Full Length Research Paper

ABSTRACT
An epidemiological survey was conducted on prevalence of malaria among children aged 1-15yrs in south east Nigeria. A total of 498 children were surveyed for malaria and other morbidity indicators. Out of these, 369 which include 195 (52.8%) males and 174 (47.2%) females were from experimental household and 129, including 66 (51.2%) males and 63 (48.8%) females from control household. Before the deployment of Lambdacyhalothrin-treated household items - curtains, mats and blankets, the total malaria prevalence and all the morbidity indicators examined were (P<0.05) high among the sexes in both the experimental households and their control. By the end of the study, there was significant (p<0.05) decrease in malaria prevalence and all the associated morbidity indicators among the sexes in the experimental households. The total percentage prevalence decreased from 69.7% to 39.4%, 63.2% to 33.3 and 69.2% to23.1% for males and 77.4% to 27.6%, 63.2 to 26.3 and 50% to 28.6% for female of ages 1-5, 6-10 and 11-15 respectively. The mean morbidity indicators dropped from 12.9≡13 to 1.9≡2; 9 to 0.6≡1 and 6.5≡7 to 0.6≡1 in sampled children of same age bracket but in the control households, they still remain on the increase (p<0.05). The least malaria prevalence was 59.1% recorded among female infants and mean morbidity indicator remained was 6.5≈7. The prevalence of malaria was comparable by sex and age and found to be statistically not significant p>0.05.
Key words: Malaria, insecticide, lambdacyhalothrin, morbidity.
INTRODUCTION
Although the overall life expectancy is pointing upwards all over the world, the situation of malaria-related mor-tality remains a hidden global scourge. The most common cause of hospital admission in children and in all age groups continuously reducing the population globally (Molineaux, 1988). Malaria is a mosquito-borne infectious disease of human and other animals caused by a eukaryotic protist of the genus Plasmodium. It is endemic in tropical and sub tropical regions, including America, Asia and Africa. It is more prevalent in sub-Saharan Africa where 85 to 90% of malaria deaths occur (Layne, 2006). Some scientist believed that one in every two people who have ever lived has died of malaria (Michael, 2007). According to WHO (2005), malaria causes an estimate of 250 million cases of fever annually and other morbidity indicators (Beare et al., 2006). It further estimated that 655,000 people died of malaria in 2010 (WHO, 2010). Currently, the 2012 meta-study from the University of Washington and University of Queensland found this number of deaths in 2010 to be higher with 1,238,000 people (Global Malaria Mortality, 1980 to 2010; Christopher et al., 2012). Breman (2001) argued that the precise statistics are hardly known because many cases occur in rural areas where people do not have access to hospital or means to afford health care; as a result, the majority of cases are not documented.
Malaria is present in both rural and urban areas of the countries in Africa, though the risk is lower in urban cities (Keiser et al., 2004). Provost (2011) reported that by 2010, countries with the highest death rate per 100,000 populations are Coted’lvoire with 86.15, Angola 56.93 and Burkina Faso 50.66 all in Africa. This is attributed to consistent temperature, high humidity, significant amount of rainfall, along with stagnant waters in which mosquitoes larvae readily mature, providing them with the environment they need for continuous breeding (Prothero, 1999) and thick vegetations which prevail in African countries.
Greenwood et al. (2005) state that majority of the cases were found in children less than five years old and pregnant women. Christopher et al. (2012) found out that 90% of malaria-related deaths occur in sub-Saharan Africa, with approximately 60% of deaths being young children under the age of five. In areas of high stable transmission of malaria, the incidence of clinical malaria peaks between one and five years of age.
Moreover, the increased speed at which strains of malaria parasite that are resistant to malaria drugs have developed especially in Africa makes the perspective even more difficult. The people of this area have been under serious dilemma concerning malaria disease. Among the strategies proposed to face this worrying situation, insecticide treated bed-net has been intensively functional (Sexton, 1994). Binka et al. (1996) also reported that the introduction of insecticide treated bed-net was associated with 17 to 33% reduction in all-case child mortality, respectively.
