Full Length Research Paper

ABSTRACT
Ethiopia has been implementing focused antenatal care package to reduce maternal and child deaths. The quality of antenatal care service has not being resolved widely due to unstandardized measurement. Hence, this study assessed determinants of focused antenatal care service satisfaction in Public Health Facilities of West Guji Zone, Ethiopia, 2018. A facility based cross-sectional triangulated with qualitative study design was conducted and multistage sampling techniques was used to select 810 pregnant women in West Guji Zone, from February 5th to 28th, 2018. Key informants were selected purposively for in-depth interview. Internal reliability test checked and Crobach‘s alpha became 86.5%. Data was cleaned, coded, entered to EPI INFO software, and then exported to SPSS version 21 for analysis. Predictors in multivariate logistic regression analysis determined where p value is less than 0.05. Qualitative data were thematically analyzed and triangulated for final conclusion. The overall prevalence of satisfaction was 66%. The predictors of overall satisfaction level were urban resident (AOR=1.91, 95%CI: 1.07-3.35), males’ sex service provider (AOR=0.42, 95%CI: 0.31-0.70), housewife in occupation (AOR=5.81, 95%CI :1.06-31.35), living alone (AOR= 0.16, 95%CI: 0.04-0.71), waiting time 30-60 minutes (AOR= 0.62, 95%CI :0.40-0.99), frequency ANC (AOR= 0.35, 95%CI: 0.16-0.76), care giving approach (AOR= 5.10, 95%CI: 2.10-12.51), and service provider respect (AOR= 2.41, 95%CI: 1.31-4.50). Three-in-ten study women were dissatisfied with the service they received and predicators were rural residence, male service providers, government employees, living alone, 30-60’ waiting time duration, frequency of antenatal care visit, care giving and respectful approach of service provider. Therefore, a multidimensional intervention is crucial to alleviate multifaceted negative outcomes in maternal health.
Key words: Antenatal care, child, maternal satisfaction.
INTRODUCTION
Pregnancy is one of the most important events that constitute powerful experiences in women. Despite pregnancy being a normal physiological process, it is associated with certain risks to health and survival both for women and infant; thus standard care is recommended, that is antenatal care (ANC). Antenatal care refers to care given to pregnant women and it includes education, counseling, screening, treatment, monitoring and promoting the well-being of the mother and fetus. Improving the quality of ANC and other reproductive health services has been fostering the uptake of services, and contributing to decrement of the adverse maternal health outcomes (WHO, 2016).
World Health Organization (WHO) has recommended a minimum of four ANC visits per pregnancy for an optimal birth outcome and to reduce maternal risks per pregnancy, especially for developing countries. In addition, WHO lunched focused antenatal care packages (FANC) guideline and which has been endorsed by many countries including Ethiopia. The main purpose of FANC is to give basic health care services including basic laboratory tests during all antenatal care (ANC) follow up, but, more attention is given in the first trimester of pregnancy (WHO, 2016). Basically, ANC visit is a key entry point for pregnant women to receive multiple ranges of health promotion, prevention, and curative services commonly on nutritional, anemia, HIV/AIDS, malaria, tuberculosis, and sexually transmitted infections. All these help women to improve their health and help them perceive visitation to health facilities as beneficial to both and fetus. However, merely implementing the protocol of different health service program is not a guarantee for measuring the overall satisfaction of service provided to women.
Client satisfaction could be the proxy measurement of service quality despite the quality issue being complex to estimate. Patient satisfaction is a subjective and dynamic perception of the extent to which the patient’s expected health care needs are met (WHO, 2000). However, the provision of high quality ANC is congruent to client’s satisfaction toward this care. High level of satisfaction among women with ANC services will increase the compliance of antenatal visits during pregnancy.
Globally, every year, over half a million women die as a result of childbirth or complication due to pregnancy, almost all (99%) of these deaths occurred in developing countries (WHO U, World Bank Group and the United Nations Population Division, 2016). Moreover, there are also complications such as obstetric fistulas, ruptured uterus, and pelvic inflammatory diseases. Eight-in-ten causes for maternal death are direct causes and of which severe bleeding disorder after women give birth is the single most scared complication claiming the lives of most mothers (WHO U, World Bank Group and the United Nations Population Division, 2016).
More than a million children lose their mothers each year due to maternal mortality. This contributed to 37% of death among under-five children. Despite different efforts have been made, maternal mortality ratio (MMR) is high in developing countries, with 66% in Sub-Saharan Africa and followed by Southern Asia. Currently, the two regions with the highest MMR are Sub-Sahara Africa and Oceania (WHO 2015, World Bank Group and the United Nations Population Division, 2016; UNICEF, 2015).
According to Ethiopia demography health survey (EDHS) of 2016, three-in-five women gets at least one ANC visit for their last pregnancy, while half them get four or more visits. In other word, nearly two-third of pregnant women is at high risk of pregnancy complications due to lack of antenatal care (Central Statistical Agency, 2016).
