Full Length Research Paper

ABSTRACT
This paper assessed healthcare facilities location and medical waste generation and handling in Nigeria. Analysis such as descriptive statistics, correlation and factor analysis was carried out to identify gaps in healthcare facilities location and medical waste management in Nigeria. The population-to-healthcare provider ratio and healthcare waste generation rates in Nigeria were also analysed. The north central geo-political zone of Nigeria has over 9,000 healthcare facilities while the south-south zone has less than 5,000. Public primary health facilities are the most evenly located health institutions in Nigeria. Seventeen states in Nigeria are under served with regards to healthcare providers in facilities and can be classified as healthcare provider shortage areas. About 19,864.03 kg/day of waste is generated in Nigeria with the north central and north east accounting for the highest rates. Standard incineration facilities for effective medical waste management existed in 22% of all health facilities surveyed. Tertiary health facilities had adequate capacity (over 70%) to incinerate medical waste while significant gaps existed at the secondary and primary healthcare levels. Pearson’s correlation of employee capacities and waste management practices was significant. Factor analysis of variables on employee capacities and waste management practices showed that the first two components extracted accounted for 70.43% of the variance. The components matrix revealed that improving the availability of appropriate waste management equipment and control procedures is required. Healthcare policy makers in developing countries and Nigeria should strive towards equitable location of healthcare infrastructure and trained medical personnel, provision of appropriate waste management technologies, and building capacity of healthcare staff involved with the utilization, handling, and disposal of infectious and hazardous medical waste items.
Key words: Healthcare, developing countries, medical waste, infectious waste, Lassa, HIV, hepatitis.
INTRODUCTION
Globally, healthcare policy makers pay attention to quality of care, level of care, and accessibility factors by citizens. According to Zhang et al. (2019), accessibility to healthcare is influenced by classified levels of care and spatial characteristics of the population and healthcare facilities. Zhang et al. (2019) stated that location of healthcare services is significant in assessing the unmet medical needs of a population. In this regard, healthcare policy makers need to be sensitive to the location of healthcare services and the distribution of healthcare types. Healthcare facilities are usually concentrated in urban areas with a significant relationship between population and healthcare distribution (Babatimehin, et al., 2015; Mustapha, 2017). The concentration of healthcare facilities in densely populated and highly dynamic urban areas increase exposure levels to hazardous medical wastes especially in settings where healthcare waste management is inadequate. The World Health Organisation (2018) stated that 15% of healthcare wastes are hazardous and infectious, and that unsatisfactory medical waste management leads to a significant risk of new infectious diseases globally (World Health Organisation, 2018).
Healthcare facilities produce various waste products including medical waste with risk of transmitting infections such as Hepatitis B and C (HBV and HCV), the Human Immunodeficiency Virus (HIV), and Haemorrhagic diseases such as Lassa fever and Ebola which are now in existence in West Africa (Tobin et al., 2013). In low- and middle-income countries, the manual handling and sorting of medical waste and scavenging of dumpsites leads to risk of needle-stick injuries and a 30, 1.8, and 0.3% chance respectively of getting infected with hepatitis B, hepatitis C, and HIV (World Health Organisation, 2018). Evidence of HIV outbreak linked to unsafe injection practices and disposal have been reported in Ijeoma et al. (2016). Musa et al. (2015) found that between 2000 and 2015, the hepatitis B was hyper endemic in Nigeria and could be the highest in sub-Saharan Africa. The World Health Organisation (2019) reported that between January 1 and February 28, 2019, a total of 327 of Lassa fever infections were confirmed and 72 deaths were recorded across 20 states and the Federal Capital Territory in Nigeria. The World Health Organisation (2019), stated that 12 cases were reported among healthcare workers in seven states. The Nigeria Centre of Disease Control Lassa fever situation report for week six (2020) stated that over 450 Lassa fever infections were confirmed across 26 states with 70 fatalities. Out of the number of fatalities, the Nigeria Centre of Disease Control recorded stated that 15 were healthcare workers.
Kumar et al. (2014) puts the number of pathogens medical waste can potentially transmit at forty and that proper medical waste management practices was one of the most important functions of health workers. According to Kumar et al. (2014), healthcare facility administrators need to ensure proper medical waste management practices and effective compliance monitoring. The importance of policy and legislation in proper medical waste management practices has been emphasised (Awodele et al., 2016). According to the World Health Organisation (2015), the percentage of healthcare institutions with unsatisfactory waste management practices is about 42% as several countries had no policy documents concerning medical waste management. As posited in Kumar et al. (2014), resource limited settings such as developing countries in sub-Saharan Africa grapple with inadequate medical waste management practices adduced to issues which are economical, technological, social and capacity based.
In Nigeria, a National Health Act was signed into law in 2014. The National Health Act provides a framework for regulating, developing and managing health systems and providing standards for health services in Nigeria. Since the commencement of National Health Act, some studies have decried the level of medical waste management in Nigeria (Oyekale and Oyekale, 2017; Ezechi et al., 2017). Another study by Ezirim and Agbo (2018) however reported some improvement in healthcare waste segregation at selected facilities in Nigeria. Overall, the management of healthcare in Nigeria is fraught with several challenges such as inadequate location of facilities, inadequate human resources, unsustainable financing, weak government spending, high user fees, commodity shortages, uptake and access issues, and the literacy levels of the populace (Obansa and Orimisan, 2013). The World Health Organisation (2016) attributed the spread of the Ebola virus disease across west Africa in 2014 to poorly prepared health systems at all levels. Nigeria, which is the largest West African country in terms of population and economy size, experience significant incidences of infectious diseases such as hepatitis, tuberculosis, Lassa fever and HIV.
