ABSTRACT
Data on dietary practices, physical activity and body mass indices of type 2 diabetics in Ghana is scanty. This study therefore assessed relationships between dietary practices, physical activity, and body mass indices of type 2 diabetic patients using a cross-sectional survey. One hundred and twenty type 2 diabetic patients were purposely recruited from the Diabetes Centre at the Korle-Bu Teaching Hospital in Accra, Ghana. Data were collected using a structured questionnaire, dietary assessment methods, anthropometry and a modified Global Physical Activity Questionnaire. Data obtained were analyzed using the Statistical Package for Social Sciences software (SPSS version 20.0) and ESHA-Food Processor Nutrient Database Software (Version 10). The Pearson correlation coefficient was used to test the associations at 5% level of significance. Most (88%) respondents had lived with diabetes for a year or more and majority (95%) ate 3 times daily with or without snacks. Both male and female respondents exceeded the recommended intakes for protein, calcium, vitamins A and C, and niacin. Energy intakes were however below the recommended values in both males and females. Respondents' level of physical activity was generally low (67%). Thirty eight percent had normal weights while 62% were either overweight or obese. There was a positive correlation and statistically significant relationship between diet quality and body mass index (BMI: r2=0.217; p= 0.017). Level of physical activity and BMI were also positively correlated and statistically significant (r2=0.213; p=0.019). Diet quality and physical activity have positive influences on the BMIs of respondents. Overweight and obese respondents need to be advised by health professionals on physical activities and proper diet to achieve healthy weights to avoid complications related to diabetes mellitus.
Key words: Dietary practices, diet quality, physical activity, body mass index (BMI), diabetes.
Diabetes mellitus (DM) is a metabolic disease charac-terized by hyperglycemia resulting from defects in insulin secretion or insulin action or both (Begum et al., 2004). It is a major health problem worldwide and many factors contribute to its onset. These include diet, obesity, and sedentary lifestyles (Zimmet et al., 2001; Sobal, 2001; Kyiamah, 2009), genetic factors, insulin resistance, age and lifestyle changes as a result of urbanization Ramachandran, 2004). Amoah and co-workers (2002) reported prevalence of type 2 diabetes mellitus to be 6.4% for adults aged 25 years and above in Ghana and further indicated that type 2 diabetes mellitus was associated with age and obesity. Again epidemiological data suggest interactions between acculturation, urbanization, and genetic disposition to be involved in development of type 2 diabetes mellitus among Ghanaians (Cooper and Rotimi, 1997; Saleh et al., 2002; Banini et al., 2003). Research suggests that about 23% of adults in Ghana are overweight, and this has been related to advanced age, female gender, urban environment, high income and tertiary education (Amoah et al., 2002; Amoah, 2003).
Diabetes is managed by dietary control, exercise and where applicable, by oral hypoglycemic agents and/or insulin. The aim of such measures is to maintain normal blood glucose level and prevent complications (Begum et al., 2004). Primary prevention of diabetes includes the promotion and adoption of healthy lifestyles such as establishing healthy eating patterns, achieving and maintaining healthy body weights and increasing physical activity. The progress of disease complications may be reduced if appropriate dietary practices are adhered to. Studies report that diet control can improve glycemic control and may reduce glycosylated hemoglobin (HbA1c) by 1.0 to 2.0% (Pastors et al., 2002; Pi-Sunyer et al., 1999; Kulkarni et al., 1998).
Physical activity plays a vital role in preventing and managing type 2 diabetes (Knowler et al., 2002; Boule et al., 2001; Tuomilehto et al., 2001; Pan et al., 1997). Exercise increases insulin sensitivity, reduces glycol-sylated hemoglobin levels, and also improves lipid profiles (Gordon et al., 2009). According to Motala and Ramaiya (2010), increasing rates of urbanization has led to reduced physical activity and reliance on motorized transportation in Ghana. The prevalence of physical inactivity has been reported to be 13% among West Africans including Ghanaians. Physical activity recom-mendations in Ghana are based on the World Health Organization guidelines which recommend a minimum of 30 min of moderate physical activity for at least five days per week (Ministry of Health, Ghana, 2010). It has been observed in prospective cohort studies that people who maintain a physically active lifestyle develop impaired glucose tolerance and type 2 diabetes mellitus less often than those with a sedentary lifestyle (Hu et al., 1999; Burchfiel et al., 1995; Helmrich et al., 1991). Reviews on exercise in diabetes patients have revealed the importance of exercise in the diabetes management plan. Regular exercise improves blood glucose control and reduces cardiovascular risk factors, maintain proper weight, blood pressure, fat levels and improve well-being. Furthermore, regular exercise may prevent type 2 diabetes in high-risk individuals (Ruderman and Schneider, 1990; Wasserman and Zinman, 1994; Williams, 2001). Both observational studies and intervention trials have shown strong beneficial effects of physical activity in reducing insulin resistance and glucose intolerance (Dunstan et al., 2004; Ezzati et al., 2004; Healy et al., 2008).
