Full Length Research Paper

ABSTRACT
The study determined the prevalence of malaria parasitemia among pregnant women using Sulphadoxine-pyrimethamine (SP) for intermittent preventive treatment (IPT) and assessed Plasmodium falciparum dihydropteroate reductase (Pfdhfr) and dihydropteroate synthetase (Pfdhps) resistance genes among the subjects. Three hundred and ninety consenting pregnant women attending antenatal clinics in Nnewi, Anambra State, Nigeria were recruited. Of this, 336 of the women were using SP for IPT, while fifty-four of the women were non-users of SP. Polymerase Chain Reaction was used in the characterization of Plasmodium species while the Sanger sequencing method was used in sequencing assay. Of the 336 pregnant women SP users, 73 (21.7%) and, 41 (12.2%) of the neonates had malaria parasitemia while 29 (53.7%) of the 54 non-users of SP and 14 (25.4%) of the babies had malaria parasitemia (p=0.022). Plasmodium falciparum and Plasmodium vivax parasitemia among subjects on IPTp-SP was 38 (11.3%) and 30 (8.9%) respectively. The prevalence of Pfdhfr and Pfdhps resistance genes in pregnant women was 11 (3.3%) and 10 (2.9%) respectively. Malaria parasitemia was significantly higher among non-users of SP. The presence of P. falciparum resistance genes among IPTp-SP users could lead to treatment failures. Therefore, novel drugs should be sought to replace SP.
Key words: Plasmodium, Sulphadoxine-pyrimethamine, pregnancy, polymerase chain reaction (PCR), Resistant gene, Nigeria.
INTRODUCTION
Malaria is an infectious disease caused by parasites of the genus Plasmodium and is transmitted by mosquitoes (Warrell and Gilles, 2002). Malaria is characterized by chills, fever, and generalized body pain (WHO, 2004).
Plasmodium falciparum, Plasmodium vivax, Plasmodium ovale, Plasmodium malariae, and Plasmodium knowlesi are the species that infect humans (Tangpukdee et al., 2009). The most prevalent species of malaria parasites in Nigeria is P. falciparum (greater than 95%) and responsible for the most severe forms of the disease in Nigeria (Umeh et al., 2013). Although P. ovale and P. malariae parasitemia play a minor role in Nigeria, P. malariae is currently isolated from children with mixed infections (Nigeria Malaria Indicator Survey, 2015). Nigeria accounts for the high prevalence of the global malaria burden in sub-Saharan Africa (National Malaria Elimination Programme, 2017; WHO, 2017). This highlights the need to focus on treatment as well as prevention. Nationwide, Malaria prevalence varies widely, ranging from 14% in the South East to 37% in the North West (National Malaria Elimination Programme, 2017; WHO, 2017). In Nigeria, malaria is responsible for the deaths of an estimated 300,000 children per year and contributes to over 4000 maternal deaths annually (WHO, 2017).
Malaria in pregnancy is a serious public health problem that impacts negatively and causes an enormous risk to the mother, fetus, and neonates (Gontie et al., 2020). It is estimated that each year approximately 25 million pregnant women in sub-Saharan Africa live at risk of P. falciparum malaria infection (WHO, 2017). Although malaria during pregnancy might be asymptomatic due to a high level of acquired immunity in mothers residing in high transmission areas (Fagbemi et al., 2020), it is still associated with an increased risk of maternal anemia, spontaneous abortion, stillbirth, prematurity, and low birth weight (Kwala et al., 2021).