Due to a number of factors associated with inadequate planning and monitoring, logistics issues, storage and access issues, developing countries including Nigeria record high amounts of expired medical commodities, and wastes which are considered hazardous and infectious (Tull, 2018). According to Aturaka et al. (2017), the total cost of expired health commodities in Nigeria from 2013 to 2014 was 51,369.02 United States dollars. Aturaka et al. (2017) described it as a huge loss to the nation. Despite the evidence which supports the existence of risks associated with improper management of medical waste, the subject has not been given adequate attention in literature. The risk of infections and disease outbreaks due to improper management of medical waste is significant in Nigeria. This paper therefore draws its relevance from the assessment of health facilities location and medical waste generation and handling in Nigeria. This is in a bid to draw the attention of stakeholders in developing countries to significant issues which could improve healthcare facilities location, quality of healthcare waste management, and in particular, reduce the risk of disease outbreaks from improper management of medical waste.
MATERIALS AND METHODS
Study area
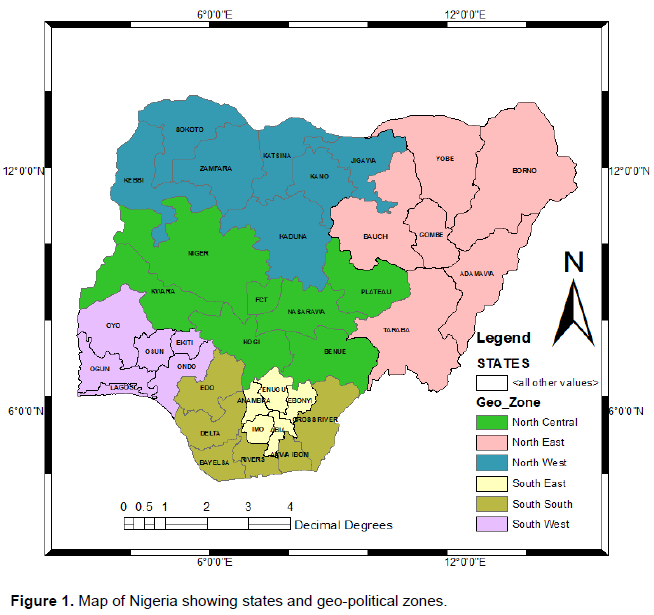
Nigeria is located between latitudes 4° 1' and 13° 9' North and longitudes 2° 2 ' and 14° 30' East. It is a tropical country bordered by Niger Republic to the north; Republic of Chad to the north east; Republic of Cameroun in the east; Republic of Benin to the west. Beyond the southern borders is the Atlantic Ocean. Nigeria’s total surface area is approximately 1, 923,768 square kilometres. Nigeria has a population of about 140,003,542 which is the highest in Africa (Federal Government of Nigeria, 2007). Over 60% of Nigerians live in rural areas (Federal Government of Nigeria, 2007). The Federal Republic of Nigeria is divided into 36 States and a Federal Capital Territory (FCT). These states have been grouped for political convenience into geopolitical zones which are North East (NE), North West (NW), North Central (NC), South East (SE), South West (SW), and South-south (SS). The location map is presented as Figure 1.
Sources of data
Data was collected from secondary sources which included several journal papers on healthcare waste management, the National Directory of Health Facilities in Nigeria by the Federal Ministry of Health (FMOH) (2011; 2019), and the World Bank funded Environmental and Social Safeguards Audit report by the National Agency for the Control of AIDS (NACA) (2015).
Information concerning types of healthcare facilities, location and other attributes was obtained from the National Directory of Health Facilities in Nigeria (Federal Ministry of Health, 2011; 2019). Information on healthcare waste generation and handling was obtained from the Environmental and Social Safeguards Audit (National Agency for the Control of AIDS, 2015). The Environmental and Social Safeguards Audit (National Agency for the Control of AIDS, 2015) was conducted within a sample framework of 7,667 health facilities located in thirty-five states in Nigeria. The Environmental and Social Safeguards Audit (National Agency for the Control of AIDS, 2015) utilised the probability proportional to size (PPS) method to randomly select 1,921 facilities from the sample framework across local government areas in 35 states. These facilities were public primary (64%), public secondary (12.4%), public tertiary (1.6%), and private health facilities (22%). Therefore, the Environmental and Social Safeguards Audit (National Agency for the Control of AIDS, 2015) was found suitable as an information source for healthcare waste management in Nigeria.
Data analysis
Data analysis including the measure of central tendencies, descriptive statistics, correlation, and factor analysis was carried out using Microsoft Excel version 2016 and SPSS version 19. These analysis were used to determine percentage types of healthcare facilities, zonal and state location percentages, and percentage distribution of staff, equipment and other attributes relevant for the management of medical waste. Correlation and factor analysis was used to establish relational attributes of variables of health facilities employee capacities and waste management practices. The methods used in New Mexico’s Indicator-Based Information System (2019) were used to calculate the threshold for population-to-healthcare provider’s ratio. According to New Mexico’s Indicator-Based Information System (2019), the threshold for population-to-healthcare provider ratio should be 3,500 to 1. In addition, the method for healthcare waste generation rate described in Meleko et al. (2018) was adapted for use in this paper. Meleko et al. (2018) calculated mean daily waste generation by multiplying amount with the number of days in one year (365) under the assumption that waste generating activities are uniform. Results of data analysis are presented as tables and figures.
