through dose limitation.
Poor compliance with standard radiation protection processes is the result of a failure to implement all the necessary steps for the application of a standard. Ionizing radiation is a form of energy released by atoms and propagated by electromagnetic waves or particles. We have two types of sources: Natural sources such as cosmic rays and artificial sources such as X-rays. As the uses of ionizing radiation increase, so do the potential health hazards if not properly used or contained (World Health Organization, 2019). Leukemias, connective tissue sarcomas and thyroid cancers are all conditions that may result from the misuse of x-rays (Collection of IRSN Scientific Books, 2007; Claude, 2002). These effects become more severe as the dose and dose rate increase. For example, the threshold dose for the development of acute radiation syndrome is about 1000 mSv. Also prenatal exposure to ionizing radiation can induce brain damage in the fetus when an acute dose of more than 100 mSv is received between 8 and 15 weeks of gestation (Collection of IRSN scientific books, 2007).
Every year worldwide, more than 3.6 billion diagnostic radiology examinations are performed, 37 million nuclear medicine procedures are performed and 7.5 million radiotherapy treatments are administered (World Health Organization, 2019). The International Labor Office in its guidelines on radiation protection states that the application of good radiation protection practices is an important aspect of reducing worker exposure and therefore represents a major step towards achieving optimal radiation protection (Shengli, 2011). According to a 2008 report by the United Nations Scientific Committee on the Effects of Atomic Radiation, some 23 million workers worldwide are exposed to ionizing radiation, 75% of them in the medical field (World Health Organization, 2019). This exposure is mainly due to the normal use of equipment, but these workers can sometimes be overexposed in the event of an accident. Concrete measures can be taken to protect them, including regular monitoring, protective equipment, or precautions such as shielding. According to the International Atomic Energy Agency, training, information exchange and continuous health surveillance are also important factors in an effective occupational radiation protection regime (International Atomic Energy Agency, 2004).
Each of these responsibilities should be clearly assigned to workers, contractors or employers, or operators of installations. National organizations use these recommendations to create or adopt laws, decrees, and ministerial orders for the application of radiation protection standards in their countries. Article 20 of the Radiation Protection Act in Benin states that any license holder who carries out an activity involving a risk of exposure is required to protect workers against work-related exposures and to observe all rules relating to the protection of workers likely to be exposed to ionizing radiation, in particular with respect to exposure assessment, health surveillance and training (Republic of Benin, 2018).
Elsewhere, especially in Nigeria, even if most of radiologist technician have good knowledge of radioprotection measures, there are inadequate radiation protection and monitoring practices in most of the functional X-ray facilities. There is poor adherence to the advice of the medical physicists due to the cost implications of the implementation (Qutbi et al., 2021; Eze et al., 2011). In Benin, the status of the implementation of radiation protection measures in medical imaging (MI) units is little known, and reports of internal or external monitoring of compliance with standard radiation protection processes are rare. Furthermore, few studies have focused on radiation protection measures in MI units, thus creating a significant gap in data and knowledge that can help decision-making. The objectives of the present study were to take stock of the situation of radiation protection in Benin and to propose solutions that will help to safeguard the health of users of medical imaging services as well as the population in general.
METHODS
Study framework
Benin has twelve departments, including the Atlantique and Littoral departments, which served as the framework for this study. With a total surface area of 3,233 km², and a population of 1 398 229 inhabitants, the Atlantic department stretches over approximately 100 km from the coast to the inland part of the country. It is subdivided into eight (8) municipalities and has three health zones. As for the Littoral department, it covers an area of 79 km², with a population of 679 012 inhabitants, and extends essentially along the coast. It is conflated with its only municipality, which is the city of Cotonou, the economic capital of Benin. As the economic capital of Benin, Cotonou benefits from more infrastructure and split into four health zones.
In this study, we scoured 09 MI units in the Atlantic department and 15 MI units in the Coastal department.
