ABSTRACT
Thyroid gland diseases are a public health problem worldwide. Imbalance in the regulation of thyroid gland hormones can cause many disorders that range from a small goiter to life threatening diseases, such as thyroid cancer. Thyroid dysfunction both hyper and hypothyroidism can affect circulatory system by affecting cardiac output, cardiac contractility, blood pressure, vascular resistance and rhythm disturbance which can further cause heart failure, fibrillation, congestive heart failure and blood pressure. Westernization and nutrition transition in Arab world have increased the burden of adeno-carcinomas, including thyroid cancer. This review aims to present the aggregated burden, risk factors and prognosis of various thyroid diseases prevalent in Arab countries. An electronic databases search was conducted using PubMed in addition to searching of accessible local journals in Arab world, using keywords and terms like epidemiology, burden, odds, risks, etc. After applying exclusion and inclusion criteria, 21 articles were selected to include in this review. The review showed that the prevalence of different types of thyroid disease varied between the reported studies in Arab world ranging from 6.18 to 47.34% prevalence of goiter reported by several studies conducted in Arab world, such as Egypt, Algeria and Bahrain with 25.25, 86 and 1.7%, respectively. Gender, dietary factors, iodine deficiency, family history, diabetes and x-ray radiation were reported as risk factors associated with different type of thyroid diseases. The most prevalence of thyroid disease was concluded to be thyroid lesions which varied in different regions of Arab and the burden of thyroid cancer is very high and very common in different Arab region, and further longitudinal studies are still needed to investigate the prognosis and determinants of these thyroid diseases in the Arab world.
Key words: Thyroid disease, prevalence, burden, odds, odds ratio, risk factors.
Thyroid gland is the hormone secreting organ that regulates body metabolism (Skarulis and Stack, 2015). Imbalance in the regulation of these hormones can cause many disorders that range from a small goiter to life threatening diseases, such as thyroid cancer (Ratini, 2015). The most common cause of thyroid disorders is iodine deficiency and literature shows that almost one-third of the world’s population lives in the area of iodine deficiency (Zimmermann, 2009). Thyroid lesion can be classified into congenital malformations, inflammatory in origin, endocrinal and neoplastic in origin (benign and malignant).
Several previous studies had reported that the most common type of thyroid disease is goiter; simple, diffuse and physiological (Vanderpump, 2005), and hypo-thyroidism and hyperthyroidism are also the prevalent types of thyroid disease (Vanderpump, 2010). Moreover, thyroid cancer is the fifth most common cancer in women (Jemal et al., 2010)and second most common cancer in Italy (Dal Maso et al., 2011). Hence, the thyroid gland disease is among the most common endocrine cancer, with approximation of 1.0 to 1.5% of all new cancers diagnosed each year in the USA, and its incidence has continuously increased in the last three decades all over the world (IARC Scientific Publications).