RESULTS
Healthcare facilities location in Nigeria
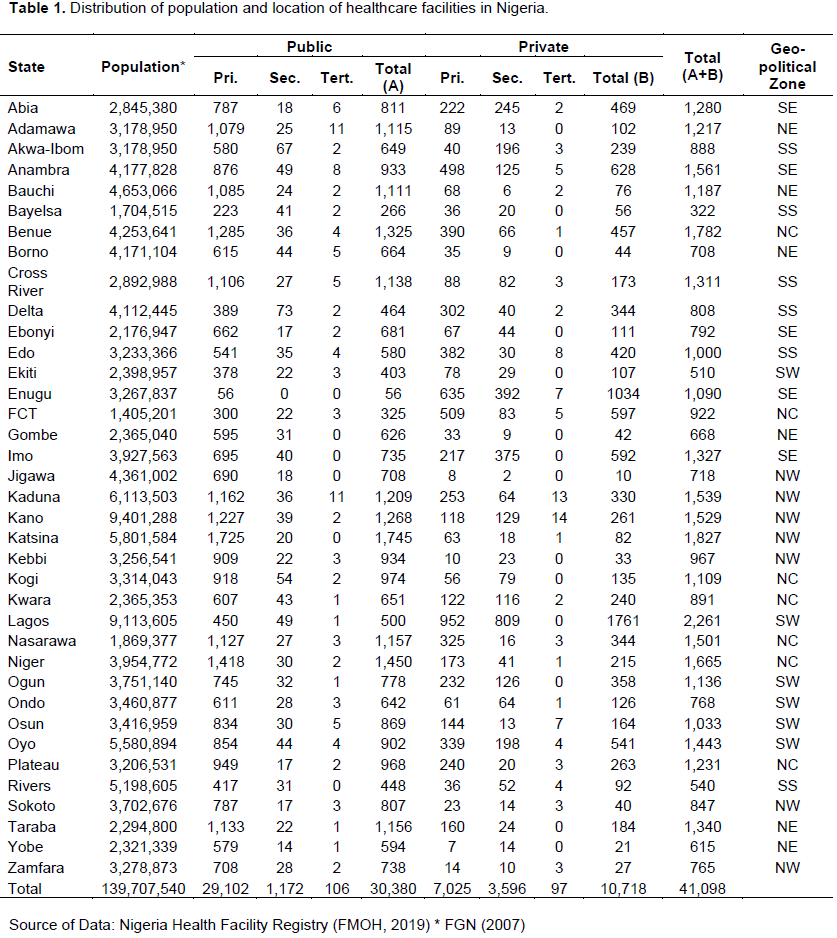
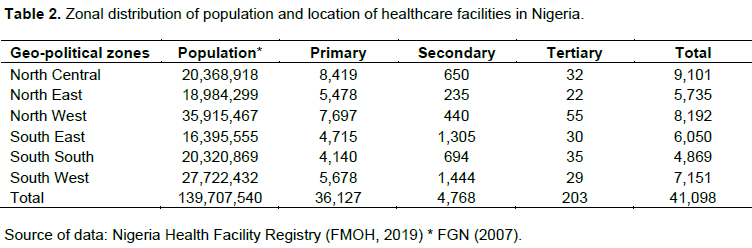
According to the directory of healthcare facilities in Nigeria (Federal Ministry of Health, 2011), there were 34,173 recognised healthcare facilities in Nigeria which included 21,463 public primary healthcare facilities, 8,290 private primary healthcare facilities, 969 public secondary healthcare facilities, 3,023 private secondary healthcare facilities, 73 public tertiary healthcare facilities, and 10 private tertiary healthcare facilities. The updated Nigeria Health Facility Registry (Federal Ministry of Health, 2019) showed that the total number of healthcare facilities in Nigeria is about 41,098. There are 29,102 public primary healthcare facilities, 1,172 public secondary healthcare facilities, and 106 public tertiary healthcare facilities. There are also 7,025 private primary healthcare facilities, 3,596 private secondary healthcare facilities, and 97 private tertiary healthcare facilities (Table 1). Healthcare facilities in Nigeria are highest in the north central geopolitical zone with 9,101 and lowest in the south-south zone with 4,869 even though the two zones have similar populations size. The north-west and south west zone with the highest population in the country also have a high number of healthcare facilities (Table 2). As shown in Table 2, there are a total of 36,127 primary healthcare facilities, a total of 4,768 secondary healthcare facilities, and a total of 203 tertiary healthcare facilities in Nigeria. When the number of healthcare facilities is weighed against the population, obvious gaps are revealed. For instance, the ratio of the population and total number of healthcare facilities in Nigeria is about 3,400 - 1. However, the ratio of the population and total primary healthcare facilities is about 3,867 - 1, while that of population against secondary and tertiary healthcare facilities is about 29,301 - 1 and 688, 214 - 1 respectively.