Intermittent preventive treatment in pregnancy with sulphadoxine-pyrimethamine (IPTp-SP) is one of the main strategies for protecting pregnant women, fetus, and their newborns against adverse effects of P. falciparum infection (Briand et al., 2009). The development of the drug resistance linked to mutations in P. falciparum dihydrofolate reductase genes (pfdhfr) and P. falciparum dihydropteroate synthetase genes (Pfdhps), is currently threatening the IPTp-SP approach and is one of the greatest challenges of malaria control programs (Fagbemi et al., 2020). Sulphadoxine-pyrimethamine (SP) resistance is linked to the substitution of amino acids in the enzyme dihydropteroate synthetase (dhps) and dihydrofolate reductase (dhfr) in the folate biosynthetic pathway (Brooks et al., 1994; Cowman et al., 1988). Mutations in dhfr confer resistance to pyrimethamine while mutations in dhps confer resistance to sulphadoxine and other sulpha drugs. There are variations in SP mutations, it may be single, double, or triple: the more the mutations, the stronger the resistance. In sub-Saharan Africa, the dhfr triple mutant (Asn- 108 + Ile- 50 + Arg - 59) and dhps double mutant (Gly- 437 = Glu – 540) have been strongly associated with potential resistance (Duraisingh et al., 1998; Triglia et al., 1997). In a study done in Lagos, Nigeria, the mutant strains of P. falciparum were present up to 75.9% of the blood samples of pregnant women (Agomo et al., 2016). In another study done in six districts in the general population of Zambia indicated variations of rates of resistance to SP with mutated dhfr frequency ranging from 71 - 92% and 39- 71% for the double mutant dhps respectively (Akanbi et al., 2009).
Therefore, there is a need for monitoring and surveillance of the efficacy of SP in the treatment of malaria among pregnant women. In the present study, maternal venous blood and neonatal cord blood samples of babies of pregnant women who were users of SP and non-users of SP attending antenatal clinic in Nnewi, a metropolitan city, were assessed for Plasmodium species using a molecular approach. The purpose was to evaluate P. falciparum resistance markers (dhps and dhfr) to SP in the study area and the Nigerian nation at large and to assess the possibility of looking for a novel drug for the treatment of falciparum malaria.
MATERIALS AND METHODS
Study area, design, and population
The study was a cross-sectional study involving pregnant women who were on antenatal visits to maternity and hospitals, primary healthcare centers (PHCCs), and Nnamdi Azikiwe University teaching hospital (NAUTH), Nnewi, Nigeria.
Consent and ethical approval
Ethical approval was obtained from Nnamdi Azikiwe University Teaching Hospital, Nnewi Ethical Committee (NAUTH/CS/66/ VOL.11/158/2018, 22/01/2019) and authorization from primary healthcare centers and maternity and hospitals’ administration. The written and oral informed consent was obtained from each participant before administering the questionnaires. The anonymity of participants involved in this study as well as the confidentiality of information collected was respected.
Sample size determination
A total of 390 participants were enrolled in the study. This was obtained by calculation using the formula as described by Naing, (2003). The formula is n = z2p (1-p)/d2, where n= required sample size, z= confidence level 95% (Standard value of 1.96). p = Prevalence rate of 30% as reported in Imo State, Nigeria by Umeh et al., 2013. d= Desired level of significance 5% (standard value is 0.05). Minimum sample size calculation performed obtained n = 302. However to adjust for non-response, n2 = n/n-f, Where n2 = adjusted sample size; n = unadjusted sample size (302.16); f = non-response rate (10%) = 0.1; n2 = 302.16/1- 0.1; n2 = 302.16/0.9 = 335.73; n2 = 336; Minimum sample size = 336.
A total number of 336 pregnant women taking SP for IPT and 54 pregnant women who were using other anti-malaria drugs for the treatment of malaria were recruited into the study, giving an overall sample size of 390 pregnant women who were recruited and enrolled in the study.
Sampling method / data collection
A stratified sampling method was used in the selection of primary healthcare centers while a convenience sampling method was used in sample collection. The enrolment of the pregnant women into the study was done consecutively until the number of pregnant women required for the study was obtained. Structured questionnaires were administered to the participants after obtaining their informed consent. Data were collected employing structured questionnaires. The study variables included socio-demographic factors, history of use of SP for malaria treatment, and other antimalarial drugs taken during pregnancy, obstetrical and gynecological records.