Other research trials using insecticide treated bed nets have demonstrated reduction in morbidity and mortality (Greenwood, 1987; Alonso et al., 1991; Nevill et al., 1996; Brieger et al., 1996, 1997). Lengeler (1998) reported that between 3.5 and 6.9% lives were saved per 1000 children protected with insecticide treated bed nets per year (based on four large scale trial in Africa). Nevertheless, due to some underlying reasons: (i) bed-net normally have very fine mesh netting (1.2 to 1.5 mm) which is sufficiently small to prevent passage of mosquitoes (Gahard, 2005). This also offer protection against a small sand flies and biting midges, but in hot climate, poor ventilation through fine mesh netting is a serious disadvantage (Gahard, 2005), it also makes sleep difficult due to heat; (ii) nets are too expensive in some areas (Winch et al., 1997); (iii) if several people especially children are sharing one net, this may result in overcrowding, part of their bodies may protrude under the net during the night (Gahard, 2005). For these reasons, people started having ill feelings about using them, hence the need for an alternative method to prevent resurgence of mosquito bites and subsequent increase in malaria infection.
This work is the result of a field survey in which lambdacyhalothrin treated curtains, mats and blankets were deployed inside living household in Oruku, Enugu State, and Eastern Nigeria as alternative strategy for malaria control. The aim is to determine an alternative to insecticide treated bed-nets using lambdacyhalothrin treated household items, including curtains mats and blankets in controlling mosquitoes’’ bites and to find the effect on morbidity indicators among children in Oruku.
MATERIALS AND METHODS
Study area
This study was conducted in four out of the six villages of Oruku community, Ameke, Isienu, Obinagu and Eziobodo in Udi local government area all in Enugu State. The state is located on latitude 6.5000° N and longitude 7.5000° E and has a population of 722,664 according to the 2006 Nigerian census. The mean daily temperature is 26.7°C (80.1°F) and is at its highest between March and November. Enugu State is hot all year round. Rainy season and dry seasons are the only weather periods that recurs in the state. The average annual rainfall is around 2,000 mm. There is harmattan season between December and January. It has land mass, covered by bushes, streams, rivers, stagnant water and these are features that promote insects’ breeding especially mosquito.
Sample selection and data collection
A total population of 498 children including 369 (195 males and 174 females) from experimental household and 129 (66 males and 63 females) from control household was sampled for malaria and other morbidity indicators. Different sampling methods were used in selection of samples. These include random sampling method and systematic sampling method (Ali, 1996).
Structured questionnaire was administered to the selected children and/or parents of infants in face to face encounters to get information on ages, sex, and frequency of occurrence of symptoms/signs. Some teachers and head teacher of Community Primary School Oruku were also interviewed to collect data on school absenteeism. All the sampled children were also tested for malaria prevalence using blood sample collected from their index fingers. The blood was collected on slide and taken to Parasitology Research Laboratory of University of Nigeria, Nsukka for possible malaria parasite and species identification using Giemsa and Leishman’s stain and data documented for both experimental and control household. This was done three times monthly. After the first malaria prevalence test, lambdacyhalothrin treated household item curtains, mats and blanket, were deployed to experimental household as a malaria control strategy. The household items were treated such that a target dose of 75 cl of 0.001 mg/L or 0.025 mg/L concentrations of lambdacyhalothrin were absorbed by each of the control items achieved.
Statistical analysis
Data collected were analyzed according to sex of the sampled children in both experimental households and their control. Data on malaria prevalence study from sampled male and female children in both experimental households and their controls were analyzed using chi-square (c²) statistic. Data on the effect of treatments with local mats, curtain and blankets treated with lambdacyhalothrin, on malaria prevalence were analyzed using analysis of variance (ANOVA). Differences between treatment and effect means were detected using the least significant difference (LSD) or protected LSD after a preliminary f-test (Obi, 2002).
RESULTS
Malaria prevalence study
Before control material deployment
The prevalence of malaria infection in Oruku was investigated among children in both the experimental households and their control. The study was based on the sex of children between the ages of 1 month to 15 years. It was done before and after the deployment of the lambdacyhalothrin treated materials.
