Full Length Research Paper

ABSTRACT
Socio-economic and socio-demographic factors have been considered as critical in disease epidemiology and need to be taken into consideration when designing health interventions. It is therefore strongly recommended to investigate population ownership to ensure sustainability of a given intervention. To this end, a household-based cross sectional survey was conducted to assess knowledge and perceptions regarding sleeping sickness and its control among populations of the four epicenter villages (Lambi, Bidjouka, Memel 1, and Ebimimbang) of the Bipindi sleeping sickness focus (South Region, Cameroon). It was found that the population of Bipindi is stable (64.0% of participants having spent on average 22 years in this focus), with high education level (64.8% having reached at least the secondary level). Overall, 92.8% (95% CI: 86.9-96.2) of the participants were aware of sleeping sickness or Human Africa Trypanosomiasis (HAT) and 68.3% (95% CI: 59.6-75.9) have been in contact with people who had suffered from this disease. Males had better knowledge of sleeping sickness clinical signs and mode of transmission than their female counterparts. Knowledge was associated both with gender (males exhibiting better knowledge of clinical signs and mode of transmission than females) and age group (participants aged 30-57 years having heard of HAT more frequently than people of other age groups). These findings suggest that the population of Bipindi exhibit knowledge and perceptions that can be useful for appropriation and sustainability of control interventions.
Key words: Sleeping sickness, knowledge, perception, Bipindi, Cameroon.
INTRODUCTION
Human African Trypanosomiasis (HAT), also called sleeping sickness, is a vector-borne parasitic disease due to trypanosomes and transmitted from one host to another by the blood sucking tsetse flies. This neglected tropical disease (NTD) is restricted to Africa, where two trypanosome species are causing the disease in humans:
Trypanosoma brucei rhodesiense distributed in East and Southern Africa, and Trypanosoma brucei gambiense found in West and Central Africa (Simarro et al., 2008).
HAT is ranked by the World Health Organization (WHO) among intensified disease management (IDM) group, and the fight against this parasitic disease mostly relies on mass screening and treatment campaigns using mainly melarsoprol, administered for the treatment of the second stage of the disease, even though serious side effects have been sometimes recorded. Despite these concerns related to the use of melarsoprol, screening and treatment campaigns have significantly reduced the occurrence of cases in all foci. Indeed, in 2009, the number of notified cases fell below 10,000 for the first time in 50 years and, in 2018, only 977 cases were recorded (WHO, 2020). This drastic reduction in the number of notified cases (more than 95% between 2000 and 2018) encouraged the WHO experts committee to target sleeping sickness for elimination as public health problem by 2020 (WHO, 2012; Simarro et al., 2013) and for transmission interruption by 2030 (Franco et al., 2018; WHO, 2020). Although active case detection and treatment remains one of the key tools to tackle sleeping sickness, a number of patients are not always identified during these screening campaigns, and the transmission of the disease is therefore ongoing. In fact, during the last decade, community participation in active screening varied very slightly, while many patients had been rather passively screened (Franco et al., 2018). Therefore, the disease is still persisting in some foci despite sustained active case detection surveys, and the surveillance system based on sentinel sites appeared not to be optimal (Franco et al, 2018).
In areas were the disease was deemed to persist, a significant decrease in the number of cases has been recorded when vector control activities have been initiated to complement medical surveys (Simarro et al., 2015). In some countries in Central Africa (Cameroon, Gabon, Congo, Equatorial Guinea), although sustained active screening and treatment of cases detected led to a significant reduction in the number of active cases, a quite silent transmission was ongoing, thus jeopardizing efforts towards elimination of the disease (Simarro et al., 2015). To overcome this situation and achieve the 2030 target, WHO recommended the integration of control and surveillance activities at the peripheral level of the health system, as well as the reinforcement of ownership by the local populations (WHO, 2020).
In Cameroon, vector control using the promising tiny targets (Lehane et al., 2016; Mahamat et al., 2017; Barrett, 2018) is being tested in the Campo HAT focus in southern Cameroon (Tanekou, Unpublished data). Although quite promising, ownership is compulsory for sustainability purpose, and it is already known that it can be influenced by the degree of knowledge and perceptions of local health personnel and populations (Launiala, 2009).