In order to alleviate the major contributions to maternal death globally, for two decades, many countries have adopted Millennium Development Goal’s (MDG) and have implemented many programs such as health themes like continuum care, focused ANC, and others to achieve the target for 2015. At the end of MDG’s, the maternal mortality ratio insignificantly reduced in Ethiopia. Currently, many countries, including Ethiopia, have been building the momentum of MDG’s and, has been adapting Sustainable Development Goal’s (SDG’s) by establishing a transformative new agenda for maternal health towards ending preventable maternal mortality targeted to be less than 70 per 100,000 live births by 2030 (UNICEF, 2015).
It is known that different efforts have been implemented worldwide in different proportion to achieve SDG’s target, which require reducing global MMR by an average of 7.5% in each year between 2016 and 2030. In other words, it requires more than three-times of the annual rate reduction observed (2.3%) between 1990 and 2015 (UNICEF, 2015). Most programs working on maternal health care like continuum cares which include FANC are based on the factors of three delays mechanisms for health facility delivery service such as health seeking of the community, infrastructural problems like road, lack of vehicles, transportation expenses, health professionals and facilities related problems.
Nevertheless, maternal death has been reported significant, especially in SSA and Asia regions. This might be due to low quality service in multiple dimensions. This contributes to low ANC service coverage, especially the forth visit due to low quality of service; this may be similar to the situation in West Guji Zone which was supported by 2018 annual report. Similarly, studies conducted in Al-Madinah Al-Menawarh and in Cameroon reported that nine-in-ten of the women were satisfied and only 4.7% expressed dissatisfaction (Sahar, 2012; Regional Hospital Bureau, 2015). A study conducted in Ondo state of Nigeria revealed that, more than half of the women were satisfied on the service they received (Fatile et al., 2016). The study conducted in Erbil city shows that, 89.7% of women were satisfied, and only 10.3% of them were dissatisfied (DJMS, 2010). Another study conducted in Pakistan reported that, general satisfaction of women was 70% on maternity services, where as 30% of women were dissatisfied (Mariam et al., 2012). Furthermore, one study in Gambia pointed out 79.9% of women was satisfied with the care they received at public health facilities (T-LLANH, 2012).
Different studies have been conducted in Ethiopia and reported the satisfaction level is found between 33%-82.6%. For instance, the study conducted in Jimma town revealed 235 (60.4%) of the women were satisfied and the rest 39.4% were not (Fantaye and Desta, 2014). A similar study conducted in Wolaita Zone, 301(82.6%) of the women were satisfied and the other 17.4% was dissatisfied (Bereket and Wondimagegn, 2013). The study conducted in Chencha Woreda of Gamogofa Zone figured out that client satisfaction on the ANC services received was 64.8% (9). In the same way, the study conducted Bahir-Dar special Zone has revealed that less than half (47.7%) of the pregnant women were satisfied with the ANC service provided by eight public health facilities (Tadesse and Kifile, 2013). Another study conducted in Bursa Woreda of Sidama Zone has reported the overall satisfaction of women on the service they received was found to be 33% (Tesfaye and Negessa, 2017).
According to the above studies, associated factors with satisfaction of focused antenatal care are geographical location of health facility, perceived quality of care, knowledge on antenatal care, educational level, setting of the facility, amenities, health education duration, service provider skills, privacy of care, service area space and neatness, communication, attitude towards FANC among nurses, availability of drugs and supply, getting information about the importance of breast feeding, waiting time, interpersonal aspect of care, management aspects, type of health facilities, educational status of women, monthly income of the family, type of pregnancy, history of still birth, absence of clean latrine, inadequate water supply, type of pregnancy, time to start first ANC follow up, residence, and parity. Therefore, this study assesses determinants of focused antenatal care service satisfaction to estimate quality and uniformity of maternal and child health service in public health facilities of Ethiopia, 2018.
MATERIALS AND METHODS
A facility based cross-sectional triangulated with qualitative study design was conducted from Feb 5th to 30th, 2018. The study was conducted in West Guji Zone. West Guji Zone is one of the 18 Zones in Oromia Region. The Zone town is 560 KM far from Addis Ababa, located in South Gediyo Zone and East of Yabelo. The total number of districts and cities in the Zone is nine, and two, respectively. The lower administrative body is kebele (the lower administrative unit in Ethiopia); hence in the Zone, a total of 196 kebeles are found. The rural kebeles are 166, while the urban kebeles are 30. In 2017, an estimated population of the Zone is 1,273,888, of which 608,918 are males and 664,970 are females.
Also, an estimated number of pregnant mothers are 43,138. The zone has 42 Health Centers, 166 Health Posts, and 2 hospitals that have been giving health services with 2 others under construction (as an unpublished report of West Guji ZHD shows).
The source populations of the study were all pregnant women attending antenatal care services at public health facilities in West Guji Zone, 2018. The study populations were all pregnant women attending antenatal care services in selected Public Health Facilities from Feb 5th to 30th 2018. For in-depth interview, MCH coordinators and Health Center Directors were interviewed. Those Pregnant women attending antenatal care services who came to selected health facilities who had lived for more than six months were included. As exclusion criteria, women who had lived less than six month in kebele, severely ill, unable to speak, and those with psychiatric problems were excluded.