Sample collection
Blood samples were collected from February to November 2019. Three milliliters of each maternal venous blood and neonatal cord blood sample were aseptically collected from participants and were placed into Ethylene diamine tetraacetic acid (EDTA) containers (Micropiont, United Kingdom). The blood samples were properly labeled in coded numbers and were transported to the laboratory for immediate analysis. For each sample, approximately 20 µl of blood was spotted on a piece of 3 mm filter paper (Whatman, Maidstone, United Kingdom) and was air-dried. The dried filter paper samples were stored in individual zipper plastic bags with a dryer at -20°C until DNA extraction.
Determination of parasite density by Giemsa-stained blood smears
Thick blood smears each measuring about 8 µl was prepared. Each blood smear was labeled with the patient’s identification number. The slides were air-dried in a dust-free environment. Staining of the blood smears was done using a 10% Giemsa stain and examined using 100x oil immersion objective lens of a binocular Olympus microscope by two blinded Laboratory Scientists (WHO, 2015). Determination of parasite density was done as described by WHO (2015). Thick blood films of the participants were made using 8 µl of well-mixed blood. Thin blood films were also prepared. Smears were stained and parasite count was performed as described by Cheesbrough (2006) and WHO (2015) Determination of total WBC was done using Sysmex hematology analyzer as the patient’s actual WBC count was used to calculate parasite density as follows:

The Sysmex KN 21 auto-hematology analyzer used to determine white blood cells (WBC) count is a quantitative automated hematology analyzer for in-vitro diagnostic use in clinical laboratories. The test was performed according to the instructions of the automatic multi-parameter blood counter. Blood films were considered negative if no parasites were detected in oil immersion fields of thick blood films. Thin blood films were also examined for malaria parasites using the 100x objective of the microscope to determine malaria parasite species.
Molecular assay
DNA extraction and purification from dried blood spots (QIAamp DNA Mini kit)
DNA was extracted from a blood spot on filter papers using a QIAamp DNA min kit as described by Chandrasekhar et al. (2016).
Polymerase chain reaction (PCR)
Quick load One Taq one-step PCR master (2X) with catalog number NEB MO486S was purchased from lnqaba Biotech Hartfield South Africa incorporated and used according to the manufacturer’s instruction.
The primers for the detection of P. malariae:
rMAL 1: 5’-ATA ACA TAG TTG TAC GTT AAG AAT AAC CGC-3’
rMAL 2: 5’-AAA ATT CCC ATG CAT AAA AAA TTA TAC AAA-3’
The primers for the detection of P.ovale:
rOVA 1: 5’-ATC TCT TTT GCT ATT TTT TAG TAT TGG AGA-3’
rOVA 2: 5’-ATC TAA GAA TTT CAC CTC TGA CAT CTG-3’
The primers that were used for P.falciparum detection:
rFAL 1: 5’-TTA AAC TGG TTT GGG AAA ACC AAA TAT ATT-3’
rFAL 2: 5’-ACA CAA TGA ACT CAA TCA TGA CTA CCC GTC-3’ and for P.vivax detection:
rVIV 1: 5-CGC TTC TAG CTT AAT CCA CAT AAC TGA TAC-3’ and
rVIV 2: 5’ ACT TCC AAG CCG AAG CAA AGA AAG TCC TTA-3’
The resistance primers are represented in Table 1.

Preparation of agarose gel
One point zero percent (1.0%) Agarose gel was prepared by dissolving 1.0 g in 100 ml Tris EDTA Buffer. The mixture was then heated in a microwave for 5 min to dissolve completely. It was then allowed to cool at 56°C and 6 µl of Ethidium bromide was added to it. The Agarose gel was poured into the electrophoresis chambers with a gel comb, and allowed to solidify.
Electrophoresis
Five microliters of the amplified PCR products were analyzed on 1.0 Agarose gel containing ethidium bromide in Tris EDTA buffer. Electrophoresis was performed at 90v for 60minutes, after electrophoresis, the PCR products were visualized by Wealth Doc UV transilluminator and photographed. Molecular weights were calculated using the molecular weight standard of the marker.
