Full Length Research Paper

ABSTRACT
Most of the sexual initiation and sexual practice of the youth begins at secondary school level. At this stage student assumed to be exposed to many risky sexual behaviors. However, little research had been explored in the Oromia region particularly in East Wollega zone on this area. A cross-sectional study design was used to assess risky sexual behavior and associated factors among high school and preparatory school students from 1st October 2016 till October 30, 2016. Data was collected using self-administered questionnaire. Focus group discussion was conducted to support the quantitative data. Probability proportionate to sample size (PPS) was used to determine the sample size for each grade 9-12. The data was coded and entered into a computer using SPSS version 16.0. Final model was fitted and P value less than 0.05 considered as statistical significance and independent predictor of risky sexual behavior. The results revealed that three hundred and twenty-four students participated in the study (response rate of 97.7%). In the past 12 months, 25.3% of students had sexual intercourse, 17.07% of them had more than one sexual partners and 11.9% of male students visited commercial sex workers. Family connectedness [AOR, 95%CI 0.73(0.67-0.89)], attitudes toward sex [AOR, 95%CI 1.22(1.04-1.43)], khat chewing [AOR, 95%CI 9.25(2.51-34.07)] and those that had been forced by classmates for sex [AOR, 95%CI 7.63(2.36-24.66)] were independent predictors of risky sexual behaviors. The study thus revealed that risky sexual behavior of school youth was increased by khat chewing, sexual coerciveness from classmates or teacher, positive attitudes toward sexual intercourse and reduced by high family connectedness alongside attending religious services regularly. In addition to parental connectedness and parental supervision intervention targeted on school youth like positive peer influence to encourage safer sexual behaviors among school youth is very important in reduction of risky sexual behaviors.
Key words: Associated factors, risky, school adolescent, sexual behaviors.
INTRODUCTION
Youth is the transition from childhood to adulthood. According to the United Nation/World Health Organization (UN/WHO), “Adolescents” include the age group between 10 and 19 years, “youth” includes the age group between 15 and 24 years and “young people” encompass both adolescents and youth which is the age group between 10 and 24 years (Deane and Reindeer, 2005). Risky sexual behavior is any behavior that increases the probability of negative consequences associated with sexual contact, sexually transmitted diseases (STD) including human immune virus/acquired immune deficiency syndrome (HIV/AIDS), abortion and unplanned pregnancy. Risk factors defined as any characteristics of individual, school, family and peers that make people exposed to negative consequences (WHO, 2001).
Worldwide, about six thousand people aged between 15 and 24 contract HIV per day and over the quarter of all the individual living with HIV were aged between 15 and 24 years with most of this age group enrolled in schools (UNAIDS, 2009). In Africa, reproductive health problems are associated with risky sexual behavior among youth and they are highly affected by sexually transmitted diseases like HIV/AIDS, gonorrhea, syphilis and vaginal discharge. Lack of knowledge about family planning, sexual and reproductive health problems and transmission and prevention of these problems were other issues that predispose youths to these problems (Fatch et al., 2013). The sexual activities among male youth have significantly occurred in those living in low-cost housing, having divorced parents, substance (tobacco, alcohol, or drug) use, involvement in gang activities, permissive attitudes, lack of confidence in resisting peer pressure to engage in sex and lack of knowledge and attitudes regarding sexuality and sexual practices especially those at secondary schools (Mee-Lian et al., 2009; Victor et al., 2000).
In Ethiopia, people aged between 10 and 24 years represented one of the country’s largest groups that is 35% of the total population (Mitike et al., 2002). Ethiopian demographic health survey (EDHS) of 2011 indicated HIV and sexually transmitted diseases (STDS) prevalence among the age group 15 to 24 was associated with risky sexual behaviors: having multiple sexual partners, early initiation of sexual intercourse and low condom use (Central Statistical Agency [Ethiopia] and ICF International, 2012). The study on risky sexual behaviors and predisposing factors among Ethiopian university students aged 15 to 24 years showed that out of 529 (40.2%) of the students who ever had sex, those that have experienced having at least one of the sign and symptoms of genitourinary tract infections such as whitish discharge from the penis or vagina were 184 (13.5%), burning sensation during urination were 128 (9.2%), foul smelling and yellowish vaginal discharge were 60 (5.1%), genital ulcers/sores by 46 (3.3%), swellings in groin area 44 (3.2%) and itching in the genital area by 67 (4.9%). The trend was somehow similar across the universities. In most of the students, the symptoms and signs were experienced after starting sex (Lemessa, 2012). Even though different works have been carried out so far to combat the effect of risky sexual practice on the youths which mainly targeted on curative based intervention, the problem still remains a great challenge for developing countries including Ethiopia. Therefore, this study tried to give the present prevalence of risky sexual behavior and further investigate contributing factors that influence youth sexual behaviors among high school and preparatory students in East Wollega zone.
