ABSTRACT
This trial aims at testing the efficacy of weekly sexo-reproductive health educational text messages to improve perception of adolescent girls on sexo-reproductive health in Cameroon. This is a single-centered randomized controlled single-blinded trial. Adolescent girls aged 10 to 19 years in the Kumbo West Health District are the target population. A central computer generated randomization list was used to prevent selection bias and enable the production of the comparable groups for this trial. Allocation concealment (1:1) was determined by sequentially numbered sealed opaque envelopes. A total of 460 participants either receive the mobile phone text message or no text message. Data was collected at baseline, three month and six month intervals. A blinded program secretary sent out text messages and record delivery. The studies primary outcomes were improved knowledge and practices towards sexo-reproductive health, while its secondary outcomes were improved behaviour and attitudes towards sexo-reproductive health. Analysis was by intention-to-change behaviour. Covariates and subgroups were taken into account. This trial investigated the potential of SMS messages on sexo-reproductive health education to improve adolescent girl’s perception to attain better health outcomes. This trial contribute to the growing body of evidence on the use of mobile phone technology as a complementary strategy for strengthening health systems and achieving health-related goals oriented towards adolescent girls.
Key words: Mobile phone, sexo-reproductive health, improved perception, randomization.
Abbreviation:
ABBREVIATIONS: ASRH, Adolescent sexo-reproductive health; CONSORT, Consolidated Standards for Reporting Trials; DS-RHNAG, determinants of ¨Sexo-Reproductive¨ Health Needs of Adolescent Girls; HIV, Human Immune Deficiency Virus; KWHD, Kumbo West Health District; MASHS, Mobile Adolescent Sexo-Reproductive Health Scheme; SPIRIT, Standard Protocol Items, Recommendations for interventional Trials; SMS, Short Message Service; SRH, Sexo-Reproductive Health; SPSS, Statistical Package for Social Sciences; WHO, World Health Organization; WMA, World Medical Association.
Adolescent girls in sub-Saharan Africa face various sexo-reproductive health risks such as unplanned pregnancy and sexually-transmitted infections (STIs), including human immunodeficiency virus (HIV) infections (Renzaho et al., 2017). Adolescent girls are less likely than older women to access sexo-reproductive health care,
including modern contraception and skilled assistance during pregnancy and childbirth (UNFPA, 2015; WHO, 2018). Many are poor, have little control over household income, have limited knowledge about sexo-reproductive health issues, and lack the ability to make independent decisions about their health (UNFPA, 2015). Moreover, they often do not have access to health care that meets their specific sexo-reproductive health needs. Most importantly, adolescent girls sexo-reproductive health needs often go unnoticed or are viewed through the lens of religious and cultural values, which in turn limit the possibility to provide highly needed care (Engen, 2013).
In Sub-Saharan Africa, few interventions have examined digital health solutions to adolescent sexo-reproductive health (L’Engle et al., 2016) (most often they are online based and hardly reach disadvantaged local communities) but yet none have primarily focused exclusively on using offline mobile phone short message service (SMS) interventions that will create a larger impact (L’Engle et al., 2016). Mobile text messages using the short message service (SMS) are a cheap and non-invasive means of communication that can be used to convey health related messages to mobile phone users (Mbuagbaw et al., 2012). The World Health Organization (WHO) has prioritized the use of new technologies to assist healthcare delivery in resource-limited settings (WHO, 2018). For many adolescents especially girls in developing countries, the mere onset of puberty that occurs during adolescence marks a time of heightened vulnerability to early pregnancy, human immuno-deficiency virus disease, leaving school, child marriage, sexual exploitation, coercion and violence (Habibolah et al., 2016). Text-messaging programs have been shown to improve adolescents’ reproductive health knowledge and had the potential to lower pregnancy risk for sexually active adolescent girls (Ippoliti and L’Engle, 2017). Another study reported high satisfaction with two way text messaging (Slawa et al., 2017). These findings suggested that the more feasible application of the mobile phone in health would be the SMS. Equally, on our search for papers on mobile phone programs for adolescent sexual and reproductive health in low- and middle-income countries, we found out some projects (70%) relied on text messaging/short message service (SMS) to transmit sexo-reproductive health information to their users. These programs demonstrated the wide utility of SMS as a way to transmit and facilitate knowledge sharing within varied domains of adolescent SRH. Programs such as OneWorld and Education as a Vaccine (EVA) in Nigeria (OneWorld, 2013), mCENAS in Mozambique (Pathfinder Finder, 2017), M-ASSIST (Cell Life, 2013) and Project Khuluma (SHM Foundation, 2013) in South Africa, highlighted the various ways in which SMS has been leveraged to transmit information, support, and counseling on different SRH services.