Studies have shown a higher prevalence of type 2 diabetes mellitus in Ghana than previously thought. This prevalence is higher than that of the world's estimate which raises concern that needs to be critically addressed. Again, studies have revealed that rapid urbanization has led to changes in food consumption patterns, physical inactivity and prevalence of obesity in adult Ghanaians. It is in this light that this study was conducted to assess the relationship between dietary practices, level of physical activity and body mass indices of Type 2 Diabetics in Ghana. The findings of the study will highlight some of the nutrition problems faced by diabetics to guide nutrition education during counseling sessions at various hospitals in Ghana.
Study design, location and population
This study, which was a cross-sectional survey, was carried out at the National Diabetes Management and Research Centre at Korle-Bu Teaching Hospital (KBTH) in the Greater-Accra Region of Ghana. The center serves as the Diabetic Clinic of the KBTH. Korle-Bu Teaching Hospital is one of the two tertiary health facilities in Ghana and a referral hospital; so it was envisaged that it would have a higher number of Type 2 diabetic patients to select a sample from. The target population was adults diagnosed with Type 2 diabetes visiting the Diabetes Centre. Both male and female diabetic patients aged 18 years and above who reported for regular clinic visits were eligible for inclusion.
Sample and sampling procedure
Purposive sampling technique was used to select participants who were willing to participate in the study. On clinic days, while patients were waiting to see the doctor, the researchers explained the purpose of the study to the patients and assured them of the confidentiality of the responses, after which their cooperation was solicited. This procedure was followed on each clinic visit until the end of the data collection period. Patients of established DM2 status and willing to participate in the study were selected. In all 120 diabetic patients were selected and participated in the study.. The data were collected between July 29, 2013 and October 2, 2013 on week days.
Data Collection
Instruments for data collection
The instruments used for data collection included a structured questionnaire, a 24-h dietary recall, a food frequency questionnaire, anthropometry and the Global Physical Activity Questionnaire (GPAQ).
A structured questionnaire consisting both open-ended and closed-ended questions was used to obtain information on respondents’ background characteristics and dietary practices. Dietary practices of respondents were assessed using five dietary practice-related questions by which respondents were classified as having good, fair or poor dietary practices. The response to each question was scored either 0 for inadequate practice or 1 for adequate practice. The highest attainable score was 5 and minimum score was 0. Scores of respondents were classified as follows: respondents with scores of 5 were classified as having good dietary practices; scores of 4 as fair dietary practices; scores between 0-3 as poor dietary practices.
A food frequency questionnaire (FFQ) comprising 71 commonly consumed food items from the Ghana Six Food Groups was used to determine the frequency of food consumption. The responses were used to provide descriptive information about respondents’ habitual food consumption patterns, dietary diversity and hence dietary quality (classified as adequate, fair or poor). Diets including at least one food item from 5 to 6 food groups daily were rated as adequate; diets including at least one food item from 4 food groups daily were rated as fair; Diets including a food item from 3 or less food groups were rated as poor.