Type and timeframe of the study
This was a cross-sectional, descriptive, evaluative study conducted from 25 March to 19 April 2019 in the functional MI units of the hospitals of the Atlantique and Littoral departments.
Study population and sampling
The study population was made up of all handlers working in MI departments and managers of MI units who gave their free and informed consent to the investigators to participate in the study. All health facilities with a functional MI unit was first identified and then preceded with non-probability sampling, for the convenience of the handlers and by reasoned choice of the MI unit managers. The size of the different samples was obtained after the data collection. 71 handlers and 18 managers of MI departments in the field filled the criteria for inclusion in this study.
Variables
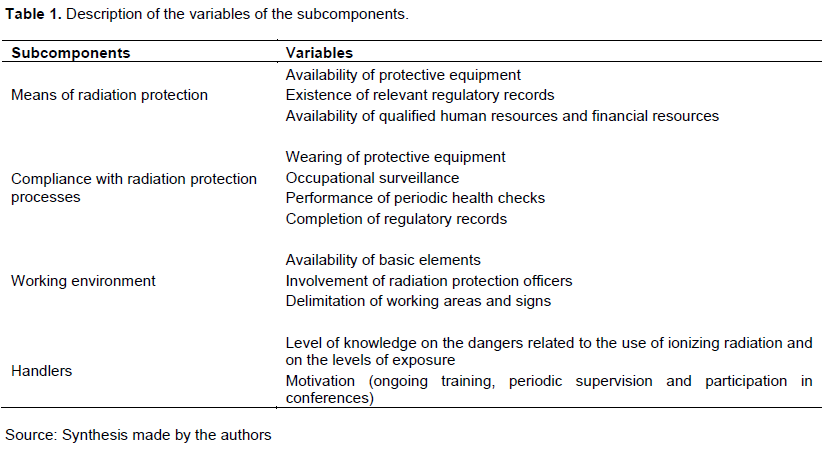
The main component was compliance with standard radiation protection processes in the MI units. There were four sub-components, which considered radiation protection means, radiation protection processes, working environment and worker factors.
The sub-component related to "means of radiation protection" takes into account the availability of protective equipment, the existence of relevant regulatory records, the availability of qualified human resources and financial resources to facilitate activities implementation.
The sub-component related to "compliance with radiation protection processes" takes into account the wearing of protective equipment, occupational surveillance, and the performance of periodic health checks and the completion of regulatory records.
The sub-component related to "working environment" covers the basic elements, the involvement of radiation protection officers and the delimitation of working areas and signs.
As for the sub-component related to the manipulators, it takes into account the level of knowledge of the manipulators on the dangers related to the use of ionizing radiation, and on the levels of exposure as well as their motivation (ongoing training, periodic supervision and participation in conferences) (Table 1).
The operational aspect of the assessment of compliance with standard procedures in the services was carried out on the basis of the percentages of scores obtained by the different sub-components. A ranking was followed. The main component, compliance with standard radiation protection processes, was composed of sub-components, each containing elements. These items had variables.
Each of these variables had one or more criteria.
The criteria were each given a dichotomous score, that is: Yes =1 if the criterion was present and No=0 if the criterion was absent (Bernoulli law).
The rating of each sub-component was based on the sums of the scores of the variables contained in these sub-components calculated beforehand. The score obtained was expressed as a percentage of the expected score, allowing each sub-component to be assessed in three ways: Good, average and poor, using the three-scale analysis adapted to the Varkevisser model (Varkevisser et al., 1993). Thus, the assessment of the sub-components was divided as follows:
1. Score ≥ 80%: the assessment is "good";
2. Score between 60 and 80%: the assessment is "medium";
3. Score < 60%: the assessment is "poor".
Data processing and analysis
A survey by direct interview was carried out using an interview guide to collect data from the directors of the health facilities visited. A questionnaire survey to gather information from the technicians and a direct observation using an observation grid to collect information on the completion of the examinations and compliance with the standard norms and processes in the area of radioprotection was undertaken. Collected data were entered and analyzed using EPI INFO software version 7 and Excel 2010 after checking for completeness and consistency. Proportions were calculated for qualitative variables; the mean and standard deviation for quantitative variables with a normal distribution. Medians and extremes (minimum and maximum) were determined for quantitative variables with a skewed distribution. Data analysis was done by specific objective and summarized in prose, tables or figures. The assessment of compliance with standard radiation protection processes in MI units was done by assigning an overall score resulting from the assessment of the sub-components, namely those related to the working environment, radiation protection resources, radiation protection processes and manipulators.
