Review

ABSTRACT
In recent years in the United States there has been a shift towards legalization of marijuana for medical and recreational purposes. The medical use of cannabis is legalized in 33 states, 4 territories and the district of Columbia. Medical marijuana use was legalized in Puerto Rico in 2015. Cannabinoid Hyperemesis Syndrome (CHS) is one of the effects of the use of cannabis. This paper will attempt to introduce CHS to providers in Puerto and provide suggestions for incorporating the diagnosis and treatment modalities into the healthcare system of Puerto Rico. Electronic searches in PubMed from 2000 to 2019, the Cumulative Index to Nursing and Allied Health Literature were used. A hand search of selected specialist journals and reference lists of articles obtained was then conducted. A total of 22 articles were reviewed. Literature review indicated that Cannabinoid Hyperemesis Syndrome (CHS) is fairly new and that healthcare providers must consider this syndrome in patients on medical marijuana. Cannabinoid Hyperemesis Syndrome (CHS) is possible in patients using medical marijuana. This further increases the need for surveillance and proper therapeutic managements. CHS needs to be added to the list of diagnosis in Puerto Rico. Health care plans would also need to begin the process for inclusion of CHS in list of covered disorders and formulate mechanisms for reimbursement and other healthcare finance approvals.
Key words: Medical marijuana, Cannabinoid Hyperemesis Syndrome, Therapeutic managements
INTRODUCTION
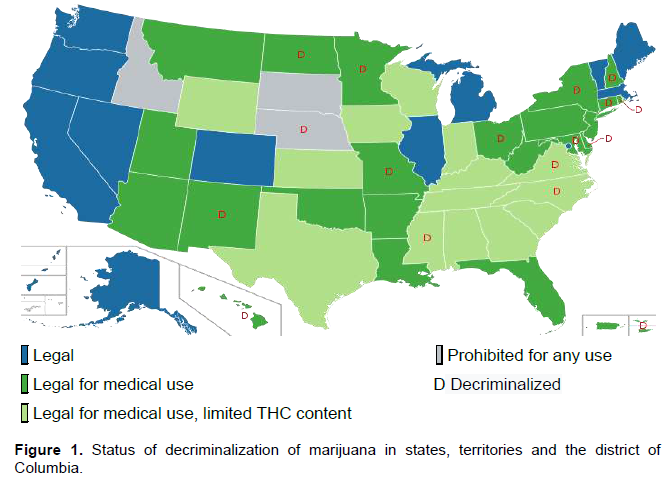
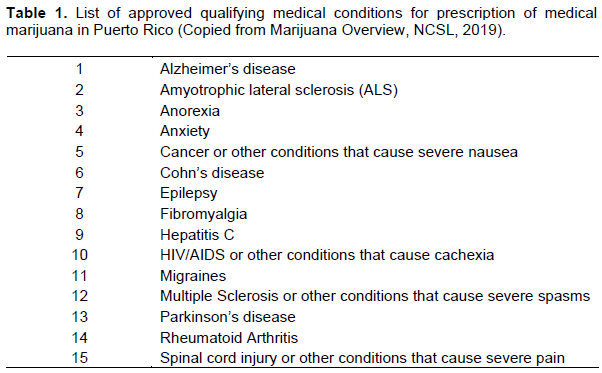
In recent years in many states and territories of the United States there has been a shift towards legalization of marijuana for medical and recreational purposes. The medical use of cannabis is legalized in 33 states, 4 territories and the District of Columbia. Recreational use of cannabis is legalized in 11 states, 2 territories and the District of Colombia. 16 states and 1 territory (Virgin Islands) have decriminalized the use of cannabis (Marijuana Overview, NCSL, 2019) (Figure 1). In May 2015, Governor Alexander Garcia Padilla of Puerto Rico permitted the use of medical marijuana through an executive order and dispensaries became operational in 2017. In Puerto Rico the use of medical marijuana is limited to 15 medical conditions (Table 1) and is only permissible in non-smoking preparations. At the time of publication of this paper 92,499 patients are registered in the medical marijuana program (Marijuana Overview, NCSL, 2019).
