Full Length Research Paper

ABSTRACT
To describe and analyse, according to sociodemographic characteristics, the major risk factors for chronic non-communicable diseases (CNCDs) in adults aged over 18 years, residing in the municipality of Porto Velho, State of Rondonia, during 2006-2011. Prevalence of major risk factors for CNCDs were estimated within the population aged 18 and over, using telephone interviews with random samples of the population covered by landline telephone service in the municipality of Porto Velho, Rondonia, Occidental Amazon. A total of 12.071 interviews were conducted. Abusive alcohol consumption, overweight, and obesity were risk factors that presented the highest percentage increase of prevalence during the period studied. Among men, the prevalence ratio (PR) for tobacco use and obesity decreased with the increase in the years of schooling. Among women, tobacco use, overweight, and obesity were risk factors that decreased in relation to the level of education. It was observed an increase of the PR for both genders for overweight and low fruit and vegetable intake (LFVI). The results showed distinct health behaviors according to gender, age and education of the population; and highlighted the decrease tendency in tobacco use and the increase in alcohol abuse, obesity and overweight in the municipality of Porto Velho.
Key words: Risk factors, chronic non-communicable diseases, epidemiological surveys, health surveillance, cross-sectional studies, occidental amazon.
INTRODUCTION
Chronic non-communicable diseases (CNCDs) are currently the main cause for morbidity and mortality. They stand out among the major global public health problems, especially in countries with low and middle socioeconomic conditions (Schmidt et al., 2011; MS, 2013). According to World Health Organization (WHO) estimates for 2008 on the global burden of diseases, 63% of world deaths were attributed to CNCDs. It represents a total of 23 million deaths caused from cardiovascular diseases, cancer, chronic respiratory diseases, diabetes, neuro-psychiatric derangements, among other cause-specific of mortality (WHO, 2005). In Brazil, these statistics are even more relevant. In 2007, the burden of disease attributable to CNCDs reached 72% and the proportional mortality increased over three times between 1930 and 2006 (Malta et al., 2006; MS, 2013).
Epidemiologic studies indicated that those outcomes have in common some modifiable and non-modifiable risk factors and are responsible for 59% of the total potential Years of Life Lost (YLL) due to diseases and premature death (Moura et al., 2009; MS, 2013). Among the major risk factors, the following stand out: alcohol abuse, overweight, obesity, low intake of fruit and vegetables and sedentary lifestyle (WHO, 2002).
Prevention and control of CNCDs and its risk factors, associated to the planning of actions of health promotion targeted at the reduction of morbidity and mortality from chronic diseases are essential, especially to minimize the effects and consequences that the epidemic increase of those diseases may cause on the health and quality of life of the population (WHO, 2005; MS, 2013).
In 2006 the Ministry of Health of Brazil launched the system Vigilance of Risk Factors and Protection of Non-transmissible Chronic Diseases (VIGITEL) (MS, 2007), with the aim of monitoring the frequency and the indicators of CNCDs in the country, by means of Computer Assisted Telephone Interviews (CATI). Intended at the annual and continuous monitoring of the adult population aged over 18 years, resident in 26 states’ capitals and the Federal Capital, VIGITEL is an important instrument for health surveillance and a data source on morbidity and the population’s lifestyle, characteristics that are not captured by the current Mortality Information System (MIS) and the Hospitalization Information System (HIS) (Malta et al., 2008).
The use of telephone surveys with self-reported information has been increasing along the years due to the low cost and the speed of collected data processing and its analysis (Mokdad and Remington, 2010; Slade et al., 1995). A successful experience of the use of telephone surveys to be mentioned is the development of the Behavioral Risk Factors Surveillance System (BRFSS) developed in 1984 in the United States of America, being useful for researches in different health areas and countries (CDC, 2015).
In this context, the aim of this study was to describe and analyse, according to sociodemographic characteristics, the major risk factors for CNDCs within the adult population aged 18 years and older, resident in the municipality of Porto Velho, State of Rondonia during 2006-2011. This municipality has been impacted by different infrastructure projects such as energy production.
The selection of the municipality of Porto Velho for this study was due to its geographic location and its importance in the socio-environmental scenario of the Brazilian Amazon Region. Porto Velho is the capital of the State of Rondonia, situated in its Northern region, with an extension of 34.096 km2 and a resident population of 428.530 inhabitants (IBGE, 2010). It stands out for being an area that incorporates all the dimensions - social, economic, technological, cultural, environmental, political and health - addressed in the socio-environmental vulnerability debate. A study carried out on the burden of CNCDs in Brazil registered that the premature deaths attributable to this outcomes differ according to socio-economic levels, affecting in different proportions the populations with low socio-economic level and the regions of the country. When relating to poverty indicators and the precarious access to care, the North region presented the highest percentage of mortality attributable to CNCDs in the country (16%). Furthermore, hospitalization costs generated for the Public Health System (Sistema Único de Saúde – SUS) are among the highest (Bassanesi et al., 2008; IBGE, 2008; Schramm et al., 2004).