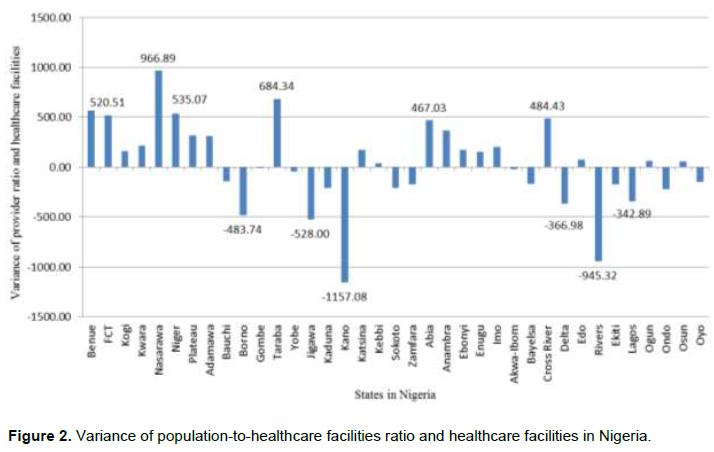
The New Mexico’s Indicator-Based Information System (2019) utilised the threshold for population-to-healthcare provider to determine “healthcare provider shortage areas.” According to New Mexico’s Indicator-Based Information System (2019), the threshold for population-to-healthcare provider ratio should be 3,500 to 1 or maintained under 3,500. Using the New Mexico’s Indicator-Based Information System (2019) method, the threshold for population-to-healthcare providers in facilities across Nigeria was calculated (Figure 2). As revealed in Figure 2, 17 states in Nigeria are under served with regards to healthcare providers in facilities and can be classified as “healthcare provider shortage areas” as determined in New Mexico’s Indicator-Based Information System (2019). The states with the most needs include Jigawa, Kano and Rivers States. States such as Benue, Nasarawa, Niger, and the FCT have healthcare facilities over the threshold ratio of 3,500 to 1 (Figure 2). Mustapha (2017) stated that tertiary healthcare facilities are the most equipped and bear the burden of care. The treatment and care services for infectious disease epidemics such as hepatitis, tuberculosis, Lassa fever and HIV are mostly delivered through tertiary and secondary healthcare facilities around the country. As emphasised by Mustapha (2017), there is a need to increase the number of specialised healthcare facilities and trained medical personnel around the country to deal with infectious diseases and haemorrhagic fevers.
Medical waste management in Nigeria
According to environmental and social safeguards audit report (National Agency for the Control of AIDS, 2015), over 70% of all facilities surveyed in the country generate universal, hazardous, and infectious waste. Over 80% of all tertiary, secondary, primary, and private health facilities surveyed in National Agency for the Control of AIDS (2015) generated hazardous and infectious wastes (Table 3). The National Health Management Plan (Federal Ministry of Health, 2012) provided healthcare waste generation rates in Nigeria. Table 4 shows that tertiary health facilities in Nigeria generate about 10.68 kg/bed/day of waste while secondary and primary healthcare facilities generate about 2.78 kg/bed/day and 1.1kg/bed/day respectively (Federal Ministry of Health, 2012). Tertiary hospitals mainly exist in urban areas and attract a high number of patients whereas secondary and primary healthcare facilities mainly exits in semi-urban and rural areas. Some literature suggests the burden of care is borne by tertiary which creates a burden of healthcare waste management with regards to the systems, personnel, and infrastructure required. The method used in Meleko et al. (2018) was used in determining healthcare waste generation rates in Nigeria. As revealed in Table 5, 19,864.03 kg/day of waste is generated in Nigeria with the north central and north east accounting for the highest rates. Table 5 also shows that Nigeria has an annual healthcare waste generation rate of 7,250,372.17 kg/year out of which about 15% (1,087,555.83 kg) is potentially infectious and hazardous medical waste.
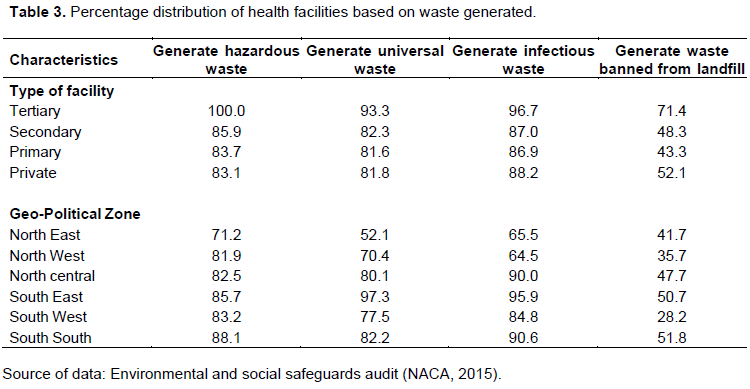
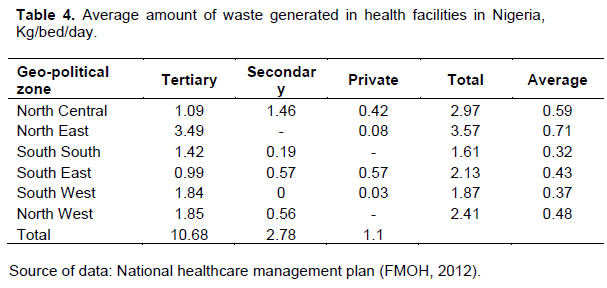
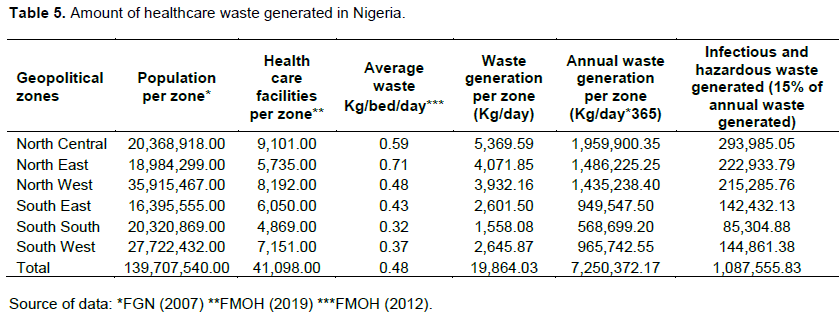
Figure 3 shows the level of healthcare waste generated in tertiary healthcare facilities across the country while Figure 4 shows the same information for secondary and primary healthcare facilities. When Figures 3 and 4 are compared, the amount of waste generated is clearly higher in secondary and primary healthcare facilities than what is obtainable in tertiary healthcare facilities. However, a higher percentage of the waste generated by tertiary healthcare facilities would include hazardous and infectious medical waste because of the level of care provided at that level. The highest amount of healthcare waste is generated at primary healthcare level (Figure 4).