Ethical and deontology concerns
The research is essentially observational and evaluative in nature, and falls within the framework of epidemiological study. It was carried out in compliance with ethical and professional rules. The authorization of each hospital director was obtained before starting data collection. The objectives of the survey were clearly explained to the participants and the different tools were only filled in after obtaining their free and informed consent. Participation in this study was strictly voluntary. According to Law No. 2010-40 of 8 December 2010 on the code of ethics and deontology for health research in the Republic of Benin, ethical approval is not required to conduct an epidemiological study. The study was carried out in accordance with articles 20 and 21 of this law in compliance with the principles of the Helsinki declaration.
RESULTS
Socio-demographic profiles of respondents
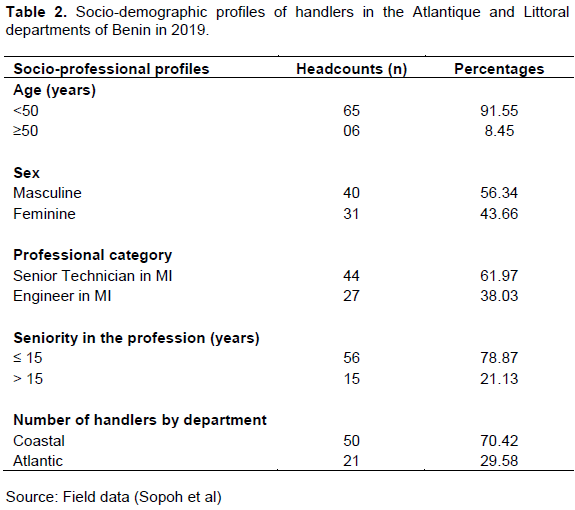
A total of 18 MI units were included in the study in the Atlantique and Littoral departments. In these different units, 89 people were surveyed, including 71 handlers and 18 managers of these facilities. The average age of the handlers was 36.5 ± 9.5 years. There was a male predominance of 56.34% (40/71) with a sex ratio (M/F) of 1.29. In 61.97% (44/71) of cases, the manipulators were MI technicians. Most (70.42% (50/71)) of the handlers came from the Coastal departments (Table 2).
Sub-component related to the means of radiation protection, the compliance with procedures, the working environment and handlers”
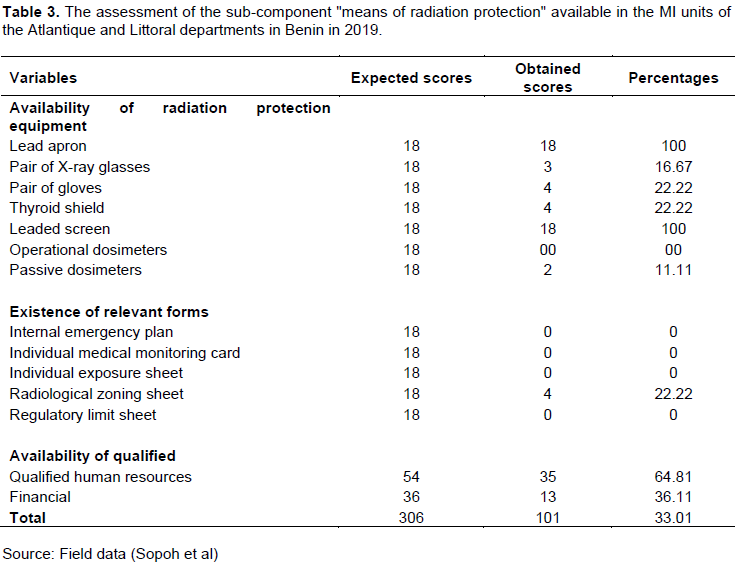
At the end of the evaluation of this sub-component, a score of 101, that is a proportion of 33.01% (101/306) was obtained. The means of radiation protection available in the medical imaging units were insufficient (< 60%). Apart from the leaded aprons and windscreens, there was little availability of radiation protection equipment and no relevant forms (Table 3).