Furthermore, thyroid dysfunction both hyper and hypothyroidism can affect circulatory system by affecting cardiac output, cardiac contractility, blood pressure, vascular resistance and rhythm disturbance which can further cause heart failure, fibrillation, congestive heart failure and blood pressure (Klein and Danzi, 2007). It has been reported that changing in life styles in Arab world has led to the emerging of double burden of diseases, including the thyroid related diseases.
The westernization lifestyle and nutrition transition in Arab world have increased the burden of adeno-carcinomas, including thyroid cancer (Sawka et al., 2008). Thyroid cancer occupies the number two position among females in Saudi Arab (Sawka et al., 2008). Secondary to westernization and the life-style of Arab countries has changed over the past years and thus the burden of thyroid diseases, specifically cancer, is increasing, which further contributes to the economic crises.
To date and best knowledge of the authors, no systemic review has been conducted in our region to highlight and consolidate the prevailing data on thyroid disease. Thus, this review aims to present the aggregated burden, risk factors and prognosis of various thyroid diseases prevalent in Arab countries.
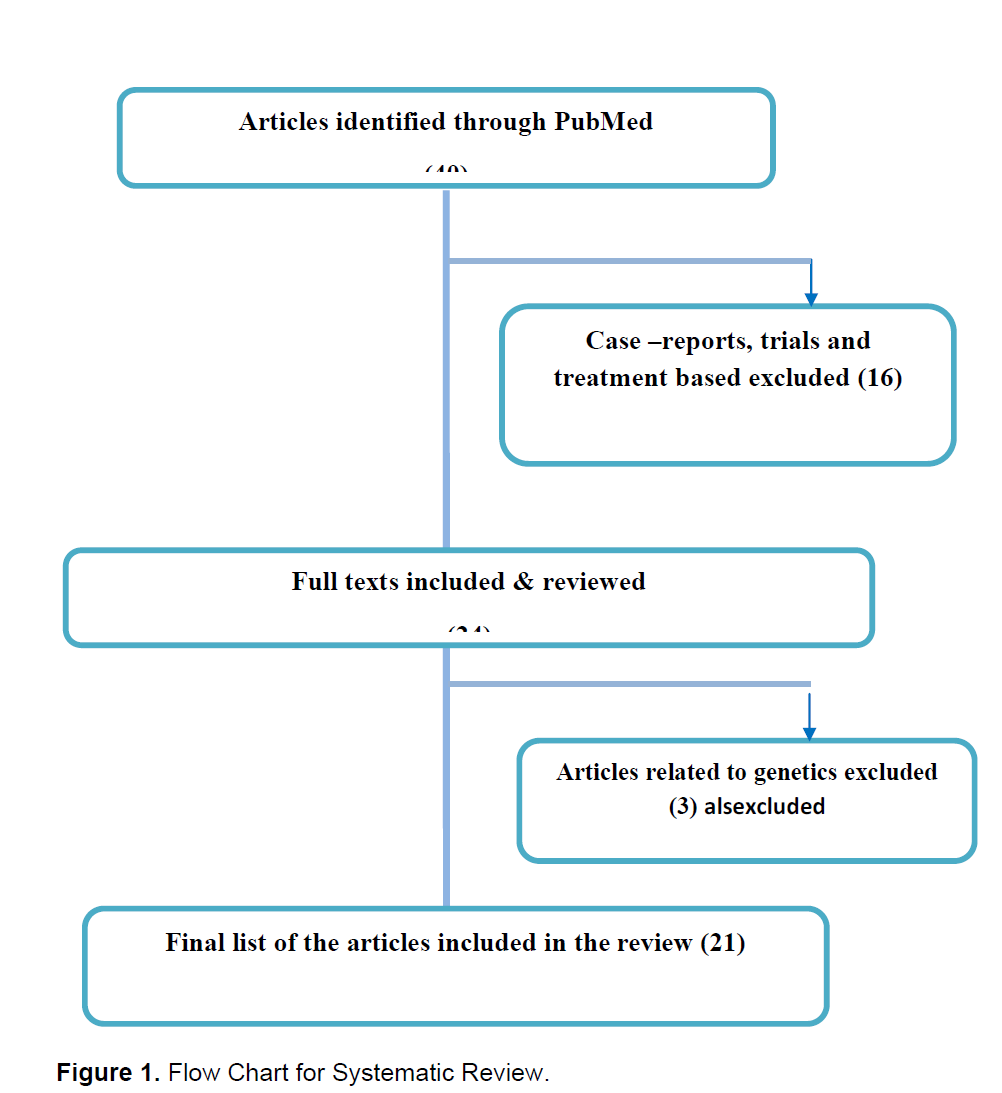
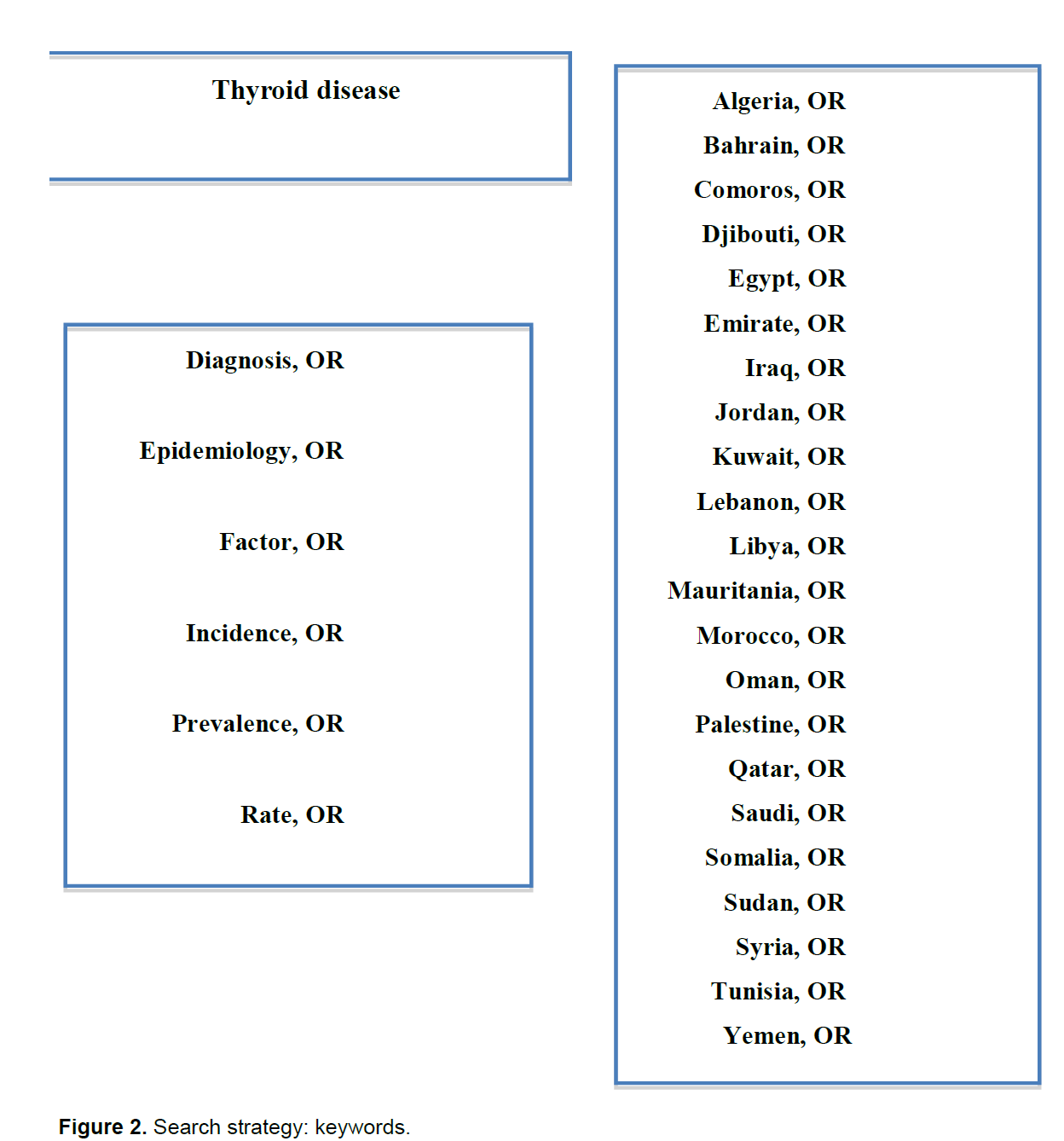
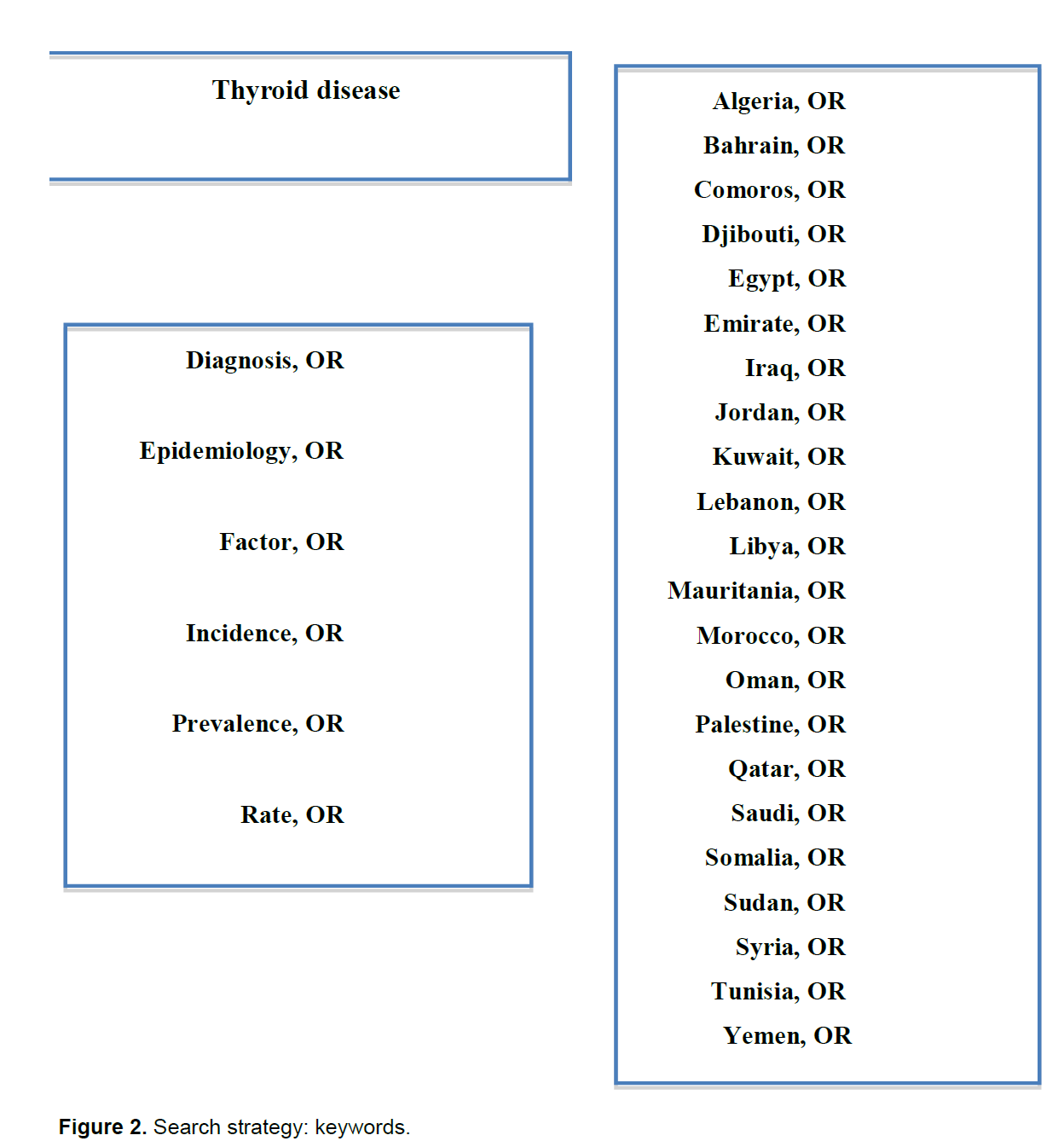
An electronic search was conducted using PubMed database during October 2014, in addition to searching of accessible local journals in Arab world. Inclusion criteria included: articles written in English language, articles describing or investigating the epidemiology, etiology, distribution, prognosis, impact and burden of thyroid diseases in Arab countries and publication date 2014. Consequently, case reports, clinical trials, including the preventive measure and treatment articles about pathological, histological premalignant, and malignant change regarding thyroid cancer were excluded (Figure 1). Then, the search results were reviewed by two authors: the first author and one co-author to identify which articles were relevant to the topic through screening the title and abstract. The search keywords used covered three main categories including thyroid diseases, epidemiological attributes and thyroid diseases geographical location. Boolean (OR/AND) were used to link all the search keywords. The main keys words were “Distribution”, “Epidemiology”, “Burden”, “Incidence”, “Pattern”, “Diagnosis”, “Etiology”, “Risk Factors”, “Odds”, “Odds ratio”, “Risk”, “Rate”, “Prevalence”, “Trend”, and “Prognosis” with combination of all Arab countries like Algeria, Iraq, Kuwait, Sudan and Yemen (Figure 2).
