Full Length Research Paper

ABSTRACT
Cervical cancer screening program based on a single visit approach through visual inspection with acetic acid (VIA) and cryotherapy is scaled up since 2012 in Cote d’Ivoire. To assess factors affecting one-year follow-up visit after cryotherapy, a retrospective cohort analysis was performed among all women tested positive and treated by cryotherapy in cervical cancer units in Abidjan from 2010 to 2014. A logistic regression analysis was used to assess factors affecting one-year follow-up attendance after cryotherapy. A total of 618 women, with median age 35 [interquartile range: (29-45)], including 362 (58.6%) HIV positive women received a cryotherapy. In multivariate analysis, being over 40 years old (aOR=3.5; 95%CI [1.9-6.6]), living with HIV (aOR=3.8; 95%CI [2.3-6.3]), attending a screening facility near district of location (aOR=2.2; 95%CI [1.2-3.3]), or HIV clinics for VIA [aOR=2.3; 95%CI (1.4-3.7)] were associated with one-year follow-up visit after cryotherapy. Close follow-up of patient as implemented in HIV clinics and geographic accessibility of cervical cancer screening units are increasing the one-year follow-up after cryotherapy. Systematic integration of cervical cancer screening into health facilities and sustainable strategies to maintain close contact with women could improve follow-up of women and avoid occurrence of cervical cancer in sub-Saharan Africa.
Key words: Cervical cancer screening, visual inspection, cryotherapy, follow-up.
INTRODUCTION
According to International Agency for Cancer Research (IARC), in 2018, 569,847 new cases of cervical cancer and 311,365 associated deaths were reported in women worldwide (Bray et al., 2018). In Côte d’Ivoire, cervical cancer is the second most common cancer among females with age-standardized (World) incidence rates of 28.6 per 100,000 women. Of the 1,789 women diagnosed in 2018, 1,448 deaths occurred making cervical cancer the leading cause of cancer related death in this country (Bray et al., 2018). This malignancy can be prevented through systematic screening for adult women and HPV immunization for adolescent females prior to sexual initiation (World Health Organization, 2014). To overcome financial and human resources challenges raised during the implementation of screening programs using pap smear, low and middle income countries (LMICs) endorsed visual inspection with acetic acid (VIA) as an alternative screening method, as recommended by the WHO (2013). Following a pilot phase of screening, the VIA-based program scaled up across sub-Saharan African countries (Shiferaw et al., 2016; Blumenthal et al., 2007; Parham et al., 2015; Boni et al., 2019; Ouedraogo et al., 2018).
In Cote d’Ivoire, a VIA based screening program was implemented since 2009 through a pilot project targeting women living with HIV and successfully scale up to women in the general population aged 25 to 55, and across the country in 2012 (Boni et al., 2019). According to the National Cancer Control Program (NCCP), approximately 140 cervical cancer screening units across the country offer screening to women following the single-visit approach (or "See-and-Treat" approach), while regular awareness campaign are conducted by Non-Government Organizations (NGOs) (PNLCa, 2020) . According to country National guidelines, women tested positive with VIA, should benefit from immediate cryotherapy when eligible. Women not eligible for immediate cryotherapy are to be referred to a specialist for Loop Electrosurgical Excision Procedure. A one-year follow-up visit for VIA control, consisting of a new VIA to ensure the healing of the cervical abnormality (proved by a new VIA negative) is mandated for all treated women regardless of HIV status (National Cancer Control Program, 2013).
A recent evaluation of the cervical cancer screening program reported a 23.1% post cryotherapy follow-up visit rate (Boni et al., 2019). However, the reasons and factors associated to this low rate are still poorly documented. The principal aim of this secondary analysis was to explore the correlates of follow-up for women receiving cryotherapy after testing positive for precancerous lesions in Abidjan, Cote d’Ivoire.
MATERIALS AND METHODS
Study design and setting
A retrospective cohort study was conducted based on data collected by the NCCP of Côte d’Ivoire, among women who received cryotherapy in the 27 facilities for cervical cancer screening in the urban area of Abidjan from January 2010 to December 2014.