To this end, a survey in the Bipindi HAT focus was conducted to investigate the knowledge and perceptions of the populations regarding the disease and its control in order to assess the feasibility of the operationalization of vector control, one of the key strategies to accelerate sleeping sickness elimination.
MATERIALS AND METHODS
Ethical considerations
This study was carried out in the framework of the Cameroon National Human African Trypanosomiasis Control routine entomological surveys aiming to update the transmission of sleeping sickness in the Bipindi focus. Prior to initiating data collection on the field, a meeting was first organized with the local administrative and traditional authorities to explain the objectives and the interest of the study. After obtaining their agreements, populations in each village were briefed on the objectives and schedule of the study, as well as on the voluntary nature of their participation. All individuals who agreed to participate provided verbal consents before enrollment, under the discretion of respective household heads. A unique identifier was assigned to each participant for anonymity purpose.
Study area and population
This study was carried out in the Bipindi (3°2’N; 10°22’E) sleeping sickness focus in Cameroon, located at 75 km from the Atlantic coast in the Lolodorf Health District (South Region, Cameroon). Bipindi has a humid equatorial climate with four seasons (02 rainy seasons and 02 dry seasons), the dominant vegetation being dense forest. The local population is composed of three ethnic groups namely Bassa, Ngoumba and Fang, and their main activities are agriculture, hunting and fishing (Grébaut et al., 2000). The cocoa plantations, the humid forest and the dense and regular hydrographic network provide a favorable habitat for the development of tsetse flies (mainly Glossina palpalis palpalis) the principal vector of sleeping sickness (Simo et al., 2008).
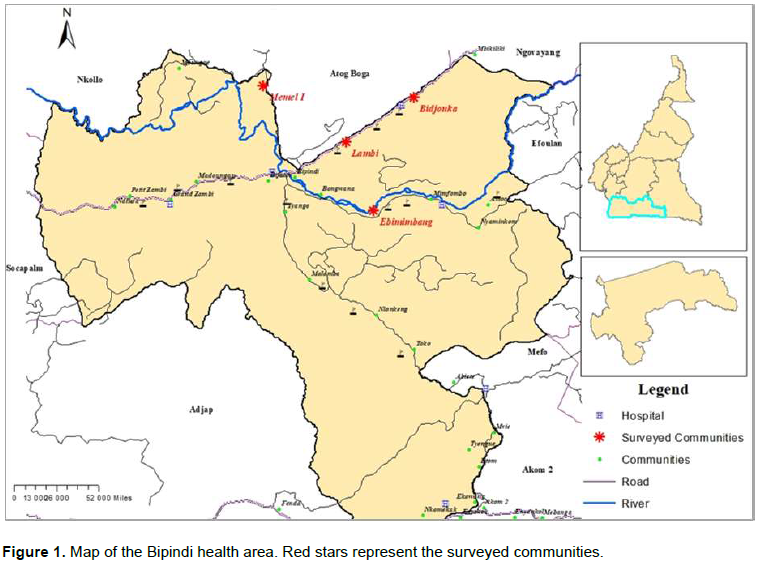
Formerly known as the Lolodorf focus, this HAT focus was identified since the 19th century (Grébaut et al., 2000). The evolution of the disease is very silent, likely explaining little attention devoted by the health authorities to this disease in the Bipindi focus. The number of patients diagnosed between 1998 and 1999 (44 cases) prompted the National program to intensify disease control activities. Since 2014, only five cases have been notified, revealing an important impact of control strategies on the transmission of the disease. This study was implemented in the villages (Lambi, Bidjouka, Memel1, Ebimimbang) (Figure 1), where cases have been reported since the last two decades (Simarro et al., 2010).