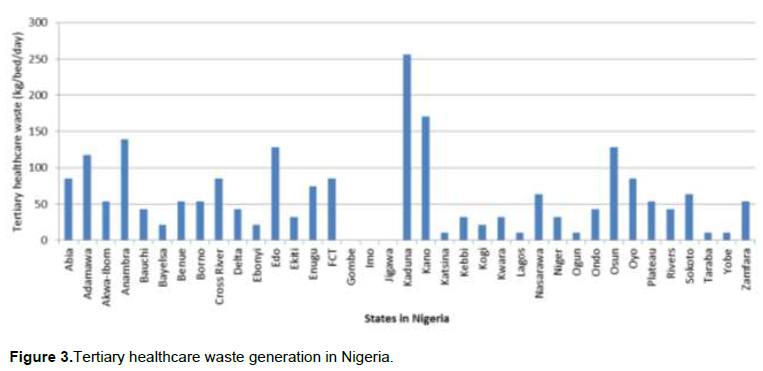
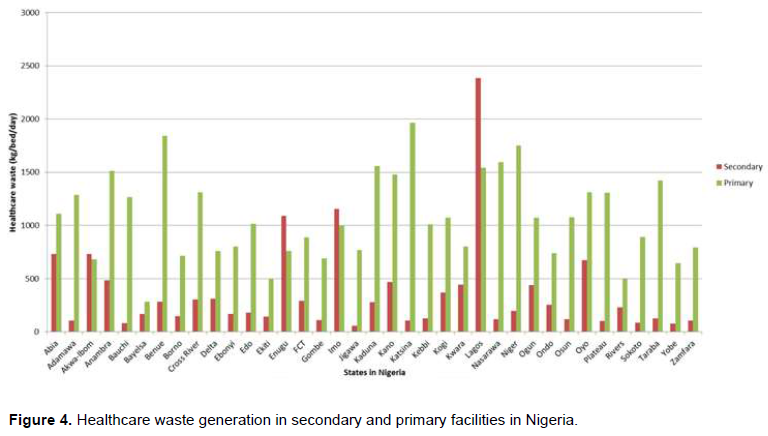
However, in Lagos, Imo, Enugu, and Akwa Ibom States, most of the healthcare waste is generated by secondary Healthcare facilities. Depending on the nature of infrastructure and human resource available, some secondary and primary healthcare facilities may generate a significant amount of hazardous and infectious medical waste.
Tertiary healthcare facilities in the country are better equipped to handle and dispose hazardous and infectious medical waste, and also to recycle waste banned from landfills. Many health facilities in Nigeria are familiar with waste identification methods and are familiar with recommended waste characterization methods. However, their ability to demonstrate effective medical waste management is hindered by inadequacies of incineration facilities and capacity to recycle waste items banned from landfills. The environmental and social safeguards audit report (National Agency for the Control of AIDS, 2015) found that only 22% of all health facilities surveyed had standard incineration facilities. Tertiary health facilities had over 70% capacity to incinerate medical waste. Tertiary health facilities also had the highest capacity for all round healthcare waste management in the country. Considering that tertiary health facilities make up the least percentage of health facilities in the country, this is inadequate. The percentage of secondary healthcare facilities with incineration facilities was 36.5 % while the percentage of primary healthcare facilities with incinerators was 19.5%. As observed, only the north west had over 40% capacity for effective waste incineration while that of the north east, south west, south east, and south south were all under 20%.
According to the environmental and social safeguards audit (National Agency for the Control of AIDS, 2015), 95% of all incineration waste treatment facilities are government owned and only 5% is privately owned. The types of incinerators available are brick and mortar (28.8%), closed combustion (23.3%), and open pit (47.9%). This places a huge resource burden on public expenditure for health which may not be reflected in the quality of management. This is simply because public sector owned entities are perceived to operate less effectively and less efficiently.
The results suggest gaps exist in Nigeria when it comes to emergency preparedness for public health diseases of international concern. This can be triggered by poor handling of medical waste among other factors. According to National Agency for the Control of AIDS (2015), 66.7% of tertiary health facilities, 36.9% of secondary health facilities, and 17.6% of primary health facilities have written emergency plans. In addition, 69% of tertiary, 45.5% of secondary, and 24.9% of primary health facilities have trained personnel with specific emergency response task. The trend among the facilities was similar for emergency response test exercises (National Agency for the Control of AIDS, 2015). The percentage distribution of basic emergency response capacity among healthcare facilities across the geo-political zones in Nigeria was inadequate.