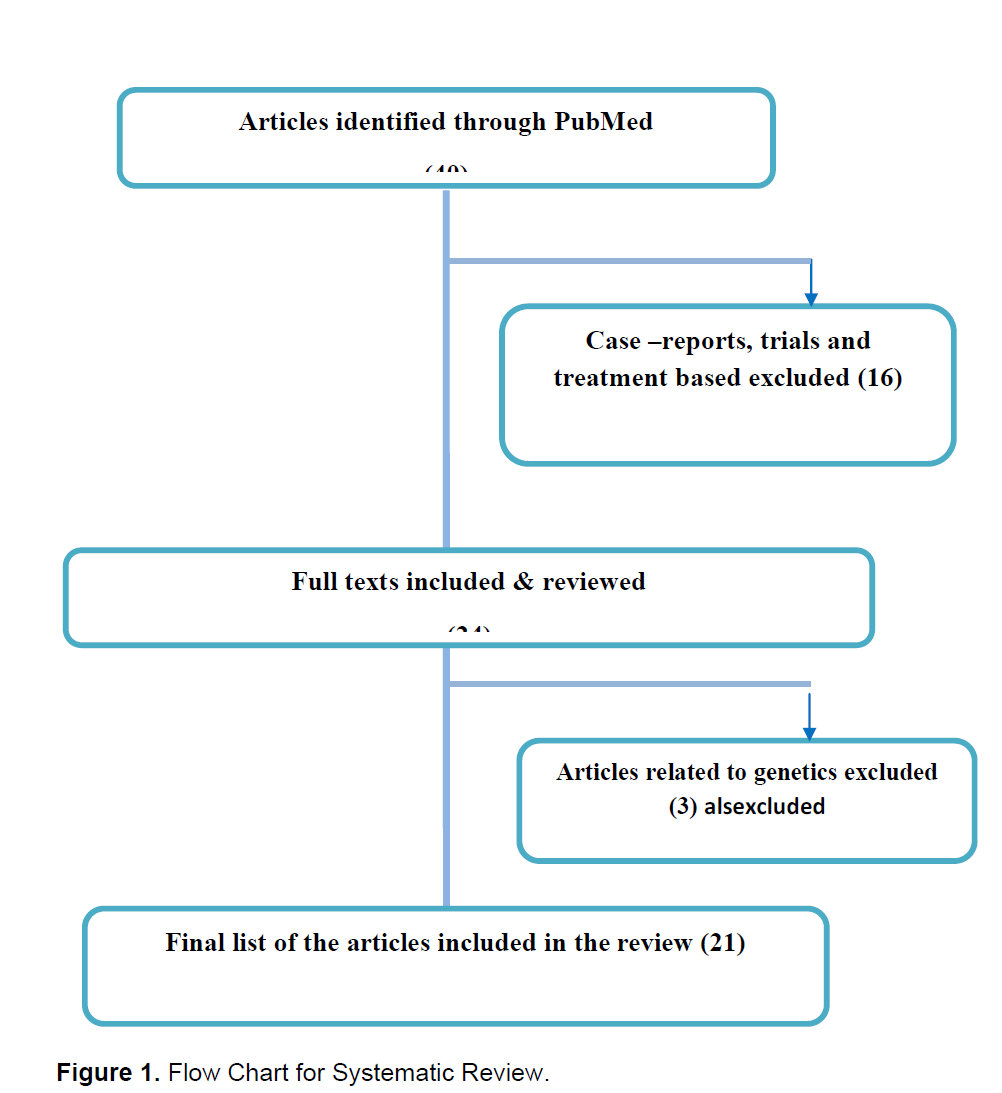
The initial screening of title/abstract of 40 identified articles resulted in excluding 16 articles as they were case reports, clinical trials and treatment based articles. The remaining 24full text articles were reviewed thoroughly by two reviewers and found 3 further articles related to genetics were excluded. Finally, only 21 articles were included in this review. The flow chart attached is given to highlight the process and sequence of article identification, evaluation and selection (1). The secondary research was performed to check the cross-referencing among the final list of the 21 articles searching for local specialized journals in Arab world, but no additional article was found through secondary search. The review results were classified according to the types of studies that are cross-sectional studies, case control retrospective and prospective studies. The studies that reported prevalence of different thyroid lesions, risk factors and studies conducted solely on thyroid cancer were further differentiated.
Study design
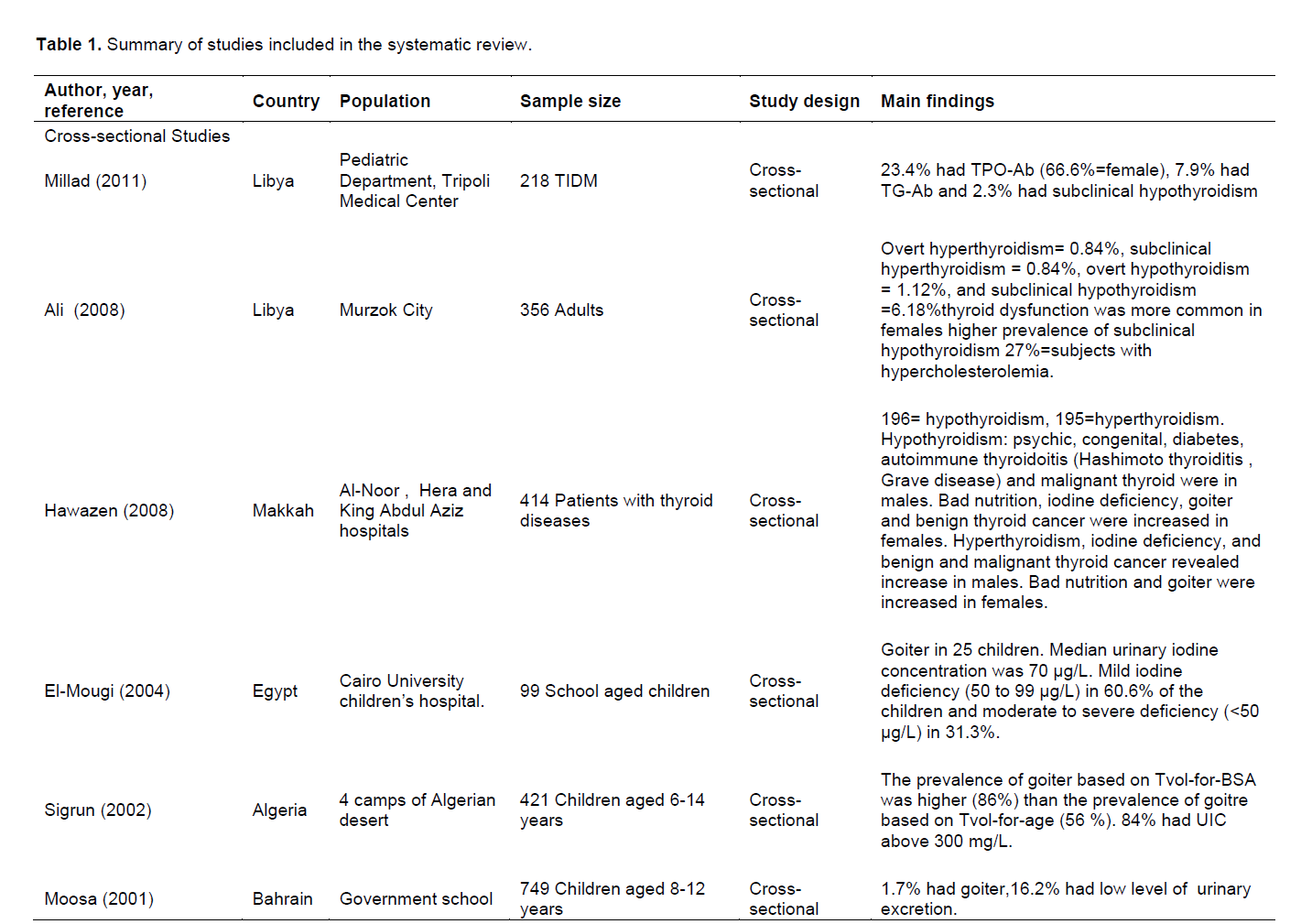
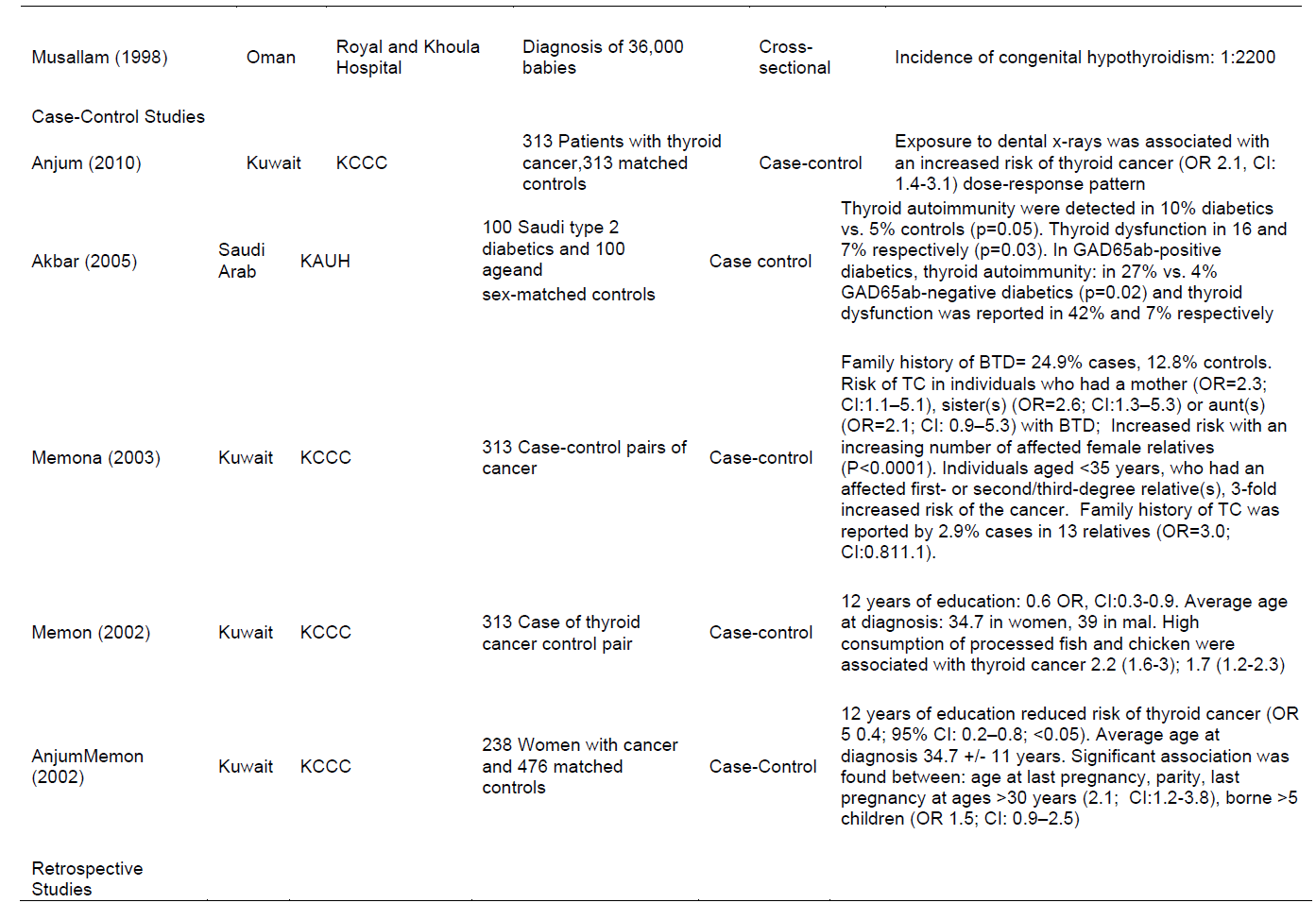
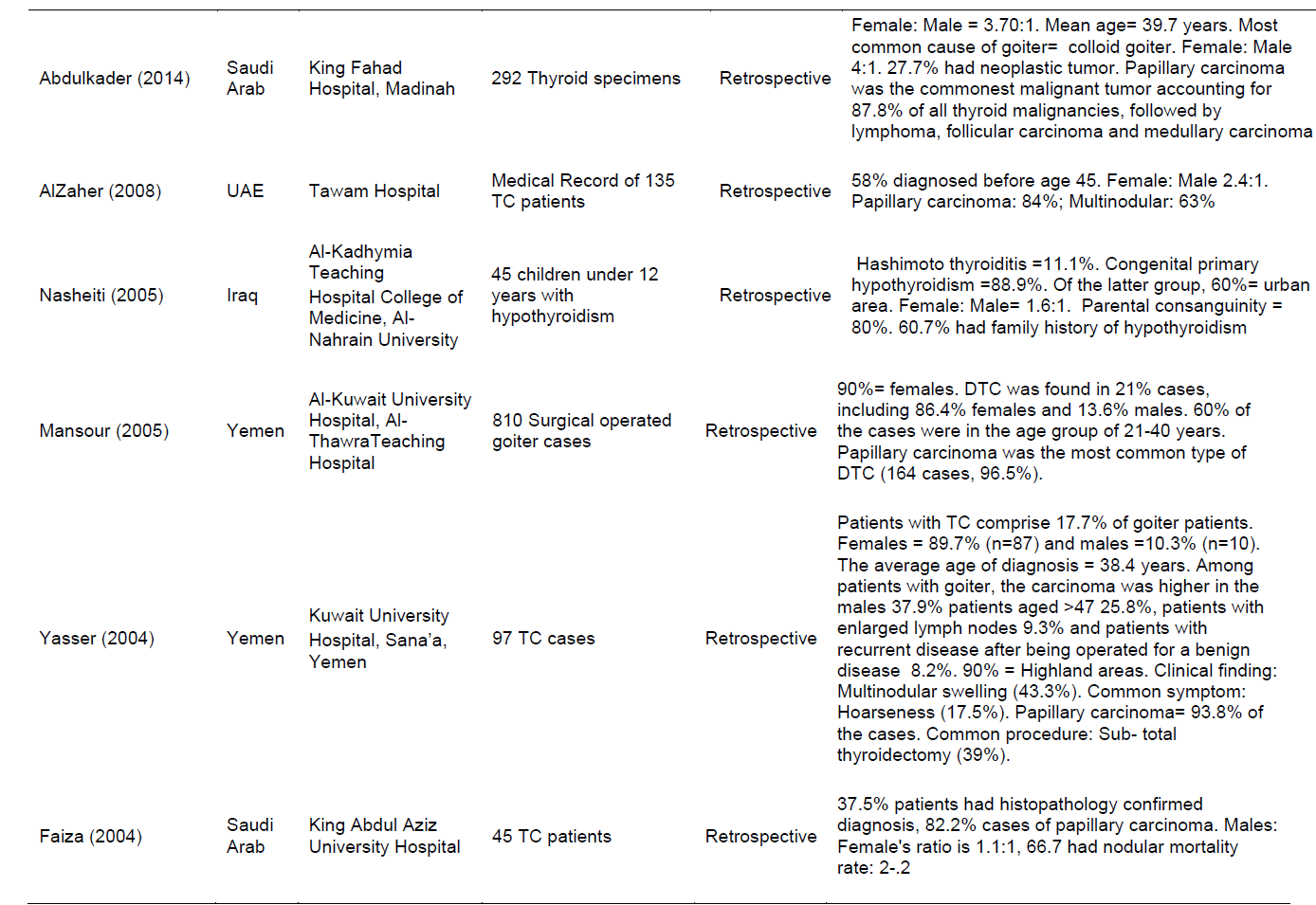
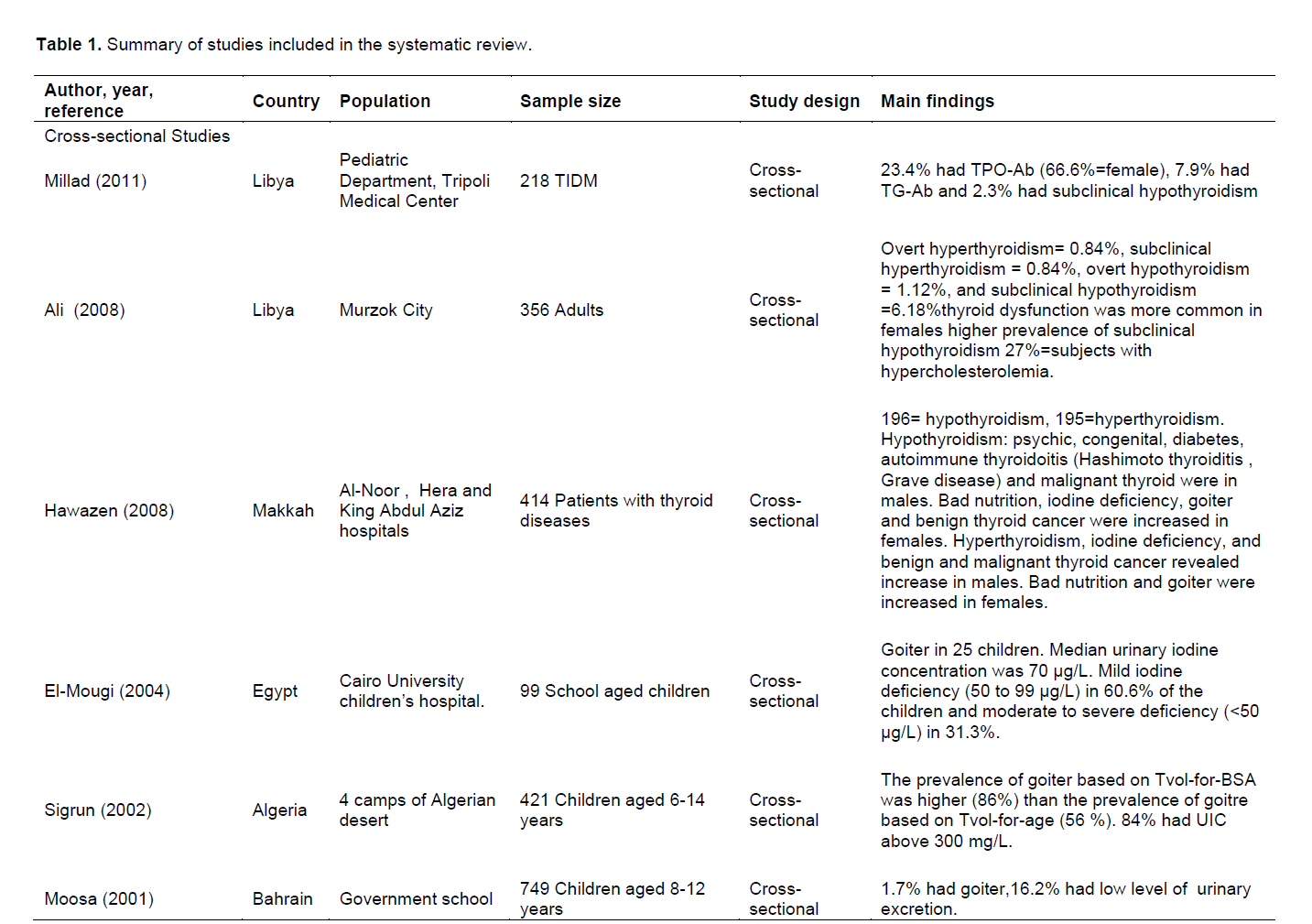
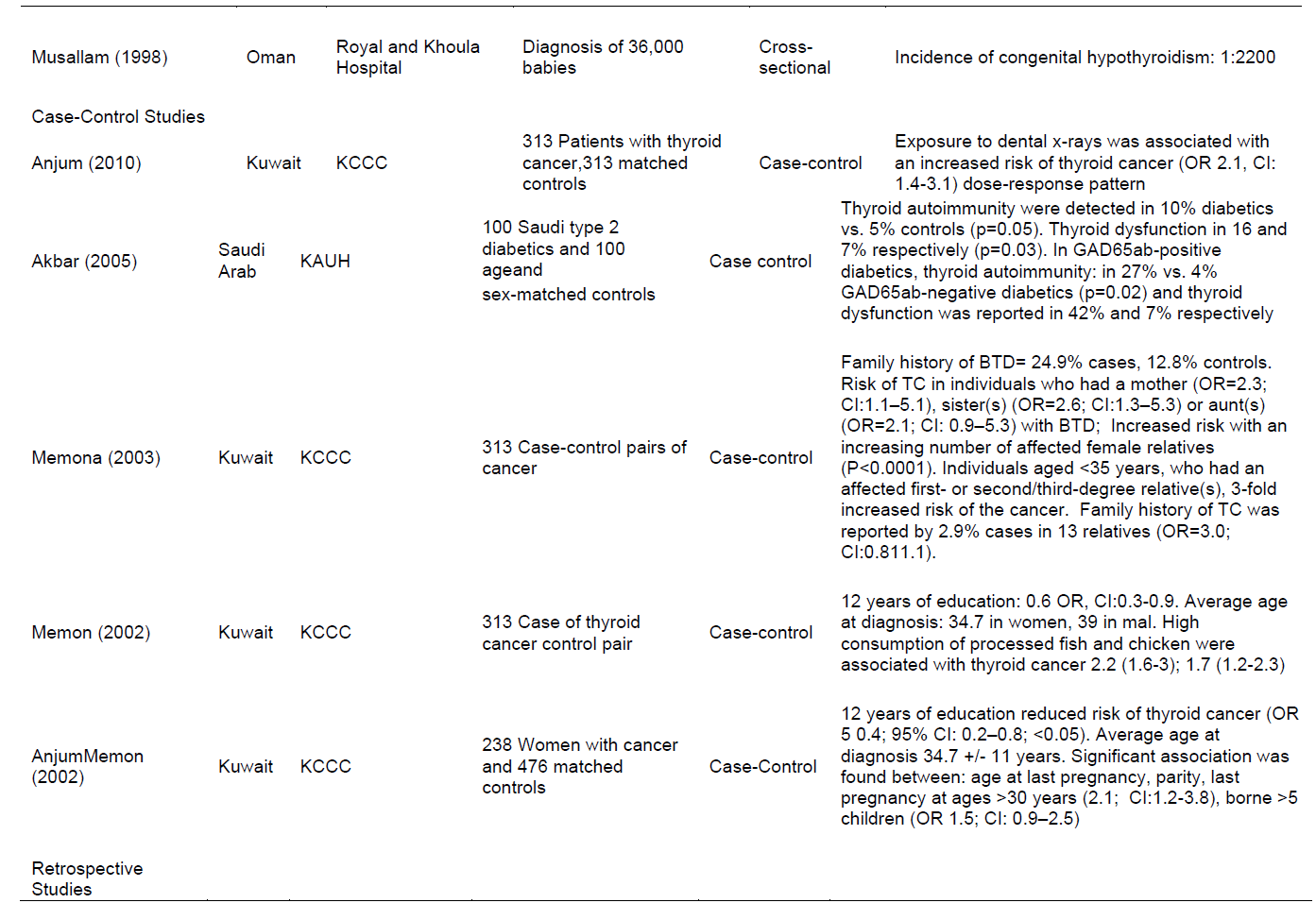
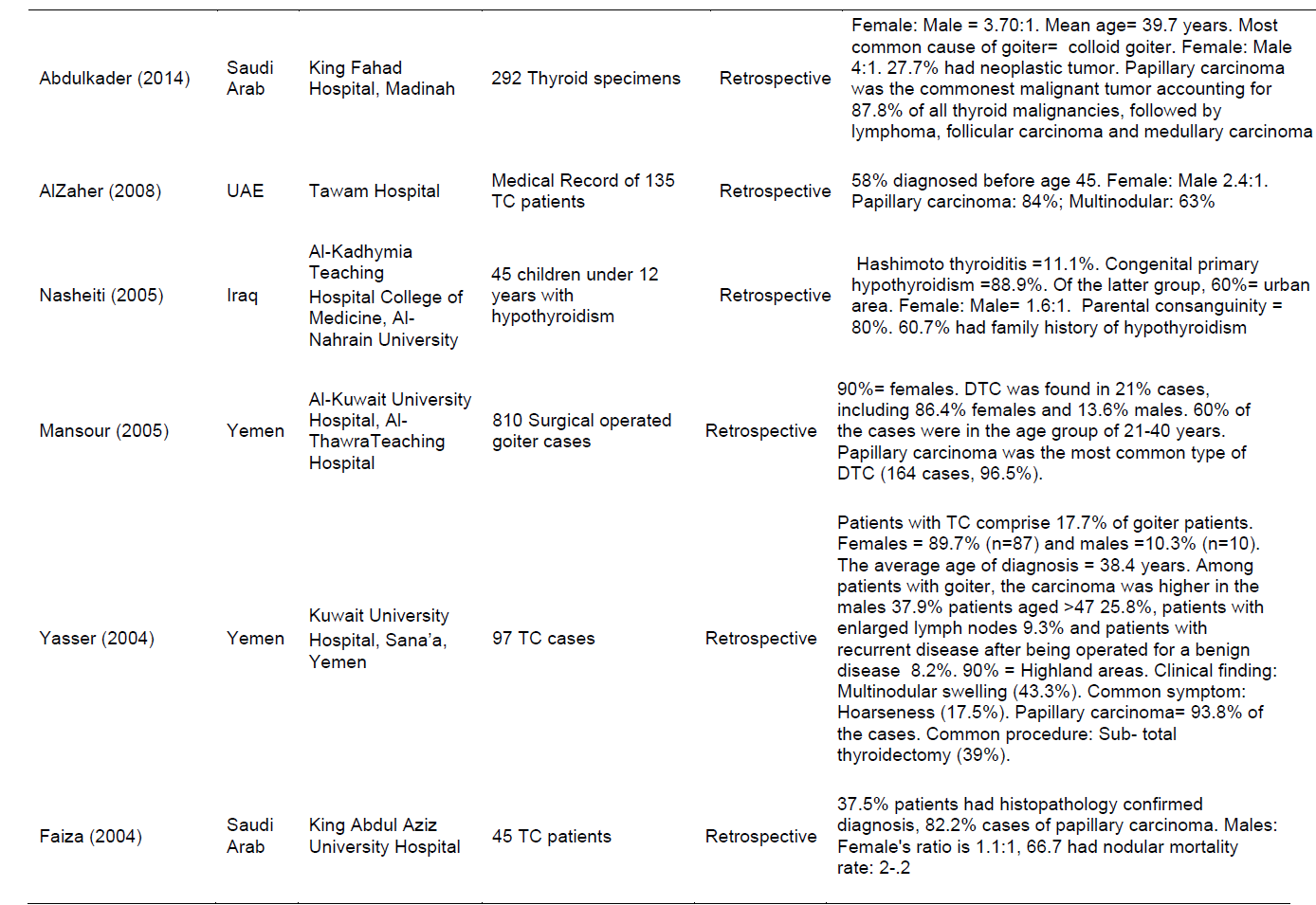
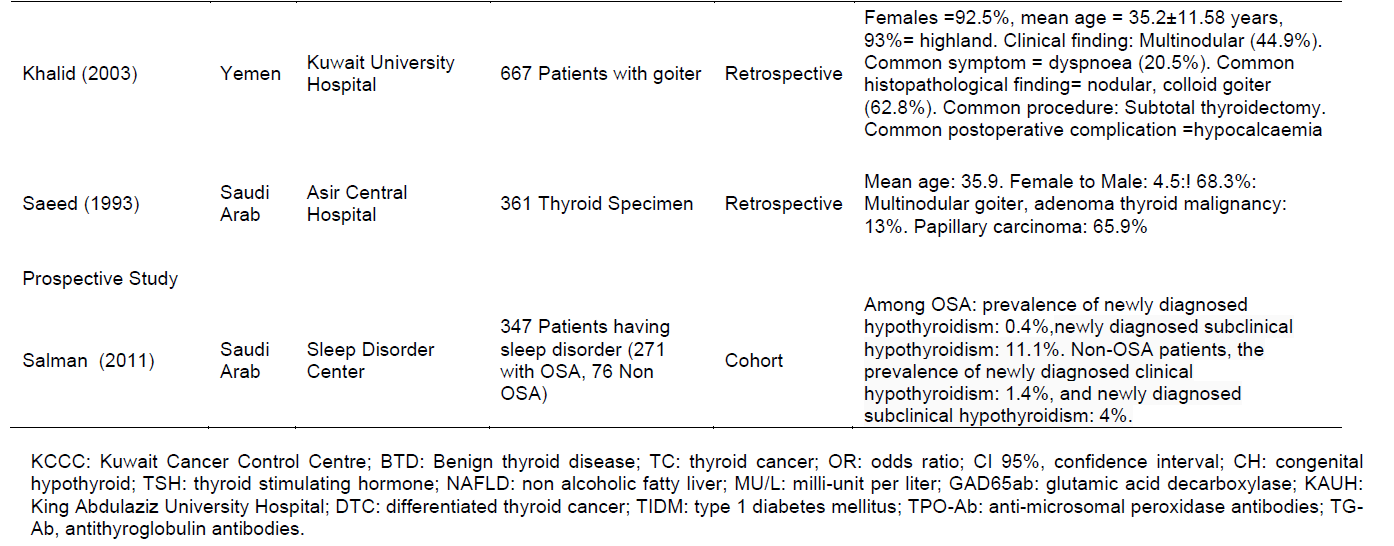
The review results showed different study designs as follows: seven cross-sectional studies were conducted in different Arab regions, including Libya, Saud Arabia, Egypt, Algeria, Bahrain and Oman (El-Mougi et al., 2004; Ghawil et al., 2011; Henjum et al., 2010; Lamfon, 2008; Moosa et al., 2000; Nouh et al., 2008; Elbualy et al.,1998). The sample size found varied from 99 to 749 subjects except for one study conducted in Oman in which 36000 babies