Study design and data collection
A household-based cross sectional survey was conducted in the Bipindi HAT focus, following a convenient sampling design, to assess knowledge and perceptions of local populations with regards with sleeping sickness and its control using a semi-structured questionnaire. In each household, the questionnaire was administered separately to all the members present regardless their gender and occupation, but who are living permanently in the village and deemed to have the intellectual capacities to answer the questions of investigators. A local guide was associated to the research team and was committed to the translation of questions in local language (Bassa, Ngoumba, Fang), especially when interviewees were illiterates. In addition to socio-demographic information’s (gender, age, occupation, educational level, village of residence and number of years of residence in the community), participants were asked whether they have already heard about HAT, and if “yes”, they were further questioned about clinical signs, transmission mode, their experience with the disease well as the organization of interventions/control approaches, notably the case detection and treatment campaigns.
Data analysis
Information collected on paper forms was entered using ODK collect application installed on a numeric tablet and the resulting Microsoft Office Excel dataset was cleaned and exported into R software (The R foundation for Statistical Computing, Vienna, Austria) for statistical analysis. Categorical variables (gender, occupation, educational level, village of residence) were expressed using proportions with 95% confidence intervals (95% CI), and continuous variables (age, number of years of residence in the targeted village) were expressed using median with their interquartile range (IQR). Knowledge variables (HAT causative agents, T. b. gambiense and vectors, Tsetse flies) as well as perceptions of populations with regards with HAT control were compared between different respondents’ socio-demographic characteristics using Chi-Square test. The threshold for significance was set at 5%.
RESULTS
Socio-demographic characteristics of the surveyed population
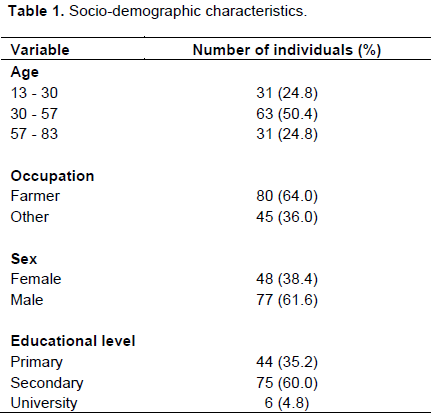
A total of 125 participants were interviewed during this survey. The sex ratio (Male/Female) was male biased (1.8), and the age of participants ranged between 13 and 83 years old (median: 42 years old; Interquartile range (IQR): 30.5 – 57.5 years old). Regarding the level of education of participants, most of them reached the secondary school (60.0%), and only a few attended high school/university (4.0%). More than half (64.0%) of participants were farmers who already spent on average 22 years (Standard deviation, SD: 39 years) in the study area (Table 1).
Knowledge and perceptions of the enrolees regarding HAT
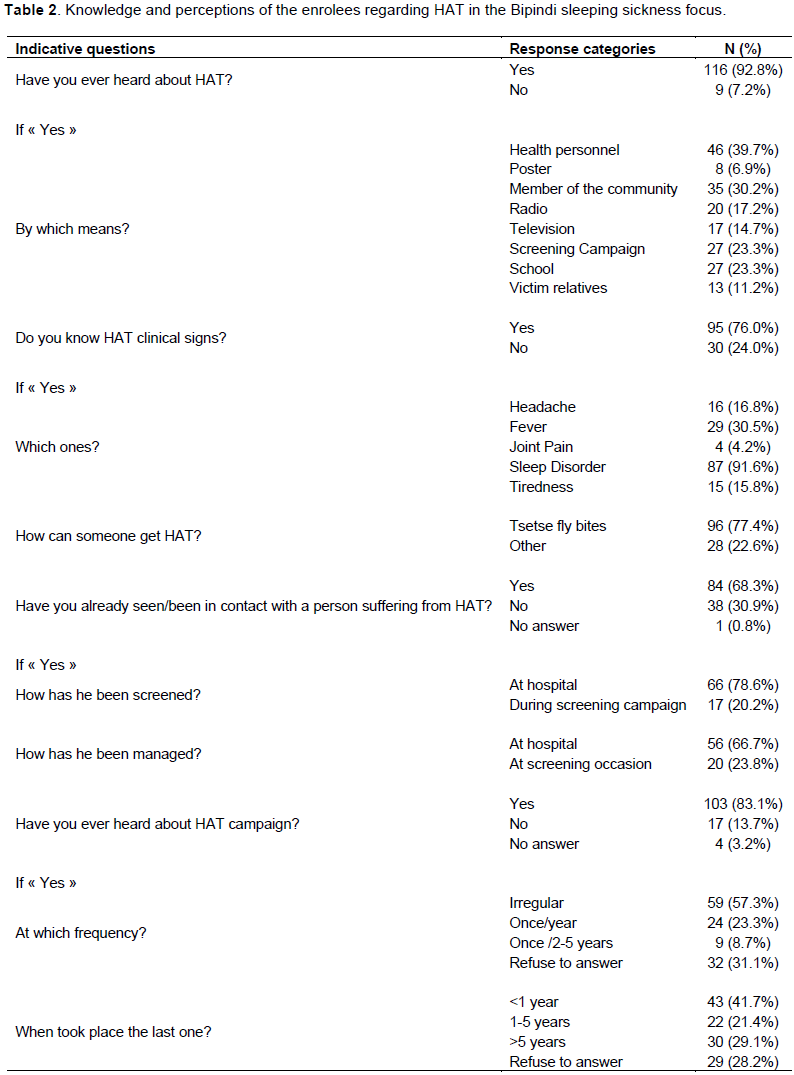