Table 1 shows the result of the study prior to the deployment of the treated items according to the sex of the sampled children in both the experimental households and their control within the various villages. The table revealed that malaria prevalence varied among the sexes in both the experimental households and their control. In experimental households, a highest prevalence of 100% was recorded among both male and female infants of ages 1 to 5 years in Isienu and Obinagu villages, respectively. The same 100% prevalence was noted among elderly males (11 to 15 years) in Eziobodo village. The least prevalence among all the sexes was 33.3%. It was recorded among elderly females in Eziobodo village. In control households, a 100% prevalence was also recorded among elderly females (11 to 15 years). 33.3% prevalence was also the least prevalence observed among the sampled children in the control households. It was recorded for infant females in Isienu village.
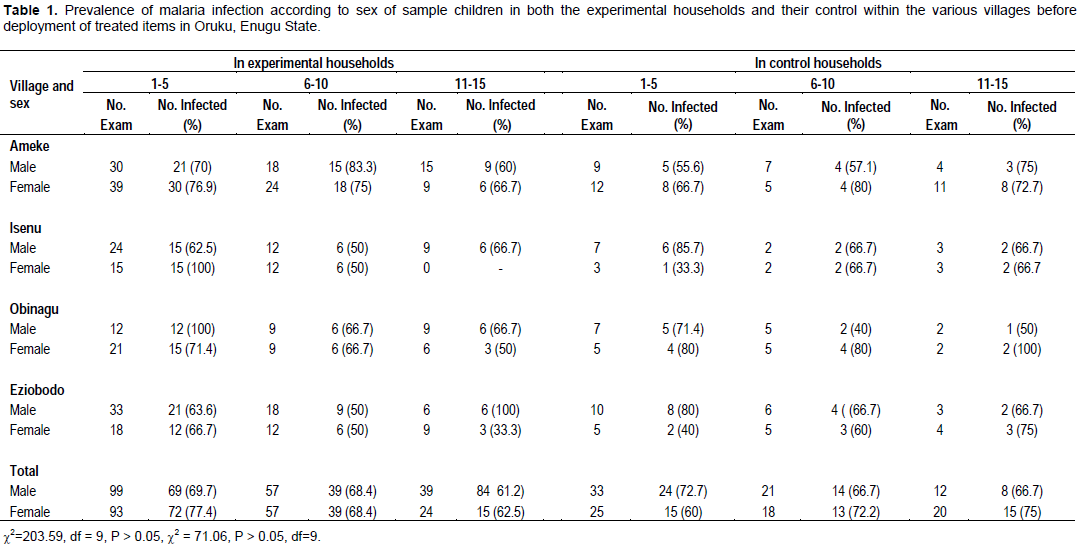
However, a chi-square analysis of this data showed that sex was not significant in the distribution of malaria infection among children examined in Oruku (c2 = 203.59, df = 9, P > 0.05) (c2 = 71.06, df = 9, P > 0.05).