were diagnosed. The study population of these studies comprised of children of school age and adults: five studies were case control with sample size varying from 100 to 313 subjects (Akbar et al., 2006; Memon et al., 2002a, b, 2004, 2010); four of the studies were from Kuwait (Memon et al., 2002a, b, 2004; Memon et al., 2010); and one from Saudi Arab (Akbar et al., 2006), and the study population was recruited from hospitals in Kuwait and Saudi Arab, retrospectively, and eight studies were retrospective; three were from Yemenone from Iraq (Nasheiti, 2005), three from Saudi Arab and one from United Arab Emirate. The sample size was found to vary from 45 to 810 subjects and comprised of children and adults, and all data collected were hospital based. One study conducted in Saudi Arab was prospective (Bahamman et al., 2011) (Table 1).
Prevalence of thyroid lesions
Different thyroid diseases were reported in different studies that include hypothyroid, hyperthyroid and goiter. The prevalence of different types of thyroid disease varied between the studies. The study conducted in 2011 in Libya reported the prevalence of subclinical hypothyroidism as 2.3% (Ghawil et al., 2011), and prevalence of hypothyroidism was reported as 6.18% in Libya (Nouh et al., 2008)and 47.34% in Saud Arabia (Makkah region) (Lamfon, 2008) and the prevalence of goiter was reported by many studies conducted in Egypt, Algeria and Bahrain (25.25, 86 and 1.7%, respectively) (El-Mougi et al., 2004; Henjum et al., 2010; Moosa et al., 2000).
Risk factors
Different risk factors were identified by different studies included in the review. The prevalence of thyroid diseases reported was found to be more prevalent in females than males. The study conducted in Iraq in 2005 reported that the female to male ratio of congenital primary