METHODS
Study design and sample collection
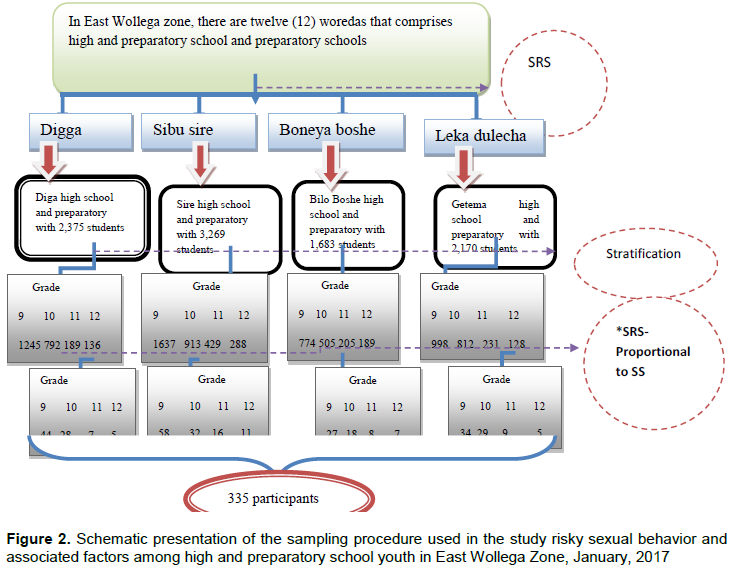
The study was conducted in Oromia Regional State, East Wollega Zone, Western Ethiopia from October 1 to 30, 2016. There are 12 preparatory and 30 high schools in the zone and are providing education services for 38,754 students of which 20,276 were males and 18,478 were females [East Wollega Zone, Education Office Report, 2013]. A cross-sectional study design was used. All high school and preparatory school students aged between15-24 years attending their education daytime during study period and sampled students from specified grades were taken as source and study population, respectively. Regular daytime students aged between 15 and 24 years who were attending high and preparatory school during time of data collection and who volunteered to participate were included in the study and students who refused to fill the questionnaire and those absent during the data collection were excluded.
Sample size and sampling techniques
Sample size determination
Single population proportion formula was employed with the assumptions: the proportion of risky sexual behavior among school students of Addis Ababa was 10.6% (Amsale and Yemane, 2012); desired precision of 5%, 95% confidence level, 2 design effect, and 15% non-response rate were considered.
where z = the confidence limits of the survey result, P = the proportion of study population practicing risky sex, d = the desired precision of the estimate, n = the total sample size. With the aforemention assumptions, the total sample size calculated was 335 students.
Sampling techniques
Quantitative: Multi-stage sampling technique was employed. Twelve high schools and preparatory schools in East Wollega zone were identified and listed. Four woreda were selected randomly and according to the WHO recommendation of facilities based sampling selection (30 - 40%) and four high and preparatory schools were selected using simple random sampling. Initially, students were stratified by grade and then lottery method technique was also employed to select section from each grade and computer generated random number was used to select study units from the sections by using student’s registration as sampling frame. The number of students included in the study from each selected schools were proportional to the total number of students in each selected schools.
Qualitative (FGD): Purposive sampling technique was used to select anti-HIV/AIDS and Women’s clubs because those students who were member of these clubs would expect to have good information on the subject matter than others.
Study variables
Dependent variable
Risky sexual behaviors [having more one sexual partner, inconsistent condom use/not using condom during sex, sex with commercial sex worker and sex with causal partner].
Independent variables
i) Socio-demographic characteristics [religion, age, sex, family educational, residence, ethnicity, parent occupation, grade level].
ii) Family factors [family connectedness, parental monitoring, and parent adolescent communication].
iii) School environment factors [teacher-student’s relationship, classmate’s relations].
iv) Peer factors [partner influence for sexual intercourse, partner influence for substance use (alcohol, chat, and cigarette)].
v) Individual factors [substance use (alcohol, chat, and cigarette), exposure to sexual film, attitudes toward sexual contact, having sexual partner, knowledge about risky sexual behavior].
Operational definitions
Consistent condom use: Using condom during each and every sexual intercourse. Respondents were asked about how they often use condom during sex [always, most of the time, some time, rarely and don’t use]. Those students who used condom always during sex with non-regular partner were taken as consistent condom user.
Non-regular partner: Sexual partner out of marital union.
Risky sexual behavior: At least practices one of the following [having more than one sexual partner, inconsistent condom use while sex, sex with commercial sex workers, have sex with risky causal /unknown sexual partner].
Substance use: Those who use at least any one of the following substances: alcohol, khat, and cigarette.
Parental monitoring: When parents supervise their children, advice their children so as to prevent them from bad behaviors including risky sexual behaviors. There were 5 items yes/no and multiple choices to assess student’s perception about their parent monitoring [high parental monitoring means those students perceived their parents know about them in detail including their sexual activities, low parental monitoring means those students perceived their parents did not know them in detail].
Parental communication: Communication between youth and parent about the sexual issues of the adolescents before the youth initiated for sexual activities [5 items, yes/no and multiple answer questions].
Family connectedness: Parent’s attachment to their children [high total score indicated high family connectedness, low total score indicated low family connectedness].
Peer influence: Pressure from peers to practice sexual intercourse or use substance (khat, alcohol, or cigarette) which intensify risky sexual practices [No pressure, some pressure, a lot of pressure]. Those who had some and a lot of pressure from peers are categorized as those who had peer influence.
School environment: The environment in which there is relationship between student-teachers and among students/ classmates that promotes risky sexual behaviors.
Enforced sex/coercive sex/non-consensual sex: Sexual intercourse which was not depending on the agreement of the two partners or one partner enforces the other.