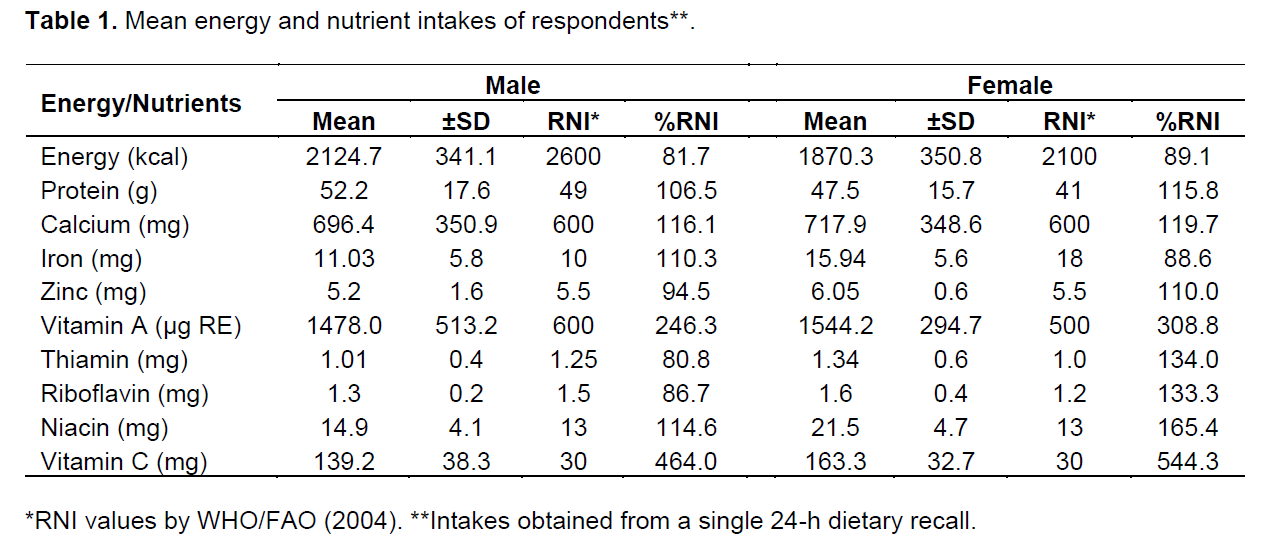
A 24-h dietary recall method was used to determine the energy and nutrient intakes of respondents. Estimated portions of the various food items consumed by the respondents in the 24-h dietary recall were converted into weights of food in grams using a food conversion table for analysis of energy and nutrients. The energy and nutrient contents of foods were calculated using the ESHA Food Processor Plus Software (Version 10). Adequacy of respondents' nutrient intakes were evaluated by comparing the computed values of energy and nutrient intakes of male and female respondents to the Recommended Nutrient Intakes (RNIs) by WHO/FAO (2004).
The levels of physical activities of respondents were assessed using a modified Global Physical Activity Questionnaire (GPAQ) by World Health Organization (2002). Physical activity was classified as low, moderate and high using the GPAQ (WHO, 2002). Weights and heights measurements were used to determine respondents’ body mass indices (BMIs) following standard procedures described by Gibson (2005). The World Health Organization classification was used to assess nutritional status of the respondents. BMI was classified as underweight, normal, overweight, and obese (WHO, 2000).
Data analysis
Data were analyzed using the Statistical Package for the Social Sciences (SPSS Version 20.0). Means and standard deviations were generated for continuous variables and frequencies for categorical variables. Pearson's correlation coefficient statistic was used to test associations between dietary practices, physical activity and BMI of respondents at 5% level of significance
Ethical consideration
Ethical approval for the study was granted by Noguchi Memorial Institute for Medical Research (NMIMR) Institutional Review Board (IRB), University of Ghana, Legon (Reference number: NMIMR-IRB CPN 110/12-13). Verbal consent was obtained from the respondents after details of the nature and procedures of the study were clearly communicated to them. They were also assured confidentiality of the data collected.
Limitations of the study
Limitations experienced in the study involved mainly the research design and the use of the 24 h recall. The purposive sampling technique was used and working in only one health care centre, may not capture a full representation of the wider population of diabetics. Again, estimates of food intakes given by respondents may not be accurate because the 24-h recall relied on the memory of respondents. They may have overestimated or underestimated foods eaten which may affect calculations of energy and nutrient intakes. Notwithstanding these limitations, the results provide some ideas about the dietary practices of the respondents which could be generalized to practices of diabetics in Ghana. For these reasons, conclusions could only be made regarding diabetic patients at the Korle-Bu Teaching hospital. However, inferences could be made regarding dietary practices, physical activity and body mass indices of Type 2 diabetic patients.
Background information of respondents
One hundred and twenty (120) respondents comprising 82 females and 38 males participated in the study. They were aged between 33 and 77 years (with a mean age of 50.7 ± 10.67 years). Seventy-eight percent (78%) were married while the rest were widowed, single or divorced. About 88% of the respondents had formal education ranging between primary and tertiary level. Half (51%) of the respondents were employed in the informal sector as traders and artisans, 27.5% were employed in the formal sector as civil servants, 15% were pensioners and the rest (7%) were unemployed. The average monthly income of the respondents was GH₵ 236.7±148.55. The national daily minimum wage at the time of the study was GH₵5.24 which translates to approximately GH₵162.44 a month (Ghana Statistical Service, 2013). Even though the average monthly income of respondents is greater than the minimum wage of the country, majority (75%) of the respondents were in Ghana’s lower income bracket. As such, the harsh economic conditions prevailing at the time of the study is likely to make it difficult for them to prepare good and diversified diets and also purchase their medications which would negatively affect the management of their condition. Majority (88.3%) of the respondents had lived with type 2diabetes for a year or more; 34% for one to five years, and 52.5% having lived with the condition for six years or more.