A single population proportion formula of EPINFO software was used to determine sample size, using the following assumptions: proportion of pregnant women satisfied with antenatal care services (P) to be 60.4%. This is according to a study conducted in Jima town, Ethiopia, 2013 (Fantaye and Desta, 2014). In addition to this, Margin of error/relative precision (d) 0.05, confidence level 95% of CI (zα/2=1.96), design effect of 2, and finally non-response rate of 10% was added. Based on the above assumptions, the total sample size of the study was 810.
A multi-stage sampling technique was used; first, four districts were selected among nine districts in the Zone by simple random sampling technique of balloting which are: Abaya, M/Soda, Bule Hora and Kercha; then, four rural health centers were selected using simple random method from four districts, two urban health centers from Bule Hora and Kercha town, and one hospital from Bule Hora General Hospital. Finally, proportionally allocated sample sizes were made for each selected health facility. From the selected health facility, the participants who fulfilled the inclusion criteria were selected by simple random method based on ANC registration book number immediately after the exit of the service room, during data collection period until the allocated sample size reached. On other hand, purposive sampling procedures applied for the qualitative study. A total of six key informants were selected for in-depth interviewed; of these, four were from rural health centers and two from hospital MCH coordinators. This is because they could not have enough information related to the topics since they were closer to MCH services than others.
Mock type training was given to ten data collectors for two days who recruited from non-selected health facilities with educational level of diploma and above. Prior to the normal data collection time, pretest was conducted using 5% sample size on non-selected health facility and necessary correction has been made accordingly. After all secured ethical issues, data was collected for duration of 20 to 30 minutes per questionnaire in separate offices, immediately after a mother receive antenatal care service in Maternal and Child care unit (MCH). The expected responsibilities of data collectors, and supervisors were orientated such as collecting data based on the training, early preparation throughout data collection days, daily base submission of collected data for supervisory, random checkup of the progress of data collection, support data collectors whenever needed, providing the required materials as early as possible, checking and assuring the daily submitted questionnaires from data collectors, and finally all questionnaires were submitted to the principal investigator.
Data were collected using structured and unstructured interviewer-administered questionnaire. The structured questionnaire contained 42 items which are related to basic socio-demographic economic variables, health facility based obstetrics profile, current health condition, and measurements of satisfaction. The English language version questionnaire was translated to local languages, and again translated back to English language to check the consistency of data. Until now, there is no reference or gold standard instrument for the measurement of patient satisfaction on health care. The outcome variable satisfaction was assessed using a 5-point Likert scales, ranging from dissatisfied to fully satisfied (1 to 5 points), using 27 items. Also, Kruskas-Wallis H test was used to check the reliability of the questions for satisfaction scaling, and Cronbach alpha became 86.5% and internally reliable.
Open ended unstructured questionnaire developed based on three thematic areas such as health facility related (input), service provider related (process), and external infrastructure related. The in-depth interviews were conducted using principal investigators and the responses of the respondents were recorded with mobile recorder and notes were taken manually. Between the main thematic questions, certain necessary probing questions were asked in order to explore more ideas; and until the idea became saturated, interview of participants continued. In-depth interview were guided by standard interview guideline.
Finally, data were checked for completeness and consistency, and then coded and entered into Epi info version 7 software, after which it was exported to SPSS version 20 software package for analysis. The data was cleaned again through simple frequency and cross tabulation, using 5% of sample size of data entered, before further analyses were made. Univariate and bivariate analyses were computed to see the frequency distribution and to test the association between satisfaction level and selected independent variables. Factors associated with satisfaction on bivariate logistic regression analyses were identified, and variables with a p value of 0.25 or less than were candidate for multivariate logistic regression analysis. Finally, p value less than 0.05 in multivariate logistic regression analysis were considered predicator for satisfaction level of pregnant women to antenatal care service they received. In addition, the most important analysis output information were presented in the form of text, graph, and tables. Corresponding with the above, qualitative data were analyzed during and after data collection period manually using thematically approach. Finally, triangulation, both for quantitative and qualitative, was made for conclusion and recommendations.