Attitudes toward sexual contact: The readiness of the students for sexual initiations. There were three 5-point Likert type questions treated as continuous and score runs from 3 to 15 [as score approaches to 15, it indicated favorable attitude and as the score approaches to 3, it indicated unfavorable attitudes].
Verbal harassment: She/He threaten verbally because of refusing sexual activities (insulting or offensive words)
Instrument and measurement
Tools were adapted from previously done similar risky sexual behavior studies and data collection instrument contains five dimensions.
Individual factors: [Substance use (3 items yes/no and 6 items multiple choice questions), knowledge (4 items multiple choice answers questions), attitude toward sex (3 items with 5 point Likert scale question)]. Attitude Likert type questions were treated as continuous variable after summed total score.
Peer influence factors: [Peer influence (4 items yes/no question) and perceived peer involvement on substance use and sexual behavior (5 items multiple choice question)].
School environment: Relationship between male teachers and female students, between classmates (9 items multiple choice questions and 2 items yes/no questions) to assess sexual coercive especially on female students in the school compound.
Family Environment factors: [Family connectedness (6 items with 5 point Likert scale), family monitoring (2 items yes/no and 2 items multiples answer question) and adolescent parent communication on sexual issues (1 item yes/no and 4 items multiple answer question)]. The Likert scale data summed and the total score treated as continuous variable for further analysis.
Risky sexual practice: 19 items were used in general to assess sexual experience and risky sexual behavior is composite variable which was created from at least one of inconsistent condom use and having more than sexual partners. The content validity of the questionnaire was assured by the experts (advisors) and the internal reliability of Likert scale items were checked through Cronbach’s alpha which was greater than 0.70.
Data collection procedures
Quantitative
A pretested, structured and translated questioners adapted from various sexual risky behavior studies (Lemessa, 2012; Kanako et al., 2008, 2009; Gurmesa et al., 2012; Lemessa et al., 2012) was used to collect the data. The questionnaire was originally developed in English and then translated into Afaan Oromo. Four diploma holder data collectors and one-degree holder health professional’s supervisor were recruited to facilitate data collections.
Qualitative
Four focus group discussions (FGDs) disaggregated by sex was conducted using discussion guide in order to provide more insight into complex pattern of sexual behavior among school youths. Furthermore, two male’s groups, first group consisting of 10 males and the second male group was consisting of 8 members; and the first female group consists of 7 members and the second female groups consists of 9 members were organized for FGDs. Male data collectors were moderate in the discussion for the male groups; while the female facilitators ‘was moderate for the female FGD groups.
Data processing and analysis
Quantitative
Data was checked for completeness, consistency, entered into computer and then analyzed using SPSS program version 16.0. Summary result was presented using frequency table, graphs, and cross tabulation. Binary logistic regression analysis was carried out to identify variables with p-value less than 0.25 for multiple logistic regressions. P-value less than 0.05 was considered as statistical significance and independent predictor of risky sexual behavior.
Qualitative
The qualitative data was analyzed into thematic areas and then it was triangulated with quantitative findings.
Data quality assurance
Quantitative
Intensive two-day training was given for both data collectors and supervisors by the principal investigator before data collections. The prepared questionnaire was pre-tested on 5% of sample size in Gute High School which was not included in the study to see the language clarity and sequence of question. During data collection, data was checked for completeness, accuracy, and consistency by supervisors and principal investigator after the data collection on daily base. Descriptive analysis carried out to see outliers, missing values and inconsistency.
Qualitative
Qualitative focus group discussion was conducted by trained professionals. Guideline was prepared and numbers of note taker were two per group because the FGD discussants were not volunteered for audio taped.
Ethical considerations
The study protocol was approved by Ethical Clearance Committee of Jimma University College of Public Health and Medical Sciences. Permission letter was obtained from East Wollega Zone Education Office. An official letter of cooperation was written to Woreda Education Office and then cooperation letter was written to respective schools. The purpose and procedure of the study were communicated to the participants, and informed consent was obtained from the school and from each participant. In order to protect confidentiality, names or school IDs were not included on the written self-administered questionnaires. Identification of an informant was only possible through numerical codes.
RESULTS
From the total of 335 students who were identified for the study from four high and preparatory schools of East Wollega zone, 324 participated in the study yielding the response rate of 97.7%. The widely held of the respondents were from grade nine 142 (43.8%) followed by grade ten 116 (35.8%). One hundred and seventy-eights (54.9%) of study subjects were males and all of the students were single in marital status. About half of the respondents 156 (48.1%) were followers of protestant followed by orthodox 132 (40.7%). Majority 299 (92.3%) of the respondents were Oromo by the ethnic group followed by the Amhara 24 (7.4%). More than half (57.4%) of the respondents were from rural residential. As the descriptive study indicates, respondent mother’s educational were illiterate (52.8%) and 33.3% respondents fathers educational status were only read and write.
About one-third 32.4% of the students reported as they communicated with their family about reproductive health and sexual issues of which the majority 49 (46.7%) of the students prefer mother to discuss on the sexual issues. The major reasons for not discussing sexual issues with family were culturally not acceptable and shame as reported by 55 (25%) and 77 (35%) of the students, respectively.
The majority of the respondents 228 (70.4%) reported that as their parents knew their close friends, of which 106 (46.5%) of the participants perceived that all of their parents knew their close friends, 90 (39.5%) of the participants reported that some of their parents knew their close friends and only 32 (14%) respondents reported that few of their parents knew their close friends. Of the total respondents, more than half 189 (58.3%) respondents perceived that their parent did not know their activities in detail including their sexual experience when they were not at home.