Text message interventions are capable of producing positive change in preventive health behaviors (Armanasco et al., 2017). We hypothesize that sending one weekly sexo-reproductive health educational message will produce a change in behavior to enhance improved knowledge on adolescent sexo-reproductive health in general and hence better health outcomes. Participants were be selected from randomly selected six health areas of the Kumbo West Health District (KWHD).
Study objectives
Primary objective
The primary objective of this trial will be to investigate the effect of MASHS SMS to usual care versus usual care alone in overcoming unmet adolescent sexo-reproductive health barriers by providing adolescents with accurate, timely, sustainable and engaging information that will improve on their knowledge, attitudes and practices on sexo-reproductive health at 3 and 6 month intervals. The methods to be used to evaluate or measure knowledge are knowledge scores and analytical test such as the Paired T-test or Wilcoxon Signed Rank test and McNemar’s test.
Secondary objectives
The secondary objectives include comparing outcomes such as knowledge of reproductive health, knowledge and ever-use of contraceptive methods, knowledge of HIV/AIDS and sexually transmitted diseases, condom knowledge and attitudes. These comparisons will be performed at 3 and 6 months.
Study design
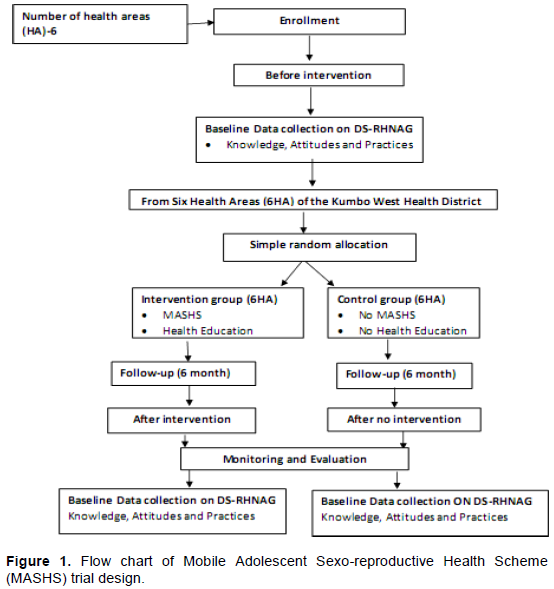
MASHS was implemented by a before-and-after intervention strategy which involve the random selection of the intervention and control groups obtained through cluster sampling such that for the intervention group, a unique SMS update portal named MASHS, which consist of the main operator and the beneficiary who shall be in possession or have access to a mobile phone was used. The operator generates the content of clear and understandable messages based on key variables of adolescent sexo-reproductive health. To start the intervention, MASHS was introduced and explained to the families of participants such that they will be expecting three to five messages from the operator per week for a period of 6 months. Using a concealed 1:1 allocation ratio, adolescent girls at Kumbo West Health District (KWHD) was randomized to receive a text message on sexo-reproductive health or not. Figure 1 shows a flow chart of MASHS study design which is in accordance with the guidelines of the Standard Protocol Items: Recommendations for interventional Trials.
Simple random allocation of participants
This is a parallel group design evaluating the effects of adding weekly SMS messages using mobile phones to usual care (intervention) versus usual care alone (control) among adolescent girls. Eligible and consenting girls were randomized to intervention and control arms using a 1:1 allocation ratio by opaque sealed envelope method. A computer generated randomization list was generated using random block sizes of 2, 4 and 6 to prevent selection bias and enable the production of the comparable groups for this trial. The allocation codes was then put in sequentially numbered opaque sealed envelopes and administered by the trained research staff at the KWHD services. Trained interviewers - blinded to group allocation - collected baseline data using a pretested data collection form containing socio-demographic data, sources of information on, and knowledge of reproductive health, knowledge and ever-use of contraceptive methods, knowledge of HIV/AIDS and sexually transmitted diseases, condom knowledge and attitudes, and use and perceptions of health services at baseline, 3 and 6 month intervals. The data analyst was also blinded to group allocation.