Table 2 summarizes the descriptive statistics of the knowledge and perceptions of the enrolees regarding HAT in the Bipindi sleeping sickness focus. Almost all the respondents (92.8%; 95% CI: 86.9-96.2) acknowledged that they had already heard about HAT, mainly through a health personnel (39.6%), community personnel (30.2%), during screening campaigns (23.3%) or at school (23.3%). A total of 76.0% (95% CI: 67.8-82.6) of the respondents were aware of clinical signs of HAT, sleep disorder (91.6%; 95% CI: 84.3-95.7) being the most frequently reported sign. Up to 77.4% (95% CI: 69.3-83.9) of the participants knew that HAT is transmitted by tsetse fly bites. Overall, 68.3% (95% CI: 59.6-75.9) of participants declared having already seen/been in contact with a person suffering from HAT, mostly at hospital (78.6%) or at the occasion of screening campaigns (20.2%) for their management, especially because hospital was the elected place for HAT management (66.7%). Also, 83.1% (95% CI: 75.5-88.6) of studied participants declared that they have already heard about HAT screening campaign, though 57.3% (95% CI: 47.6-66.4) of them indicated that these campaigns are irregular while 41.7% (95% CI: 32.7-51.4) declared that the last screening campaign took place less than one year ago.
Association between knowledge regarding HAT and socio-demographic characteristics of the enrolees
The knowledge of HAT clinical signs was significantly associated with gender (P = 0.001), males exhibiting better knowledge than females. No association was found with either educational level (P = 0.25), occupation (P = 0.55) or age group (P = 0.44). The fact to have “ever heard about HAT” was significantly associated with the participant age group (P-value = 0.04); participants aged 30-57 years having heard of HAT more frequently than people of other age groups; while no association was found with educational level (P = 0.14), occupation (P = 0.72) or gender (P = 0.3). The knowledge of mode of HAT transmission was significantly associated with education (P = 0.001), gender (P = 0.002), while no association was found with the participant occupation (P = 0.8) or participant age group (P = 0.19). Males exhibited better knowledge of the mode of transmission of HAT than females; In addition, the knowledge of the mode of transmission of HAT was associated with educational level; those who attended secondary school exhibited better knowledge.
DISCUSSION
The current survey was conducted to investigate whether populations are well aware of sleeping sickness and its control measures; important prerequisites for ownership of interventions. Indeed, the ownership of interventions by the local populations could be useful for their sustainability (WHO, 2009; 2017; Simarro et al., 2013). It was previously demonstrated that socio-economic and socio-demographic factors such as education, age, gender and occupation could play a critical role in disease epidemiology and need to be taken into consideration when designing health interventions (Keeling et al., 2010; Laskowski et al., 2011). Therefore, such survey is strongly recommended to ensure whether a target population or sociological group is eligible to own and successfully implement a strategy or an intervention (Launiala, 2009).