Therefore, the knowledge and the understanding of the dynamics of the major determinants of the CNCDs in the municipality are fundamentally important, in order to contribute for the formulation of public policies that promote the enhancement of quality of life to population from municipality and from Brazilian Amazon Region.
MATERIALS AND METHODS
The VIGITEL survey uses specific sampling procedures for each Brazilian State capital and the Federal District. For the municipality of Porto Velho, micro data was provided by the Data Processing Department of the Public Health System (DATASUS/Ministry of Health), containing the probabilistic sample of adult population aged over 18 years, resident in housing units with at least one landline telephone. The VIGITEL sampling was carried out in two stages. First, a random selection of housing units with residential and active telephone lines was made. On the second stage, a new random selection was made to elect the potential respondent individuals and who would agree to participate in the study. For the study period between 2006 and 2011, a drawing was made, obtaining approximately 5.000 eligible telephone lines annually. With the purpose of ensuring frequency estimates of risk factors with a maximum error of 2% and a confidence interval (CI) of 95%, a minimum was determined of 2.000 interviews carried out with adults aged over 18 years, resident in the municipality of Porto Velho. For specific estimates by gender, the maximum error expected was of 3% due to the similar proportions between men and women in the sample. No telephone lines were selected that were: related to firms; that were out of order; or that were inexistent. Lines excluded from the sample were those to which there was no reply after six calls, in distinct days and hours of the day (including Saturdays and Sundays and evening periods) and that probably corresponded to closed housing units.
For each period analysed, telephone interviews were carried out in different months, in intervals of six to eight months, performed by computer and immediately registered in digital media. The dimensions addressed by VIGITEL survey and used in this study were: demographic and socio-economic characteristics of individuals (age, gender, marital status, race/ethnicity, level of education, number of residents in the housing unit, number of adults and number of telephone lines); characteristics of the dietary pattern and physical activity, associated to the occurrence of CNCD (example: frequency of consumption of fruit/vegetables and food that is source of saturated fat, and frequency and duration of physical exercises practice and of watching television); height and weight referred and frequency of tobacco and alcohol abuse.
The following risk factors for CNCD were selected as dependent variables: tobacco use, overweight, obesity, low fruit and vegetable intake (LFVI), alcohol abuse and sedentary lifestyle. As independent variable, the level of education was selected with control of confounding for age. The dependent variables were divided in dichotomic categories (yes/no). The tobacco use was considered positive for daily or occasional smoking. In compliance with the WHO recommendations (WHO, 1995), overweight was defined according to the Body Mass Index (BMI) ≥ 25 kg/m2 and obesity to BMI ≥ 30 kg/m2. The LFVI was defined as the intake of fruit/vegetables lower than five times a day, and sedentary lifestyle was classified as no practice of physical activity during leisure time in the last three months, as well as no intense exercise carried out at work, not going on foot or on bicycle to work, and not being responsible for heavy cleaning at home. Abusive consumption of alcohol was considered as more than five units for men and more than four units for women on at least one occasion in the last 30 days, the consumption level defined as high risk for acute problems according to WHO criteria (WHO, 2000). Regarding information on level of education, it was divided into three categories (“0 to 8”, “9 to 11” and “more than 12 years”) and the age of the respondents was organized in six age groups (“18 to 24”, “25 to 34“, “35 to 44”, “45 to 54”, “55 to 64” and “Over 65 years”).
To estimate the frequency and the prevalence of risk factors from CNCDs for the municipality of Porto Velho it was necessary to apply weighting factors for complex samples. This technique is applied when the telephone coverage is not universal and it considers the socio-economic and demographic differences of each city, enabling statistical inferences for the total adult population. In this study, three weighting factors were used: the first factor corrects the greater chance that individuals of housing units with more than one telephone line had when selected for the sample. It is calculated according to the inverse of the quantity of lines in the respondent’s household. The second factor corrects the lesser chance that housing units with more residents had when selected for the sample and it was obtained according to the number of adults that live in the respondent’s household. The product of those two factors provides the sampling weight for more reliable estimates. The third and last weighting factor is denominated post-stratification. This technique allows carrying out the statistic inference for the total adult population of each city, by considering the estimates on the socio-demographic composition of the adult population with landline telephone and the total adult population. The variables considered in this socio-demographic composition were gender, age, and education level. The distribution of each estimated socio-demographic variable considered the distribution made for the Demographic Census 2000 and 2010 and the average annual variation (geometric rate) in the intercensus period. The post-stratification weight was calculated according to the rake method (Graham, 1983; Bernal, 2011) and is made available on the micro data provided by VIGITEL for the municipality of Porto Velho for all years studied.