Data management
This secondary data analysis was performed using the cervical cancer screening program database developed by the NCCP to follow-up cervical cancer screening activities (Boni et al., 2019). Individual data of all VIA positive women treated by cryotherapy were extracted, including demographic characteristics (age, district of location), HIV status (positive, negative, unknown), The type of VIA provider (physician, midwife) and characteristics of facilities where women received VIA and cryotherapy. These health facilities were disaggregated according to the level in the health pyramid (primary level; secondary level and tertiary level), the HIV services delivery (exclusive HIV clinics; integrated health facility; no HIV service offer), and their proximity to the participant house (around or far from the living place of the participant).
Data analysis
Categorical variables were described using frequencies and percentages while continuous variables were described using medians and interquartile range (IQR). Chi-square test and Fisher exact test were used for the comparison of categorical variables. Univariate and multivariate logistic regression were used to assess factors associated with follow-up after cryotherapy. All variables associated with follow-up after cryotherapy with a significance level ≤0.25 in univariate analysis were included in multivariate analysis. All analyzes were performed using STATA V14.0 (StataCorp, College Station, Texas).
Ethics
Administrative clearance was obtained from the Ministry of Health to use the NCCP cervical cancer screening database for this secondary analysis. Given the retrospective nature of these anonymous routinely collected data, a consent weaver was also granted.
RESULTS
Characteristics of women and cervical cancer screening facilities
From 2010 to 2014, 618 women with median age 35 [IQR (29-45)] benefited from a first cryotherapy after VIA positivity. Among them, 362 (58.6%) were HIV positive and 256 (41.4%) HIV negative or unknown status. They were screened VIA positive mainly in HIV clinic for 404 (65.4%), by midwives or nurses (68.0%) and physicians (32.0%). In terms of level in the health pyramid, 96 (15.5%) women attended facilities from primary or secondary level, while 369 (59.7%) and 153 (24.8%) were screened VIA positive in tertiary level facilities and private or NGO sector, respectively. The majority (98.1%) of the treated women were tested in a “see and treat” facility.
Factors associated with one-year follow-up visit after a first cryotherapy
Among the 618 women treated by cryotherapy, 143 (23.1%) attended one of the screening units for a follow-up visit.
Both in bivariable and multivariable analysis, factors significantly associated with an effective follow-up visit one-year after cryotherapy among treated women in Abidjan (Table 1) included: age over 40 [aOR=3.5; 95%CIa (1.9-6.6)]; living with HIV [aOR=3.8; 95%CIa (2.3-6.3)]; attending a screening facility in the district of location [aOR=2.2; 95%CIa (1.2-3.3)]; or HIV services for VIA [aOR=2.3; 95%CI (1.4-3.7)]; in 2013 and 2014 [aOR=6.7; 95%CIa (3.7-12.20)].
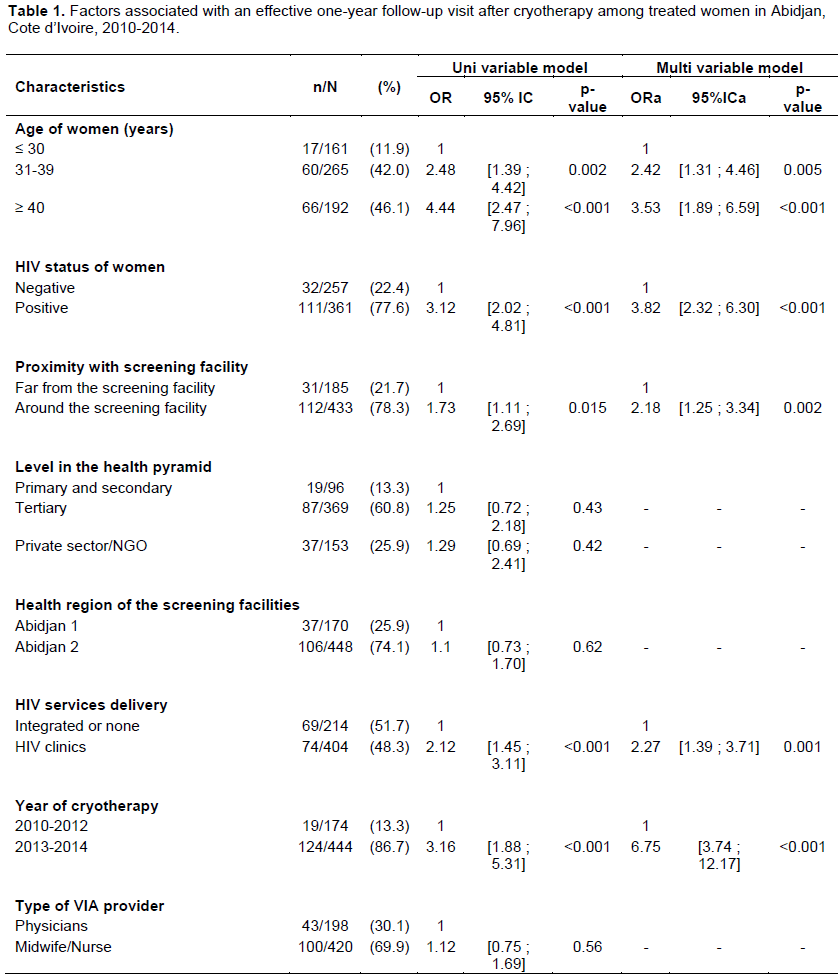
The quality of VIA provider [OR=1.1; 95%CI (0.7-1.7)] and the level of facility in the health system [OR=1.2; 95%CI (0.7-2.2)] were not associated with a follow-up visit after cryotherapy.