Dietary practices and nutrient intakes of respondents
Majority (95%) of the respondents ate three times a day with 5% eating twice daily. Amoah et al. (2006) recommended that diabetics should eat three meals a day about the same time every day to maintain a fair control of their blood glucose levels. Respondents in this study seemed to have adhered to this recommendation. Mohammed et al. (2013) in a study in Saudi Arabia, on the contrary, reported fewer respondents (59.9%) who ate three meals daily. Ninety five percent (95%) of the respondents ate breakfast, lunch and supper each day, 3.3% ate only breakfast and supper; and 1.7% ate breakfast and lunch. Most (85%) of the respondents ate either one or two snacks on a daily basis in addition to their meals. Breakfast, lunch, supper and snack con-sumption as well as meal timing have been reported to play an important role in energy intake and weight management (Taylor et al., 2004). This could help diabetics manage their weights and also properly control blood sugar levels. It is therefore commendable that most respondents consumed three meals and snacks.
Generally, the dietary practices of most respondents were good (71.7%), though, 28.3% had poor to fair dietary practices. According to Pastors et al. (2002), appropriate dietary practices are basic and integral parts of diabetes management and may lead to the reduction of the development of disease complications by improving risk factor profiles. The dietary practices of respondents in this study therefore are encouraging hence they should be urged to continue with the practices to enhance their health status. These findings however differ from the study conducted on dietary practices among patients with type 2 diabetes in Riyadh, Saudi Arabia which revealed inadequate dietary practices of respondents (Mohammed et al., 2013).
Even though 95% of respondents consumed three meals daily, only 67% had good quality and diversified diets. It must be noted however that number of meals consumed may not necessarily be a good measure of diet quality especially if the meals are not diversified. Lack of variety in the diet, skipping meals, and generally low income levels may account for poor or fair diet qualities of some of the respondents.
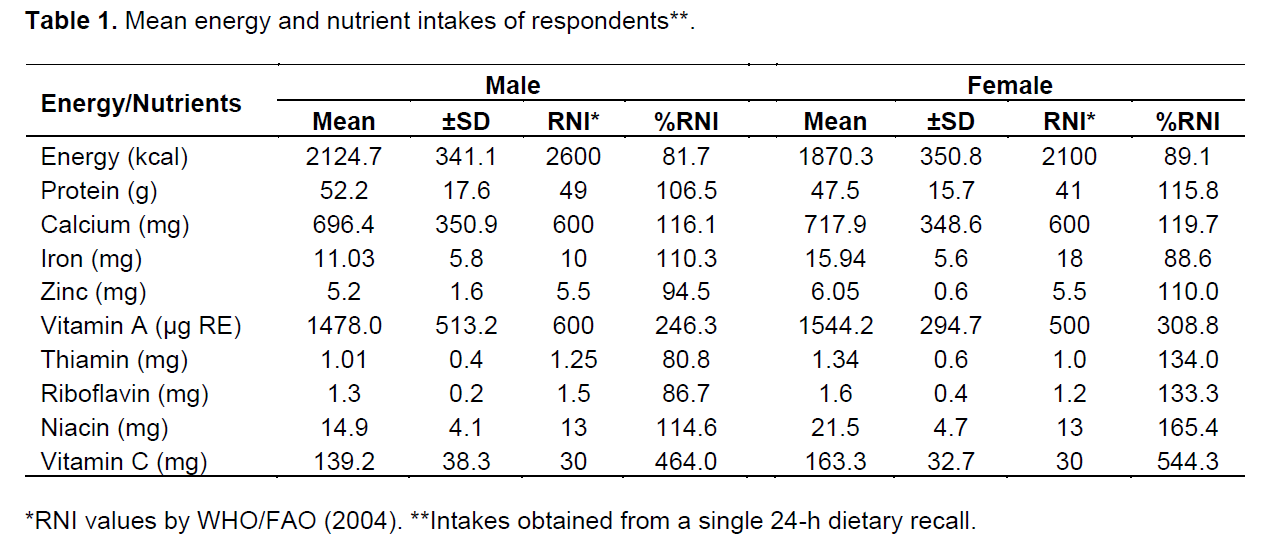