RESULTS
Socio-demographic and economic characteristics
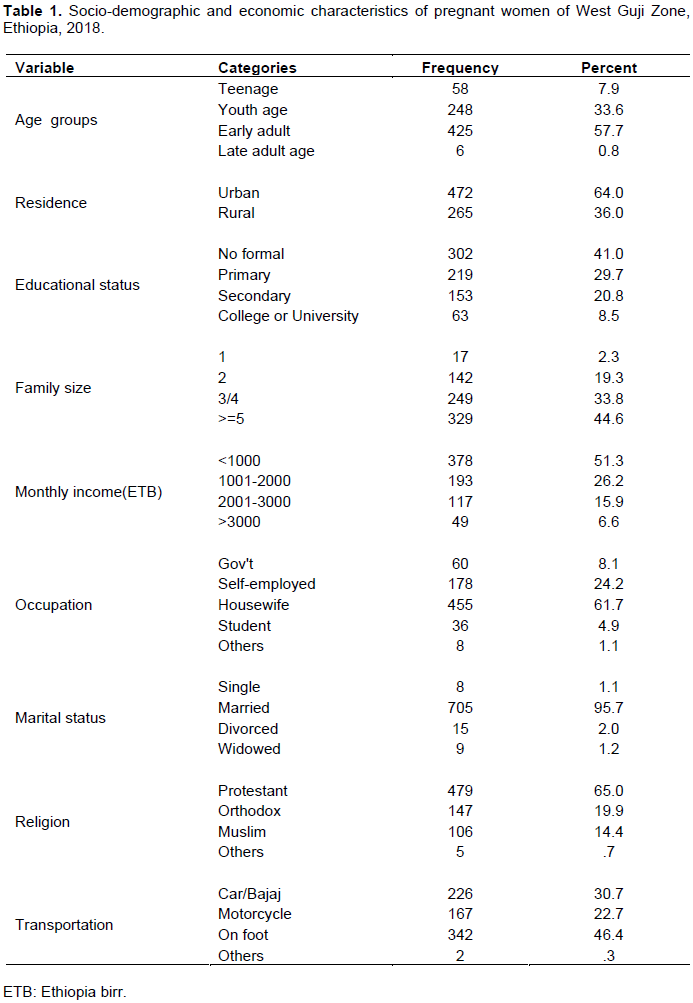
The total response rate of the study was nearly 91%, of which, those grouped under early adult age accounted for 57.7%, followed by youth age (33.6%), and the other 7.9% and 0.8% were for teenager and late adult age groups, respectively. Majority of women resided in urban setting (64%), and the other 34% were rural residents. Regarding educational status, 41% of women had no formal education, while others had primary (29.7%), secondary (20.8%), as well as College and above (8.5%) (Table 1).
Gynecological, obstetrics, and other medical history
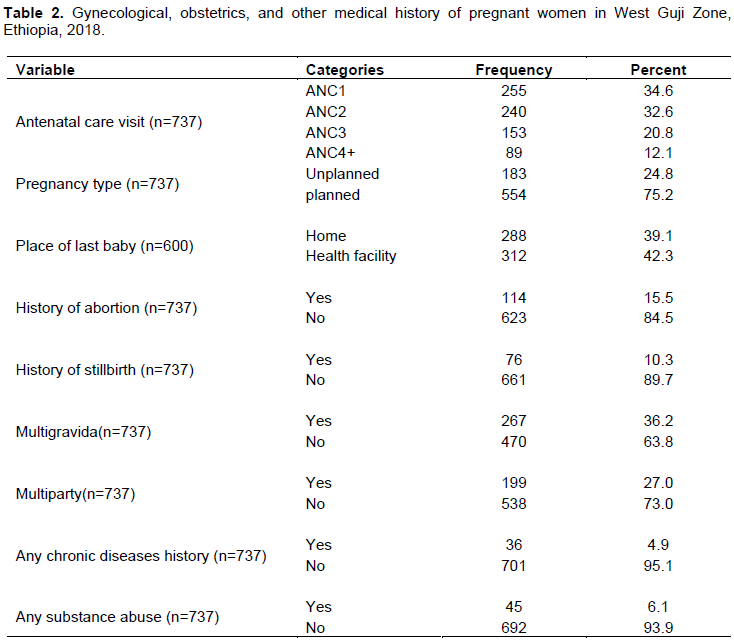
From the total number of pregnant women who visited the health facilities for antenatal care services, 34.6% were first time visitors, 32.6% were second time visitors, 20.8% were third-time visitors, and the 12.1% had visited four times and above. Obstetrics history of women shows, for instance; unplanned pregnancy rate was nearly 25%, last child delivery at home reported 39%, history of any type of abortion accounted for 15.5%, whereas still birth took 10.3%. In addition to this, 36.2% of study participants were multigravida mother, study participants who had chronic disease history in the past took only 5%, and those study participants who use any substance accounted for 6% (Table 2).
Overall and categorical satisfaction level
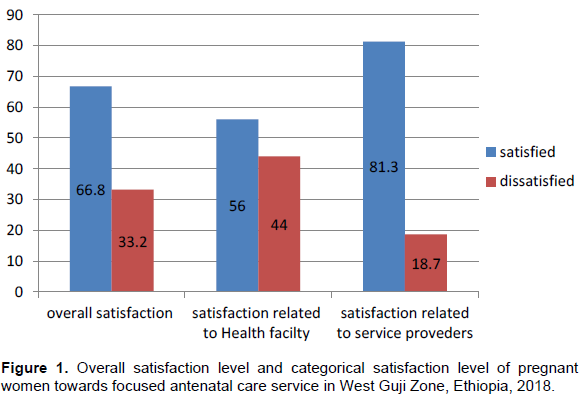
Overall satisfaction level of pregnant women towards the focused antenatal care service they received was nearly 67%; in other words, dissatisfaction was 33%, and major attributes for overall satisfaction of focused antenatal care service was in relation to service providers. Contrary to this, most attributes of overall dissatisfaction of mothers during antenatal care services were received from health facilities and transportation, i.e. structural dimensions (Figure 1).