hypothyroidism was 1.6:1 (Nasheiti, 2005), and studies conducted in Yemen in 2005 and 2004 reported higher prevalence of thyroid cancer in female than in males, that is, 90 and 89.7% respectively (Abdulmughni et al., 2004; FCPSP, 2005). The bad nutrition and iodine deficiency was reported as risk factors in study conducted in Makkah (Lamfon, 2008), and iodine deficiency in Egypt was also reported in 31.3% of school aged children by estimating urinary concentration of iodine (El-Mougi et al., 2004). A case control study conducted in 2005 in Saudi Arab among diabetic patients reported that 16% of the cases had thyroid dysfunction (Akbar et al., 2006), and one cohort study reported that the study participant having sleep disorder had high prevalence of subclinical hypothyroidism compared to the newly diagnosed clinical hypothyroidism. One retrospective study conducted in Iraq in 2005 documented that patients with hypothyroidism 89% had congenital hypothyroidism and 60% were from urban areas and more than half had parental consanguinity and family history of hypothyroidism (Nasheiti, 2005) (Table1).
Thyroid cancer
The nine studies included in this review had reported risk factors and clinical findings of thyroid cancer. Study conducted in 2010 in Kuwait reported dose-response relationship between dental x-ray and thyroid cancer (Memon et al., 2010). Another study from Kuwait conducted in 2003 reported association between family history of benign thyroid disease and thyroid cancer (Memon et al., 2004). Case control study conducted in 2002 in Kuwait reported that in female factors, such as age at last pregnancy, parity, pregnancy at age of 30 and above was associated with the increased risk of thyroid cancer (Memon et al., 2002). The papillary carcinoma was more prevalent in Yemen in 2005 and 2004 than any other