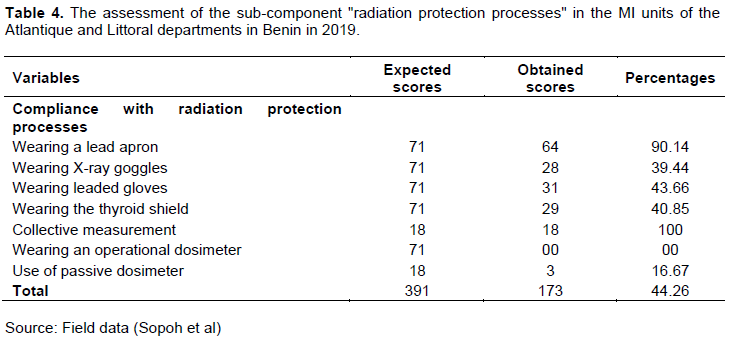
When assessing compliance with radiation protection procedures in the MI units, a score of 173, representing 44.24% (173/391) of the total expected score was obtained. Compliance with radiation protection processes in the MI units was insufficient (< 60%). The main findings were the absence of an operational dosimeter and the poor use of passive dosimeters (16.67%) (Table 4).
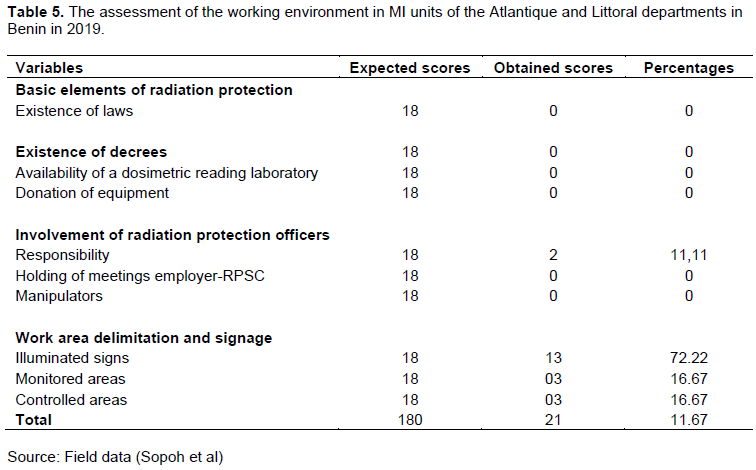
By the end of the assessment of the working environment, a score of 21, which is 11.67% (21/180) of the total expected score was obtained. This score was therefore insufficient (< 60%). There was a lack of basic elements of radiation protection (laws, decrees and regulations) and a low involvement of radiation protection officers in the design and implementation of radiation protection procedures (Table 5).