The present study revealed that the population of Bipindi is stable (64.0% of participants having spent on average 22 years on site) and exhibits a high level of education; these factors are favorable assets for the implementation, sustainability, self-monitoring and operationalization of control strategies or interventions. In general, the participants were aware and had good knowledge of sleeping sickness, its mode of transmission and the control strategy organized by the HAT national control program. Similar results have been previously described in South Sudan (Bukachi et al., 2018). Unlike in South Sudan where only 18% of participants reported sleep disorder, the majority of participants (91.6%) in the Bipindi focus reported that the latter is the most evocative sign of HAT. This high level of awareness could be explained by the fact that most of the participants (68.3%) had been in contact with HAT cases who are, for most of them, still alive in the villages. Also, the frequency of control case detection and treatment campaigns as well as research activities in this focus since the 1998 HAT outbreak can explain this awareness (Miézan et al., 1991; Grébaut et al., 2000; Simo et al., 2008; Njiokou et al., 2010; Farikou et al., 2010; Tanekou et al., 2011; Tchouomene et al., 2013). About 22.6% of participants were not aware of the mode of transmission of sleeping sickness and about 23.8% didn’t trust that hospital can be used for the management of HAT cases; this knowledge gaps can constitute firstly weaknesses to a possible community involvement in strategies to fight against sleeping sickness and secondly a barrier to activities that may facilitate elimination of HAT transmission in Bipindi. These gaps must be targeted and tackled before the implementation of complementary activities to strengthen the HAT control strategy in the Bipindi focus. Nevertheless, most of the participants trusted health services for sleeping sickness treatment (66.7%). This result is very interesting and can be explained by the fact that the populations visited during this survey experienced the 1998s outbreak of the disease and live with many villagers who were successfully cured at the Bipindi integrated health center during previous screening campaigns. This observation is similar to what was already described in the Yei County focus in South Sudan where up to 97.2% of participants trusted health services for suspected HAT infection (Bukachi et al., 2018).
More than half (57.3%) of participants declared that control campaigns were irregular, as the HAT national control program usually complains about the insufficiency/lack of financial resources to organize regular screening campaigns (PNLTHA, 2019). This irregularity in the organization of screening campaigns could be attributed to the low priority granted to this deadly disease as per the scarcity of cases after the outbreak periods (Simarro et al., 2008).
The knowledge of HAT clinical signs was significantly associated with gender (P = 0.001), males having better knowledge than their female counterparts. This result could be explained by the fact that men are usually involved in vector control and research activities conducted in the Bipindi HAT focus.
The fact to have “ever heard about HAT” was significantly associated with the age of participants (p-value = 0.04); individuals aged 30-57 years having heard of HAT more frequently than people of the other age groups. This is likely because most of these participants experienced the outbreak which had devastated populations of the Bipindi HAT focus in the 1990s. No association was however found between the fact to “ever heard about HAT” and educational level (P = 0.14), occupation (P = 0.72) or gender (P = 0.3); these results, together with the fact that 68.3% of participants had already seen/been in contact with a person suffering of HAT, is a very important epidemiologic information showing that individuals from all age groups regardless of occupation, level of education or gender are aware that they are at risk of sleeping sickness in the Bipindi HAT focus.
The knowledge of the mode of HAT transmission was significantly associated with education (P-value = 0.001) and gender (P-value = 0.002). Indeed, male participants exhibited better knowledge than their female counterparts, and individuals who attended the secondary level were more aware of the mode of transmission of HAT. Similar findings have already been observed in southern Sudan (Bukachi et al., 2018), and could be explained by the fact that the participants who attended secondary school constitute the most important section of the population in the Bipindi focus. No association of the transmission mode was found with the participant occupation (P-value = 0.8) or participant age group (P-value = 0.19), as most of the enrollees (77.4%) knew the transmission mode of sleeping sickness, whatever their societal classes were. This is quite informative for the development of alternative strategies for the elimination of sleeping sickness by integrating Bipindi’s populations in the fight against the disease, especially in the vector control strategy (PNLTHA, 2019).