types of cancer (96.5 and 93.8%, respectively). Both studies concluded that proportion of cancer was higher in female than male (Abdulmughni et al., 2004; FCPSP, 2005). Likewise, study conducted in Saudi Arab and UAE also reported high proportion of cancer in female than male and the prevalence of papillary carcinoma is higher than the other types of cancer (Abu-Eshy et al, 1995, Albasri et al, 2014, Al Zahir et al 2008, Qari, 2004) (Table 1).
Our review has covered wide variety of thyroid diseases, including hypothyroid and hyperthyroid, goiter, subclinical thyroid, congenital hypothyroid, hashimoto thyroid disease and thyroid cancer.The prevalence reported and study sample size varied from one study to another study. The prevalence of subclinical hypothyroidism was reported as 2.3 times in adult population of Libya (Ghawil et al., 2011)compared with study conducted in Colorado documented that the prevalence of subclinical hypothyroid in the general population ranged between 4 and 10% (Canaris et al., 2000). So, our review suggested that the prevalence in Arab region is comparatively low. This could be due to the small sample size that has been used in the study. Prevalence of hypothyroidism was reported as 6.18% in Libya and 47.34% in Saudi Arabia (Lamfon, 2008; Nouh et al., 2008)showing the prevalence is much higher than the prevalence reported in the study conducted in Scotland of 0.135% prevalence in people of age less than 22 years (Hunter et al., 2000). The possible explanation of the high prevalence in study conducted in Saudi Arabia could be because of the reasons and risk factors mentioned in the study that the iodine deficiency and bad nutrition. Furthermore, the sample size and variation in participants’ characteristics could have resulted in different prevalence of thyroid lesions.