Table 1 presents the mean energy and nutrient intakes of respondents. Males had a mean calorie intake of 2,124.7 kcal while females had 1,870.3 kcal. Female respondents met 89% of the recommended energy intake while the males met 82% of recommended energy intake. The body needs energy for maintaining metabolic activities, support growth and maintenance and for physical activity. Inadequate intake as observed in this study may lead to breakdown of tissues and fat for energy. This situation is not good for diabetics hence the need to encourage adequate consumption of carbohydrate-based foods, especially the complex. Both male and female respondents exceeded the RNIs for protein, calcium, Vitamin A, Niacin, and Vitamin C.Description of daily physical activity of respondents
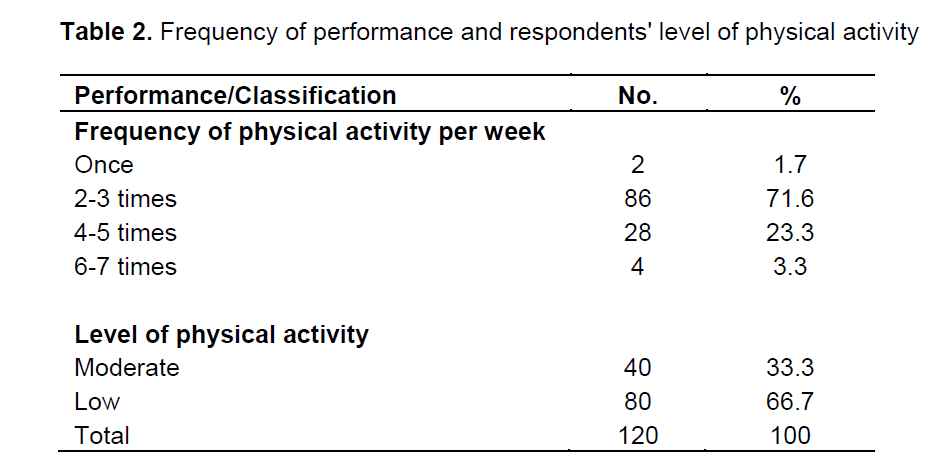
Assessment of physical activity revealed that two-thirds (67%) of the respondents' level of physical activity was low although 95% of the respondents exercised 2 to 5 times in a week. This indicates that the intensity of their exercise was low. Only a third (33%) had moderate level of physical activity (Table 2). According to Warburton et al. (2006), regular physical activity helps prevent some chronic diseases in adults. In some cohort studies in United States, it was observed that persons who maintained physically active lifestyles developed impaired glucose tolerance and type 2 diabetes mellitus less often than do those with a sedentary lifestyle (Hu et al., 1999; Burchfiel et al., 1995; Helmrich et al., 1991). Helmrich et al. (1991) also reported that men who exercised regularly, at moderate or vigorous intensity, had a 35% lower risk of developing type 2 diabetes mellitus than men who were sedentary.
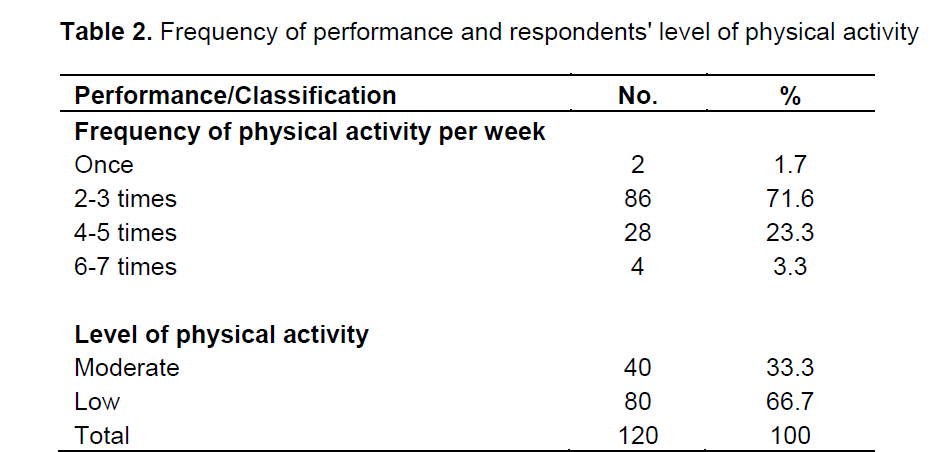
Although health benefits of exercise are well-established, a U.S study by Nelson et al. (2002) revealed that 69% of people with type 2 diabetes did not engage in sufficient physical activity, a finding which is similar to what was observed in this study. As such, developing strategies to increase physical activity in respondents in this present study would be highly desirable. This is because besides the health benefits listed above, physical activity helps increase insulin sensitivity, maintains blood pressure and blood fat levels of the diabetic patient (Williams, 2001). There was no statistically significant difference between the level of physical activity of males and females (p=0.165) in this study sample. However, a statistically significant difference existed between age and level of physical activity of respondents (p=0.043). Physical activity of respondents decreased with age. Diabetics should therefore be encouraged to engage in moderate physical activities as they get older to help improve glycemic control so as to prevent diabetes complications.