Half 165 (50.9%) of students of which 84 (51%) are males and 81 (49%) are females reported that they had pressure from their peer group to involve in the sexual activities prior to the research and it was supported by focused group discussion, with discussants explaining that peer can influence each other on the sexual behavior, especially peers of similar age group could influence each other towards their own behavior. A 23 years old student described that:
“If I tell you with a simple example, she/he may have a friend who has sexual experience, then her/his friend most of the time talk to her/him about his/her sexual behavior. As the time goes, she/he has a high probability to share the behavior of her/his friend” Male participant.
Descriptive analysis result 49.3, 32.7 and 18.9% of the respondents reported that their peer group drinks alcohol, chewing khat and smoking cigarette, respectively. Of this, 33.3, 18.2 and 8.6% of the students reported that they had pressure from their peer group to drink alcohol, chewing khat and smoking cigarette, respectively. This finding was triangulated with focused group discussion, as participants across the groups described having friends smoking cigarette, drinking alcohol and chewing khat; thus, they have a chance to involve in such activities because of peer influence to have their own behaviors.
Among all female respondents, 32 (9.9%) reported that they had high pressure for sexual intercourse from their male teachers of which 5 (15.6%), 10 (31.3%) and 16 (53.1%) female respondents were raped, practiced voluntary sex and experienced verbal harassment, respectively. To pass the exam because of low academic performance, gift or money and false promising for marriage were the main reasons for this sexual act. From those who had sexual intercourse, the most of them (86.6%), female respondents reported that they kept practicing unprotected sexual intercourse with their male teachers. From the total 324 respondents, 67 (20.7%) students reported that they were enforced for sex by classmates of which 32 (47.8%), 14 (20.8%) and 21 (31.3%) of respondents reported that they were at risk of verbal harassment, raped and had voluntary sexual practice with their classmates, respectively.
Descriptive analysis indicated that 64 (19.8%), 41 (12.7%) and 20 (6.2%) of students reported that they drink alcohol, chewing khat and smoking cigarette, correspondingly. Of which 42, 48.8 and 35%, respectively were those who use alcohol, khat and cigarette in the last two months and 12 months for those who participated in risky sexual practices.
Of total, 275 (84.9%) of the participants heard about the sexual health problem from which 60 (21.8%) of study subjects classified it as: sexually transmitted diseases, unwanted pregnancy, abortion and fistula. Regarding ways of preventing these problems, 151 (46.6%), 58 (17.9%) and 55 (17%) of study subjects reported that abstinence, use of condoms and being faithful are ways to reduce the risky sexual behaviors, respectively. Of the total respondents, 139 (42.9%) students watched or read films or magazines that mainly focus on sex and 61 (18.8%) of the respondents had a sexual partner.
Almost all (99.4%) of the respondents responded to the attitudes related to risky sexual behavior questions. The mean score of attitudes related to risky sexual behavior of respondents was 8.69 ± 3.558 standard deviation (SD) with a median score of 9.00. The t-test indicated that, there was a mean difference between students who were monitored by parents and those free from parental monitoring have positive attitudes toward sex and statistically significant (t=-2.539, (DF)=320, p=0.012).
About quarter 82 (25.3%) of students reported that they ever had sexual intercourse of which 42 (12.96%) and 40 (12.04%) were males and females, respectively prior to the study. This finding was supported by the qualitative study which discussants from all groups stated that even though premarital sex has negative consequences, many high school adolescents had premarital sex and one participant from the group stated that:
“… today having a boy/girl friend at this age looks as a fashion/seen as a sigh of modernizing among school adolescents. But I think this prevents us from achieving our plan because as dating becomes normal premarital sex comes through the process.” Male age 16
The minimum and maximum age of sexual debut for males was 14 and 20 years and that of females was 12 and 20 years. The mean age at first sexual intercourse was 16.1±1.51 years (16.31±1.585 for males and 15.9±1.429 for females). There was no statistical mean difference between male and female respondents that ever started sexual intercourse (t=1.230, DF=79.766, p=0.222). Among those adolescents who had sexual intercourse, the majority (85.4%) of the students had their first sexual intercourse in at age between 16 to 19 years.
Of respondents who had sexual intercourse, more than half (59.75%) of the students reported that they had sex with their friends. Personal desire and peer pressure were the most common reasons to start the first sexual intercourse reported by 31 (37.80%) and 25 (30.48%) of sexually active students respectively.
Promising for marriage, money or gift from a partner and for passing exam were the other reasons to start first sexual intercourse reported by 12 (14.63%), 6 (7.31%) and 7 (8.54%) of students, respectively. This finding is complemented by FGD, participants stated that risky sexual behavior of some female high school adolescents were related to finance. Some students were financially insecure and they need money/other gifts from their sexual partner. As a result, during sexual intercourse they fail to negotiate their partner to use condom, thus they practiced unsafe sex.
Twenty-four (29.26%) of the students reported that they had experienced forced sexual intercourse or enforced someone to be involved in the sexual activities. This finding was similar to result from the focused group discussion in which some participants described that sexual activities among school adolescent mainly focus on getting pleasure form sex or to satisfy their body needs and one female participant from the group said that:
“… I think, most of the time, they are males that enforce girls to have sexual intercourse to satisfy only their body needs without understanding the consequences that comes behind” Female age 17.