Trial setting
Cameroon is a culturally diverse coastal country in Africa, which lies on the western side of Africa on the Eastern Atlantic Ocean (World Population Review, 2018). Cameroon is bordered by Chad, Nigeria, the Central African Republic, Gabon, Equatorial Guinea, and the Republic of the Congo. The 2018 Cameroon population is estimated at 24.68 million (World Population Review, 2018). The study was conducted in Kumbo located in the North West region of Cameroon. This study was precisely carried out in the Kumbo West Health District (KWHD), a semi-urban/rural community with many adolescent girls. The study involved community mobilization and participatory approaches which specifically was implemented in six randomly selected health areas of the KWHD for the study. According to the Department of Economic and Social Affairs; Population Division of the United Nations (United Nations Population Division, 2017), 22.8% adolescent girls of the total population of KWHD. Applying this population model, a total of 25120 adolescent girls was involved in the KWHD out of total population of 110,173.
Participants: Inclusion/exclusion criteria
The study included adolescent girls aged between 10 and 19 years; the parent or guardian or adolescent girl must own a mobile phone and can read text messages. The study involved selected residents of the community who have lived in that community for at least a month. Informed assent and consent is a prerequisite for participating in the study, provided orally and in writing. Participants who refuse to participate in the study and those aged less than 10 years or above 19 years were excluded.
Intervention
Mobile-based adolescent sexo-reproductive health scheme (MASHS) - SMS
A short text message was sent to the participants in the intervention group in English. The content of the message was motivated and act both as a reminder and a cue to action. The message was sent through a phone number they can call back or text if they need help. The content varied so as to retain participants' attention throughout the period of the study. The program secretary have a list of phone numbers to which he/she will send the messages every week and will use the 'delivery report' function to ensure that the messages have been delivered. One message was sent per week in the morning of a chosen day. The average cost for text messages on any networks in Cameroon is 50 CFA Frs. MASHS provided adolescents with a sustainable/long-term mobile based Reproductive Health Scheme that will basically involve the provision of accurate and persuasive information on how adolescents can meet their sexo-reproductive health needs. MASHS’ philosophical paradigm is simply using the mobile phone as the main medium of relaying information and this is such that the scheme shall use the comprehensive education base approach to; reduce the vulnerability of adolescent girls to the risk of; early pregnancy and its complications, acquiring HIV/AIDS, leaving school, child marriage, sexual exploitation, coercion and violence. MASHS implementation also improve the knowledge of adolescent girls on contraceptive use, dialogue between adolescents and their peers, parents and guardians, encourage adolescent girls to visit health facilities for individual counseling on sexo-reproductive health. The MASHS predictive model has been built based on the health promotion theory.
Health education
Health education on adolescent sexo-reproductive health was delivered to the intervention group. These were done for one to three times per month for a period of 6 months.
Control
In the control arm, subjects receive the usual care provided to all adolescent girls as concerns sexo-reproductive health education which includes education at schools and reproductive health services delivered at health facilities. They were not sent text messages, but interviewed at baseline, 3 and 6 months.
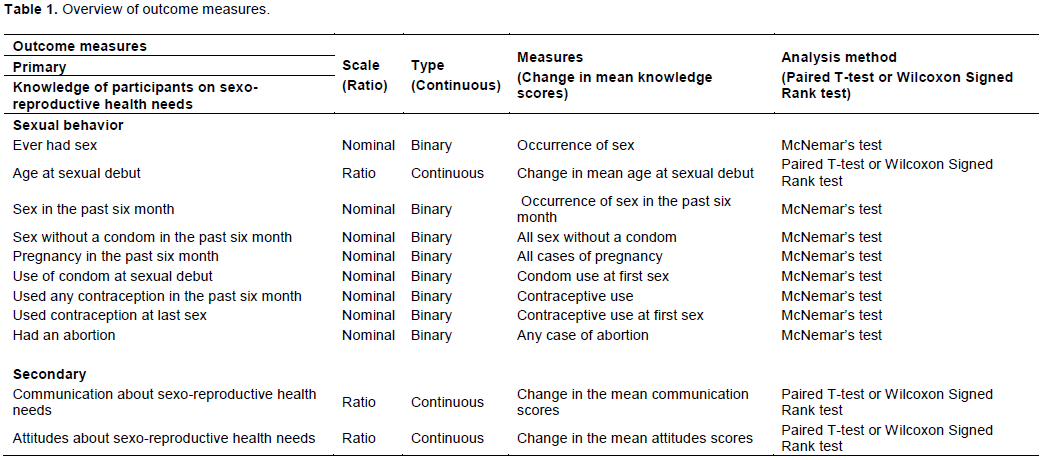
Outcome measures
Our primary outcome was the knowledge of participants on sexo-reproductive health needs and their sexual behaviours. Our secondary end point was communication and attitudes about sexo-reproductive health needs (Table 1).