Anthropometric measurements of respondents
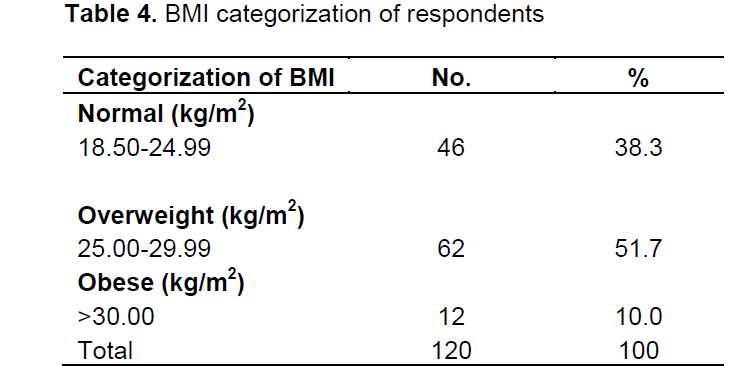
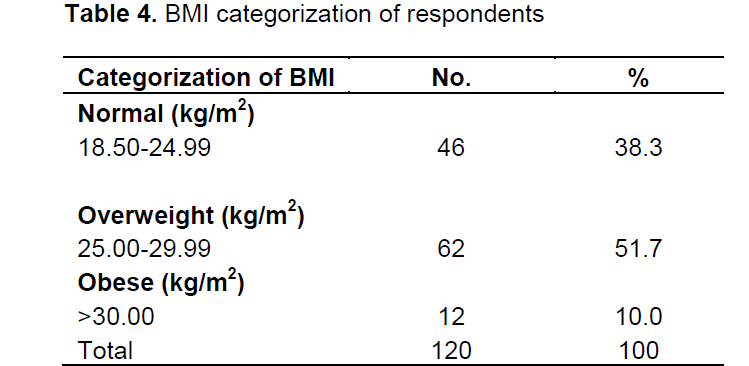
Mean weights, heights and BMIs of respondents are presented in Table 3. The heights of respondents ranged between 1.49 and 1.74 m, while their weights were between 43 and 90 kg. The mean BMI of the study sample was 24.4 ± 3.17 kg/m2 which is slightly lower and better than that reported in the study by Danquah et al. (2012) among type 2 diabetics (BMI of 25.9 ± 5.1 kg/m2) in urban Ghana. Table 4 presents the categorization of BMIs of respondents. About a half (52%) of the respondents were overweight and 10% were obese. Only 38% of the sample had normal BMIs. Findings of this study are similar to a study on type 2 diabetes mellitus in urban Ghana by Danquah et al. (2012). They reported that about a half (53%) of their respondents were overweight. This study also compares well with Abubakari and Bhopal (2008) with respect to prevalence of obesity in West Africa, which was reported to be 10%. This suggests that the findings of this study might be a good representation of what is going on in West Africa.

There was no significant difference between the BMIs of males and females (p=0.336), indicating that BMIs of respondents were not influenced by gender in this study sample. There was a statistically significant relationship between age and BMIs of respondents, with BMI increasing with age (p=0.00). Close to 41% of respondents who were overweight or obese were aged 50 years and above. This finding confirms the report by the Expert Committee on the Diagnosis and Classification of Diabetes Mellitus (2007) that Type 2 diabetes mellitus is more prevalent in older overweight or obese individuals. Respondents should therefore be encouraged to maintain healthy weights as they grow older to help improve glycemic control so as to avoid complications of the disease.
A positive correlation, though weak (r2 = 0.150), but statistically insignificant (p = 0.101) existed between dietary practices and diet quality of respondents, suggesting that as respondents dietary practices improved, their diet quality would also improve. A positive correlation (r2= 0.213) existed between level of physical activity and BMI which was of statistical significance (p = 0.019). This suggests that as respondents’ physical activity increased, the BMI also improved. As such, diabetics need to engage in regular moderate physical activities, at least five times a week, to be able to maintain healthy weights. There was also a positive correlation (r2 = 0.217) between diet quality and BMI which was statistically significant (p = 0.017).
CONCLUSION AND RECOMMENDATION
In conclusion, dietary practices and diet quality of type 2 diabetics attending clinic at Korle-bu Teaching hospital were good but their levels of physical activity were generally low. Overweight/Obesity is however high among the respondents. Whereas dietary practices did not significantly affect diet quality of respondents, as diet quality increased, BMIs improved. Increased physical activity also improved BMIs of respondents.