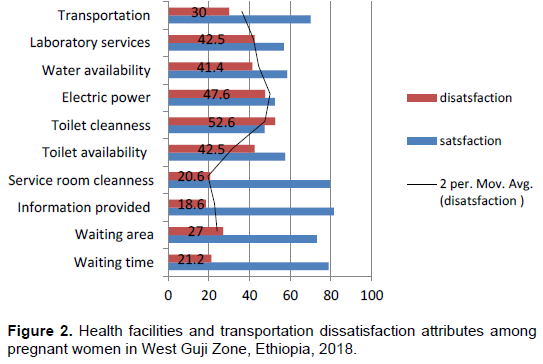
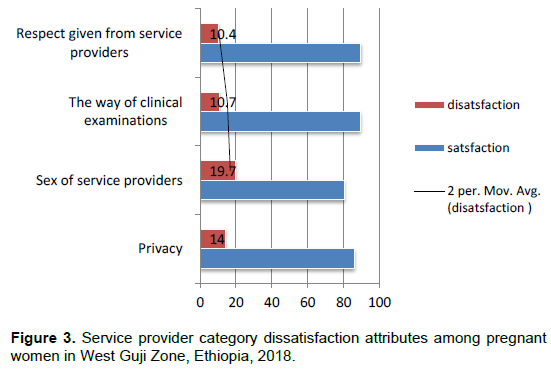
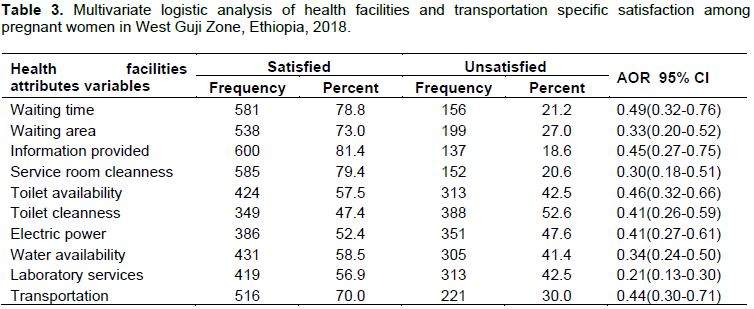
Specifically, major attributes for health facilities and transportation dissatisfaction were toilet related, electric power availability, laboratory service, water availability, transportation, waiting area, service room cleanness, and others (Figure 2). Also, regarding major dissatisfaction factors of service provider sides were sex of service provider, keeping client privacy during examination, the way of clinical examination, and respectful given to client during examination (Figure 3).
Multivariate logistic analyses for categorical satisfaction level
Health facilities and service provider specific multivariate logistic analysis
The concerns of women who received laboratory services and their satisfaction during antenatal care visit made their health facilities and transportation specific satisfaction rate reduced by 79% compared to those unsatisfied with laboratory service (
Multivariate logistic analysis for overall satisfaction level
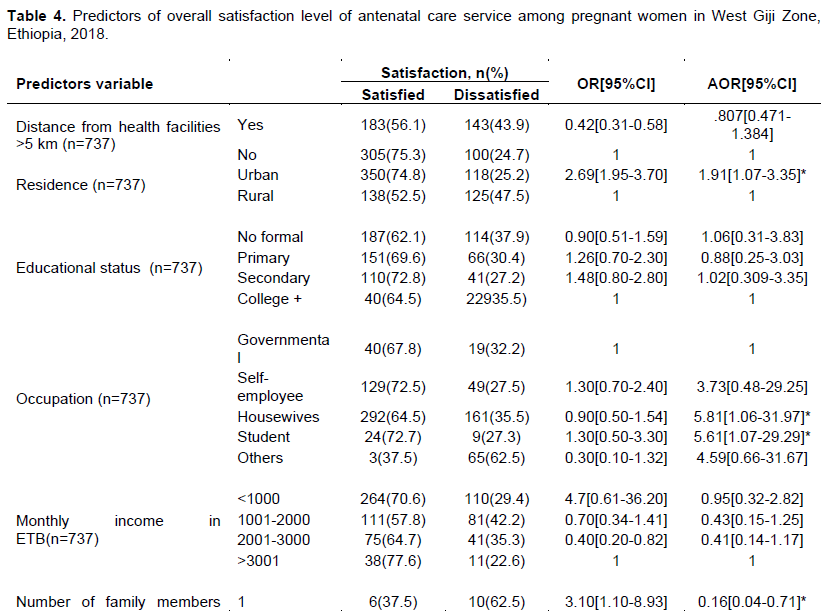
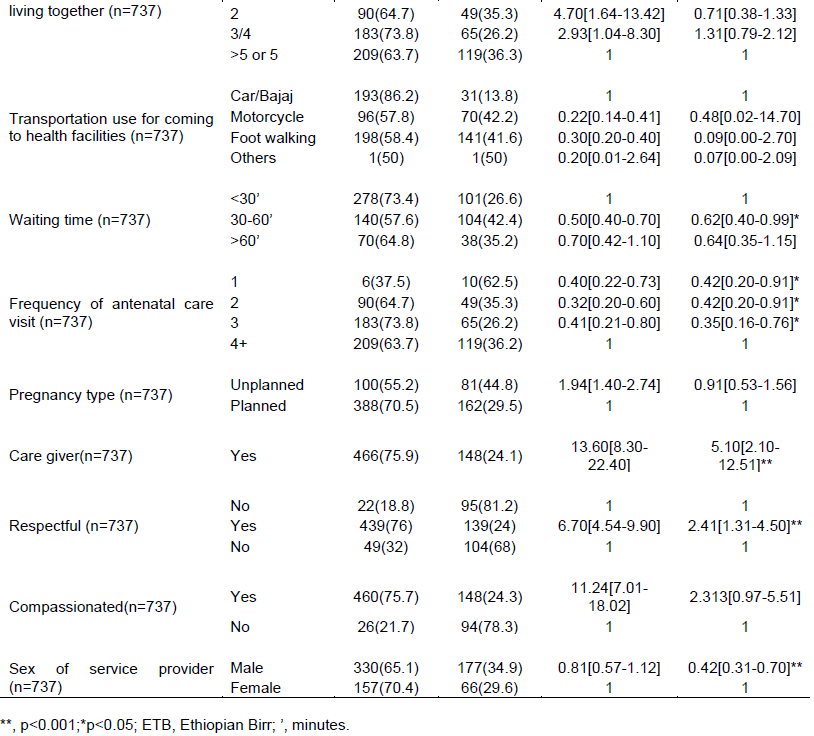
The resident setting of pregnant women who received antenatal care was significantly associated with an overall satisfaction. Women who resided in urban settings were probably 91% more satisfied than those who resided in rural settings (AOR= 1.9, 95% CI: 1.07-3.35). Similarly for occupation type; the odds of housewives and student women who are satisfied with antenatal care service received were 5.81 (AOR=5.81, 95%CI: 1.06-31.97), and 5.61 (AOR=5.61, 95%CI: 1.07-29.30) as compared to governmental employed women. So far, women who have been living alone decreased their overall satisfaction with 84% than pregnant women who live with five or more than five family members (AOR= 0.16, 95%CI: 0.04-0.71).
The probability of the overall satisfaction was reduced by 38%, when pregnant women waited for antenatal care service for the duration of 30-60 minutes than duration less than 30 minutes (AOR=0.62, 95%CI:0.40-0.99). In addition, women who received antenatal care services and prefer male gender service providers, were 58% less likely satisfied than their counterpart (AOR=0.42, 95%CI:0.31-0.70).
Regarding provider service approach, pregnant women who receive antenatal care service in the way of care giving approaches were five-times more likely to be satisfied than their counterparts (AOR=5.10, 95%CI:2.10-12.51). Similarly, pregnant women treated with respect were nearly two-times higher in overall satisfaction for antenatal care service than their counterparts (AOR= 2.41, 95%CI: 1.31-4.50).
Concerning the frequency of antenatal care follow up, pregnant women who visited the health facilities to receive their first, second, and third care service were less likely to be satisfied compared to those visiting for the fourth or more than four visits by 58% (AOR=0.42, 95%CI:0.20-0.91), 58% (AOR=0.42, 95%CI:0.20-0.91), 65% (AOR=0.35, 95%CI:0.16-0.76), respectively (Table 4).
Perceptions of MCH Coordinators and health facilities Directors towards FANC service satisfaction
Theme one: how health facilities affect the satisfaction level of women regarding the service they receive?