The study subjects (5.6%) complained of signs and symptoms of STDs like ulceration or discharges from their genital organ after starting sexual intercourse. Of those female respondents who had sexual intercourse in the past, 15 (37.5%) and 3 (7.5%) reported that they were pregnant one time and more than one times, respectively. This was also supported by the qualitative finding that the majority of the discussants of FGD groups expressed that the major reproductive health problem of school adolescents was unwanted pregnancy with subsequent consequences; as a result many student default from the school and migrate to town to be commercial sex workers and search for other activities.
From those who had sex in the past 12 months, the majority 53 (79.10%) of them reported that they had one sexual partner of which 28 (52.8%) and 25 (47.2%) of the students were male and female respectively. Of those who had sex in the previous 12 months, 14 (17.07%) of the students reported that they had more than one sexual partner. The minimum and maximum numbers of sexual partners of both sexes were 1 and 4, respectively. The average numbers of partners for sexes (per respondent) in the past 12 months was 1.25 ± 0.531 (median=1). The mean numbers of partners 1.23±0.490 (median=1) and 1.28±0.581 (median=1) for males and females respectively. From these, we can observe that female respondents had a high number of sexual partners more likely than their male counterparts but there was no statistically significant difference between the male and female respondents (t=-0.402, (DF)=65, p=0.689).
Commercial sex partners were assessed by asking the male respondents whether or not they had sexual intercourse with a commercial sex worker. Of those male respondents who had sexual intercourse in the past 12 months, 5 (11.9%) male respondents reported that they had sexual intercourse with commercial sex workers of which no male respondents used condom all these period. From these we can observe that male students who had sex with commercial sex partners were at risk of contracting sexually transmitted diseases and are exposed to different social and psychological problems.
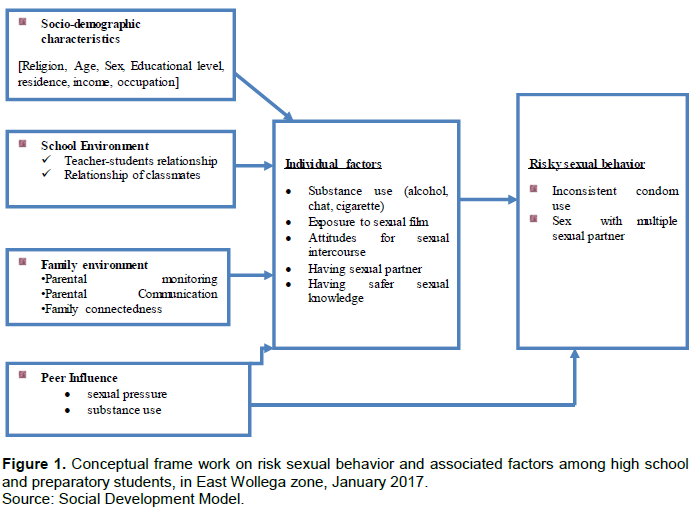
Condom use was assessed and recorded in a way that a respondent or their partners use condoms always with all except marital partner. From those who had sexual intercourse, only 12 (14.6%) used condom consistently in the past 12 months. But only 25 (30.5%) had used condoms in the first time they had sexual intercourse of which 18 (72%) and 7 (28%) were respondent’s male and female, respectively. Figure 1 was also supported by qualitative study that most of FGD discussants across the group however agreed to use of condom during sexual intercourse; most of sexual intercourse practiced among the school adolescents were unprotected and some participants described that most adolescents think that condom prevent satisfaction during sex and according to their ideas, school adolescents choose sex without a condom than use it.
Of those who ever had sexual intercourse, 12 (24%) of students of which 8 (66.7%) males and 4 (33.3%) females reported that they used condom all the time during sexual intercourse in past and 63.6% of male and 36.4% of females reported that they used condom most of the time; 16 (32%) of students of which (37.5% of males and 62.5% of females) used condom sometimes during sexual contact in the past 12 months and 42 (62.68%) of students reported that they did not use condom in their most recent sexual encounters. Twenty-one (30%), 14 (20%) and 13 (18.57%) of students reported their main reason for non-use of condom were being in love with a partner, could not find condom and trusted partner, respectively. This finding was supported by the focus group discussion which some discussants of the group described that school environment was not conducive to reduce risky sexual behaviors. Even if the person assigned in the school compound for counseling those adolescents at risk of these problems, the confidentiality of the issue was not guaranteed:
“I think unavailability of condom is another issue that aggravates risky sexual intercourse. There is no safe place for condom distribution. Even if some students have interest to use condom, they were afraid go to private clinics/pharmacy, health center or other places to buy or ask condom. This is another challenge for condom utilization. So for this issue, I recommend that it is better if a condom is placed in a safe place that keeps privacy of adolescents” Male age 20.
Overall, 76 (23.5%) of the study participants were involved in the risky sexual behaviors in the previous 12 months prior to the study.