Polymerase chain reaction product cleaning and purification
The PCR products were cleaned using Exonuclease/Shrimp Alkaline Phosphatase (NEBMO 371) Iµ/µl in a 0.6 ml microcentrifuge tube. Purification was done with ABI V 3.1 Big dye kit according to the manufacturer’s instructions.
Sequencing and phylogenetic analysis
The Ultra-pure DNA was sequenced with an AB13500XL analyzer with a 50 cm array, using POP7 at Inqaba Biotechnical Industries Ltd (Hatfield, South Africa). The manufacturer’s protocols were strictly followed. Sequences data generated were analyzed with Geneious version 9.0.5 and phylogenetic trees were constructed using neighbor-joining.
Statistical analysis
Data were analyzed using SPSS version 25 (Stanford, United States of America). Frequencies of Pfdhps and Pfdhfr were placed in percentages. Pearson’s Chi-Square test and Fisher’s exact test were employed in the analysis of data. Analysis of variance (ANOVA) was used to determine the mean parasite density and doses of SP intake. A p-value < 0.05 was considered significant.
RESULTS
A total of 390 participants were enrolled in the study. Three hundred and thirty-six women were IPTp-SP users while 54 women were non-users of SP. This study recorded a compliance gap of 13.8%. The pregnant women were enrolled in the study during their antenatal care visits to health facilities. Background characteristics/ basic socio-demographic information of the participants were as follows: The participants aged between 18 and 45 years. In consideration of their parity, they were composed of primigravidae 73 (18.7%), secondigravidae 104 (26.7%), and multigravidae 213 (54.6%). Their educational levels: none 3 (0.8%), primary level 140 (35.9%), secondary 165 (42.3) and tertiary 82 (21.0%). Only 117 (30.0%) out of three hundred and ninety pregnant women made their first antenatal care visit during their first trimester, with 234 (60.0%) making their first visit during their second trimester. Thirty-nine 39 (10.0%) made their first antenatal care visit during their third trimester. Most of the participants 387 (99.2%) were married. A total number of 342 (87.7%) of the participants used insecticidal nets. This is shown in Table 2.

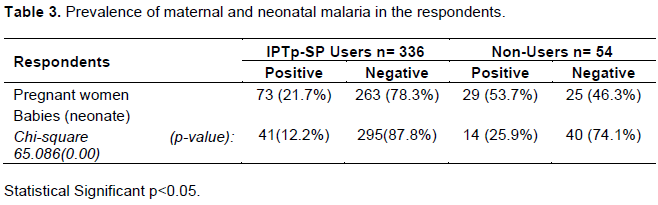
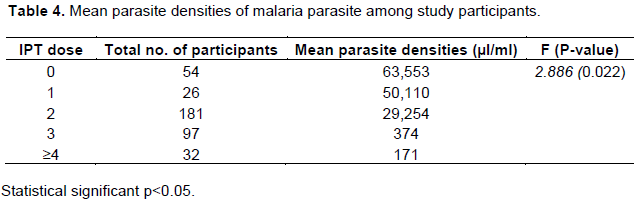
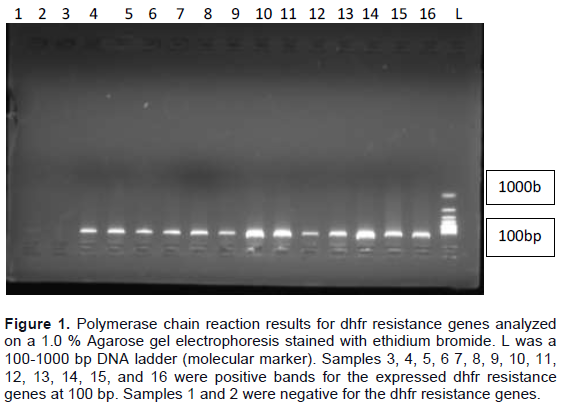
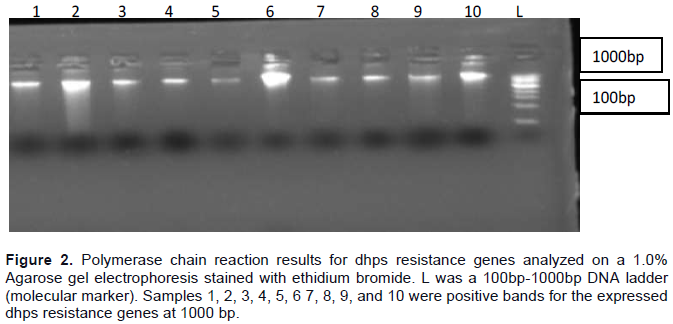
Table 3 shows the prevalence and neonatal malaria among participants. Table 3 also shows the analysis of malaria prevalence in pregnant women and babies of SP users and non-SP users. Mean parasite densities of malaria parasites among study participants are shown in Table 3. Also, Table 4 shows the comparative analysis of parasite density and IPT dose. The PCR results of Pfdhfr resistance genes are shown in Figure 1 while Figure 2 shows PCR results of Phdhps resistance genes. Figure 3 shows two sequence data of P. vivax-4 and P. vivax-5. The phylogenetic tree of P. vivax-4 is shown in Figure 4 while the phylogenetic tree of P. vivax-5 is shown in Figure 5.