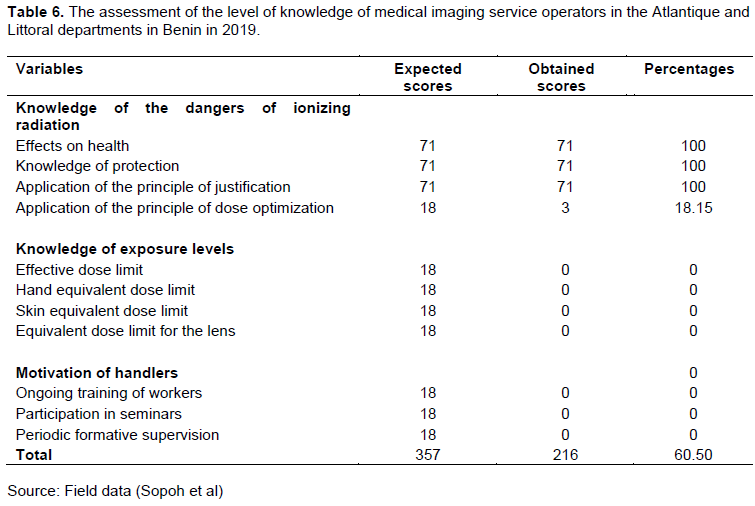
At the end of the evaluation of this sub-component, a score of 216 accounting for 60.50% (216/357) of the total expected score was obtained. The handlers therefore have an average knowledge (score between 60 and 80%). They had a good knowledge of the dangers of ionizing radiation, but no awareness of exposure levels and no incentive factors (Table 6).
Compliance with radiation protection standard processes
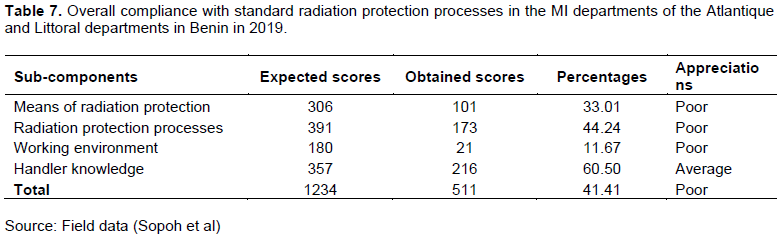
The overall score for compliance with radiation safety standard procedures was 511, which is 41.41% (511/1234) of the expected total score, therefore insufficient (< 60%), mainly due to a weakness in the sub-components "Radiation protection means", "Radiation protection procedures", "Working environment" and "Handler knowledge", which had scores of 33.01, 44.24 and 11.67% respectively. Only the sub-component related to handlers was average, with a score of 60.50% (Table 7).
DISCUSSION
This study allowed us to understand that compliance with standard radiation protection processes in the medical imaging units of the Atlantique and Littoral departments in Benin was insufficient (41.41%). The same is true for the ratings of the different sub-components such as radiation protection means (33.01%); radiation protection processes (44.24%); work environment (11.67%) except for the sub-component related to the handlers where the rating was average (60.50%). Among the means of radiation protection, leaded aprons were the most available personal protective equipment. This situation could be explained by the low commitment of the facility managers to protect the handlers under their responsibility and the lack of sufficient information on the set of personal protective equipment that should be used during special examinations. These results have also been found by other studies such as the one carried out in Cameroon by Néossi and al, which notes that the centers surveyed had at least one leaded apron, a pair of leaded gloves and one leaded screen per examination room. They have also found that leaded goggles did not exist in any of the centers and that only one center had a thyroid cover (Guena et al., 2018). Others studies, reported by Muhogora and Rehani, had reported insufficiencies in radioprotection measures in Africa. Indeed, conventional radiography is still being used in a large part of Africa. Even if the basic radiation protection practices such as wearing a lead apron and a personnel dosimeter, are routine in many countries, there still need to enhance the routine use of either lead glass eyewear or a lead protective screen (Moussa and Kamoun, 2015).
This assessment also showed that no MI unit has operational dosimeters for individual dose collection. Only 02 units have passive dosimeters for collective dose measurement. Moussa and Kamoun led a study on workers' knowledge of radiation protection at the CHU Mongi Slim in La Marsa in Tunisia. They reported that the wearing of dosimeters was not respected by 70% of the staff due to the non-existence of this work equipment (Muhogora and Rehani, 2017). The absence of an individual dosimeter is a failure due to the absence of a radiation safety authority or control body. It is also due to a lack of subsidies or donations from organizations such as the International Atomic Energy Agency (IAEA), the World Health Organization (WHO), and the International Labor Organization (ILO); given the high cost of these devices. Improving the availability of dosimeters in MI units is a key aspect of ensuring compliance with standard processes.