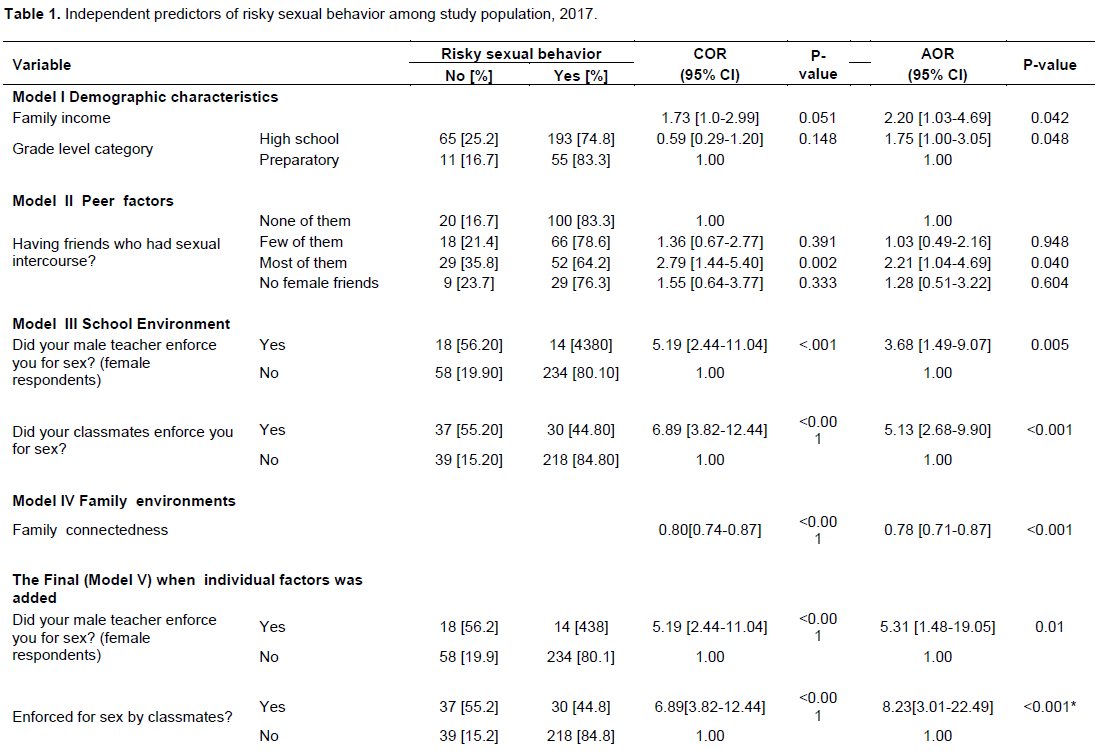
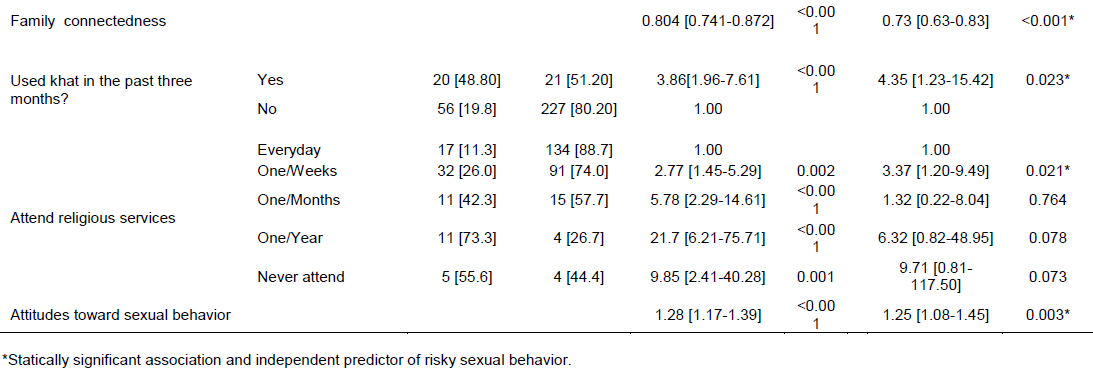
Family connectedness was a protective factor and per unit increases in the total score of family connectedness, the odds of becoming involved in risky sexual behavior reduced by 0.73 and the observed difference was statistically significant [AOR, 95%CI 0.73(0.63-0.83)]. This finding is supported by focus group discussion as most participants agreed to the importance of family monitoring and connectedness on reduction of risky sexual behavior of adolescents. Participants in the group described that family who strictly monitor/follow their children, openly and freely communicate with their children on how to resist peer influence on bad behaviors, and families who show signs of love to their children helped to protect their child from negative peer influences.
Students who had been forced for sex with their classmates were 7.57 times more likely involved in risky sexual behavior than their counterparts [AOR, 95%CI: 7.57 (2.69-21.28)] and students who used khat in the previous three months were 4.35 times more likely to have experienced risky sexual behavior as compared to non-users in the past three months [AOR, 95%CI: 4.35 (1.23-15.42)]. This finding agrees with the qualitative result which some discussants described that when someone use substances like alcohol, khat, and cigarette, the chemical of these substances disturb the mental thinking process of human being. At that time, she/he may out of control and involved in the risky sexual behavior including sex without condom.
Attitudes toward sexual intercourse were positively associated with risky sexual behaviors and per unit increases in the total scores of attitudes toward sexual contact, the odds of becoming at risk of sexual behavior increased by 1.22 and it was statistically significant [AOR, 95%CI: 1.22 (1.04-1.43)]. Students who attended religious services per week were 3.37 times more likely participating in risky sexual behavior than those who attended religious services regularly [AOR, 95%CI: 3.4 (1.20-9.49)] (Table 1).