Resistance genes of P. falciparum to Sulphadoxine- pyrimethamine
Sequencing assay
Sequence data generated were analyzed with Geneious version 9.0.5 and phylogenetic trees constructed using neighbor-joining. The sequences were subsequently deposited in the National Center for Biotechnology Information (NCBI) data base with their corresponding accession identities (Figure 3).
Phylogenetic analysis
Figures 4 and 5 shows Phylogenetic tree of P. Vivax.
DISCUSSION
The prevalence of maternal malaria among SP- users was 73(21.7%), while 41 (12.9%) of neonates among SP users were infected with the malaria parasite. In non- users of SP, 29(53.7%) were infected with the malaria parasite. The number of neonates among non-users of SP infected with malaria was 14(25.9%). In IPTp-SP users, 263(78.3%) were not infected with malaria while in non-SP users, 25(46.3%) were not infected with malaria. Overall maternal malaria prevalence in SP-users and non-SP users was 102(26.2%) while overall neonatal malaria prevalence in SP-users and non-users of SP was 55(14.1%). The result of the present study is in agreement with a study at Rivers State, Nigeria by Onoja et al. (2019) in which 66(25.3%) of SP users had maternal malaria infection while 17(43.6%) of non-users of SP had maternal malaria infection. Also, in that study; overall maternal malaria prevalence was 83(27.7%). Neonatal malaria infection was 40(13.3%) and placental infection 66(22.0%). In that study also, overall placental and cord blood malaria infection was 106(35.3%). The present study recorded a low prevalence of malaria among IPTp-SP users; this may be as a result of the majority of the participants adhering to the drug policy guiding the use of SP for malaria treatment in pregnancy. In 2013, malaria prevalence in pregnant women attending antenatal clinics in hospitals in Anambra State, Nigeria was 73.1% (Ukibe et al., 2013). The present study recorded a lower prevalence of malaria when compared with the study by Ukibe et al. (2013) on malaria prevalence in women attending antenatal clinics in Anambra State. The result of this study showed that the majority of malaria-infected mothers that took SP admitted having taken the dosage once, twice, thrice while others four times and above. The mean parasite densities of non-users of SP range between 73,000 to 82,400 µl/ml. Pregnant women who used SP for malaria treatment for once, twice, thrice and four times and above had mean malaria parasite densities in ranges of 2,800 to 56,700 µl/ml, 1,230 to 6,344 µl/ml, 137 to 618 µl/ml, and 137 to 200 µl/ml respectively. Non-users of SP had the highest mean malaria parasite density 63,553 µl/ml, followed by those who took SP once, twice, thrice, and four times and above respectively. Mean malaria parasite densities of participants who took SP for malaria treatment for once, twice, thrice, and four times and above were 50110, 29,254, 374 and 171 µl/ml respectively. There was a significant difference in parasite densities of SP users and non-SP users (p=0.022). Therefore mean parasite density was reduced in SP users than in non-users of SP (p<0.001). Pregnant women who took SP had reduced malaria parasitemia than those who did not take SP (p<0.001). Babies of SP users had reduced malaria parasitemia when compared with babies of non-SP users (p=0.002). This finding also agrees with the result of a study carried out by Chukwurah et al. (2016) which showed that pregnant women that took SP once had higher malaria parasitemia than those that took SP twice and thrice respectively. However, low compliance to SP directives increases the risk of maternal, placental, and neonatal malaria in endemic regions (Mdetele and Kidima, 2017).