From four MCH Coordinators and Health facilities Directors who participated in the in-depth interviews, almost all of them had a similar understanding about the satisfaction of women towards FANC service and forwarded that, a 31 year old female health professional with a working experience of nearly 7 years, from one district said that,” to improve women satisfaction on FANC service, the service have to be given on time and the facility should work to reduce the overcrowded condition of clients as well as equip the health facilities with basic equipment like microscope, delivery couch and others.”
Theme two: how health professionals affect the satisfaction level of women on services they receive?
A male Director from one district, with BSc in nurse profession and four years’ work experience explained that,” in order to satisfy the pregnant women on the FANC service they receive, we have to carry out continuous health professional capacity building program such as on site or off-site training, and with safe, care giving, and respectfully behaved service providers.”. In addition a female delegated as Director in one district, 28years old with six years of experience stated that,” dissatisfaction on FANC service comes from mainly service providers who have negative attitude towards their profession.”
Theme three: How the external driving factors affect the level of satisfaction on ANC service?
A male MCH coordinator of 28 years revealed that, “the satisfaction of women on FANC services they receive could be fostered when service provider is motivated, trained, and equipped by government or non-governmental bodies.”
In summary, the measures one undertake as a mitigation to foster the satisfaction level of pregnant women towards FANC service is to encourage all MCH Coordinators and Health Facilities Directors”all stakeholders, governmental and non-governmental bodies to invest on the known gaps in an integrated approach and sustainable way.”
DISCUSSION
According to this study, the overall satisfaction level of focused antenatal care among pregnant women sub-optimal lies between 82.6 to 33%. The overall satisfaction level of this study is greater compared to the studies done in Sidama Zone, Gamo Gofa Zone, Wordha district in India, and El-Behaire (Sintayehu and Dirar, 2017, Tadesse and Kifle, 2013, Nemat and Vasent, 2017; Najinin and Vasent, 2012). The possible reason for this discrepancy might be due to the socio-economic and demographic characteristics difference, and the study participants of Sidima Zone, Gamo Gofa Zone, and El-Behaire were only from rural residents. This made the overall level of satisfaction to be underestimated as compared to the study, which include both the rural and urban residents in order to reduce over-and under estimation of the result. On the contrary, the overall satisfaction level of this study is lower than the studies conducted in different areas such as the study in Wolaita Zone in Ambo, also in South West Nigeria (Bereket and Wondimaghghn, 2013; Sanusi et al., 2015; Amsalu et al., 2015). The assumptions behind the difference might be the study participant’s socio-economic and demographic variability, measurement tools applied for scaling overall satisfaction level, the infrastructures and human resource capacity in Wolaita Zone as well as South West Nigeria might be relatively good compared to West Guji Zone.