After control material deployment
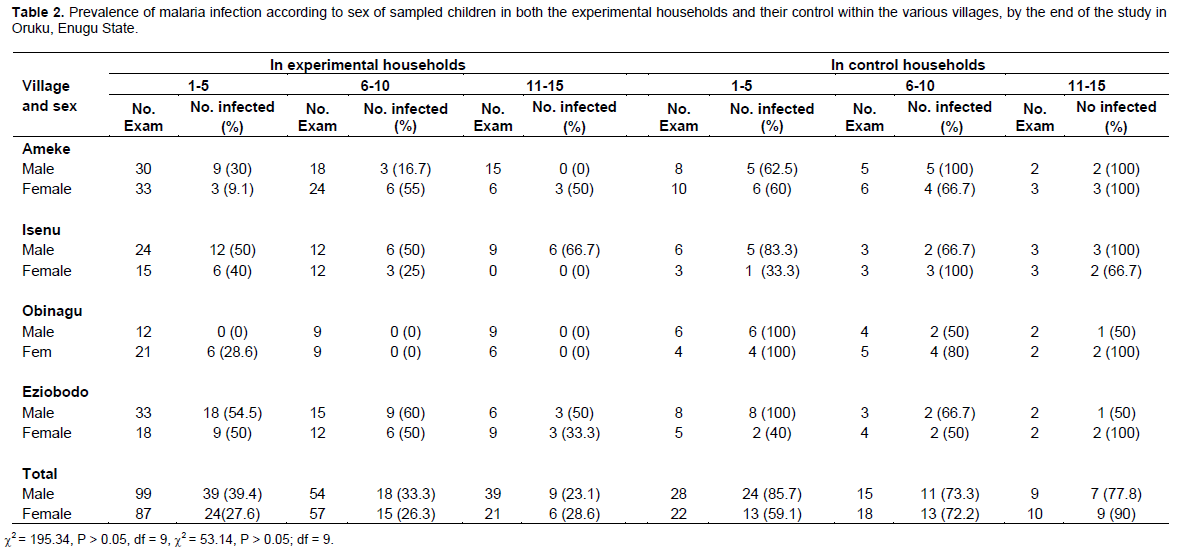
By the end of the study, the impact of the treated household items based on the sex of sampled children showed that in the experimental households, total percentage prevalence for malaria was reduced from 69.7 to 39.4%, 63.2 to 33.3 and 69.2 to 23.1% for males and 77.4 to 27.6%, 63.2 to 26.3 and 50 to 28.6% for female of ages 1 to 5, 6 to 10 and 11 to 15, respectively. 0% (zero) prevalence was recorded for infant males (1 to 5 years) in Obinagu village and for both elderly males and females (11 to 15 years) in Ameke, Obinagu and Isienu villages, respectively (Table 2). While in the control households, the least prevalence was 33.3% recorded among infant females in Isienu village. Nevertheless, sex was still not significant in the distribution of infection and reduction in prevalence is accordingly (c2 = 195.34, p > 0.05, df = 9) (c2 = 53.14, P 0.05, df = 9).
Fever among other symptoms/signs
Table 3 shows the symptoms/signs and their frequency of occurrence reported by the sampled children in experimental households and effect of lambdacyhalothrin treated household items on this frequency of occurrence, one and two months after deployment of the treated items. It was observed that rashes/itching, fever, cough, stomach ache, and loss of appetite were the most frequent malaria symptoms among children within ages 1 to 5 years. The symptoms differed significantly (P = 0.05) from each other. On the other hand, the mean number of occurrence of these symptoms within one month, for children within this age group who had these symptoms and hence an indication of having malaria infection before deployment of lambdacyhalothrin treated household items, was approximately 13 times within one month compared to 3 and 2 times in one and two months after the deployment of protective items to the study households. There was statistically significant (P = 0.05) decrease in the number of occurrence from 13 times to 2, two months after, an indication that the treated items were effective. Calculating the relative importance of the symptoms/signs in the community, it was found that fever (26.76%) was the commonest and thus the most important symptom among children of ages 1 to 5 years, while rigor (2.11%) was the least common.
Also, it was noticed that headache, fever, loss of appetite and stomach-ache, were the most frequent malaria symptoms among children within ages 6 to 10 years (Table 3). They differed significantly (P = 0.05) from each other. The mean number of occurrence of these symptoms for children within this age group, who had these symptoms, hence an indication of having malaria infection before deployment of protective items was 9. However, one and two months after deployment of protective items, the mean number decreased to approximately one, which was a statistically significant (P = 0.05) decrease, indicating that the protective items were effective. When the relative importance of the symptoms/signs among children of this age group in the community was calculated, headache (36.36%) was found to be the most common and thus the most important symptom, while rigor (1.01%) was the least common.
For group 11 to 15 years (Table 3), headache and fever were observed to be the most frequent malaria symptoms. These two symptoms differed (P = 0.05) from others in their frequency of occurrence. It was also noticed that the mean number of occurrence of these symptoms for children within this age group before deployment of protective items was approximately 7. One and two months after the deployment of the protective items, the number statistically (P = 0.05) decreased to approximately 1. An indication that lambdacyhalothrin treated items were effective. This is because there was no reported case of self medication or health seeking movement by the sampled children, after the treated items were deployed. For the relative importance of the symptoms and signs among this age group in the community, headache (57.14%) was the commonest and thus the most important symptom while catarrh (1.43%) was the least common.