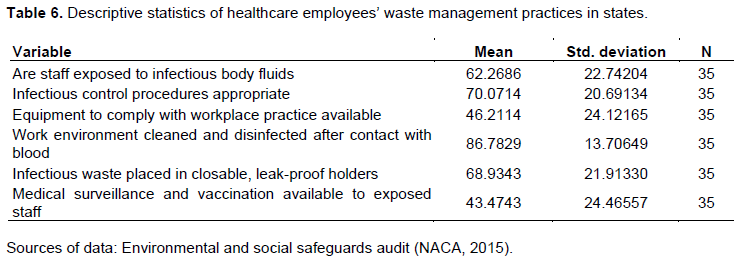
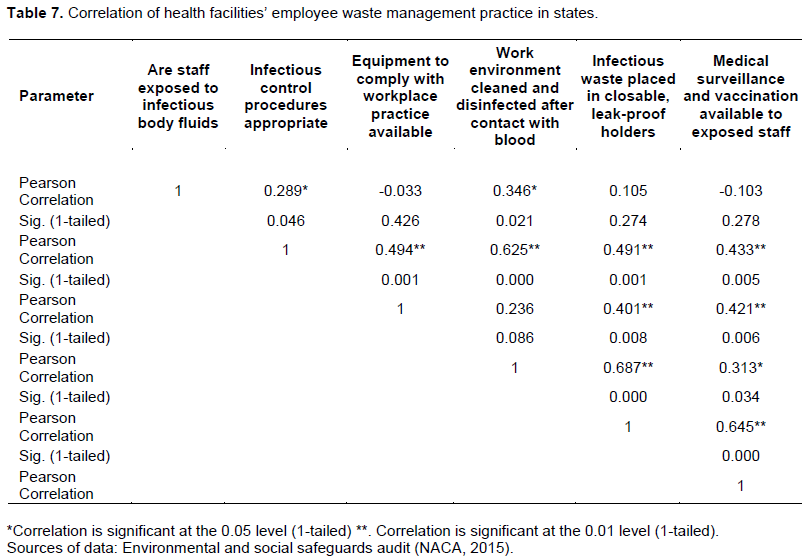
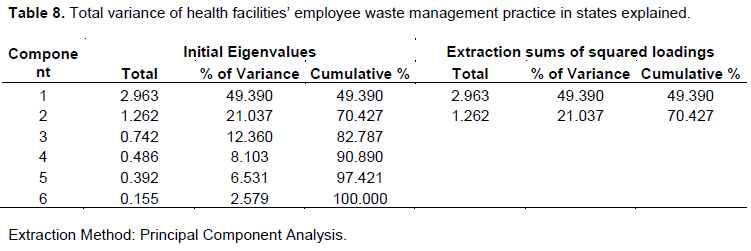
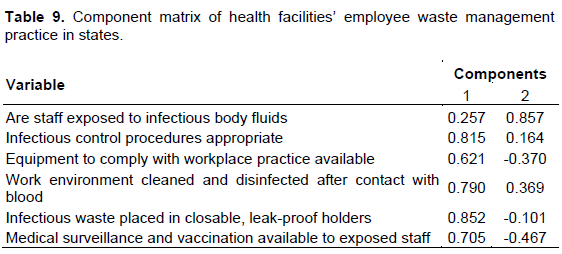
The paper observed that over 60% of employees of sampled health facilities were exposed to infectious body fluids, while only 46.2% and 43.5% had access to protective equipment, medical surveillance and vaccination respectively (Table 6). The results of Pearson’s correlation carried out on variables of employees of sampled health facilities in Nigeria revealed that there was a significant relationship between some of the variables at p<0.01 and p<0.05 (Table 7). Factor analysis using the principal component extraction method was carried out on the same data set (Tables 8 and 9). Table 8 shows the initial eigenvalues for six extracted components and the first two accounted for 70.43% of the variance. The components matrix (Table 9) revealed that the first component will increase with increases in the following variables which include infectious waste placed in closable, leak-proof holders, infectious control procedures appropriate, work environment cleaned and disinfected after contact with blood, medical surveillance and vaccination available to exposed staff, and equipment to comply with workplace practice available. These variables fluctuate together and an increase in one can lead to an increase in others. Therefore, the first component is a measure of the quality of the mentioned variables. The second component (Table 9) clearly revealed that an increase in the first variable concerning exposure to body fluids is a negative indication of the quality of the other variables.
DISCUSSION
The total number of healthcare facilities may seem to be sufficient to support universal access to healthcare in Nigeria. However, the number, location and management systems of health facilities in Nigeria may pose access, referral, and service uptake challenges. There is a need to locate new healthcare facilities in healthcare shortage areas and new facilities should be guided by deliberate criteria and modelling to address location disparities between secondary and tertiary facilities. As stated in Olukanni et al. (2014), tertiary health facilities in Nigeria are the most equipped, have the highest number of trained specialists, and serve as referral hospitals. Healthcare policy makers need to optimise location and upgrade the infrastructure and equipment of secondary and primary healthcare facilities to effectively scale up care and complement tertiary healthcare facilities. An effective ‘hub and spoke’ relational arrangement can enable healthcare policy makers strengthen the operational relationships between public and private healthcare facilities in the country. The ‘hub and spoke’ model can be used to network existing healthcare waste handling capacities to improve medical waste management in Nigeria. This can be achieved by effectively linking the healthcare waste management logistics and value chain with existing incineration infrastructure. In addition, it is necessary to improve the distribution of trained and specialised medical personnel across the types of healthcare facilities. Improving welfare conditions for medical personnel and leveraging on technological advancements, electronic medical records and telemedicine will enable the availability of more trained specialists in lower level healthcare facilities.