Concerning the factors that predicate the level of overall satisfaction towards focused antenatal care service received by pregnant women, the study found that the resident setting of mothers is significantly associated with overall satisfaction of focused antenatal care services received; that is, women who reside in urban setting are probably more (91%) satisfied than those who reside in rural setting. This finding is similar to that of Gamogofa Zone Chencha district and Cameroon (Sintayehu and Dirar, 2017). This might be due to the fact that urban women have good access to information, service from experienced health care providers, well-equipped health facilities, high level of education, and have good economic level than rural women.
As Regards occupation of women, housewife and students in occupation are more satisfied than women employed in governmental organizations. The possible reason might be those pregnant women who are housewives and students get adequate rest and time for advice than the others; thus, enhancing their satisfaction towards the care they received.
In terms of the number of family members, pregnant women living alone are more dissatisfied than women living with more family members. It was believed that every person is better off living with one or more family or non-family members, this provides supports such as information exchange, economic support, psychological support, and others when needed. Therefore, these might enhance the satisfaction level of women living with other family members, directly or indirectly.
With reference to gender of service providers, the study shows that pregnant women who receive care from females care providers are more satisfied than services received from males care providers. This is due to the fact that female service providers might be more respectful, better care givers and compassionate with pregnant women than males service providers. In addition to this, there might be some male service providers with negative attitude towards working in maternal health care unit, since most cases were women related.
Regarding duration of waiting time taken, this study has pointed out those pregnant women who took less than 30 minutes for focused antenatal care service are more likely to be satisfied than those who took between 30-60 minutes duration. This is consistent with the study reported in South West Nigeria which stated that women are expected to attend antenatal care service at health facilities within 30 minutes to make them satisfied. The study is and also in line with the study reported in Bahir dar (Tadesse and Kifle, 2013; Sanusi et al., 2017). This similarity is due to general in all service provision sectors whereby clients want to receive the expected service in short time duration and this make the clients to have frequent revisit and also paves the way for cordially inviting other clients too.
This study also showed that, frequency of ANC follow up determined the overall satisfaction level of focused antenatal care which is supported by this study. During three consecutive antenatal care follow up (first, second and third) the overall satisfaction became less and less than the forth focused antenatal care follow up time. This is in line with Ethiopia demographic health survey report of 2016 which states that the quality of antenatal care depends on the qualification of health provider as well as the number and frequency of antenatal care visit (Central Stastical Agency, 2016). Conversely, this finding is paradox with the study done in Gamogofa Zone which revealed that the first antenatal care visit women are more likely to be satisfied than revisits (Niguse et al., 2017). This might be due to West Guji Zone Public health facilities. The implementation of focused antenatal care has faced a problem, not all service providers were trained on focused antenatal care. This is because, WHO focused antenatal care guideline recommends that all pregnant women should receive standard services during the first visit more than other visits; and this increases their satisfaction level of the services they receive (WHO, 2016).
Moreover, this study revealed that pregnant women who receive focused antenatal care service in a respectful way and care giving approach of service providers were two and five _times more satisfied than their counterparts, respectively. This finding is in line with the study reported in Jimma Zone which revealed the highest satisfaction due to respectful and supportive approach service provision of service providers (Fantaye and Desta, 2014). This in accordance with one Pakistan study, which revealed, interpersonal aspects of service provider predicate the satisfaction level of service taker (Mariam et al., 2012). This is owing to the fact that in social and psychological point of views, if you give respect and care to anybody, it will create a positive or satisfaction feeling. Thus, if service providers offer their services in a respectful and care giving approach, the satisfaction of pregnant women towards the care they received will increase.
In other words, the qualitative section of this study showed that in order to foster satisfaction of women on FANC service, the internal environment of health facilities should be fulfilled like medical and laboratory equipment, update training provision for service providers, employment of health profession field should be based on their needs. All these needs integrate efforts of different stakeholders, likewise health and medical sciences education sectors, health offices and, others. These all explored views have supported the quantitative section findings so far, directly or indirectly.