Molecular genotyping of Plasmodium revealed two species: P. falciparum and P. vivax were prevalent in the study population. P. ovale and P. malariae were not seen among the study participants. The number of pregnant women who were positive for molecular genotyping in IPTp-SP users was 68(20.2%). P. vivax infection which was discovered in this study should be a matter of public health concern because P. vivax infection is not common malaria parasite species seen in the study area. This may be probably a result of misdiagnosis which is common in most laboratories in sub-Saharan Africa. Misdiagnosis of P. vivax is common especially in African countries (Ghai et al., 2016; Yegorov et al., 2016). However, the result of this study is in agreement with the result of a study carried out by Howes et al. (2013) in which they reported that there has been an incidence of P. vivax infection among the Duffy negative population in sub- Saharan Africa. There has been also evidence of mortality associated with acute P. vivax malaria (Baird, 2013). The number of pregnant women that had P. falciparum parasitemia was 38(11.3%) of pregnant women on IPTp-SP while 30(8.9%) of pregnant women on IPTp-SP had P. vivax parasitemia. The number of pregnant women on IPTp-SP that had co-infection of P. falciparum and P. vivax was 27(8.0%). P. vivax infection is not absent in sub-Saharan Africa. In this study, two resistance genes were assessed in the malaria parasite genes. The two resistance genes were dihydrofolate reductase (dhfr) and dihydropteroate synthetase (dhps). The result revealed that 13(3.9%) of the participants expressed the genes for dhfr while for dhps resistance genes, 10(2.9%) of the participants had expression for them. The number of participants that had expression for both dhfr and dhps resistance genes was 8(2.3%) among the study participants. The result of the present study when compared with the results of other researchers showed lower frequencies of these resistance genes (Agomo et al., 2016; Akanbi et al., 2009). These researchers observed higher frequencies of these resistance genes and they also studied mutations in these genes. In the present study mutations of these resistance genes were also studied. In the present study, the frequencies for dhfr and dhps resistance gene mutations were 64.86 and 91.9% respectively. Agomo et al 2016 observed mutated resistance genes up to 75.9% while another researcher Akanbi et al 2009 observed mutated resistance genes of up 71- 92% frequency for dhfr and 39 -71% frequency for double mutant dhps respectively among the participants.
CONCLUSION AND RECOMMENDATIONS
In conclusion, the molecular analysis indicated the presence of P. falciparum dhfr and dhps resistance genes in the study area which are associated with SP treatment failure, although, the SP drug has been recommended by the World Health Organization (WHO, 2001) as a first line antimalarial medicine and adopted in Nigeria for IPTp in 2005 (Federal Ministry of Health, 2005). Similarly, the present study, which indicated the presence of P. falciparum dhfr and dhps resistance genes of which mutations of these resistance genes are associated with SP resistance should be of public health concern. Our results suggest that the presence of these resistance genes can lead to treatment failures among IPTp-SP users. Therefore, novel drugs should be sought to replace SP in near future. The result of the present study might be used as a basis for surveillance as molecular markers for anti-malarial resistance in Nigeria and continuous surveillance using these molecular markers can provide a valuable aid to developing and updating national anti-malarial policy guidelines.