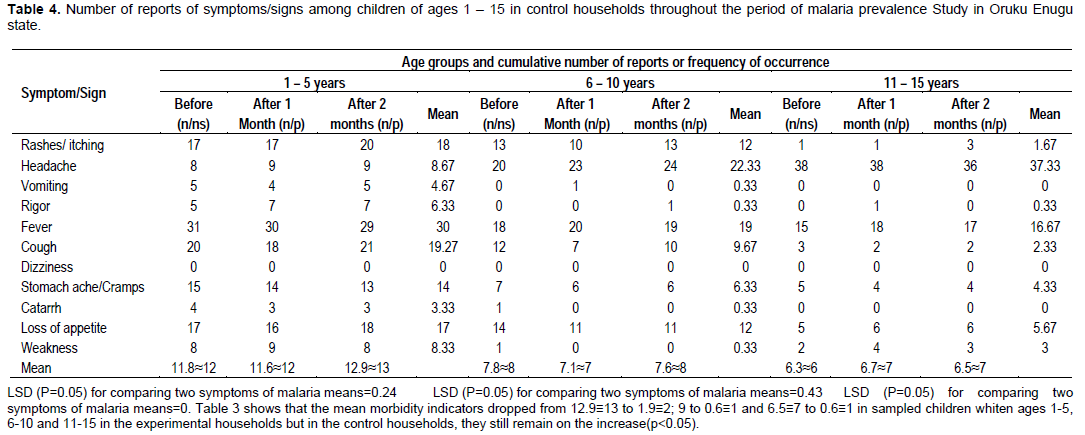
On the other hand, a different result was recorded in the control households. Table 4 shows the frequency of occurrence of fever and other symptoms at the start of this study and throughout the study period. It was observed from analysis of data, that the frequency of fever and other symptoms was statistically (P = 0.05) high at the start of this study. It further showed that these symptoms/signs remained on the increase throughout the period of the study. For ages 1 to 5, the mean number of occurrence of these symptoms/signs within one month, was 12 at the beginning of the experiment, but statistically increased to 13 (P = 0.05) by the end of the experiment. For ages 6 to 10 and 11 to 15, the mean number of occurrence at the beginning of the experiment were 6 and 8, respectively and by the end of the study, the number remained statistically (P = 0.05) at the same 6 and 8.
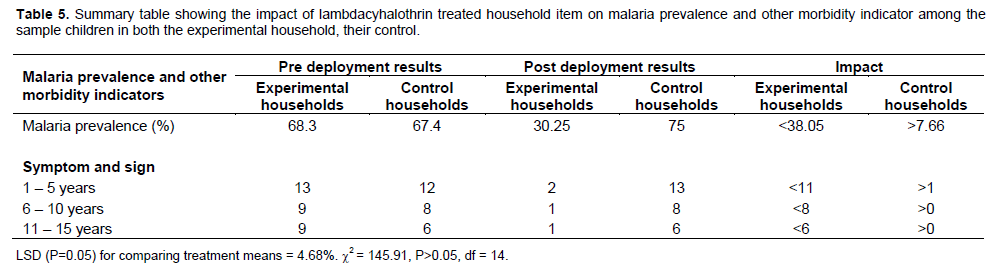
Table 5 shows that an impact of <38.05% was made in experimental households post deployment of lambdacyhalothrin-treated items, while in control households impact of 7.6% was made. The table also show the impact made on morbidity indicators among children in the experimental households as <11, <8, <6 for children within ages 1 to 5, 6 to 10 and 11 to 15. However, the opposite was noted in the control household. It was >1, >0 and >0 for children of same age group. These evidence indicated that lambdacyhalothrin-treated household items were effective.