Although these states and territories have moved independently to pass various legislations with regard to marijuana, the federal government and congress have taken steps that allow states to legally prescribe marijuana (Drug Alliance, 2015). The use, possession and sale of cannabis containing more than 0.3% of delta-9-tetrahydrocannabinol (THC) by content was illegal under federal law up to 2018, that changed with the passage of the United States Farm Bill (USDA, 2019). Under the Controlled Substance Act of 1970 marijuana was considered a schedule I drug until passage of the CARERS Act of 2015, that changed marijuana from scheduled I to scheduled II allowing for potential regulated use of medical marijuana. The same act excludes cannabidiol (CBD) from the definition of marijuana (DEA, 2020). Although changes have been made on the federal level towards marijuana, the federal government through the Centers for Disease Control and Prevention (CDC) remains steadfast that there is no clinical benefit to be had from the smoking of marijuana and its derivatives (DEA, 2020). There have also been some changes on the criminalization of marijuana under Federal Statutes. In 2013 the Justice Department adopted the Cole Memo that eased the enforcement of criminal laws with regards to the possession and use of marijuana. These restrictions would not apply if they include the production and use involved firearms, gang activities, sending proceeds to cartel and distribution to states where marijuana is still illegal (Rough, 2017). In 2018, the Cole Memo was rescinded restoring the authorization of the enforcement of federal marijuana laws even in states that have legalized marijuana in whatever form (Newman and McDonald, 2018). In the 2019 National Drug Assessment Analysis published by the Drug Enforcement Agency (DEA), marijuana is listed as the most commonly abused illegal drug in the United States. The same report further explained that states that have legalized the use of marijuana in any capacity have not indicated or regulated an acceptable level of THC and as such the United States is seeing a rise in more potent formulation of marijuana and marijuana products. The report further noted that the production of marijuana both legal and illegal is on the rise in the United States (DEA, 2020).
The information presented earlier outlined the challenges that legalization of marijuana poses for federal, state, territorial and tribal governments. This is further compounded by the fact that health experts cannot all agree on the benefits of the use of cannabis. This is under the backdrop of the approval that was granted by the Centers for Disease Control and Prevention (CDC) for two synthetic cannabis drugs (Dronabinol, Nabilone) in the treatment of cancer and other medical issues. While some efficacy of cannabinoids in randomized controlled trials has been demonstrated, there remain many safety concerns that still need to be addressed. Cannabinoid Hyperemesis Syndrome results from chronic cannabis use and produces cyclic episodes of nausea and vomiting accompanied by frequent hot bathing. This brief paper will attempt to examine one particular effect of the long-term use of cannabis, Cannabinoid Hyperemesis Syndrome (CHS) and its implications for Puerto Rico and the already strained healthcare system.
WHAT IS CANNABIS AND WHERE IS IT FROM?
Marijuana also referred to as weed, herb, pot, grass, bud, ganja, Mary Jane, Kush, and a vast array of other names and slang terms, is a greenish-gray mixture of the dried flowers of Cannabis sativa. The most potent psychoactive chemical in marijuana is delta-9-tetrahydrocannabinol (THC). THC is commonly found in the resins from the leaves and buds in the female cannabis plant. Besides THC cannabis trees contain some more than 500 other chemicals, in particular more than 100 of these compounds are chemically related to THC and are called cannabinoids (Mehmedic, 2010). There are others such phytocannabinoids in the cannabis plant such as cannabidiol (CBD) that has been shown to have opposing properties to that of THC (Voeks, 2014). Other cannabinoids may have synergistic or additive effects with THC and modify its actions when herbal cannabis is smoked. The brain produces a chemical call anandamides that is part of the cannaboid family. These anandamides are believed to play a role in memory, movement control and pain sensitivity (Manzanares et al., 2006).
The cannabis plant is native to Asia, in particular, China, India, Central Asia and Southeast Asia where it still grows wild. There are a number of species of the cannabis plant including C. sativa, Cannabis indica, Cannabis ruderalis, and C. sativa rasta. C. sativa has male and female varieties. The female plant is the primary source of marijuana and hashish. It is taller with denser foliage than the male plant and contains the buds containing high amounts of THC. C. indica, with higher THC content than sativa plant, is native to Himalayan regions, found mostly in Afghanistan and Morocco, where it is used to make hashish. C. ruderalis has minimal amounts of THC. C. sativa rasta plants found in Jamaica, Mexico and Africa, are similar to C. sativa but have even higher levels of THC (Voeks, 2014). Not only does THC content vary by the source but also by different preparations of cannabis. Nowadays the cannabis smoker may be exposed to doses of THC many times greater than 40 or 50 years ago which is important given that the effects of THC are dose related (Ashton, 2001).