DISCUSSION
This study tried to see the association of risky sexual behavior with demographic factors, family environment factors, school environment factors, peer factors and individual factors. The finding of this study revealed that about one in four high school and preparatory school youths had sexual intercourse. This implies that many students were sexually active prior to the study. However, finding of this study is consistent with similar studies conducted among high school students in Nekemte town, Ethiopia (Tesfaye and Abulie, 2013) and slightly lower than study in Nairobi, Kenya and much lower than the study conducted in Hosanna, Southern Ethiopia and the Lema, Peru (Fatch et al., 2013; Caroline and Pamela, 2008; Likawunt and Mulugeta, 2012). This discrepancy of finding might be attributed due to different sample size of study subjects, geographical difference, time variation and there might be underreporting and over reporting of responses, that is, there might be respondents that conceal the fact that they are shy and unable to disclose their sexual contact to interviewers.
In Ethiopia, many literatures showed that school youths engaged in the sexual activities of which the majority was unsafe sexual intercourse (Adeoye et al., 2012; Gurmesa et al., 2012). This study also found that 23.5% of the students were involved in risky sexual behaviors prior to the survey. This study finding is higher than the previous study done in Addis Ababa among school youths and much higher than the study done among in-school adolescents at national level of Ethiopia (Amsale and Yemane, 2012; Derege et al., 2005). The higher result might be due to knowledge gap related to sexual issues including condom use and reproductive health problems between the subject of the study area and previous studies. The other reason might be widespread notion that having a sexual partner seen is a sign of modernizing. Furthermore, this study also revealed that 17% of students had more than one sexual partner. This finding is almost comparable with previous studies (Melisew, 2008; Bereket et al., 2013); however, these findings were lower than the previous studies (Bo et al., 2007; Adeoye et al., 2012; Amsale and Yemane, 2012; Amon et al., 2011). In general, those who had more than one sexual partner were at risk of contracting disease like sexually transmitted diseases, HIV/AIDS and these groups are the main focus area of the research and needs immediate attention from a responsible body. The possible explanation of the difference might be the study area being more rural than the previous studies.
In Ethiopia, condom is one of the strategies for preventing sexually transmitted diseases including HIV prevention program. However, prevalence of condom uses especially among youths is still very low despite the efforts made so far to improve the utilization (UNAIDS, 2008, 2009; Nyovani et al., 2002; Tariku et al., 2012; Lemessa et al., 2012). This study showed that only 14% of sexually active students used condom consistently with non-regular partner prior to the study. From these figure 2 we concluded that majority of sexually active students practicing unprotected sex is much lower than the previous studies conducted in Jimma University (69.1%), in Addis Ababa city (43.4%) and in four districts in Tanzania (Bo et al., 2007; Amsale and Yemane, 2012; Amon et al., 2011) and it is also a little lower than the study conducted in Hosanna, Southern Ethiopia (80%) (Likawunt and Mulugeta, 2012).This lower finding might be the knowledge gaps to utilize condom among the youths in this study area and the other reason might be misunderstanding of condom among school youths, that is, condom itself transmit diseases and it prevents satisfaction during sex. From this we could observe that most sexual active school youths experience unsafe sexual activities which expose them to risks. The reasons that prevent them from using condoms were not persuasive enough and it is important to prevent themselves from the negative impact of risky sexual activities and consequent reproductive health problems.In this study, 11.9% of male students had sex with commercial sex workers in the 12 past months. This finding is comparable with the previous study done among students of the Wolaita Sodo University (13.9%) and study in North West Ethiopia (7.8%) but a little lower than the previous studies conducted among secondary schools in Ethiopia (25.3%) (Bereket et al., 2013; Adamu et al., 2003; Yohannis and Alemayehu, 2002) and this study also shows that none of the students who had sex with commercial sex workers use condom consistently which expose them to sexually transmitted problems.Since students are the generation who take responsibility and will have a great role in the growth and development of the country,the responsible body will need to alleviate this problem as soon as possible.
Among the 324 subjects, alcohol and khat were the most used substances among the students. Even though alcohol was the more frequently reported substance, it was not associated with risky sexual behavior but khat chewing was significantly associated, and those who chew khat were 4.35 times more likely to practice risky sexual behavior than those non users. This finding is consistent with previous studies in Ethiopia which revealed that school youths who used khat daily were 2.26 times more likely practicing unprotected sex than non-users. This finding is also supported by Expectancy theory which mainly focuses on the importance of internalized cultural and social expectation about the effect of substances on the sexual behavior. In this theory, the individuals’ expectation that substance use lowers sexual inhibitions and/or enhances sexual pleasure moderates its relationships to sexual behavior, making sexual behavior under the influence more likely and more risky as such expectation increases. However, in contrast with study done in Hosanna, Southern Ethiopia, among health college students, khat was not significantly associated with risky sexual behavior (Likawunt and Mulugeta, 2012; Derege et al., 2005; Brooke et al., 2011). The possible explanations for this discrepancy might be confounding factors controlled or might be sample size of study subjects.