Aturaka et al. (2017) recommended improved coordination, network and capacity development of healthcare staff to achieve the level of efficiency desired to address gaps in the utilisation of high amounts of health commodities for various public health interventions such as hepatitis, tuberculosis, Lassa fever and HIV to mention a few. As presented in the results, inadequacies with regards to management of medical waste can be addressed through compliance with healthcare waste management policies in Nigeria. Oli et al. (2016) assessed healthcare waste management in southeast Nigeria and found that compliance with policy guidelines on handling and disposal was quite low and needed to improve. According to Oli et al. (2016), non-availability of waste disposal materials, inadvertence to procedure, and lack of adequate training were major issues in both public and private hospitals assessed in south east Nigeria. Awodele et al. (2016) studied medical waste management in healthcare facilities in Lagos Nigeria and found that all the facilities surveyed did not have policies and guidelines on waste management at which should guide health workers in the proper handling of medical waste. Similar findings have been reported in Anyika (2014) and in Oyekale and Oyekale (2017).
There is a need to advocate for the implementation of the National Healthcare Act nationwide to ensure health facilities domesticate policies and guidelines on waste management and imbibe a culture of compliance with appropriate waste management practices. This amplifies the role of staff of health facilities in maintaining an effective medical waste management system. The results have reflected gaps in capacity of staff to effectively carryout duties related to proper waste management segregation, handling, and disposal. Capacity building for healthcare workers on medical waste management is quite important. This will reduce exposure of staff of health facilities to injury and infections and ensure medical waste is properly disposed. In all health facilities surveyed by Olukanni et al. (2014), none of the medical waste handlers pre-treated waste before disposal and they claimed there was no need for medical waste pre-treatment before disposal. Similarly, Ogoina et al. (2014) found an unusually high rate of exposure of health workers in Nigeria to body fluids and most cases were newly qualified medical personnel.
Amira and Awobusuyi (2014) posited that medical waste handlers and health workers involved with the handling of blood contaminated items face a high risk of infections such as hepatitis B (HBV), hepatitis C (HCV), and Human Immunodeficiency Virus (HIV). Haemorrhagic diseases such as Lassa fever and Ebola virus diseases are also highly infectious from blood contaminated waste items. According to the study by Amira and Awobusuyi (2014), 40.2% of health workers sampled had experienced an infection from exposure to infectious and hazardous waste. Non segregation of waste and the lack of use of protective clothing during waste handling are major factors contributing to infections from medical waste (Erekpitan et al., 2015). Inadequacies of appropriate management practices and infrastructure make medical waste management in Nigeria unsustainable (Ezechi et al., 2017). Infrastructure for incineration which is a preferred healthcare waste management practice for the treatment of a wide range of waste materials including infectious and hazardous waste should be developed in Nigeria (Abila and Kantola 2013; Ikpeze, 2014; Ezechi et al., 2017). The inadequacy of incineration infrastructure was evident from the results.
The main limitation of this paper was the reliance and utilisation of data from secondary sources as no ground-truth was carried. However, the findings are significant for the assessment of healthcare facilities location and medical waste management in developing countries and in Nigeria.
CONCLUSION
This paper has assessed healthcare facilities location and medical waste generation and handling in Nigeria. This paper found inadequacies with the location of healthcare facilities and medical waste management in Nigeria. The gaps observed in healthcare access, and medical waste management practices and infrastructure may affect the sustainability of the health system in Nigeria. An effective relational arrangement can strengthen the network of healthcare facilities, create operational linkages between the various facility types, encourage public and private healthcare partnerships, and strengthen existing healthcare waste handling and management capacities. Provision of sustainable healthcare waste management practices in Nigeria would require appropriate waste management technologies in sufficient quantities, and building capacity of healthcare staff that are involved with the utilisation, handling, and disposal of medical waste items. As the country progresses with the implementation of the National Health Act, healthcare policy makers in Nigeria should strive towards equitable location of healthcare infrastructure and trained medical personnel to enhance universal access to healthcare services. Addressing the challenges facing the management of healthcare in Nigeria has become a necessity of high significance in the light of recent public health diseases of international concern. These recommendations can build the resilience and preparedness of the healthcare systems in developing countries with regards to public health disease outbreaks, attendant consequences of climate change, and achievement of the sustainable development goals related to health.
CONFLICT OF INTERESTS
The author has not declared any conflict of interests.