Data analysis and processing used the software STATA version 12 to generate frequencies, proportions, confidence intervals (CI) of 95%, considering the described weighting factors. Chi-square trend test was calculated analysing the trend in the studied period. Prevalence Ratio (PRs) according to levels of education was estimated by gender, using the Poisson Regression, log-linear model, with significance level of 5%.
This manuscript is a part of project which was submitted and accepted by Research Ethics Committee of the Sergio Arouca National Public Health School (Comitê de Ética em Pesquisa da Escola Nacional de Saúde Pública Sergio Arouca – ENSP / FIOCRUZ) according to Resolution number 466/2012 from National Research Ethics Council (Conselho Nacional de Pesquisa – CONEP) with CAAE number 41732615.4.0000.5240.
RESULTS
In the period from 2006 to 2011 interviews were undertaken with a total of 12.071 adults aged over 18 years’ residents in the municipality of Porto Velho, State of Rondonia. Of the total amount, 5.132 respondents were men and 6,939 were women. For the whole period analysed the average duration of the interviews was 10 min. According to Brazilian Ministry of Health (2013) the average success rate between the quantity of lines sorted and the quantity of interviews undertaken was 72% and the average rate of refusal to participate in the study was 4% (MS, 2013).
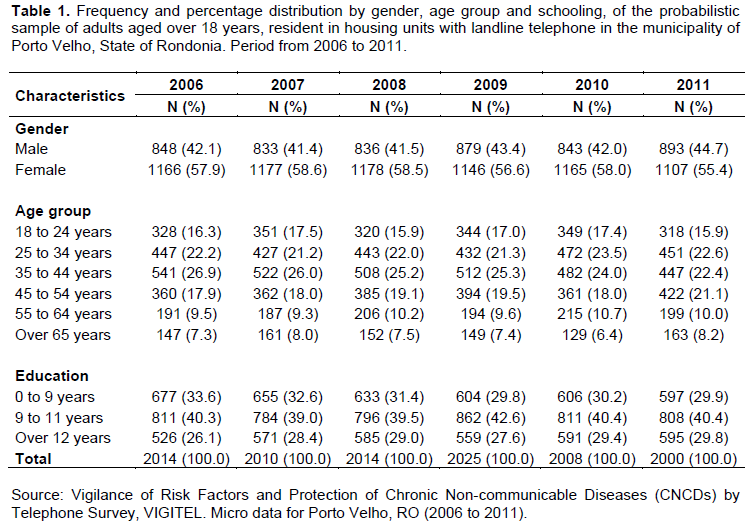
Table 1 shows the general characteristics of the probabilistic sample of the residents in housing units with landline telephone in the municipality of Porto Velho. For the years from 2006 to 2011, it was found that respondents were proportionally higher among women (58%), ranged from 35 to 44 years of age (25%) and from 9 to 11 years of schooling (40%).
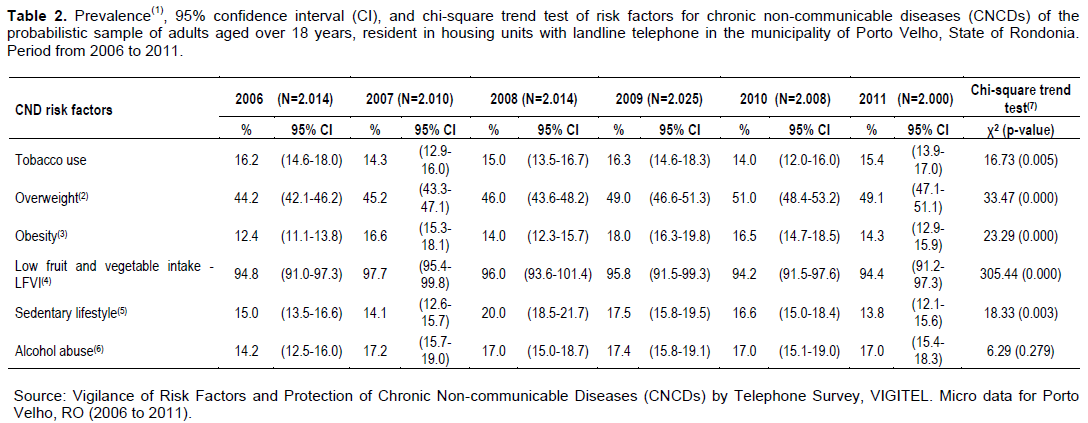
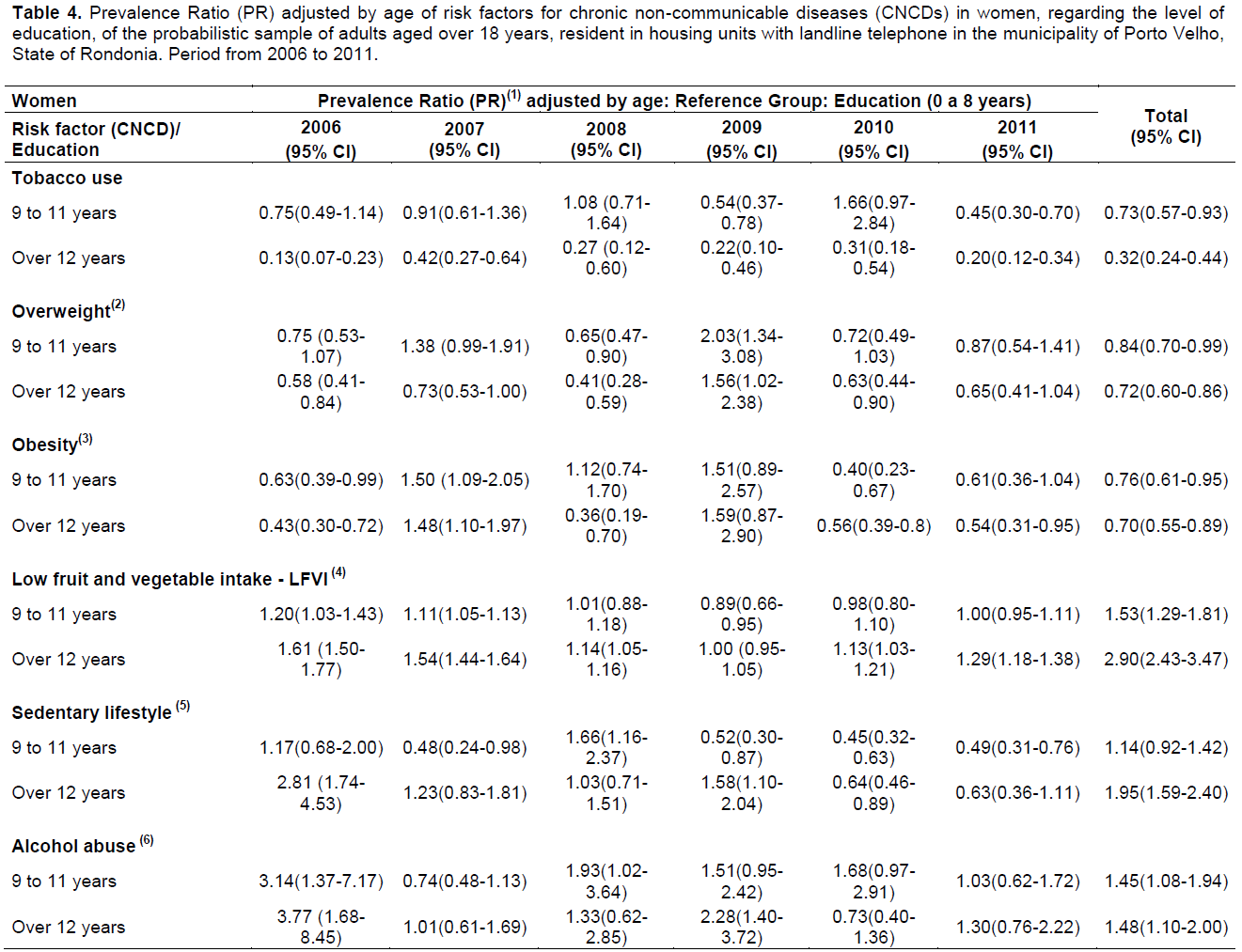
Considering the chi-square test the prevalence of major risk factors for CNCDs shown a linear trend and these results suggest increase in the prevalence between the years from 2006 to 2011. The exception was the abusive alcohol consumption which was not significant (p=0.279) and presented the highest percentage increase (16%) in the analysed period (Table 2). Tables 3 and 4 show the annual evolution of prevalence ratio (PR) of risk factors for CNDCs observing the differences between men and women according to levels of education adjusted by age.