Duration
The trial was run for six months, with outcome assessment at baseline, 3 and 6 month intervals.
Sample size
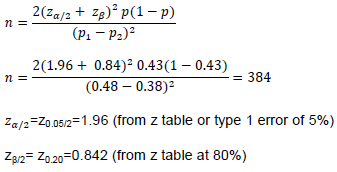
The sample size calculation for this trial study was based on sample size calculation for comparison between two groups (Jaykaran and Tamoghna, 2013) as follows:
p1-p2=pooled prevalence=(prevalence in intervention group (p1) + prevalence in control group (p2)/2 Considering a 20% non-response rate, n = 460. Hence, 230 subjects for the control group and 230 subjects for the intervention group.
Analysis plan
The analysis and reporting of the results follow the CONSORT-SPIRIT guidelines (Schulz, 2010). The statistician/data analyst was blinded to the study group. The process of adolescent selection and flow throughout the study was summarized using a flow-diagram. The analysis results of adolescent girl’s demographics and baseline outcome variables (both primary and secondary) was summarized using descriptive summary measures: Expressed as mean (standard deviation) or median (minimum-maximum) for continuous variables and number (percent) for categorical variables.
Ethical considerations
The trial was conducted in compliance with the local protocol and applicable regulatory requirements in Cameroon. The study was approved by the Institutional Review Board of the Faculty of Health Sciences of the University of Buea (IRB-FHS No: 765-03). Any deviations from the protocol was reported and explained. The study was conducted in accordance with the Helsinki declaration (WMA, 2013) and other established clinical practice guidelines for research on human subjects. Research personnel approached all potentially eligible adolescent girls who fulfill eligibility criteria for assent/consent. All adolescents’ girls sign a consent form or give verbal consent to participate in the trial.
The potential of mobile phone technology to improve health outcomes is a domain worth exploring, especially in this era of increased uptake and dependence on mobile phones. Studies investigating the use of text messages to improve adolescent sexual and reproductive health yielded varied results (L’Engle et al., 2016; Salam et al., 2016, Ippoliti et al., 2017). The implementation of MASHS contributes in the improvement of adolescent sexo-reproductive health and prevention of adolescent pregnancies in Cameroon. Mobile phones areinexpensive, portable, and accessible. The penetration of mobile phone networks in many low- and middle-income countries surpasses other infrastructure such as paved roads and electricity, and dwarfs fixed Internet deployment (WHO, 2018). This promising approach called mHealth, which uses mobile phones to improve adolescent health knowledge, behaviors and outcomes, has advantages when used in health programming for young people.
Adolescents commonly report low SRH knowledge and risky sexual behaviors (L’Engle et al., 2016), but they also face barriers to care such as provider bias and fear of stigma, refusal, and embarrassment in seeking information and services. Mobile phone solutions may help overcome many of these barriers by providing accurate, timely, engaging information and appropriate care for highly sensitive adolescent sexo-reproductive health topics (Ippoliti et al., 2017). Mobile phones offer privacy in comparison with face-to-face meetings with health care providers, and they can provide young people with tailored and anonymous health information without stigma or judgment (Ippoliti et al., 2017). Furthermore, young people are responsive to and excited about using new technologies for SRH promotion. Better assessments of mHealth solutions for young people are needed to rigorously evaluate whether they are a viable and effective strategy for reaching adolescents and improving ASRH behaviors in particular (Shiferaw et al., 2014). Although a few published reviews have examined digital health solutions to ASRH, none have focused exclusively on mobile phone interventions and used a comprehensive definition of ASRH.