LIMITATIONS OF THE STUDY
Distant primary healthcare centers, poor road network especially in rural places. The financial burden particularly in molecular studies imposed great constraints. Collection of cord blood samples during deliveries and clotted blood samples. These limitations did not in any way, however, bias the results of the present study.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGEMENTS
The authors are grateful to all the study participants who willingly volunteered to participate in the study and sincerely provided their valuable data. Special thanks go to the Chief Medical Directors of Chidera Maternity and Hospital, Nnewi and Trinity Maternity and Hospital, Nnewi together with their staff for their support in diverse ways. Special thanks also go to Doctors and Nurses in the Gynaecology department, Nnamdi Azikiwe University Teaching Hospital, Nnewi for their valuable contributions in sample collection. The authors express their gratitude to all the research assistants for their help in data collection.
REFERENCES
|
Agomo CO, Oyibo WA, Sutherland C, Hallet R, Oguike M (2016). Assessment of markers of Antimalarial Drug Resistance in Plasmodium falciparum isolates in Lagos, Nigeria. PLoS One 11(1):eo146908, 10.1371/journal.pone |
|
|
Akanbi OM, Odaibo AB, Ademowo AG (2009).The burden of malaria infection on pregnant women and birth weight of infants in Southern Western Nigeria. East African Journal of Public Health 6:63-68. |
|
|
Baird JK (2013). Evidence and implications of mortality associated with Plasmodium vivax malaria. Clinical Microbiology Reviews 26:36 -57. |
|
|
Briand V, Bottero J, Noel H, Masse V, Cordel H, Guerra J, Kassou H, Fayomi B, Ayemonnan P, Fievet N, Massougbodji A, Cot M (2009). Intermittent treatment for the prevention of malaria during pregnancy in Benin. A randomized, open-label equivalence trial comparing sulfadoxine-pyrimethamine with Mefloquine. Journal of Infectious Diseases 200:991-1001. |
|
|
Brooks DR, Wang P, Read M, Watkins WM, Sims PF, Hyde JE (1994). Sequence variation of the hydroxymethyl-dihydro pterin in pyrophosphokinase: dihydropteroate synthetase genes in lines of the human malaria parasite, Plasmodium falciparum with differing resistance to sulfadoxine. European Journal of Biochemistry 224(2):397-405. |
|
|
Chandrasekhar BN, Jagannath M, Mulakkapurath NM, Sukriti M, Phani KP, Pillarisetti VS (2016). Protocol for DNA Purification from Dried Blood Spots. Quality Improvement Agency amplification DNA mini and Blood mini Handbook, fifth edition, Public Library of Science San Francisco California, United States of America pp. 42-43. |
|
|
Cheesbrough M (2006).Examination of blood for malaria parasites. District Laboratory Practice in Tropical Countries part 2, 2nd edition, Cambridge University Press, United Kingdom P 605. |
|
|
Chukwurah JN, Emmanuel TI Adeniyi KA, Oluwagbemiga OA, Philip UA, Adetoro OO (2016). Knowledge, attitude, and practice on malaria prevention and sulphadoxine-pyrimethamine utilization among pregnant women in Badagry, Lagos State, Nigeria. Malaria World Journal 7(3):1-6. |
|
|
Cowman AF, Mony MJ, Biggs BS, Cross GA, Foote SJ (1988). Amino acid changes linked to pyrimethamine resistance in the dihydrofolate reductase-thymidylate synthase gene of Plasmodium falciparum. Proceedings of the National Academy of Sciences 85(23):9109-9113. |
|
|
Duraisingh MJ, Curtis J, Warhurst DS (1998). Plasmodium falciparum detection of polymorphism in the dihydrofolate reductase and dihydropteroate synthetase genes by a polymerase chain reaction and restriction digestion. Experimental Parasitology 89(1):1-8. |
|
|