HOW DOES CANNABIS PRODUCED ITS EFFECTS
The binding of cannabinoid compounds to and subsequent activation of cannabinoids receptors are responsible for their biological effects. Four subtypes of these receptors have been identified. Cannabinoid receptor type 1 (CB1) and type 2 (CB2) have been cloned (Mechoulam, 2000). These receptors are Gi/o-protein coupled receptors anchored in the cell membrane. The CB1 and CB2 receptors are coupled through G proteins, negatively to adenylate cyclase and positively to mitogen-activated protein kinase. The CB1 receptors are also coupled through G proteins to certain ion channels, and the same receptors can also activate adenylate cyclase (Mackie, 2008). Structurally these cannabinoid receptors consist of seven folded transmembrane helices with intra- and extracellular loops, functionally involved in signal transduction. CB1 is the most studied cannabinoid receptor and is located primarily in the brain but have some concentration in the spinal and peripheral nervous system, and minimal concentration in other non-nervous tissues such as endothelial cells, uterus and others. CB2 is found mainly in the immune system but has been found in other sites such as keratinocytes (Howlett, 2004).
THC has the ability to alter the functioning of the hippocampus and orbitofrontal cortex of the brain. This allows a person to form new memories and shift attentional focus. The use of marijuana causes impaired thinking and interferes with one’s ability to learn and perform complex tasks. THC also has the ability to disrupt the functioning of the cerebellum and basal ganglia. These areas of the brain are responsible for regulating balance, posture, coordination, and reaction time. This could explain why marijuana use may affect one’s ability to drive safely, may affect one’s ability to play sports or engage in other physical activities. THC also activates the brain’s reward center to include areas that regulate sex and eating. The activation of the reward center by marijuana leads to the release of dopamine at levels higher than those observed in natural stimuli. It is this hyper release of dopamine that contributes to the pleasurable “high” that individuals experience from the recreational use of marijuana.
CANNABIS AND PUERTO RICO
The Commonwealth of Puerto Rico (Esatdo Libre Asociado de Puerto Rico) is a US territory located in the Caribbean with a population of 3,449,000 as of the last US census in 2015, with an estimate of 3,195,153 as of July 2018 (US Census, 2018). There has been a decline in the population of Puerto Rico since 2003. From 2006 through 2015 Puerto Rico has experienced an overall decline of over 12% compared to an 8% increase in population size on the US mainland (US Census, 2018). As of 2016 the median household income in Puerto Rico is $20,078 compared to $57,617 in the US mainland. This puts the median income at a rate of 33% of that of the US mainland. The population in Puerto Rican is 99% Hispanic compared to 18% in the US mainland. As of 2018 the unemployment rate in Puerto Rico was 9.3% compared to 4.0% of the US mainland. This high unemployment rate coupled with low wages and declining and aging population puts Puerto Rico in a precarious position and adds to the already declining and bankrupt economy.
In the 5 populated US territories (Northern Mariana Islands, Guam, Puerto Rico, US Virgin islands, American Samoa) 4 have laws that permit some legal use of marijuana and 1 still maintain the use of marijuana illegal and also have some of the strictest penalties for its use in the entire United States. The Commonwealth of Puerto Rico in 2015 through an executive order permitted the legal use of marijuana for selected medical conditions (Table 1). The law only allows for the use of marijuana in pills, creams, patches and oral drops. Smoking and cultivation of marijuana remains illegal and is punishable under Puerto Rico Laws Ann. tit. 24 (Puerto Rico Case Law, 2020). Punishment ranges from 2 to 96 years in prison and fines up to $80,000 (Puerto Rico Case Law, 2020). Another executive order was signed in 2015 by Governor Alejandro Garcia Padilla asking judges not to enforce penal codes for possession of marijuana under 6 g.
Since the legalization of medical marijuana in Puerto Rico, the island territory has seen exponential increase and profits from the marijuana industry and is often referred to as the “legal marijuana boomtown.” As Puerto Rico is not a state, income made from individuals or businesses are exempted from paying federal taxes. This has made Puerto Rico a magnet for manufacturing businesses that account for over 44% of Puerto Rico’s Gross Domestic Product (GDP). Tourism is also a source of great revenue for the island territory, logging over five million tourists visit annually (Schain, 2017). Most of these visitors from the island are from the continental United States. Being a hot spot for tourism and manufacturing, Puerto Rico’s marijuana industry is tailored to capitalize on the economic strengths of the island. Apart from the generous tax and economic incentives to do business in Puerto Rico, the marijuana industry target those out of state visitors that visit the island territory and are in possession of a medical marijuana card from their home states.