This study review showed that the prevalence of goiter was in studies conducted in Egypt, Algeria and Bahrain (25.25, 86 and 1.7%, respectively) (El-Mougi et al., 2004; Henjum et al., 2010; Moosa et al., 2000). The possible explanation for the high goiter in the study of Algeria was due to high intake of iodine, and the result is line with a study conducted in 1998 among the Saharawi refugees that showed a prevalence of 28% for goiter (Pezzino et al., 1998). Some recent studies showed higher prevalence as the recent one had used ultrasound. The study conducted in past years in Oman and Saudi Arab showed 10 and 30% goiter of grades 1 and 2, respectively (Al Nuaim, 1995; Oman Ministry of Health, 1995). This high prevalence of goiter in Arab world is in agreement with the high prevalence encountered in countries, such as in Turkey, where goiter prevalence ranged from 5 to 56%, indicating severe to moderate iodine deficiency (ErdoÄŸan et al., 2002). However, the variation in the prevalence of different thyroid lesions in Arab world could be because the study methods, including different sample size, participant characteristics, source of recruitment of participants, and different tools, were used to identify the burden and different underline causes, such as high intake of iodine and bad nutrition.
The thyroid cancer was found prevalent in Arab region in this review similar to the study finding from India where the thyroid cancer was found to be one of the five most common cancer in India (Kalyani et al., 2010); whereas in Iranian population, thyroid cancer is the 7th most common cancer in females with an overall 5-year survival rate of 88% (Khayamzadeh et al., 2011). Moreover, in a study spanned over 25 years about the incidence of common cancers in Hong Kong, a number of cancers including thyroid cancers were found to be on an increase throughout the study period (Xie et al., 2012). Likewise, a study from Nepal on head and neck carcinomas reported that the most common site of primary lesion was larynx, followed by the thyroid (Lasrado et al., 2012).
The different studies included in this review have commented on the risk factors, clinical presentation and symptoms of thyroid cancer. Female predominance can be seen in our review and the common type of cancer was reported as papillary carcinoma. These findings are in agreement with the findings of study conducted in Iran over the period of 2000 to 2010 (Sokouti et al., 2013). The thyroid diseases as reported in this review are all multi-factorial. For example, as reported in the study of Kuwait that age at last pregnancy, parity, last pregnancy at ages >30 years were all associated with thyroid cancer. These finding are in agreement with what was mentioned in study done in Iran that TG-Ab and TPO-Ab were identified more frequently in women with recurrent abortions (Iravani et al., 2008). A study conducted in Kuwait in 2003 reported the association between benign thyroid disease and thyroid cancer (Memon et al., 2004). This findings are inconsistent with the study among Iribarren et al. (2001) which included 196 incident cases of thyroid cancer, and reported an approximately 2-fold increased risk with a family history of thyroid disease (Relative Risk (RR) = 2.2; 95%
CI: 1.2–4.1) (Iribarren et al., 2001). In addition, Helene et al., from a case-control study reported that seventeen cases (5.0%) and 2 controls (0.6%) reported at least one first degree in relation with thyroid cancer thus suggesting that genetic factors are important for thyroid cancer. Pal et al. (2001)showed that irrespective of the type of disease, the male to female ratio is higher for female having any type of thyroid disease. These findings are consistent with studies conducted in different countries. For example, the study conducted in Norway in 2000 concluded that the prevalence of former diagnosed hyperthyroidism was 2.5% in females and 0.6% in males, hypothyroidism 4.8 and 0.9%, and goiter 2.9 and 0.4% respectively. In both sexes, the prevalence increased with age (Bjoro, 2000).
Another interesting finding in this review is that the study conducted in Kuwait reported the association of Dental X-rays with thyroid cancer. These findings are consistent with the findings from number of previous studies, including a case-control study conducted in Sweden reporting the association of dental x-rays with thyroid cancer. A cross-sectional study also reported this association (Hallquist and Näsman, 2001), and cohort study conducted in USA also reported that x-ray workers had more risk of developing cancer than the other specialties (Zabel et al., 2006).
The limitations of this review includes limiting our search for articles in English, however, most if not all, studies by research institutes and universities are in English in the Arab world. Some articles might have been missed because different databases, like KoreaMed and Embase, were not search into but local journals were reviewed to include all the study related to the Saudi Arab. Publication bias, which is the tendency for publishing manuscripts positive findings, is a potential limitation of all systematic reviews including our review. Limitations of this systematic review also derive from limitations of the individual studies included. Most of the studies conducted in Saudi Arabia were cross-sectional and retrospective with very few follow-up studies that aim to know the prognosis, burden and consequences of these conditions on the society and healthcare services. On the other hand, the strength of this review to the best of our knowledge is the first review that highlights the burden of thyroid diseases in Arab world. Secondly, this review has included considerate amount of studies from many geographical territory of Arab, including Saudi Arab, Jordan, Yemen, Algeria, Kuwait, Egypt, etc. This study includes all the diseases that have been studied in Arab region such as hypothyroidism and hyperthyroidism, goiter, Hashimoto’s disease, Graves’ disease and thyroid cancer. The review has, to the best of its ability, consolidated the epidemiology, including prevalence of different types of thyroid diseases, the risk factors and clinical features of different thyroid diseases including thyroid cancer. Different study designs, such as cross-sectional, retrospectives and case-controls were included to highlight the true burden of the disease.
Prevalence of thyroid varied in different regions of Arab and the burden of thyroid cancer is very high and very common in different Arab region. Risk factors, such as female gender, bad nutrition, and diabetes and x-ray radiations were highlighted in the studies. Identified risk factors are potentially modifiable, emphasizing the importance of public health programs that are aimed at tackling such determinants. Future longitudinal studies are needed to investigate the prognosis and determinants of this condition in the Arab world. This study recommended early detection and prevention of disease at primary level by educating the population should be practiced.
Authors have no conflict of interests and the work was not supported or funded by any drug company.
The author’s would like to thank KSAU-HS for their support.
REFERENCES
|
Skarulis MC, Stack BC Jr (2015). Thyroid disease. e-Publication; Office on Women's Health (OWH). U.S. Department of Health and Human Services, Washington DC. View
|
|
|
|
Ratini M (2015). Understanding Thyroid Problems- the Basics: Women's Health. WebMD Medical Reference, WebMD, LLC. View
|
|
|
|
|
Abdulmughni YA, Al-Hureibi MA, Al-Hureibi KA, Ghafoor MA, Al-Wadan AH, Al-Hureibi YA (2004). Thyroid cancer in Yemen. Saudi Med. J. 25(1):55-59.
Pubmed
|
|
|
|
|
Abu-Eshy SA, Al-Shehri MY, Khan AR, Khan GM, Al-Humaidi MA, Malatani TS (1995). Causes of goiter in the Asir region: A histopathological analysis of 361 cases. Ann. Saudi Med.15(1):74-6.
Pubmed
|
|
|
|
|
Akbar D, Ahmed M, Al-Mughales J (2006). Thyroid dysfunction and thyroid autoimmunity in Saudi type 2 diabetics. Acta Diabetologica 43(1):14-18.
Crossref
|
|
|
|
|
Albasri A, Sawaf Z, Hussainy AS, Alhujaily A (2014). Histopathological patterns of thyroid disease in Al-Madinah region of Saud i Arabia. Asian Pac. J. Cancer Prev. 15:5565-5570.
Crossref
|
|
|
|
|
Al Nuaim AR (1995). National deficiency disorders survey in Saudi Arab Riyadh. King Khalid University Hospital.
|
|
|
|
|
Al Zahir N, Al Salam S, El Teraifi H (2008). Thyroid carcinoma in the United Arab Emirates: perspectives and experience of a tertiary care hospital. Hematol. Oncol. Stem. Cell Ther. 1(1):14-21.
Crossref
|
|
|
|
|
Bahamman SA, Sharif MM, Jammah AA, Bahammam AS (2011). Prevalence of thyroid disease in patients with obstructive sleep apnea. Respir. Med. 105(11):1755-1760.
Crossref
|
|
|
|
|
Bjoro T, Holmen J, Kruger O, Midthjell K, Hunstad K, Schreiner T, Sandnes L, Brochmann H (2000). Prevalence of thyroid disease, thyroid dysfunction and thyroid peroxidase antibodies in a large, unselected population. The Health Study of Nord-Trondelag (HUNT). Eur. J. Endocrinol. 143(5):639-647.
Crossref
|
|
|
|
|
Canaris GJ, Manowitz NR, Mayor G, Ridgway EC (2000). The Colorado thyroid disease prevalence study. Arch. Intern. Med. 160(4):526-534.
Crossref
|
|
|
|
|
Dal Maso L, Lise M, Zambon P, Falcini F, Crocetti E, Serraino D, . . . Cirilli C, Zanetti R, Vercelli M, Ferretti S, Stracci F, De Lisi V, Busco S,Tagliabue G, Budroni M, Tumino R, Giacomin A, Franceschi S (2011). Incidence of thyroid cancer in Italy, 1991–2005: time trends and age–period–cohort effects. Ann. oncol. 22(4):957-963.
Crossref
|
|
|
|
|
Elbualy M, Bold A, De Silva V, Gibbons U (1998) Congenital hypothyroid screening: the Oman experience. J. Trop. Perdiatr. 44(2):81-83.