CONCLUSION
This study revealed that the populations of the four villages visited during the survey, whatever their age, gender, occupation or level of education were, were well aware of sleeping sickness and exhibited good knowledge of its mode of transmission, clinical manifestations, and control strategies implemented by the Cameroon national HAT control program. Most of the participants acknowledged the impact of screening and treatment campaigns, although they lamented on the fact that these campaigns are irregular. Vector control against HAT remains challenging because optimal tool and implementation strategy are yet to be established. The operationalization approach of vector control, with the active involvement of communities, appeared feasible based on population’s knowledge, perceptions and willingness to participate. This could help in reducing implementation costs and achieving the WHO goal of eliminating sleeping sickness by 2030.
LIMITATIONS
The main limitations of this study are related to sampling. Indeed, because of limited financial resources, the survey was carried out only in the sleeping sickness epicenter villages of the Bipindi focus where the populations might be more aware of the disease and its control measures because of its historic burden. In addition, sample size was not computed as a convenient sampling design, which is known to be prune to bias, was used.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGMENTS
This study was supported by the Partnership for Increasing the Impact of Vector Control (PIIVec) consortium, hosted by the Liverpool School of Tropical Medicine (LTSM) and managed in Cameroon by the Center for Research in Infectious Diseases (CRID). The authors are grateful to the Bipindi’s population who willingly accepted to participate to the study.
REFERENCES
|
Barrett MP (2018). The elimination of human African trypanosomiasis is in sight: Report from the third WHO stakeholders meeting on elimination of gambiense human African trypanosomiasis. PLoS Neglected Tropical Diseases 12(12):e0006925. |
|
|
Bukachi SA, Mumbo AA, Alak AC, Sebit W, Rumunu J, Biéler S, Ndung'u JM.(2018) Knowledge, attitudes and practices about human African trypanosomiasis and their implications in designing intervention strategies for Yei county, South Sudan. PLoS Neglected Tropical Diseases 12(10):e0006826. |
|
|
Farikou O, Njiokou F, Mbida JA, Njitchouang GR, Djeunga HN, Asonganyi T, Simarro PP, Cuny G, Geiger A (2010). Tripartite interactions between tsetse flies, Sodalis glossinidius and trypanosomes-an epidemiological approach in two historical human African trypanosomiasis foci in Cameroon. Infection, Genetics and Evolution 10(1):115-21. |
|
|
Franco JR, Cecchi G, Priotto G, Paone M, Diarra A, Grout L, Simarro PP, Zhao W, Argaw D (2018). Monitoring the elimination of human African trypanosomiasis: Update to 2016. PLoS Negl Trop Dis 12(12): e0006890. |
|
|
Grébaut P, Wang S, Bodo JM, Ebo'o Eyenga V, Binzouli JJ, Ndong Ngoe C, Nomo E, Nkinin S, Njiokou F, Ollivier G, Foumane V (2000). Aspects épidémiologiques d'un foyer de maladie du sommeil mal connu: le foyer de Bipindi au Cameroun. Bulletin de Liaison et de Documentation-OCEAC 33(2):16-22. |
|
|
Keeling MJ, Danon L, Vernon MC, House TA (2010). Individual identity and movement networks for disease metapopulations. Proceedings of the National Academy of Sciences 107(19):8866-8870. |
|
|
Laskowski M, Mostaço-Guidolin LC, Greer AL, Wu J, Moghadas SM (2011). The impact of demographic variables on disease spread: influenza in remote communities. Scientific Reports 1(1):1-7. |
|
|
Launiala A (2009). How much can a KAP survey tell us about people's knowledge, attitudes and practices? Some observations from medical anthropology research on malaria in pregnancy in Malawi. Anthropology Matters 11(1). |
|
|
Lehane M, Alfaroukh I, Bucheton B, Camara M, Harris A, Kaba D, Lumbala C, Peka M, Rayaisse JB, Waiswa C, Solano P (2016). Tsetse control and the elimination of Gambian sleeping sickness. PLoS Neglected Tropical Diseases 10(4):e0004437. |