CANNABINOID HYPEREMESIS SYNDROME (CHS)
First described in Australia in 2004, Cannabinoid Hyperemesis Syndrome results from chronic cannabis use and produces cyclic episodes of nausea and vomiting accompanied by frequent hot bathing. The nausea and vomiting ceases when marijuana use stops and when regular marijuana use resumes the nausea and vomiting returns (Allen et al., 2004). Currently, the mechanism of CHS is unknown. The clinical course of CHS can be divided into prodromal, hyperemetic and recovery phases. Chronic use of marijuana, often accepted as some months to years, predates the prodromal phase of CHS in which patients have some early morning nausea and vomiting for one or more days a week. The sight or smell of food often triggers the nausea but patients maintain normal eating patterns and appetite. Weight loss is the common presentation in this phase. Profuse vomiting without warning marks the hyperemetic phase. Nausea, sweating, colicky abdominal pain, and polydipsia are also common. During this period patients would have acquired the learned behavior of taking multiple hot showers that minimize symptoms. When these home remedies do not control symptoms or the vomiting becomes retractable the patients may then present to emergency departments. Intravenous fluid replacement is the hallmark of treatment, the vomiting often does not respond to antiemetic treatments. Most patients are discharged after 24 to 48 h of intravenous fluid replacement. These visits to the emergency departments become more common on a weekly or monthly basis for many years. Cannabinoid Hyperemesis Syndrome is a very difficult diagnosis to make as the symptoms are so generic and broad and as such often lead to delay in diagnosis. CHS is often confused with Cyclic Vomiting Syndrome. Cyclic Vomiting Syndrome is characterized by recurrent bout of nausea and vomiting accompanied by lethargy. The broad differential diagnosis of nausea and vomiting often leads to delay in the diagnosis of Cannabinoid Hyperemesis Syndrome. Cyclic Vomiting Syndrome shares several similarities with CHS and the two conditions are often confused. For the recovery phase, patients will need to stop the daily use of marijuana. However, there are two general types of patients that present with CHS, those that are in agreement that marijuana use is the cause of the nausea and vomiting and then there are those other patients who scorn the idea that cannabis was the cause of their vomiting syndrome. The latter group often refuses treatment and follows up. During treatment that includes the cessation of cannabis use, patients are given benzodiazepines for up to a maximum of two weeks from initial presentation to avert cannabis craving and withdrawal symptoms. Psychotherapy is also included in the treatment regimen to allow for support and success in stopping cannabis use (Bonnet and Preuss, 2017).
CANNABINOID HYPEREMESIS SYNDROME AND PUERTO RICO
The healthcare system in Puerto Rico is similar to the other 50 states and District of Columbia. In the 50 states and the district Colombia healthcare funding is unlimited but in the other 5 territories federal funding is capped, and when the funds are exhausted there are no additional funding. In Puerto Rico there is an aging population with an increase in migration to the continental United State by young adults (US Census Bureau, 2018). The island territory has over 80% of its population enrolled in welfare services. Medicare is the island territory’s major payor of healthcare services. However, since 1993 Puerto Rico has been privatizing healthcare, where private companies manage Medicare. This privatization has led to reduction in reimbursements, Medicare reimbursement rate in Puerto Rico is 70% less than that in the 50 US states and the district of Columbia. Puerto Rico shares the same percentage of Medicare enrollees as in the mainland US (Centers for Medicaid Services, 2018). These inherent problems in the healthcare system of Puerto Rico coupled by two consecutive hurricanes in 2017, and the numerous earthquakes and the Coronavirus pandemic have placed the already unstable healthcare system in a very precarious and uncertain position.
Cannabinoid Hyperemesis Syndrome does not have a unique ICD-10 code, instead it is accepted that the following codes will be used to designate and code for CHS: T40.7x1A, Poisoning by cannabis (derivatives), accidental (unintentional), initial encounter, and code R11.2, nausea with vomiting, unspecified, for the documented nausea and vomiting due to marijuana. For inpatient hospital care in an acute-care hospital, hospitals in Puerto Rico are reimbursed under the inpatient prospective payment system (IPPS). After the passage of the Consolidated Appropriations Act of 2016 (CAA 16; P.L. 114-113) of 2016, the reimbursement under IPPS for Puerto Rico’s hospitals equaled those of the 50 other states and the district of Columbia. Physicians are reimbursed on a fee for services schedule (The Medicare physician fee schedule (MPFS)). MPFS assigns relative value units to each of the approximately 7,500 service codes that reflect physician work (that is, the time, skill, and intensity it takes to provide the service), practice expenses, and malpractice costs. The value of reimbursement is adjusted based on geographic variation. There are currently 89 geographic regions under Medicare and Puerto Rico is its own locality. Therefore, reimbursement for Puerto Rico is unique and cannot be compared to the other 88 localities (CMS, 2019).