Crossref
|
|
|
|
|
El-Mougi F, Abd-El-Ghaffar S, Fayek N, Mohammed M (2004). Urinary iodine and other iodine deficiency indicators in a sample of school-age children in Egypt. East Mediterr Health J. 10(6):863-870.
Pubmed
|
|
|
|
|
ErdoÄŸan G, ErdoÄŸan M, Emral R, BaÅŸtemir M, Sav H, HaznedaroÄŸlu D, UstündaÄŸ M, Köse R, Kamel N, Genç Y (2002). Iodine status and goiter prevalence in Turkey before mandatory iodization. J. Endocrinological Investigation 25(3):224-228.
Crossref
|
|
|
|
|
Qari FA (2004). Pattern of thyroid malignancy at a University Hospital in Western Saudi Arabia. Saudi Med. J. 25(7):866-870.
Pubmed
|
|
|
|
|
Al-Jaradi M, Sallam A, Jabr H, Borda A, Decaussin-Petrucci M, Berger N (2005). Prevalence of differentiated thyroid cancer in 810 cases of surgically treated goiter in Yemen. Ann. Saudi Med. 25(5):394-397.
Pubmed
|
|
|
|
|
Ghawil M, Tonutti E, Abusrewil S, Visentini D, Hadeed I, Miotti V, Tenore A (2011). Autoimmune thyroid disease in Libyan children and young adults with type 1 diabetes mellitus. Eur. J.pediatr. 170(8):983-987.
Crossref
|
|
|
|
|
Hallquist A, Näsman Å (2001). Medical diagnostic Xâ€ray radiation-an evaluation from medical records and dentist cards in a case–control study of thyroid cancer in the northern medical region of Sweden. Eur. J. cancer prev. 10(2):147-152.
Crossref
|
|
|
|
|
Henjum S, Barikmo I, Gjerlaug AK, Mohamed-Lehabib A, Oshaug A, Arne Strand T, Torheim LE (2010). Endemic goitre and excessive iodine in urine and drinking water among Saharawi refugee children. Public Health Nutr. 13(09):1472-1477.
Crossref
|
|
|
|
|
Hunter I, Greene SA, MacDonald TM, Morris AD (2000). Prevalence and aetiology of hypothyroidism in the young. Arch. Dis. childhood 83(3):207-210.
Crossref
|
|
|
|
|
Iravani AT, Saeedi MM, Pakravesh J, Hamidi S, Abbasi M (2008). Thyroid autoimmunity and recurrent spontaneous abortion in Iran: A case-control study. Endocrine Practice 14(4):458-464.
Crossref
|
|
|
|
|
Iribarren C, Haselkorn T, Tekawa IS, Friedman GD (2001). Cohort study of thyroid cancer in a San Francisco Bay area population. Int. J. Cancer 93(5):745-750.
Crossref
|
|
|
|
|
Jemal A, Siegel R, Xu J, Ward E (2010). Cancer statistics, 2010. CA: a cancer J. Clin. 60(5):277-300.
Crossref
|
|
|
|
|
Kalyani R, Das S, Kumar M (2010). Pattern of cancer in adolescent and young adults: A ten year study in India. Asian Pac. J. Cancer Prev. 11(3):655-659.
Pubmed
|
|
|
|
|
Khayamzadeh M, Khayamzadeh M, Tadayon N, Salmanian R, Zham H, Razzaghi Z, Akbari ME (2011). Survival of Thyroid Cancer and Social Determinants in Iran. Asian Pac. J. Cancer Prev. 12:95-98.
Pubmed
|
|
|
|
|
Klein I, Danzi S (2007). Thyroid disease and the heart. Circulation 116(15):1725-1735.
Crossref
|
|
|
|
|
Lamfon HA (2008). Thyroid Disorders in Makkah, Saudi Arabia. Ozean J. Appl. Sci. 1(1):52-58.
|
|
|
|
|
Lasrado S, Prabhu P, Kakria A, Kanchan T, Pant S, Sathian B, Gangadharan P, Binu V, Arathisenthil S, Jeergal PA, Luis NA, Menezes RG (2012). Clinicopathological profile of head and neck cancers in the Western development region, Nepal: A 4-year snapshot. Asian Pac. J. Cancer Prev. 13(12):6059-6062.
Crossref
|
|
|
|
|
Memon A, Berrington De Gonzalez A, Luqmani Y, Suresh A (2004). Family history of benign thyroid disease and cancer and risk of thyroid cancer. Eur. J. Cancer 40(5):754-760.
Crossref
|
|
|
|
|
Memon A, Darif M, Alâ€Saleh K, Suresh A (2002a). Epidemiology of reproductive and hormonal factors in thyroid cancer: Evidence from a caseâ€control study in the Middle East. Int. J. cancer 97(1):82-89.
Crossref
|
|
|
|
|
Memon A, Godward S, Williams D, Siddique I, Al-Saleh K (2010). Dental x-rays and the risk of thyroid cancer: a case-control study. Acta Oncologica 49(4):447-453.
Crossref
|
|
|
|
|
Memon A, Varghese A, Suresh A (2002b). Benign thyroid disease and dietary factors in thyroid cancer: A case–control study in Kuwait. Br. J. Cancer 86(11):1745-1750.
Crossref
|
|
|
|
|
Moosa K, Abdul WA, Al-Sayyad J, Baig B (2000). National study on the prevalence of iodine deficiency disorders among schoolchildren 8-12 years of age in Bahrain. Eastern Mediterranean health journal= La revue de sante de la Mediterraneeorientale= al-Majallah al-sihhiyah li-sharq al-mutawassit, 7(4-5):609-616.
|
|
|
|
|
Nasheiti N (2005). Childhood hypothyroidism in Iraq: a retrospective study. Int. J. Endocrinol. Metabol. 3(3):136-139.
|
|
|
|
|
Oman Ministry of Health (1995). National study on the prevalence of iodine deficiency disorder in Oman. Ministry of Health, Sultanate of Oman.
|
|
|
|
|
Nouh AM, Eshnaf I, Basher MA (2008). Prevalence of thyroid dysfunction and its effect on serum lipid profiles in a Murzok, Libya Population. Thyroid Sci. 3(10):1-6.
|
|
|
|
|
Pal T, Vogl FD, Chappuis PO, Tsang R, Brierley J, Renard H, Sanders K, Kantemiroff T, Bagha S, Goldgar DE, Narod SA, Foulkes WD (2001). Increased risk for nonmedullary thyroid cancer in the first degree relatives of prevalent cases of nonmedullary thyroid cancer: a hospital-based study. J. Clin. Endocrinol. Metabol. 86(11):5307-5312.
Crossref
|
|
|
|
|
Pezzino V, Padova G, Vigneri R, Turiano G, Compagno L, Branca F, Mustafa S (1998). Iodine-independent endemic goiter in Saharawi refugee camps in Southwestern Algeria. IDD newsletter, 14(1):12-13.
|
|
|
|
|
Sawka AM, Brierley JD, Tsang RW, Thabane L, Rotstein L, Gafni A, Straus S, Goldstein DP (2008). An updated systematic review and commentary examining the effectiveness of radioactive iodine remnant ablation in well-differentiated thyroid cancer. Endocrinol. Metab. Clin. North Am. 37(2):457-480.
Crossref
|
|
|
|
|
Sokouti M, Montazeri V, Fakhrjou A, Samankan S, Goldust M (2013). 25 Years in Tabriz, Iran (2000-2012). Pakistan J. Biol. Sci. 16(24):2003-2008.
Crossref
|
|
|
|
|
Vanderpump M (2010). The epidemiology of thyroid disease. Br. Med. Bull. 99:39-51. PMID: 5673172
Crossref
|
|
|
|
|
Vanderpump MPJ (2005). The epidemiology of thyroid diseases. In: Braverman LE, Utiger RD, editors. Werner and Ingbar's The Thyroid: A Fundamental and Clinical Text. 9th edn. Philadelphia: JB Lippincott-Raven pp. 398-496.
|
|
|
|
|
Xie WC, Chan MH, Mak KC, Chan WT, He M (2012). Trends in the Incidence of 15 Common Cancers in Hong Kong. Asian Pac. J. Cancer Prev. 13:3911-3916.
Crossref
|
|
|
|
|
Zabel EW, Alexander BH, Mongin SJ, Doody MM, Sigurdson AJ, Linet MS, Freedman M, Hauptmann M, Kiyohiko M, Ron E (2006) Thyroid cancer and employment as a radiologic technologist. Int. J. Cancer 119(8):1940-1945.
Crossref
|
|
|
|
|
Zimmermann MB (2009). Iodine deficiency. Endocrine Rev. 30(4):376-408.
Crossref
|
|