MHealth as a technical area has seen increasing interest and promise from both developed and developing countries (Hurt et al., 2016). While published research adolescent sexual and reproductive health from higher income countries on mHealth solutions for SRH is growing, there is much less documentation of SRH mHealth interventions for youth living in resource-poor settings (Ippoliti et al., 2017). Using the mobile phone as the main medium of relaying information, the scheme shall use a comprehensive sexo-reproductive health education (through a two way unique SMS text base messaging) approach to indirectly reduce the vulnerability of adolescents to the risk of early pregnancy and its complications, acquiring HIV, leaving school, child marriage, sexual exploitation, coercion and violence by improving the knowledge of adolescent girls on contraceptive use, improving dialogue between adolescents and their peers, parents and guardians, encouraging adolescents to visit health facilities for individual counseling on sexo- reproductive health.
It has been found in several studies that the use of SMS generally improves health outcomes in resource limited settings like Cameroon. This was exemplified by Nsagha et al. (2016) that SMS improved adherence to anti-retroviral (ARV) medication in Cameroon. The study further established that key constraints which affect adhere to ARV medication can be addressed using SMS. Also, Mbuagbaw et al. (2015) had reported that text messaging interventions improve health outcomes in people living with HIV and other chronic diseases. A study by Bediang et al. (2018) suggested that SMS reminders do not increase treatment success and cure proportions of tuberculosis patients in Cameroon. However, this study showed that the low proportion of tuberculosis patients cured at 6 months may be an underestimation due to a high dropout rate between the fifth and the sixth months of treatment. They recommended future trials should focus on reducing the dropout rate. Finally, the MASHS trial may contribute to the growing body of evidence on the use of mobile phone technology as a complementary strategy for strengthening health systems and achieving health-related goals oriented towards adolescent girls.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
All the principles of a good ethical research was respected. Ethical approval was obtained from the Institutional Review Board of the Faculty of Health Sciences of the University of Buea.
The authors have not declared any conflict of interests.
ASRH, Adolescent sexo-reproductive health; CONSORT, Consolidated Standards for Reporting Trials; DS-RHNAG, determinants of ¨Sexo-Reproductive¨ Health Needs of Adolescent Girls; HIV, Human Immune Deficiency Virus; KWHD, Kumbo West Health District; MASHS, Mobile Adolescent Sexo-Reproductive Health Scheme; SPIRIT, Standard Protocol Items, Recommendations for interventional Trials; SMS, Short Message Service; SRH, Sexo-Reproductive Health; SPSS, Statistical Package for Social Sciences; WHO, World Health Organization; WMA, World Medical Association.
This is part of a Ph.D. thesis by Wirsiy Frankline Sevidzem under the supervision of Professor Nsagha Dickson Shey and co-supervision of Professor Omer Tchikamgou Njajou and Dr. Joseph Besong Besong in the Department of Public Health and Hygiene of the University of Buea. The authors acknowledge all stakeholders including the District Medical Officer of Kumbo West Health District, Regional Delegate for Public Health-North West Region, Chiefs of Health Centres, Data Collectors and Community Leaders who shall be instrumental in the realisation of this study. They equally acknowledge all the participants who participated in this study.
REFERENCES
|
Armanasco AA, Miller YD, Fjeldsoe BS, Marshall AL (2017). Preventive Health Behavior Change Text Message Interventions: A Meta-analysis. American Journal of Preventive Medicine 52(3):391-402.
Crossref
|
|
|
|
Bediang G, Stoll B, Elia N, Abena JL, Geissbuhler A (2018).SMS reminders to improve adherence and cure of tuberculosis patients in Cameroon (TB-SMS Cameroon): a randomized controlled trial. BMC Public Health 18(1):583.
Crossref
|
|
|
|
|
Cell-Life NGO Pulse (2013). Cell-Life: mHealth Project; M-ASSIST, OneWorld.
|
|
|
|
|
Engen I (2013). Adolescent Reproductive Health in Cameroon-Prevention of adolescent pregnancies through access to sexual and reproductive health measures in Cameroon. Oslo and Akershus University College of Applied Sciences.
|
|
|
|
|
Habibolah T, Abbas B, Maryam A, Fatemeh F, Masumeh S (2016). Adolescence Health: the Needs, Problems and Attention. International Journal of Pediatrics 4(2):1423-1438.
|
|
|
|
|
Hurt K, Walker RJ, Campbell JA, Egede LE (2016). Health Interventions in Low and Middle-Income Countries: A Systematic Review. Journal of Health Sciences 8(9):183-193.