As outlined previously CHS treatment includes psychiatric management to include but not limited to benzodiazepines and psychotherapy. Puerto Rico has been experiencing a rise in mental illness and the hurricanes of 2017 further exacerbate this crisis. Utilization of mental health services has traditionally been low and insurance companies on the island normally do not facilitate the entry into mental health services. Among Puerto Ricans, there is a belief that spiritism, witchcraft, bad luck, fate, dana, and envy are important causative factors of mental illnesses. These believes could affect Puerto Ricans utilization of mental health services. Privatization of mental health services has shown a decreased in the quality, the access and the scope of mental health services. All these sociocultural factors coupled with the shortage of mental health providers on the island could further delay the effective treatment of Cannabinoid Hyperemesis Syndrome in Puerto Rico.
CONCLUSION
The legalization of marijuana in 33 states, 4 territories and the District of Columbia for medical use and for recreational use in 11 states and the District of Columbia have brought an increase in the use of cannabis in the United States. This increased use of marijuana has led to more patients presenting with Cannabinoid Hyperemesis Syndrome. Cannabinoid Hyperemesis Syndrome results from chronic cannabis use and produces cyclic episodes of nausea and vomiting accompanied by frequent hot bathing.. The nausea and vomiting ceases when marijuana use stops and when regular marijuana use resumes the nausea and vomiting returns. The treatment for this syndrome includes medical and psychiatric treatment. As with any new syndrome, medical billing and coding need to developed and agreed upon, especially as with regards to health care finance and reimbursement. Puerto Rico with the privatization of its health care system finds itself in a unique position with regards to reimbursement. The island has to develop a system for reimbursement and all individual medical payees on the island have to develop its own fee schedule. As with anything that includes various entities, agreement is often met with some challenges.
This information on Cannabinoid Hyperemesis Syndrome is provided so that the health care providers on the island territory can become aware of the disorder and remain vigilant in daily practice so as not to miss any case of Cannabinoid Hyperemesis Syndrome. On the other hand the island’s health care finance agency can use this information to start the discussion with the various approved medical payees on the island to develop a reimbursement strategy to address this disorder which if not already present on the island will certainly become more apparent in the near future.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Allen JH, de Moore GM, Heddle R, Twartz JC (2004) Cannabinoid hyperemesis: cyclical hyperemesis in association with chronic cannabis abuse. Gut 53(11):1566-70. |
|
|
Ashton C (2001). Pharmacology and effects of cannabis: A brief review. British Journal of Psychiatry 178(2):101-106. |
|
|
Bonnet U, Preuss UW (2017). The cannabis withdrawal syndrome: current insights. Substance Abuse and Rehabilitation 8:9-37. |
|
|
CMS (2019). Final Rule Addendum E, "Geographic Practice Cost Indices. |
|
|
DEA, Drug Scheduling (2020). |
|
|
Drug Alliance. S.683 CARERS Act (2015) |
|
|
Howlett AC (2004). Efficacy in CB1 receptor-mediated signal transduction. British Journal of Pharmacology 142(8):1209-1218. |
|
|
Mackie K (2008). Cannabinoid receptors: where they are and what they do. Journal of Neuroendocrinology 20:10-14. |
|
|
Manzanares J, Julian M, Carrascosa A (2006). Role of the cannabinoid system in pain control and therapeutic implications for the management of acute and chronic pain episodes. Current Neuropharmacology 4(3):239-257. |
|
|
Marijuana Overview National Conference of State Legislatures (2019). |
|
|
Mechoulam R (2000) Looking back at Cannabis research. Current Pharmaceutical Design 6(13):1313-1322 |
|
|
Mehmedic Z, Chandra S, Slade D, Denham H, Foster S, Patel AS, ElSohly MA (2010). Potency trends of Δ9-THC and other cannabinoids in confiscated cannabis preparations from 1993 to 2008. Journal of Forensic Sciences 55(5):1209-1217. |
|
|
Newman T, McDonald (2018); DPA Statement: This is Bad News For Civil and Human Rights- and Bad Politics for Team Trump. |
|
|
Rough L ((2017). The Cole Memo: What Is It and What Does It Mean. |
|
|
Puerto Rico Case Law (2020). |
|
|
Schain S (2017). How Puerto Rico Became Legalized Marijuana's Boomtown. |
|
|
USDA (2019). Agriculture Improvement Act of 2018: Highlights and Implications. |
|
|
Voeks R (2014). Cannabis: Evolution and Ethnobotany, The AAG Review of Books 2:2, 54-56 |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