In their study on "Compliance with the rules of radiation protection in conventional radiology in SEGMA hospitals in the Marrakech Tensift Al Haouz region" conducted in Morocco in 2013, Jaouad and Essolbi (2013) found that most (74.30%) of the handlers were qualified agents. These results are similar to the findings in this study (100% qualified agents). The high prevalence of qualified staff in this study could be explained by the existence and implementation of bylaws defining the practice conditions of medical and paramedical occupations in Benin.
Furthermore, the majority of the RCPs available in the MI units were unqualified agents, who had not received any basic training, but who were just appointed by the directors of the establishment from among the handlers to play this role. This is a hindrance to the monitoring of the exposure of professionals. In fact, Beninese regulations stipulate that the employer is required to appoint a competent person in radiation protection, with the necessary training in the functioning of equipment, the use of sources and the dangers associated with ionizing radiation (Republic of Benin, Ministry of Health (2013)). However, there are no qualified establishments that train RCPs, nor are there any training plans for operators who wish to improve their radiation protection skills. The availability of a budget line for radiation protection is also important to ensure the purchase of equipment in real time.
The results of this investigation showed that only the leaded aprons that were most available were worn by the handlers when performing special examinations. A similar finding was made by Kouassi (2005) in their study of compliance with radiation protection rules in hospitals in Abidjan. They found that the majority of workers (97.5%) protected themselves with a lead apron.
The absence of occupational physicians is an obstacle to good compliance with standard radiation protection processes. Their presence does not guarantee compliance if a dosimetric reading laboratory is not set up. Without the results of the monitoring of the occupational exposure of radiation workers by the PCRs, the latter will not be able to carry out the periodic health check-ups intended for radiation workers. These findings are in line with those of Amvene and al through the study conducted on compliance with radiation protection rules in the Imaging Departments of Hospitals in the Far North of Cameroon. They found that none of the handlers had benefited from the services of an occupational physician (Amvene et al., 2017).
The laws and decrees concerning the measures to be taken for the radiation protection of handlers are materials which should be disseminated in the MI units and which allow access to the information for the facility managers (Republic of Benin, Ministry of Labor and Public Service, 2018). However, no law or decree has been disseminated in the MI departments. This fosters the ignorance of facility directors in their responsibility for radiation protection of the handlers and the absence of meetings with the PCRs; to learn about the malfunctions in the MI units.
Ongoing training is a process that ensures the necessary increase in skills to master the use of more sophisticated equipment and to adapt to the requirements of the ever-changing environment. It is the employer's responsibility. The results of this evaluation showed that the continuous training of the handlers is very insufficient, as none of them benefited from it. All the handlers expressed the need for further training and participation in seminars and conferences to improve their skills. Néossi et al. through the study carried out in Cameroon also found that ongoing training of staff in radiation protection is only effective for 30.43% of staff (Guena et al., 2018), Ongolo in Cameroon found that 79.50% of staff have never had ongoing training (Ongolo et al., 2012), due to the inaccessibility to ongoing training. Also in Cameroon, Moifo et al. (2017) showed that most doctors were not aware of the risks of ionizing radiation and were not trained in routine imaging procedures and reference guidelines in clinical imaging, leading to requests for unwarranted imagery (Moifo et al., 2017).