REFERENCES
|
Abila B, Kantola J (2013). Municipal solid waste management problems in Nigeria: evolving knowledge management solution. International Journal of Environmental and Ecological Engineering 7(6):303-308. |
|
|
Amira CO, Awobusuyi JO (2014). Needle-stick injury among health care workers in haemodialysis units in Nigeria: a multi-centre studyInternational Journal of Occupational and Environmental Medicine 5:1-8 |
|
|
Anyika EN (2014). Challenges of implementing sustainable health care delivery in Nigeria under environmental uncertainty. Journal of Hospital Administration 3(6):113-126 |
|
|
Aturaka SO, Abiodun O, Omotola O, Adebimpe WO, Imohi P, Okon O (2017). Challenges associated with supply chain management of HIV/AIDS programs in Cross River State, Nigeria. American Journal of Health Research 5(4):114-118. |
|
|
Awodele O, Adewoye AA, Oparah AC (2016). Assessment of medical waste management in seven hospitals in Lagos, Nigeria. BMC Public Health 16:269. |
|
|
Babatimehin OI, Nelson NE, Oyinloye RO, Adeoye NO, Taiwo OJ, Ige JD (2015). Geographical analysis of the patterns of healthcare facilities and HIV/ AIDS response sites in Benue State, Nigeria. The Open Geography Journal 7:17-27 |
|
|
Erekpitan OO, Mangden YPE, Sati YC, Adisa JO (2015). Knowledge, attitudes/beliefs and practices in medical waste management - an appraisal of Jos North LGA, Plateau State, Nigeria. International Journal of Research in Humanities and Social Studies 2(12):43-56 |
|
|
Ezechi EH, Nwabuko CG, Enyinnaya OC, Babington CJ (2017). Municipal solid waste management in Aba, Nigeria: challenges and prospects. Environmental Engineering Research 22(3):231-236. |
|
|
Ezirim I, Agbo F (2018). Role of national policy in improving health care waste management in Nigeria. Journal of Health Pollution 8(16):180913. |
|
|
Federal Government of Nigeria (FGN) (2007). Details of the breakdown of the national and state provisional population totals of 2006 census. Federal Government of Nigeria (FGN) Official Gazette 94(24):B175-B198. Abuja. |
|
|
Federal Ministry of Health (FMOH) (2011). A directory of health facilities in Nigeria. Federal Ministry of Health, Abuja, Nigeria. |
|
|
Federal Ministry of Health (FMOH) (2012). National healthcare waste management policy. Federal Ministry of Health, Abuja, Nigeria |
|
|
Federal Ministry of Health (2019). Nigeria health facility registry. Federal Ministry of Health (FMOH), Abuja, Nigeria. |
|
|
Ijeoma UC, Sansam S, Srun S, Vannara H, Sanith S, Sopheap T, Newman RD, Gadde R, Dejana S, Hassani AS, Ly V (2016). Notes from the field: Public health response to a Human Immunodeficiency Virus outbreak associated with unsafe injection practices - Roka Commune, Cambodia. Morbidity and Mortality Weekly Report (MMWR) 67(4):135-136 |
|
|
Ikpeze N (2014).Safe disposal of municipal wastes in Nigeria: perspectives on a rights-based approach. Journal of Sustainable Development Law and Policy 3(1):72-86 |
|
|
Kumar R, Gupta AK, Aggarwal AK, Kumar A (2014). A descriptive study on evaluation of bio-medical waste management in a tertiary care public hospital of North India. Journal of Environmental Health Science and Engineering 12:69. |
|
|
Meleko A, Tesfaye T, Henok A, (2018). Assessment of Healthcare Waste Generation Rate and Its Management System in Health Centers of Bench Maji Zone. Ethiopian Journal of Health Sciences 28(2):125-134. |
|
|
Musa BM, Bussell S, Borodo MM, Samaila AA, Femi OL (2015). Prevalence of hepatitis B virus infection in Nigeria, 2000-2013: A systematic review and meta-analysis. Nigerian Journal of Clinical Practice 18:163-72 |
|
|
Mustapha A (2017). Lassa fever: Unveiling the misery of the Nigerian health worker. Annals of Nigerian Medicine 11(1):1-5. |
|
|
National Agency for the Control of AIDS (NACA) (2015). Environmental and social safeguards audit report (World Bank Funded). National Agency for the Control of AIDS (NACA), Abuja, Nigeria. |
|
|
New Mexico's Indicator-Based Information System (2019). New Mexico Department of Health, Indicator-Based Information System for Public Health (NM-IBIS). New Mexico Department of Health. |
|
|
Nigeria Centre for Disease Control (2020). Lassa fever situation report, week 6, February 2020. |
|
|
Obansa SA, Orimisan A (2013). Health care financing in Nigeria: prospects and challenges. Mediterranean Journal of Social Sciences 4(1):221-236 |
|
|
Ogoina D, Pondei K, Adetunji B, Chima G, Isichei C, Gidado S (2014). Prevalence and determinants of occupational exposures to blood and body fluids among health workers in two tertiary hospitals in Nigeria. African Journal of Infectious Diseases 8(2):50-54 |
|
|
Oli AN, Ekejindu CC, Adje DU, Ezeobi I, Ejiofor OS, Ibeh CC, Ubajaka CF (2016). Healthcare waste management in selected government and private hospitals in Southeast Nigeria. Asian Pacific Journal of Tropical Biomedicine 6(1):84-89. |
|
|
Olukanni DO, Azuh DE, Toogun TO, Okorie UE (2014). Medical waste management practices among selected health-care facilities in Nigeria: a case study. Scientific Research and Essays 9(10):431-439 |
|
|
Oyekale AS, Oyekale TO (2017). Healthcare waste management practices and safety indicators in Nigeria. BMC Public Health. |
|
|
Tobin EA, Ediagbonya TF, Asogun DA, Oteri AJ (2013). Assessment of healthcare waste management practices in primary health care facilities in a Lassa fever endemic Local Government Area of Edo state, Nigeria. AFRIMEDIC Journal 4(2):16-23 |
|
|
Tull K (2018). Drug expiry standards in developing countries. K4D Helpdesk Report. Brighton, UK: Institute of Development Studies |
|
|
World Health Organisation (WHO) (2015). Water, sanitation and hygiene in health care facilities: status in low- and middle-income countries. World Health Organization (WHO)/UNICEF, Geneva |
|
|
World Health Organisation (2016). Ebola outbreak 2014 - 2016. |
|
|
World Health Organisation (WHO) (2018). Fact sheet: Health care waste. |
|
|
World Health Organisation (WHO) (2019). Emergencies preparedness, response: Lassa fever - Nigeria. |
|
|
Zhang S, Song X, Wei Y, Deng W (2019). Spatial equity of multilevel healthcare in the metropolis of Chengdu, China: A new assessment approach. International Journal of Environmental Research and Public Health 16(3):493. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