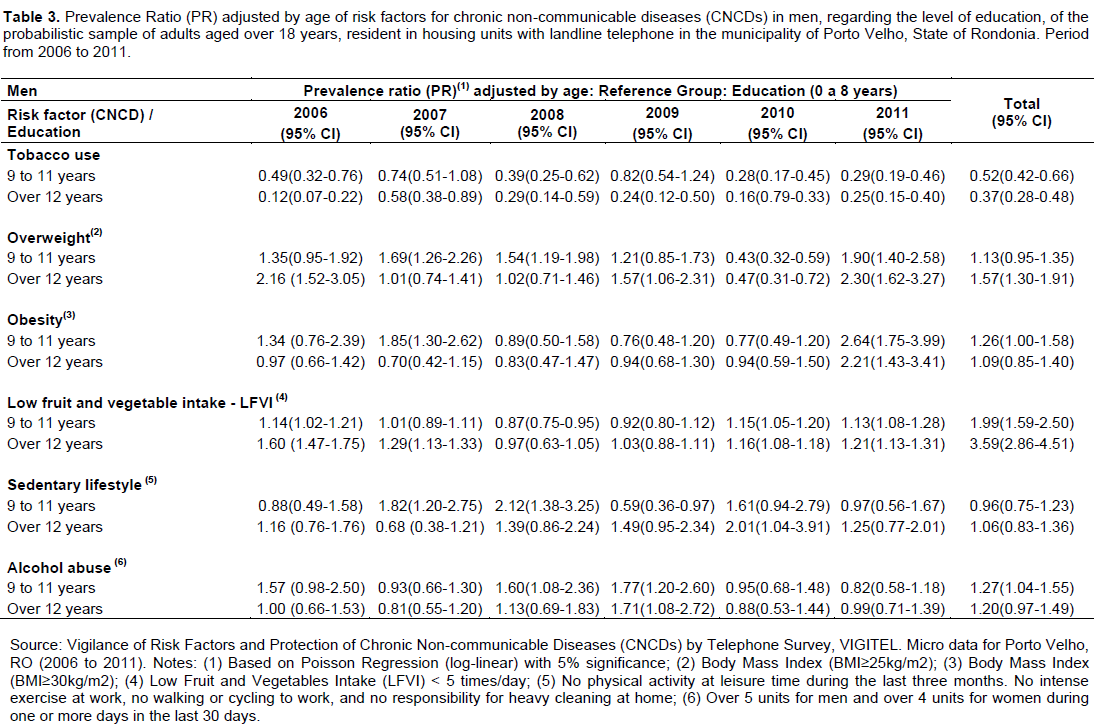

Among men, it was possible to verify that the PR for tobacco use and obesity decreased according to the increment in years of schooling. For the year 2011, the value observed among the respondents with over 12 years of schooling was 0.25 (95% CI 0.15; 0.40) for those who referred to tobacco use, and 2.21 (95% CI 1.43; 3.41) among the obese. Nevertheless, when analysing overweight and LFVI, the inverse behavior was observed, with the increase of PRs, according to the high education level. The values observed for the year 2011 for men with overweight and with more than 12 years of schooling was 2.30 (95% CI 1.62; 3.27). Among those who reported LFVI and high level of schooling, the value observed was 1.21 (95% CI 1.13; 1.31). Sedentary lifestyle and the alcohol abuse were not strongly affected by education. Differences between the years of 2006 and 2011 were not statistically significant.
Among women, the tobacco use, overweight, and obesity were the risk factors that decreased in relation to the years of schooling. For the year 2011, it was registered PR of 0.20 (95% CI 0.12; 0.34) for the tobacco use, 0.65 (95% CI 0.41; 1.04) for overweight, and 0.54 (95% CI 0.31; 0.95) for obesity. Risk factors that showed an increase of PR, regarding high levels of schooling, were the LFVI and sedentary lifestyle with values in 2011 of 1.29 (95% CI 1.18; 1.38) and 0.63 (95% CI 0.36; 1.11), respectively. As was observed among men, the alcohol abuse was not strongly affected by the level of education, as well as no significant statistic differences were observed between the years 2006 and 2011.
DISCUSSION
The results of the VIGITEL survey for the period from 2006 to 2011 showed important differences in the prevalence of risk factors of CNCDs considering gender and level of education. In the municipality of Porto Velho, the abusive use of alcohol stood out as the risk factor presenting the highest percentage increase (16%) of prevalence in the studied years. This finding corroborates with the 2nd National Survey on Alcohol and Drugs (II Levantamento Nacional de Álcool e Drogas - Lenad) for the period from 2006 to 2012, conducted in 149 municipalities in Brazil. The results showed an increase of 31% in the abusive consumption of alcohol in the Brazilian population, especially among young women (Laranjeira et al., 2013). In the United States of America, an assessment of the major deaths for the year 2000 concluded that 3.5% of the total number of deaths was attributed to the high level of alcoholic drinks consumption (Mokdad et al., 2004). The findings also match other studies conducted in Brazil and in the world (MS, 2004; CDC, 2004). It is important to highlight that this risk factor is associated to outcome such as hypertension, cirrhosis, cerebrovascular accident, cancer and the high levels of accidents and violence (Moura et al., 2009).
Obesity and overweight have also stood out in the municipality of Porto Velho, both in the percentage increase of the prevalence along the years and in differences observed between men and women. It was observed that the prevalence in men that referred to obesity decreased as there was an increase on the level of education. The opposite was observed for overweight, which was more prevalent among men with high level of education. Among women obesity and overweight showed similar pattern, being less prevalent among those who reported more years of schooling.