|
|
Mahamat MH, Peka M, Rayaisse JB, Rock KS, Toko MA, Darnas J, Brahim GM, Alkatib AB, Yoni W, Tirados I, Courtin F (2017). Adding tsetse control to medical activities contributes to decreasing transmission of sleeping sickness in the Mandoul focus (Chad). PLoS Neglected Tropical Diseases 11(7):e0005792. |
|
|
Miézan T, Doua F, Cattand P, De Raadt P (1991) Evaluation du Testryp CATT appliqué au sang prélevé sur papier filtre et au sang dilué, dans le foyer de trypanosomiase à Trypanosoma brucei gambiense en Côte d'Ivoire. Bulletin of the World Health Organization 69(5):603. |
|
|
Njiokou F, Nimpaye H, Simo G, Njitchouang GR, Asonganyi T, Cuny G, Herder S (2010) Domestic animals as potential reservoir hosts of Trypanosoma brucei gambiense in sleeping sickness foci in Cameroon. Parasite 17(1):61-66. |
|
|
Programme National de Lutte contre la Trypanosomiase Humaine Africaine (PNLTHA) (2019). Cameroun: mise à jour et priorités-THA gambiense. Réunion des Coordonnateurs et Responsables Nationaux de Programmes de Lutte contre la Trypanosomiase Humaine Africaine à T. b. gambiense. Oral Communication, 26-28 February 2019, Grand Bassam, Kribi, Cameroon. |
|
|
Simarro PP, Cecchi G, Franco JR, Paone M, Diarra A, Priotto G, Mattioli RC, Jannin JG (2015) Monitoring the progress towards the elimination of gambiense human African trypanosomiasis. PLoS Neglected Tropical Diseases 9(6):e0003785. |
|
|
Simarro PP, Cecchi G, Paone M, Franco JR, Diarra A, Ruiz JA Fèvre EM, Courtin F, Mattioli RC, Jannin JG (2010) The Atlas of Human African Trypanosomiasis: a contribution to global mapping of neglected tropical diseases. International Journal of Health Geographics 9(1):1-18 |
|
|
Simarro PP, Franco JR, Diarra JA, Ruiz Postigo JA, Jannin J (2013). Diversity of Human African Trypanosomiasis epidemiological settings requires fine-tuning control strategies to facilitate disease elimination. Research and Reports in Tropical Medicine 1-6. |
|
|
Simarro PP, Jannin J, Cattand P (2008) Eliminating human African trypanosomiasis: where do we stand and what comes next? PLoS Medicine 5(2):e55. |
|
|
Simo G, Njiokou F, Mbida JM, Njitchouang GR, Herder S, Asonganyi T, Cuny G. (2008) Tsetse fly host preference from sleeping sickness foci in Cameroon: epidemiological implications. Infection, Genetics and Evolution 8(1):34-39. |
|
|
Tanekou TT, Melachio TT, Simo G, Ravel S, De Meeûs T, Causse S, Solano P, Lutumba P, Asonganyi T, Njiokou F (2011) Population genetics of Glossina palpalis palpalis from central African sleeping sickness foci. Parasites and Vectors 4(1):1-8. |
|
|
Tchouomene-Labou J, Nana-Djeunga H, Simo G, Njitchouang GR, Cuny G, Asonganyi T, Njiokou F (2013) Spatial and temporal variations relevant to tsetse control in the Bipindi focus of southern Cameroon. Parasites and Vectors 6(1):1-0. |
|
|
World Health Organization (WHO) (2009). Interventions sous directives communautaires pour résoudre les grands problèmes de santé en Afrique : une étude multi-pays. Programme spécial de recherche et de formation concernant les maladies tropicales, 144p |
|
|
World Health Organization (WHO) (2012). Accelerating work to overcome the global impact of Neglected Tropical Diseases. A Roadmap for Implementation. Geneva, Switzerland: World Health Organization. |
|
|
World Health Organization (WHO) (2013). Report of a WHO meeting on elimination of African trypanosomiasis (Trypanosoma brucei gambiense). Geneva: World Health Organization. |
|
|
World Health Organization (WHO) (2017). Report of the second WHO stakeholders meeting on rhodesiense human African trypanosomiasis; Geneva WHO/HTM/NTD/IDM/2017.04 |
|
|
World Health Organization (WHO) (2020). A road map for Neglected Tropical Diseases 2021-2030. WHO reports 55 p. |
|
|
World Health Organization (WHO) (2020). Trypanosomiase Humaine Africaine (Maladie du Sommeil).who.int/fr/news-room/fact-sheets/detail/trypa |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