CONCLUSION AND RECOMMENDATION
The quality of maternal health services is significant and complicated because it has no specific factors to determine it. That is, factors are interrelated with each other directly and indirectly. According to this study, the quality of maternal and health services are still compromised due to several unresolved factors. For instance, the overall dissatisfaction has statistically significant with rural resident women, governmental employed women, pregnant women living alone, male sex service providers, waiting time for the care taking 30-60 minutes, frequency of antenatal care visit, and service provider respectful or disrespectful and care giving. As regards the qualitative part, it is concluded with the explanation of one health facility Director who says,” in order to satisfy pregnant women on FANC services they receive, we have to carry out health professional capacity building programs such as training, and the health facilities should be equipped with basic equipment like microscope, delivery couch, and others.” Therefore, to summarize the findings from both sides (quantitative and qualitative), the factors enhancing quality of services are multifaceted, that is, human factors, infrastructural factors, and antenatal care visit protocol factors. Of these factors, human factor is the most important. Thus, it is recommended that special attention should be given to the rural dwellers and provision of continuous capacity building programs for service providers. Also, further insight into local based-approach on antenatal care services and protocol should be carried out.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Amsalu N, Yabo E, Ejeta C (2015). Assessment of Quality of Antenatal Care (ANC) Service Provision among Pregnant Women in Ambo Town Public Health Institution in Ethiopia, 2013. America Journal of Nursing Sciences 4(3):57. Crossref |
||||
| Bereket Y, Wondimagegn MT (2013). Utilization of antenatal care and their satisfaction with delivery services in selected public health facilities of Wolaita Zone, Southern Ethiopia. International Journal of Scientific Technology Research 2(2):12. | ||||
| Central Statistical Agency (CSA) (2016). Ethiopia Demographic and Health Survey of. 2016:59. https://dhsprogram.com › pubs › pdf | ||||
|
Regional Hospital Bureau (2015). Department of Surgery and Obstetrics-Gynecology UoB B. Department of Gynecology and Obstetrics, Regional Hospital Bureau. Perceptions of antenatal care services by pregnant women attending government health centers in the Buea Health District, Cameroon: a cross sectional study. Pan Africa Medical Journal 9. |
||||
| DJMS Z (2010). Women's satisfaction about MCH care services provided to pregnant attends antenatal care units in Erbil city. Zanco Journal Medical Science 1:14. | ||||
|
Fantaye CFA, Desta W (2014). Satisfaction with focused antenatal care service and associated factors among pregnant women attending focused antenatal care at health centers in Jimma town, Jimma Zone, South West Ethiopia; a facility based cross-sectional study triangulated with qualitative study. BMC 7(164). Crossref |
||||
| Mariam Ashraf FA, Khan AR (2012). Assessing women's satisfaction level with maternity services: Evidence from Pakistan. International Journal of Collaborative Research on Internal Medicine Public Health 11:4. | ||||
| Najinin K, Vasent ZQS (2012). Vasant Wagh. Patient Satisfaction on Maternal and Child Health Services. Indian Medical Gazette 45 p. | ||||
| Nemat IA, Vasent RME (2017). Pregnant Women's Satisfaction with the Quality of Antenatal Care At Maternal and Child Health Centers in El-Beheira Governorate. Journal of Nursing and Health Science 6(2):11. | ||||
|
Niguse M, Shimeles TMB, Ololo, FT (2017). Quality of Antenatal Care Services in Demba Gofa Woreda, Gamo Gofa Zone, Rural Ethiopia. Health Science Journal 11:17. Crossref |
||||
|
Fatile OA, Akpor OA, Okanlawon FA, Fatile EO (2016). Women and Providers' Perception, Attitude and Satisfaction with Focused Antenatal Care in Ondo State. Nigeria International Journal of tropical disease and health 3:12. Crossref |
||||
| Sahar ML (2012). Women's Satisfaction with the Quality of Antenatal Care at the Primary Health Care Centers in Al-Madinah Al-Menawarh, KSA. Life Science Journal 4:9. | ||||
|
Sanusi M, Ibrahim MB, Hadiza U, Abdullahi, Mohammed Bukar (2017). Clients' perception of antenatal care services in a tertiary hospital in North Eastern Nigeria. International Journal of Reproduction, Contraception, Obstetrics and Gynecology 7 p. Crossref |
||||
|
Sintayehu AA, Dirar AGA (2017). Quality of Antenatal Care Service in Public Health Facilities of Chencha District, Gamo Gofa Zone, Southern Ethiopia. MOJ Women's Health 3:4. Crossref |
||||
|
Tadesse EM, Kifle Y (2013). Quality of antenatal care services at public health facilities of Bahir-Dar special Zone, Northwest Ethiopia. BMC Health Services Research (443):13. Crossref |
||||
|
Tesfaye T, Negessa L (2017). Maternal Antenatal Care Service Satisfaction and Factors Associated with Rural Health Centers, Bursa District, Sidama Zone, Southern Ethiopia: A Cross-sectional Study. Journal of Women's Health Care 6(2) Crossref |
||||
|
T-Llanh Y-JC (2012). Women's perception of antenatal care services in public and private clinics in the Gambia. International journal of Quality in Health care 6:24. Crossref |
||||
| UNICEF (2015). Transforming our world: the 2030 agenda for sustainable development 29 p. | ||||
| World Health Organization (WHO) (2015). World Bank Group and the United Nations Population Division. Trends in Maternal Mortality 1990 to 2016:92. | ||||
| World Health Organization (WHO) (2000). Clent Satisfaction Evaluations.38 p. | ||||
|
World Health Organization (WHO) (2016). Recommendations on antenatal care for a positive pregnancy experience. 172. |
||||
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