In this context, some studies indicate an association between overweight and socio-economic conditions. For example, a research carried out in Canada demonstrated that men with high socio-economic conditions had a higher BMI than those in lower conditions, whereas the inverse was found among women (Matheson et al., 2008). Furthermore, this difference between genders could be attributed to cultural issues. Women with higher level of education, when compared to men, tend to be more concerned about their body and consequently to take more care regarding food consumption, whereas men consume more fat food and alcoholic drinks. Data from the Research on Household Budget (Pesquisa de Orçamentos Familiares - POF) (POF, 2010) for the years from 2008 to 2009 corroborate with those findings, which overweight was diagnosed in approximately 50% of the men and women aged 20 years and over. In relation to the tendencies according to gender, the prevalence of overweight in the male population has increased approximately three times from 18% in 1974 to 50% in 2009 (IBGE, 1975; POF, 2010). Among women, the prevalence has doubled, from 29 to 48% in the same period. In relation to obesity, it increased four times among men (3 to 12%) and over two times among women (from 8 to 17%) (POF, 2010).
The analysis of the prevalence of the tobacco use in the municipality of Porto Velho showed a decrease along the years analysed and a significant relation with level of education. In both genders the prevalence of tobacco use decreased with the increase of years of schooling. According to the National Research on Health and Nutrition (Nacional de Alimentação e Nutrição, 1989) the prevalence of smokers decreased from 33% in 1989 to 17% in 2008, among individuals aged over 15 years, resident in different regions of Brazil (IBGE, 1989; Monteiro et al., 2007). This value is similar to those found in this study. In the year 2006, The prevalence of the tobacco use was of 16.2% (CI95% 14.6-18.0), decreasing to 15.4% (CI95% 13.9-17.0) in the year 2011, among individuals aged over 18 years resident in the municipality of Porto Velho. It is noteworthy that the intensity of the annual decrease of tobacco use in Brazil is considered one of the highest in the world (Monteiro et al., 2007).
In relation to the sedentary lifestyle, the prevalence observed for the years from 2006 to 2011 showed an increase. In this study, it was not possible to infer differences between men and women according to the level of education. In Brazil, studies indicate that men are more inclined to having a sedentary lifestyle when compared to women (Moura et al., 2008; MS, 2013). Sedentary lifestyle is related to the increase of obesity and to the development of different types of chronic diseases such as cardiovascular diseases, diabetes and cancer (WHO, 2002). In spite of the efforts on the promotion of physical activity the prevalence referred to sedentary lifestyle has not suffered significant changes in the last years (MS,2013).
According to WHO, the low intake of fruit and vegetables (LFVI) (daily intake less to 400 g or around five portions per person) is responsible for 2.7 million deaths worldwide annually: 31% from coronary ischemic diseases, 11% from cerebro-vascular diseases, and 19% from gastro-intestinal cancer (WHO, 2004, 2005).
In this study, it was found that an average of 95% of adults aged over 18 years resident in the municipality of Porto Velho in the years from 2006 to 2011 do not consume the recommended daily quantity of fruit and vegetables.
Furthermore, this study showed the increase of the prevalence of LFVI concerning the increment of years of schooling in both genders despite the well-established evidences of the benefits of a healthy diet in the prevention of CNCDs.
The limitations of this study are as follows: the use of the restriction of the sample to the individual resident in the municipality of Porto Velho with landline telephone, not considering the regional differences, especially in the North region of the country, regarding telephone coverage. Furthermore care should be reiterated about producing cause-effect inferences from cross- sectional methodological study design, as in the case of VIGITEL survey. Although stratification strategies and weighting factors have been used to adjust the estimates obtained from the telephone survey and to correct the differences between the population with and without telephone, no supposition may be made regarding the population of adults aged over 18 years without landline telephone (Moura et al., 2008; MS, 2013). It should be highlighted that since 2006 the data from VIGITEL are submitted to an enhancement process through studies of validation and comparison with other household surveys (Ferreira et al., 2011; Mendes et al., 2011; Gigante et al., 2011; Francisco et al., 2011).
Concerning the limitations of self-reported behaviors, with overreported or underreported, in general some studies using telephone surveys have reported high reliability and validity (Jackson et al., 1992; Bowlin et al., 1996). Multivariate regression was not applied because the major aim of this study was describe and analyse the contribution of each risk factor in separate. These analyses will be done in next studies.
Despite the limitations mentioned above, the VIGITEL survey permitted the description of the major risk factors for chronic non-communicable diseases in the muni-cipality of Porto Velho, State of Rondonia. Understanding the challenges and considering the social, economic, environmental and cultural difficulties to be faced in the Brazilian Amazon Region the survey is a valuable instrument to estimate the prevalence of modifiable risk factors and also to guide the development of public policies and health vigilance, as well as the identification of social inequalities, a fundamental condition for the definition of public policies in the North Region of Brazil.