Crossref
|
|
|
|
|
Ippoliti BN (2017) Mobile Phone Programs for Adolescent and Youth Sexual and Reproductive Health in Low- And Middle-Income Countries. USAID, K4Health, FHI 360; Available at
View
|
|
|
|
|
Ippoliti BN, L'Engle K (2017). Meet us on the phone: Mobile phone programs for adolescent sexual and reproductive health in low-to-middle income countries. BMC Research Notes - Reprod Health, pp. 1-2.
Crossref
|
|
|
|
|
Jaykaran C , Tamoghna B (2013). How to Calculate Sample Size for Different Study Designs in Medical Research. Indian Journal of Psychological Medicine 35(2):121.
Crossref
|
|
|
|
|
L'Engle K, Mangone ER, Parcesepe AM, Agarwal S, Ippoliti NB (2016). Mobile Phone Interventions for Adolescent Sexual and Reproductive Health: A Systematic Review. PubMed Pediatrics 138(3):e20160884.
Crossref
|
|
|
|
|
Mbuagbaw L, Mursleen S, Lytvyn L, Smieja M, Dolovich L, Thabane L (2015). Mobile phone text messaging interventions for HIV and other chronic diseases: an overview of systematic reviews and framework for evidence transfer. BMC Health Services Research 15:1472-6963
Crossref
|
|
|
|
|
Mbuagbaw L, Thabane L, Ongolo-Zogo P, Lester RT, Mills EJ, Dolovich L, Kouanfack C (2012). The Cameroon Mobile Phone SMS (CAMPS) Trial: A Randomized Trial of Text Messaging versus Usual Care for Adherence to Antiretroviral Therapy. PLoS ONE 7:e46909.
Crossref
|
|
|
|
|
Nsagha DS, Lange I, Fon PN, Assob JCN, Tanue EA (2016). A Randomized Controlled Trial on the Usefulness of Mobile Text Phone Messages to Improve the Quality of Care of HIV and AIDS Patients in Cameroon. The Open AIDS Journal 10:93-103.
Crossref
|
|
|
|
|
OneWorld (2013). Learning about Living Nigeria-Education as a Vaccine (EVA); Available at
View
|
|
|
|
|
Pathfinder F (2017). mCENAS - Mozambique. Path Finder International; Available at
View
|
|
|
|
|
Project K (2013). A mobile phone support group initiative to address the mental health and wellbeing needs of HIV positive adolescents in South Africa, SHM Foundation. Available at
View
|
|
|
|
|
Renzaho A, Kamara J, Georgeou N, Kamanga G (2017). Sexual, Reproductive Health Needs, and Rights of Young People in Slum Areas of Kampala, Uganda: A Cross Sectional Study. PLoS ONE 12(1):e0169721.
Crossref
|
|
|
|
|
Salam RA, Faqqah A, Sajjad N, Lassi ZS, Das JK, Kaufman M, Zulfiqar A (2016). Improving Adolescent Sexual and Reproductive Health: A Systematic Review of Potential Interventions. Journal of Adolescent Health 59(4):11-28.
Crossref
|
|
|
|
|
Schulz KF, Altman DG, Moher D (2010). Statement: Updated guidelines for reporting parallel group randomised trials. Journal of Clinical Epidemiology 340(332):2-6.
Crossref
|
|
|
|
|
Shiferaw K, Getahun F, Asres G (2014). Assessment of adolescents' communication on sexual and reproductive health matters with parents and associated factors among secondary and preparatory schools' students in Debremarkos town, North West Ethiopia. BMC Reproductive Health 11(1):2.
Crossref
|
|
|
|
|
Slawa R, Jessica C, Joshua A, Günther F (2017). Impact of a text messaging program on adolescent reproductive health: a cluster-randomized trial in Ghana. UCD Geary Institute for Public Policy Discussion Paper Series. Available at
View
|
|
|
|
|
United Nations Population Division (2017). Sub-Saharan Africa - Adolescents and Young People Dashboard, UN. Available at
View
|
|
|
|
|
United Nations Population Fund (UNFPA) (2015). From childhood to motherhood: Meeting the sexual and reproductive health needs of adolescent girls. UNFPA;
View
|
|
|
|
|
World Health Organization (WHO) (2018). Adolescent Pregnancy.
|
|
|
|
|
World Medical Association (WMA) (2013) Declaration of Helsinki: ethical principles for medical research involving human subjects. The Journal of the American Medical Association 310(20):2191-2194.
Crossref
|
|
|
|
|
World Population Review. Cameroon Population (2018). Demographics, Maps, Graphs. Available at
View
|
|