DISCUSSION
This study provides the first data on factors affecting a follow-up after cryotherapy uptake in Côte d'Ivoire. Being HIV positive and attending an HIV clinic were significantly associated with attendance to the follow-up visit. In addition, proximity with a cervical cancer screening facility and access to screening and cryotherapy after the year 2013 also showed a significant link with one-year follow-up visit.
This study suggests a higher one-year post cryotherapy attendance rate among HIV positive women followed up in HIV clinics. This higher rate among HIV positive women could be the positive impact of the “retention to care” package implemented in HIV clinics. These includes SMS reminders and phone calls for antiretroviral drug pick up, as well as transport reimbursement and food supply during psychosocial support groups (Project Djidja Brief (2020). These retention strategies led to more frequent contacts with the health facility among HIV positive women, increasing the possibility for health care workers to remind participants of the post cryotherapy follow-up visit, as well as for women to attend the integrated cervical cancer unit at the time of this visit. In addition, the improved patients file management and existence of HIV client’s databases in almost all HIV clinics facilitates the follow-up of HIV positive women receiving cervical cancer screening services. Leveraging on the HIV clinics experience, the cervical cancer prevention programs in Sub-Saharan Africa could identify innovative and sustainable interventions to maintain frequent contact (mainly virtual) with women attending cervical cancer screening units. Strategies for introducing mobile health interventions such as SMS reminders, mobile apps calendars, and phones calls have been shown to be acceptable and feasible for cervical cancer screening in previous studies from South Africa and Australia respectively (Moodley et al., 2019; Downer et al., 2006).
In our study, women attending cervical cancer units for screening and cryotherapy between 2013 and 2014 were more likely to attend the cervical cancer screening unit for their one-year post cryotherapy follow-up visit. The analysis of NCCP activity reports 2010-2015 retrieved that the implementation of the cervical cancer prevention program was done in two phases. It commenced by pilot phases that focused on HIV clinics from 2009 to 2012 and was followed by a scale-up phase characterized by integration of cervical cancer screening activities in public and private non-HIV health facilities (Boni et al., 2019). Thus, there is a strong association between scaling up and integrating cervical cancer screening services in all health facilities and the attendance to the one-year post cryotherapy follow-up. This reinforces the WHO recommendation to provide cervical cancer screening services for the general population by integrating these services in reproductive health activities or in maternal and child health units of all the health facilities (World Health Organization, 2014).
Implementing this integration strategy will help overcome some challenges to the cervical cancer screening and the post treatment follow-up visit such as geographic accessibility (Lim and Ojo, 2017). This idea is reinforced by the positive association between the proximity of the cervical cancer screening unit to the living place of the women and the attendance to the one-year post cryotherapy follow-up visit, found in our study and also was reported in a systematic review in sub-Saharan Africa (Lim and Ojo, 2017). Thus, the decentralization of cervical cancer screening and treatment services through their integration into all public and private health facilities is a game changer for the cervical cancer prevention, and should be strengthened at a national level to achieve and sustain the appropriate follow-up of women and avoid recurrence of cervical abnormalities leading to cervical cancer.