Specified cardiovascular risk factors, namely over-weight, obesity, tobacco and alcohol intake, and particular unhealthy dietary and sedentary habits, are highly prevalent in the Brazilian Amazon Region, picturing a high-risk scenario for adverse cardiovascular outcomes. In the population of this region, distribution and prevalence of those risk factors have shown a relative stability over time, in the past decade, regardless educational level, gender and age groups, requiring special attention of public health authorities. Imple-mentation and dissemination of campaigns fostering healthy lifestyle habits are mandatory and urgent to reduce a prospective advancement of cardiovascular disease in this population.
CONFLICT OF INTERESTS
ACKNOWLEDGEMENT
REFERENCES
|
Bassanesi SL, Azambuja MI, Achutti A. (2008). Premature mortality due to cardiovascular disease and social inequalities in Porto Alegre: from evidence to action. Arq. Bras. Cardiol. 90:370-79. |
|
|
Bernal RTI (2011). Inquéritos por telefone: inferências válidas em regiões com baixa taxa de cobertura de linhas residenciais. 2011. Tese (Doutorado) – Faculdade de Saúde Pública, USP, São Paulo, 2011. View |
|
|
Bowlin SJ, Morrill BD, Nafziger AN, Lewis C, Pearson TA (1996). Reliability and changes in validity of self-reported cardiovascular disease risk factors using dual response" the Behavioral Risk Factor Survey. J. Clin. Epidemiol. 49:511-517. |
|
|
Centers for Disease Control and Prevention (CDC) (2015). Behavioral Risk Factor Surveillance System – BRFSS. |
|
|
Centers for Disease Control and Prevention. (CDC) (2004). Alcohol use among adolescents and adults--New Hampshire, 1991-2003. MMWR: Morbid. Mortal. Wkly. Rep. 53(8):174-175. |
|
|
Ferreira AD, Cesa CC, Malta DC, Andrade ACS, Ramos CGC, Proietti FA, Bernal RTI, CaiaffaI WT (2011). Validade de estimativas obtidas por inquérito telefônico: comparação entre VIGITEL 2008 e inquérito Saúde em Beagá. Rev. Bras. Epidemiol. 14(suppl.1):16-30. |
|
|
Francisco PMSB, Barros MBA, Segri NJ, Alves MCGP, Cesar CLG, Malta DC (2011). Comparison of estimates for the self-reported chronic conditions among household survey and telephone survey - Campinas (SP), Brazil. Rev. Bras. Epidemiol. 14(suppl.1):5-15. |
|
|
Gigante DP, França GVA, Sardinha LMV, Iser BMP, Velasquez Meléndez G (2011). Temporal variation in the prevalence of weight and obesity excess in adults: Brazil, 2006 to 2009. Rev. Bras. Epidemiol. Rev. Bras. Epidemiol. 14(Suppl 1):157-65. |
|
|
Graham K (1983). Compensating for missing survey data. Michigan: Ann Arbor; Institute for Social Research, The University of Michigan, 1983. |
|
|
Instituto Brasileiro de Geografia e Estatística (IBGE) Brasil (2008). Ministério do Planejamento, Orçamento e Gestão. Instituto Brasileiro de Geografia e Estatística – IBGE. Pesquisa Nacional por amostra de domicílios (PNAD 2008). Pesquisa Especial de Tabagismo (PETab). Rio de Janeiro: IBGE; 2009. |
|
|
Instituto Brasileiro de Geografia e Estatística (IBGE) (1975). Diretoria de Pesquisas, Coordenação de Trabalho e Rendimento. Estudo Nacional da Despesa Familiar (ENDEF) 1974-1975. |
|
|
Instituto Brasileiro de Geografia e Estatística (IBGE) (2009). Indicadores Sociodemográficos e de Saúde no Brasil 2009. Estudos e Pesquisas Informação Demográfica e Socioeconômica, número 25. 2009. View |
|
|
Instituto Brasileiro de Geografia e Estatística (IBGE) (1989). Sistema de Contas Nacionais – Reestimação da CEI de 2010 a 2013. |
|
|
Jackson C, Jatulis DE, Fortmann SP (1992). The Behavioral Risk Factor Survey and the Stanford Five-City Project Survey: A comparison of cardiovascular risk behavior estimates. Am. J. Public Health 82:412-416. |
|
|
Laranjeira R, Madruga CS, Pinsky I, Caetano R, Ribeiro M, Mitsuhiro S (2013). II Levantamento Nacional de Álcool e Drogas - Consumo de Álcool no Brasil: Tendências entre 2006/2012. São Paulo: INPAD; 2013. |
|
|