It is therefore recommended that both overweight and obese diabetics should be encouraged to achieve healthy weights by engaging in moderate physical activities to effectively manage the condition. There is also the need to emphasize education on diet diversity for diabetics to help them make healthy food choices to enable them manage the condition well.
The authors have not declared any conflict of interests.
REFERENCES
|
Abubakari AR, Bhopal RS (2008). Systematic review on the prevalence of diabetes, overweight/obesity and physical inactivity in Ghanaians and Nigerians. Public Health 122(2):173-182.
crossref
|
|
|
|
Amoah AGB, Owusu SK, Adjei S (2002). Diabetes in Ghana: a community based prevalence study in Greater Accra. Diabetes Res. Clin. Pract. 56:197-205.
crossref
|
|
|
|
Amoah AGB (2003). Sociodemographic variations in obesity among Ghanaian adults. Public Health Nutr. 6:751-757.
crossref
|
|
|
|
Amoah AGB, Owusu AA, Owusu SK (2006). Living well with diabetes. Diabetes Outreach Programme, Charlottesville, Virginia, USA; pp. 11-13.
|
|
|
|
Banini AE, Allen JC, Allen HG, Boyd LC, Lartey A (2003). Fatty acids, diet, and body mass Indices of type II diabetic American whites and blacks and Ghanaians. Nutrition 19:722-726.
crossref
|
|
|
|
Begum FAMA, Azad AK, Alim MA, Ekram ARMS (2004). Nutritional status of diabetic patients attending a district level diabetic center. TAJ 17(2):89-92.
|
|
|
|
Boule NG, Haddad E, Kenny GP (2001). Effects of exercise on glycemic control and body mass in type 2 diabetes mellitus. JAMA 286:1218-1227.
crossref
|
|
|
|
Burchfiel CM, Sharp DS, Curb JD, Rodriguez BL, Hwang LJ, Marcus EB, Yano K (1995). Physical activity and incidence of diabetes: The Honolulu Heart Program. Am. J. Epidemiol. 141:360-368.
crossref
|
|
|
|
Cooper R, Rotimi C (1997). Hypertension in blacks. Am. J. Hypertens 10:804-812.
crossref
|
|
|
|
Danquah I, Bedu-Addo G, Terpe K, Micah F, Amoako YA, Awuku YA, Dietz E, Giet MV, Spranger J, Mockenhaupt FP (2012). Diabetes mellitus type 2 in urban Ghana: characteristics and associated factors. BMC Public Health12:210.
crossref
|
|
|
|
Dunstan DW, Salmon J, Owen N, Armstrong T, Zimmet PZ, Welborn TA (2004). Physical activity and television viewing in relation to risk of undiagnosed abnormal glucose metabolism in adults. Diabetes Care 27:2603-2609.
crossref
|
|
|
|
Ezzati M, Lopez A, Rodgers A, Murray C (2004). Comparative quantification of health risks: Global and regional burden of disease due to selected major risk factors. Geneva: World Health Organization. 729.
|
|
|
|
Ghana Statistical Service. Ghana Announces New Minimum Wage: Raises it by 17%. 2013.
|
|
|
|
Gibson RS (2005). Principles of nutritional assessment. 2nd edition. New York: Oxford University Press, USA.
|
|
|
|
Gordon BA, Benson AC, Bird SR, Fraser SF (2009). Resistance Training Improves Metabolic Health in Type 2 Diabetes: A Systematic Review. Diabetes Res. Clin. Pract. 83:157-175.
crossref
|
|
|
|
Healy GN, Wijndaele K, Dunstan DW, Shaw JE, Salmon J, Zimmet PZ (2008). Objectively measured sedentary time, physical activity, and metabolic risk: The Australian diabetes, obesity and lifestyle study (AusDiab). Diabetes Care 31:369-371.
crossref
|
|
|
|
Helmrich SP, Ragland DR, Leung RW, Paffenbarger RS (1991). Physical activity and reduced occurrence of non-insulin-dependent diabetes mellitus. N. Engl. J. Med. 325:147-152.
crossref
|
|
|
|
Hu FB, Sigal RJ, Rich-Edwards JW, Colditz GA, Solomon CG, Willett WC, Speizer FE, Manson JE (1999). Walking compared with vigorous physical activity and risk of Type 2 diabetes in women: A prospective study. JAMA 282:1433-1439.
crossref
|
|
|
|
Knowler WC, Barrett-Connor E, Fowler SE (2002). Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N. Engl. J. Med. 346:393-403.