This study did not assess some of the demographic and socioeconomic factors encompassing marital status and personal income that could help explore patient-related barriers to attending post cryotherapy follow-up visits. However, this study is among the first to explore the correlates of attendance to follow-up visit after cryotherapy in West Africa. Findings from this study could implementing partners, in designing or adopting innovative and sustainable interventions to effectively prevent cervical cancers in Sub-Saharan African countries. However, further studies are needed to better understand the determinants of follow-up after cryotherapy or thermo-coagulation in developing countries, and assess the effectiveness of some promising approaches.
CONCLUSION
Close follow-up of patient as implemented in HIV clinics and geographic accessibility of cervical cancer screening units were determinant to one-year follow-up after cryotherapy. Innovative and sustainable strategies to maintain close contact with women could be implemented along with systematic integration of cervical cancer screening activities into health facilities, to improve follow-up of women and avoid occurrence of cervical cancer in sub-Saharan Africa.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGMENTS
Warm appreciation is extended to “International Epidemiology Databases to Evaluate AIDS (IeDEA) West Africa” and Dr Antoine Jaquet for their support to NCCP in data management and cancer registry improvement. The NCCP team is also thanked for the collaboration.
REFERENCES
|
Blumenthal PD, Gaffikin L, Deganus S, Lewis R, Emerson M, Adadevoh S, Group GC (2007). Cervical cancer prevention: Safety, acceptability, and feasibility of a single-visit approach in Accra, Ghana. American Journal of Obstetrics and Gynecology 196(4):407-409. |
|
|
Boni S, Tchounga B, Comoe K, Guie P, Adié M, Horo A,Jaquet A (2019). Assessment of the scaleâ€up of cervical cancer screening in Abidjan stratified by HIV status. International Journal of Gynecology and Obstetrics 147(2):246-251. |
|
|
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA,Jemal A (2018). Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: A Cancer Journal for Clinicians 68(6):394-424. |
|
|
Downer SR, Meara JG, Da Costa AC, Sethuraman K (2006). SMS text messaging improves outpatient attendance. Australian Health Review 30(3):389-396. |
|
|
Project Djidja Brief (2020). Improving the quality of HIV services to increase retention in care and treatment [internet]. [cited 2020 jun 2]. |
|
|
Lim JN, Ojo AA (2017). Barriers to utilisation of cervical cancer screening in Sub Saharan Africa: A systematic review. European Journal of Cancer Care 26(1):e12444. |
|
|
Moodley J, Constant D, Botha MH, Van der Merwe FH, Edwards A, Momberg M (2019). Exploring the feasibility of using mobile phones to improve the management of clients with cervical cancer precursor lesions. BMC Women's Health 19(1):2. |
|
|
National Cancer Control Program (2013). National guidelines for cervical cancer prevention, Cote d'Ivoire. National Cancer Control Program (NCCP), Cote d'Ivoire, 2013. |
|
|
Ouedraogo Y, Furlane G, Fruhauf T, Badolo O, Bonkoungou M, Pleah T, Bazant ES (2018). Expanding the single-visit approach for cervical cancer prevention: Successes and lessons from Burkina Faso. Global Health: Science and Practice 6(2):288-298. |
|
|
Parham GP, Mwanahamuntu MH, Kapambwe S, Muwonge R, Bateman AC, Blevins M, Chisele S(2015). Population-level scale-up of cervical cancer prevention services in a low-resource setting: Development, implementation, and evaluation of the cervical cancer prevention program in Zambia. PloS One 10(4):e0122169. |
|
|
PNLCa (2020). Prévention du cancer du col de l'uterus: Sites de dépistage [Internet]. pnlca. [cited 2020 Mar 17]. |
|
|
Shiferaw N, Salvador-Davila G, Kassahun K, Brooks MI, Weldegebreal T, Tilahun Y, Blumenthal PD (2016). The single-visit approach as a cervical cancer prevention strategy among women with HIV in Ethiopia: Successes and lessons learned. Global Health: Science and Practice 4(1):87-98. |
|
|
World Health Organization (2013). WHO guidelines for screening and treatment of precancerous lesions for cervical cancer prevention. Geneva: World Health Organization, 40p. |
|
|
World Health Organization (2014). WHO Comprehensive cervical cancer control: A guide to essential practice - 2nd ed. [Internet]. Geneva, Switzerland: WHO [cited 2017 Sep 15] P. 408. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