DISCUSSION
The result of this study showed that household items including curtain, mat and blanket treated with 0.01 and 0.025 mg/L concentration of lambdacyhalothrin had significant effect on malaria prevalence, fever and other symptoms and signs of malaria among both male and female children of Oruku. Prevalence of 69.7, 63.2, and 69.2% for males and 77.4, 63.2 and 50% for female of ages 1 to 5, 6 to 10 and 11 to 15 indicated that malaria infection was highly endemic in Oruku community especially among children. And reduction in prevalence from 69.7 to 39.4%, 63.2 to 33.3 and 69.2 to23.1% for males and 77.4 to 27.6%, 63.2 to 26.3% and 50 to 28.6% for female of ages 1 to 5, 6 to 10 and 11 to 15, respectively (P < 0.05) is quite encouraging. It indicated that curtains, mats and blankets treated with lambdacyhalothrin were as efficacious as other insecticide treated materials.
Many researchers have demonstrated convincingly that the use of bed-nets and curtains treated with insecticide reduces morbidity from malaria substantially. Lengeler et al. (1998) reported that insecticide treated nets and curtains now provide residents of malaria endemic area (Gambia) with an effective means of protecting themselves against malaria.
Observation was made in this study of variation in prevalence rates both in the villages, among the age groups and within the individual households. This could be attributed to house location within the community and age of individual child. Despite the fact that anopheles mosquitoes can fly substantial distances, the distance between a village or house and a breeding site may be very important in determining malaria risk. In Pikine, a suburb of Senegal, Trape et al. (1992) showed that there was a steep gradient in the prevalence of malaria between the centre and the edge of town which is adjacent to marshy areas where breeding of anopheles mosquito take place. In this study, it was found that the risk of malaria was higher among those who live near the rivers (Ameke and Obinagu villages). Also malaria prevalence is naturally higher in children of lower age groups Eneanya, (1998). In Oruku, like most rural communities in the tropics, most houses are made of mud blocks, thatch roofed without ceilings. In the households where these mud walls are cracked, they form eaves which allowed easy access for mosquitoes inside sleeping rooms (Schofield and White, 1984). It was also observed that in some households, children are left under the care of either their grandparents or their sake “Ogbo” as they call it, who lacked the knowledge of basic hygiene and as a result dirty water that should be thrown away are left in cans, cups, buckets, pots and bowels within the compounds very near the houses and in some cases, even within the households. These are breeding sites for mosquitoes. The researcher also observed from this study that the cumulative number of symptoms/signs among these sampled children seem to be proportionally small, compared with the degree of parasite positivity. This may be attributed to the level of immunity developed by these children as a result of constant attack of malaria infection. This is in line with the report of Gerhard (2005) who observed that in many parts of Africa where malaria infection has been endemic, people are infected so frequently that they develop a certain degree of immunity and in many cases they carry malaria parasites without showing any symptoms.
The inhabitants did not complain of any adverse reaction in the course of using the treated items. Manifestations of acute or residual poisoning were not found. It was clear therefore that curtain, mat and blanket treated with graded dose of lambdacyhalothrin, control mosquito bites and consequently malaria infection. And more importantly, is well tolerated by humans. Steps should therefore be taken by the government and donor agents to produce these treated items in large quantities, for they will go a long way in getting rid of mosquitoes and save the people of Oruku in particular and Africa in general from acute and chronic problems.
CONCLUSION AND RECOMMENDATION
This study concludes that the use of insecticide treated bed net, curtains and mats with lambdacyhalothrin can serve in controlling mosquito bite thus reducing malaria infection among the experimental area. Therefore, it is suggested that there should be public health awareness on the general use of lambdacyhalothrin by individual households, because of its long term sustainability to control of mosquito bite and non-acute or residual poisonous effect to services than other mosquito control measures.
ACKNOWLEDGEMENTS
The authors wish to appreciate in a special way the effort of Professor Okafor Fabian, the kind effort of Oruku community primary schools especially the head teachers and pupils of the school. The assistance of staff of Parasitology Unit of University of Nigeria Nsukka were also kindly appreciated.
CONFLICT OF INTEREST
The author declared he has no conflict of interest.