Malta DC, Cezário AC, Moura L, Morais Neto OL, Silva Junior JB (2006). Building surveillance and prevention for chronic non communicable diseases in the national Unified Health System. Epidemiol. Serv. Saúde 15:47-65. |
|
|
Malta DC, Leal MC, Costa MFL, Moraes Neto OL (2008). Inquéritos Nacionais de Saúde: experiência acumulada e proposta para o inquérito de saúde brasileiro. Rev. Bras. Epidemiol. 11(Suppl 1):159-67. |
|
|
Matheson FI, Moineddin R, Glazier RH (2008). The weight of place: a multilevel analysis of gender, neighborhood material deprivation, and body mass index among Canadian adults. Soc. Sci. Med. 66(3):675-690. |
|
|
Mendes LL, Campos SF, Malta DC, Bernal RTI, Sá NNB Velásquez-Meléndez G (2011). Validity and reliability of foods and beverages intake obtained by telephone survey in Belo Horizonte, Brazil. Rev. Bras. Epidemiol. 14(suppl.1):80-89. |
|
|
Ministério da Saúde (2004). Secretaria de Vigilância em Saúde/Secretaria de Atenção à Saúde/Instituto Nacional de Câncer, Coordenação de Prevenção e Vigilância. Inquérito domiciliar sobre |
|
|
Ministério da Saúde (1989). Política nacional de alimentação e nutrição. |
|
|
Mokdad A, Marks J, Stroup D, Gerberding J (2004). Actual causes of death in the United States, 2000. JAMA 291:1238-45. |
|
|
Mokdad AH, Remington PL (2010). Measuring health behaviors in populations. Prev. Chron. Dis. 7(4):A75. |
|
|
Monteiro CA, Cavalcante TM, Moura EC, Claro RM, Szwarcwald CL (2007). Population-based evidence of a strong decline in the prevalence of smokers in Brazil (1989-2003). Bull. World Health Organ. 85(7):527-34. |
|
|
Moura EC, Malta DC, Morais Neto OL, Monteiro CA (2009). Prevalence and social distribution of risk factors for chronic noncommunicable diseases in Brazil. Rev. Panam Salud Publica 26(1):17-22. |
|
|
Moura EC, Morais Neto OL, Malta DC, Moura L, Silva NN, Bernal R (2009). Risk and protection factors for chronic non communicable diseases by telephone survey - Vigitel Brazil – 2009. Rev. Bras. Epidemiol. 11(Suppl 1):20-37. |
|
|
Pesquisa de Orçamentos Familiares (POF) 2008-2009. Antropometria e Estado Nutricional de Crianças, Adolescentes e Adultos no Brasil. Rio de Janeiro: IBGE, Ministério da Saúde. 2010. |
|
|
Schramm JMA, Oliveira AF, Leite IC, Valente JG, Gadelha AMJ, Portela MC, Campos MR (2004). Epidemiological transition and the study of burden of disease in Brazil. Rev Ciência Saúde Coletiva 9(4):897-908. |
|
|
Schmidt MI, Duncan BB, Silva GA, Menezes AM, Monteiro CA, Barreto SM, Chor D, Menezes PR (2011). Chronic non-communicable diseases in Brazil: burden and current challenges. Lancet 377(9781):1949-1961. |
|
|
Slade GD, Brennan D, Spencer AJ (1995). Methodological aspects of a computer-assisted telephone interview survey of oral health. Aust. Dent. J. 40(5):306-10. |
|
|
VIGITEL Brazil (2006). Departamento de Análise de Situação de Saúde. Vigilância de Fatores de Risco e Proteção para Doenças Crônicas por Inquérito Telefônico, VIGITEL 2006. Brasília: DF; 2007. |
|
|
World Health Organization (WHO) (2005). Preventing chronic diseases: a vital investment. |
|
|
World Health Organization (WHO) (2002). The world health report 2002: reducing risks, promoting healthy life. Geneva: WHO; 2002. |
|
|
World Health Organization (WHO) (2005). World Health Organization. Prevenção de doenças crônicas, um investimento vital. Geneva: WHO Global Report, 2005. 36p. |
|
|
World Health Organization (WHO) (1995). Physical status: the use and interpretation of anthropometry. Report of a WHO Expert Committee. World Health Organ. Tech. Rep. Serv. 854:1-452. |
|
|
World Health Organization (WHO) (2000). International guide for monitoring alcohol consumption and related harm. Geneva: WHO, Department of Mental Health and Substance Dependence; 2000. (WHO/MSD/MSB/00.4). |
|
|
World Health Organization (WHO) (2004). Global strategy on diet, physical activity and health. Geneva: WHO; 2004 Document Number: WHA57.17. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