crossref
|
|
|
|
Kulkarni K, Castle G, Gregory R, Holmes A, Leontos C, Powers M, Snetselaar L, Splett P, Wylie-Rosett J (1998). Nutrition practice guidelines for Type 1 diabetes mellitus positively affect dietitian practices and patient outcomes. The Diabetes Care and Education Dietetic Practice Group. J. Am. Diet. Assoc. 98(1):62-70.
crossref
|
|
|
|
Kyiamah K (2009). Elimination of trans-fatty acids from the food chain in Ghana. Press release to the President of Ghana.
|
|
|
|
Ministry of Health (2010). Dietary and physical activity guidelines for Ghana. pp. 1-71.
|
|
|
|
Mohammed BA, Almajwal AM, Saeed AA, Bani IA (2013). Dietary practices among patients with type 2 diabetes in Riyadh, Saudi Arabia. J. Food Agric. Environ. 11(2):110-114.
|
|
|
|
Motala A, Ramaiya K (2010). Diabetes: The hidden pandemic and its impact on Sub-Saharan Africa. Diabetes Leadership Forum, September 30, 2010; Johannesburg. pp. 1-48.
|
|
|
|
Nelson KM, Reiber G, Boyko EJ (2002). Diet and exercise among adults with type 2 diabetes: findings from the Third National Health and Nutrition Examination Survey (NHANES III). Diabetes Care 25:1722-1728.
crossref
|
|
|
|
Pan X, Li G, Hu Y (1997). Effects of diet and exercise in preventing NIDDM in people with impaired glucose tolerance. Diabetes Care 20:537-544.
crossref
|
|
|
|
Pastors JG, Warshaw H, Daly A, Franz M, Kulkarni K (2002). The evidence for the effectiveness of medical nutrition therapy in diabetes management. Diabetes Care 25(3):608-613.
crossref
|
|
|
|
Pi-Sunyer FX, Maggio CA, McCarron DA, Reusser ME, Stern JS, Haynes RB, Oparil S, Kris-Etherton P, Resnick LM, Chait A (1999). Multicenter randomized trial of a comprehensive prepared meal program in Type 2 diabetes. Diabetes Care 22(2):191-197.
crossref
|
|
|
|
Ramachandran A (2004). Epidemiology of type II diabetes mellitus in Indians. International Conference on Diabetes and Nutrition, International Life Science Institute, New Delhi.
|
|
|
|
Ruderman NB, Schneider SH (1990). Exercise and diabetes: New insights and therapeutic goals. Diabetes Care 13: 804-805.
|
|
|
|
Saleh A, Amanatidis S, Samman S (2002). Cross-Sectional study of diet and risk factors for metabolic diseases in a Ghanaian population in Sydney, Australia. Asia Pac. J. Clin. Nutr. 11:210-216.
crossref
|
|
|
|
Sobal J (2001). Globalization and the epidemiology of obesity. Int. J. Epidemiol. 30:1136-1137.
crossref
|
|
|
|
Taylor E, Missik E, Hurley R, Hudak S, Logue E (2004). Obesity Treatment: broadening our perspective. Am. J. Health Behav.28:242-249.
crossref
|
|
|
|
The Expert Committee on the Diagnosis and Classification of Diabetes Mellitus (2007). Position statement of the expert committee on the diagnosis and classification of diabetes mellitus. Diabetes Care 30(supplement l):S42.
crossref
|
|
|
|
Tuomilehto J, Lindstrom J, Eriksson JG (2001). Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. N. Engl. J. Med. 344:1343-1350.
crossref
|
|
|
|
Warburton DER, Nicol CW, Bredin SSD (2006). Health benefits of physical activity: the evidence. CMAJ 174(6):801.
crossref
|
|
|
|
Wasserman D, Zinman B (1994). Fat distribution and weight gain as risk factors for clinical diabetes in men. Diabetes Care 17:961-969.
crossref
|
|
|
|
Williams CL (2001). Can childhood obesity be prevented? Am. J. Clin. Nutr. 72:1032-1039.
crossref
|
|
|
|
World Health Organization (2000). Obesity: preventing and managing the global epidemic. Report of a WHO Consultation. WHO Technical Report Series 894. Geneva.
|
|
|
|
World Health Organization 2002. Global physical activity analysis guide. World Health Organization. Geneva, Switzerland.
|
|
|
|
World Health Organization/Food and Agriculture Organization (2004). Vitamin and mineral requirements in human nutrition, 2nd ed., Bangkok, Thailand.
|
|
|
|
Zimmet P, Alberti MM, Shaw J (2001). Global and societal implications of the diabetes epidemic. Nature 414:782-787.
crossref
|