CONCLUSION
There are shortcomings in the implementation of radiation protection measures in the medical imaging units of the Atlantique and Littoral departments in Benin. The establishment of a regulatory and nuclear safety authority and the reinforcement of these structures with medical-technical equipment could help to meet the challenge of radiation protection in Benin's imaging departments.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Amvene JM, Djonyang B, Amougou JM, Ngaroua D, Amvene SN (2017). Compliance with Radiation Protection Rules in Hospital Imaging Services in the Far North of Cameroon. Health sciences and diseases 18(2):83-87. |
|
|
Claude ZJ (2002). Occupational diseases caused by ionizing radiation. MP-Cfdt-Energy, 27. |
|
|
Collection of IRSN scientific books (2007). ICRP Publication 103: 2007 Recommendations of the International Commission on Radiological Protection. Editions TEC& DOC 11, rue Lavoisier 75008 Paris: Nénot JC, 417 p. Guidelines collection. |
|
|
Eze KC, Nzotta CC, Marchie TT, Okegbunam B, Eze TE (2011). The state of occupational radiation protection and monitoring in public and private X-ray facilities in Edo state, Nigeria. Nigerian Journal of Clinical Practice 14(3):308-310. |
|
|
Guena MN, Nanfack BD, Fotsing JG (2019). Exposure of the Population of Ngaoundere-Cameroon to Ionizing Radiation Related to Medical Diagnosis in 2018. Open Journal of Radiology 9(2):125-138. |
|
|
International Atomic Energy Agency (2004). Assessment of Occupational Exposure Due to External Radiation Sources No. RS-G-1.3 Aiea Safety Guide. Vienna: 106 p safety standards collection |
|
|
Jaouad S, Essolbi A (2013). Study of the observance of radiation protection rules in conventional radiology in Segma hospitals in the Marrakech Tensiftal Haouz region. National School of Public Health, management of health organizations. Memory 97 p |
|
|
Kouassi Y (2005). Study of compliance with radiation protection rules in hospitals in Abidjan Archives des Maladies Professionnelles et de l'Environnement 66(4):369-374. |
|
|
Moifo B, Tene U, Moulion Tapouh JR, Samba NO, Tchemtchoua YJ, Simo A, Fotsin JG (2017). Knowledge on Irradiation, Medical Imaging Prescriptions, and Clinical Imaging Referral Guidelines among Physicians in a Sub-Saharan African Country (Cameroon). Radiology Research and Practice: 7 p. |
|
|
Moussa IM, Kamoun H (2015). Knowledge of radiation protection workers - Survey at CHU Mongi Slim in La Marsa (Tunisia). radiation protection 51(2):123-128. |
|
|
Muhogora W, Rehani MM (2017). Review of the current status of radiation protection in diagnostic radiology in Africa. Journal of Medical Imaging 4(3):031202. |
|
|
Ongolo ZP, P, Nguehouo Mb, Yomi J, Nko'o S (2012). Knowledge of radiation protection: survey of personnel in hospital radiodiagnosis, radiotherapy and nuclear medicine departments in Yaoundé Cameroon; Radiation Protection 48(1):39-49. |
|
|
Qutbi HAS, Taher TMJ, Mahdi SA (2021). Knowledge about risk and protective measures related to diagnostic radiation among medical staff in teaching hospitals (wasit province). Wiad Lek 74(9 p.II):2345-2351. |
|
|
Republic of Benin (2018). Law N°-2017-29 of March 15, 2018, on radiological safety and nuclear security in the Republic of Benin. Presidency of the Republic. |
|
|
Republic of Benin, Ministry of Labor and Public Service (2018). Interministerial Order No. 2018-015/MTFP/MS/DC/SGM/DGT/DSS, setting the procedures for delimiting substation study areas in the case of the use of ionizing agents in the Republic of Benin 13 p. 1EE58BD7F.pdf (abrp.bj) |
|
|
Republic of Benin. Ministry of Health (2013). Profile and function of persons competent in radiation protection. National Service for Medical Imaging and Radiation Protection 29 p. |
|
|
Shengli N (2011). International Labor Office (ILO) Code of Practice. Radiation protection of workers (ionizing radiation). SafeWork Briefing Notes Series, Briefing Note #1, 21 p. |
|
|
Varkevisser CM, Pathmanathan I, Brownlee A (1993). Development and implementation of research programs on health systems. Vol 2, Part 1: Proposal Formulation and Testing. International Development Research Center, IDRC-287f.1: 396 p. ISBN: 0-88936-615-2 |
|
|
World Health Organization (WHO) (2019). Report on Ionizing Radiation, Health Effects and Protective Measures 2016. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