Fagbemi KA, Adebusuyi SA, Nderu D, Adedokun SA, Pallerla SR, Amoo AOJ, Thomas BN, Velavan TP Ojurongbe O (2020). Analysis of sulphadoxine-pyrimethamine resistance-associated mutations in Plasmodium falciparum isolates obtained from asymptomatic pregnant women in Ogun State, Southwest Nigeria. Infection and Genetic Evolution 85:104503. |
|
|
Federal Ministry of Health (2005). National guidelines and strategies for malaria prevention and control during pregnancy. Federal Ministry of Health, Abuja, Nigeria P 50. |
|
|
Ghai RR, Thurber MI, Ei-Bakry A, Chapman CA, Goldberg TL (2016). Multi-method assessment of patients with febrile illness reveals the over-diagnosis of malaria in rural Uganda. Malaria Journal 15(1):1475 -2875. |
|
|
Gontie GB, Wolde HF, Baraki AG (2020). Prevalence and associated factors of Malaria among pregnant women in Sherkole district, Benishanjul Gumuz regional State, West Ethiopia. BMC Infectious Diseases 20:573. |
|
|
Howes RE, Patil AP, Piel BF, Nyangiri AO, Kabaria WC, Gething WP, Zimmerman AP, Barnadas C, Beall MC, Gebremedhin A, Menard D, Williams NT, Weatherall JD, Hay IS (2013). The global distribution of the Duffy blood group. Nature Communications 2:266. |
|
|
Kwala KH, Asika AI, Adiel T (2021). Prevalence of Malaria Infection among Pregnant Women attending Specialist Hospital Yola, Adamawa State, Nigeria. South Asian Journal of Parasitology 5(2):24-31. |
|
|
Mdetele BA, Kidima WB (2017).Monitoring compliance and acceptability of intermittent preventive treatment of malaria using sulphadoxine-pyrimethamine after ten years of intervention in Tanzania. Journal of Malaria Research and Treatment 2017:1-5. |
|
|
Naing NN (2003). Determination of sample size.Malaysian Journal of Medical Sciences 10(2):84-86. |
|
|
National Malaria Elimination Programme (NMEP) (2017). Malaria Report. Federal Ministry of Health, Abuja, Nigeria. |
|
|
Nigeria Malaria Indicator Survey (NMIS) (2015). Malaria transmission. Federal Ministry of Health, Federal Republic of Nigeria, Abuja, Nigeria pp. 3-10. |
|
|
Onoja H, Nduka FO, Abah AE (2019). Intermittent preventive treatment and its effect on maternal and neonatal malaria in two health facilities, Rivers State, South-South, Nigeria. Nigerian Journal of Parasitology 40(2):145-151. |
|
|
Tangpukdee N, Duangdee C, Wilairatana P, Krudsood S (2009). Malaria Diagnosis: A Brief Review. Korean Journal of Parasitology 47(2):93-102. |
|
|
Triglia T, Menting JG, Wilson C, Cowman F (1997). Mutations in dihydropteroate synthetase are responsible for sulphadoxine resistance in Plasmodium falciparum. National Academy of Science 94:13944-13949. |
|
|
Ukibe SN, Ukibe NR, Mbanugo JI Ikeakor LC (2013). Prevalence of malaria among pregnant women attending antenatal clinics in Anambra State South-east Nigeria. International Nigerian Journal of Parasitology 37(2):240-244. |
|
|
Umeh SI, Enwuru CP, Egbuobi RC (2013). Diagnosis of malaria in pregnancy: A comparison of microscopy with rapid diagnostic tests. Microbiology Research International 1(3):35-39. |
|
|
Warrell DA, Gilles HM (2002). Essential Malariology. 4th Ed. Published by Book Power formerly ELST with Arnold in cooperation with the British Council pp. 8-58. |
|
|
World Health Organization (WHO) (2001). World Malaria Report. Geneva, Switzerland. |
|
|
World Health Organization (WHO) (2015). World malaria report. Geneva, Switzerland. |
|
|
World Health Organization (WHO) (2017). World malaria report. Geneva, Switzerland. |
|
|
Yegorov S, Galiwango R.M, Semaganda A, Muwanga M, Wesonga I, Miro G, Drajole DA, Kain KC, Kiwanuka N (2016). Low prevalence of laboratory-confirmed malaria in clinically diagnosed adult women from the Wakiso district of Uganda. Malaria Journal 15(1):555. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