REFERENCES
| Ali A (1996). Population and samples. Foundation of Research in Education. Merks publishers, Awka Anambra State P 320. | ||||
|
Alonso PL, Lindsay SW, Armstrong JRM, Conteeh M, Hill AG, David PH, Fegan G, Francisco A, Hall AJ, Shenton FC, Cham K, Greenwood BM (1991). Effect of insecticide treated bed-nets on mortality of Gambian children. Lancet 337:1499-1502. Crossref |
||||
|
Binka FN, Kubaye A, Adjuik M, Smith PG (1996). Impact of permethrin Impregnated bed-nets on child mortality in Kassena-Nankana District, Ghana: Randomized controlled trial. Trop. Med. Int. Health 1:147-154 Crossref |
||||
|
Beare NA, Taylor TE, Harding SP, Lewallen S, Molyneux ME (2006). Malaria retinopathy: A New established diagnostic signs in severe malaria. Am. J. Trop. Med. Hyg. 75(5):790-7. Pubmed |
||||
|
Breman J (2001). The ears of the hippopotamus: Manifestation, determinants and estimates of malaria burden. Am. J. Trop. Med. Hyg. 64(1-2):1-11. Pubmed |
||||
| Brieger (1996, 1997). Use of impregnated mosquito net for malaria control. Bulletin of World Health Organisation, pp 69-594. | ||||
|
Christopher JLM, Lisa CR, Stephen SL, Kathryn GA, Kyle JF, Diana H, Nancy F, Mohsen N, Rafael L, Alan DL (2012). Global malaria mortality between 1980 and 2010:a systematic analysis. Lancet 379(9814):413-431 Crossref |
||||
|
Greenwood BM, Bojang K, Whitty CJ, Targett GA (2005). "Malaria". Lancent 365(9469):1487-98 Crossref |
||||
|
Keiser J, Utzinger J, Caldas M, Smith T, Tanner M, Singer B (2004). Urbanization in sub-Saharan and implication for malaria. Am. J. Trop. Med. Hyg. 71(2):118-27 Pubmed |
||||
| Layne SP (2006). Principles of infectious disease epidemiology. Available at: http://health.mo.gov/training/epi/Mod1StudentOutline.pdf | ||||
| Lengeler C (1998). Insecticide treated bed nets and curtains for malaria control Issue 3, Oxford Uk. Available at: http://www.thecochranelibrary.com/userfiles/ccoch/file/CD000363.pdf | ||||
| Michael F (2007). Stopping a global killer: the rapidly spreading disease affects more people than before but until recently, the outcry has been muted. National Geographic Magazine. | ||||
| Molineaux L (1988). The epidemiology of human malaria as an explanation of its distribution, including some implications for its control In W.H. Wemsdorfer and I.J.Mc. Churchill Livingstone Publishers, Uk pp. 913-998. | ||||
|
Nevill CG, Some ES, Mungala VO, Mutemi W, New L, Marsh K, Lengeler C, Snow RW (1996). Insecticide-treated bed nets reduce morbidity from malaria among children on the Kenyan coast. Am. J. trop. Med. Hyg. 1:139-146 Crossref |
||||
| Obi IU (2002). Statistical Methods of Declining Differences Between Treatment Means and Research Methodology Issues in Laboratory and Field Experiments. AP Express Publishers Ltd Nsukka, Nigeria xiii. pp 117. | ||||
| Provost C (2011). World malaria day: Which countries are the hardest hit. The Gardian Retrieved 2012-05-03. Available at: http://www.theguardian.com/global-development/datablog/2011/apr/25/world-malaria-day-data | ||||
|
Prothero RM (1999). Forest and people in southeast Asia. Singapore J. Trop. Geog. 20(1):76-85. Crossref |
||||
|
Sexton JD (1994). Impregnated bed net for malaria control: biological success and social responsibility. Am. J. Trop. Med. Hyg. 50:72-81. Pubmed |
||||
| WHO (2005). Guidelines for laboratory and field testing of mosquito larvicides. World Health Organization Communicable Disease Control, Prevention and Eradication. WHO Pesticide Evaluation Scheme. HO/CDS/WHOPES/GCDPP/2005.13. | ||||
| WHO (2010). Guidelines for the treatment of malaria (Report) (2nd ed) 978-9-2415-4792-5 Accessed May 11, 2012. | ||||
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