In this study, having positive attitude toward sex increased the odds of risky sexual behavior and one-unit increase in the total score of attitude toward sex increased the odds of risky sexual behavior by 1.22. This finding is comparable with the previous studies. Among Kenyan school youths, those who had a positive attitude toward sex were less conservative to use condom and in China among school youths, those who had positive attitudes toward premarital sex, had sex more likely than those who had an unfavorable attitude toward premarital sex (Joy et al., 2009; Sunday et al., 2010).
In this study, family connection was a protective factor from risky sexual behavior. As one unit increased, the total score of family connection decreased the odds of risky sexual behavior by 0.77 and this finding is consistent with the study done in Jimma Zone; family connection was protective factors and one unit increase of family connection decreased the odds of risky sexual behavior by 0.94. As reported by WHO report, family connection or love is one of the important bearing dimensions of youth health; also, another study in Houston, Texas indicated students higher score on a scale of perceived family connectedness, decreased the odds of having had unprotected sex by 0.97 (Abebe et al., 2013; World Health Organization, 2007; Christine et al., 2003).
Attending religious services were a protective factor from youth risky sexual behavior. This study is consistent with the study done in Jamaica among school youths which indicated that attendance of religious services was the most protective factor of risky sexual behavior (Lemessa et al., 2012).
Programs that targeted behavior change of school youth towards healthy sexual behavior were incorporated in the school curriculum to promote safer sexual behavior of school youths. So, establishing and promoting peer education program in school to make positive influence of peers around the school compound is crucial and very important in changing the risky sexual behavior of school youths to sustain the life of future generation. Generally, encouraging safe sexual behavior was one of the strategies to prevent sexually related problems like HIV/AIDS and ensuring good relation among students and student-teacher can encourage sexual risky behavior reduction.
CONCLUSION
This study identified substance use [chewing khat], attitudes toward sexual contact and influences for sexual activities from classmates as risky factors for risky sexual behavior whereas family connectedness and attending of religious services were protective factors and independent predictors for risky sexual behavior of school adolescents.
Sexuality was a sensitive issue and the respondents may over report or underreport their experience. As a result, tendency to give false information may be a limitation to this study. Recall bias may be introduced because the study asked for the past experience of the respondents and social desirability was a limitation of this study.
RECOMMENDATION
Family should be showing signs of love to their children and family connectedness to their children should be strengthened and well promoted. Youth organization should lead out in reducing risky sexual behavior, promoting sports and recreational activities, discouraging substance use like alcohol consumption and smoking cigarette.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGEMENTS
The authors would like to express their sincere gratitude to Jimma University Department of Health Education and Behavioral Science for their support in the accomplishment of this study. The authors are thankful to East Wollega Zonal Education Office, Bilo High Schools and Preparatory administration, Sibu Sire High Schools and Preparatory School administration, Gatema High School and Preparatory administration and Ifa High School and Diga Preparatory School administration for their support and cooperation during data collection. They are glad to thank the East Wollega High School and Preparatory students who participated in the study and provide information with their full cooperation. Finally, they would like to thank Bilo Health Center, Boneya Boshe Health Office and Bilo High School administration for their financial and stationery including duplicating questionnaire support.
REFERENCES
|
Abebe M, Tsion A, Netsanet F (2013). Living with parents and risky sexual behavior among Jimma town preparatory students. African Health Science Journal 13(2):498–506. |
|
|
Adamu R, Mulatu MS, Haile SI (2003). Patterns and correlates of sexual initiation, sexual risk behaviors, and condom use among secondary school students in Ethiopia. Ethiopian Medical Journal 41(2):163-77. |
|
|
Adeoye AO, Ola O, Aliu B (2012). Prevalence of premarital sex and factors influencing it among students in a private tertiary institution in Nigeria. International Journal of Psychology and Counseling 4(1):6-9. |
|
|
Amon E, Angelina LM, Godfrey MM, Khadija K, Godfrey MU, Honorati M (2011). Multiple sexual partners and condom use among 10 - 19 year-olds in four districts in Tanzania; BioMed Central Public Health 11:490. |
|
|
Amsale Ch, Yemane B (2012). Peer Pressure Is the Prime Driver of Risky Sexual Behaviors among School Adolescents in Addis Ababa, Ethiopia. World Journal of AIDS 2:159-164. |
|
|
Bereket Y, Terefe G, Mulat T (2013). Prevalence and Associated Factors of Sexually Transmitted Infections among Students of Wolaita Sodo University, Southern Ethiopia. International journal of scientific and technology research 2(2). |
|
|
Bo W, Xiaoming L, Bonita S, Vafa K, Sylvie NK, Iqbal SH (2007). Sexual attitudes, pattern of communication, and sexual behavior among unmarried in-school youth in china. BioMed Central Public Health 7:189. |
|
|
Brooke WE, Sarit GA, Jeffrey PT (2011). An Integrated Theoretical Approach to Substance Use and Risky Sexual Behavior among Men Who Have Sex with Men. AIDS and Behavior 15(3):509-520. |
|
|
Caroline KW, Pamela O (2008). Factors associated with sexual activities among high school students in Nairobi, Kenya. Journal of adolescence 32(4):1023-1039 |
|
|
Central Statistical Agency [Ethiopia] and ICF International (2012). Ethiopia Demographic and Health Survey. Addis Ababa, Ethiopia and Calverton, Maryland, USA: Central Statistical Agency and ICF International. |
|
|
Christine M, Markham, Susan R, Tortolero, Liliana EC, Guy PS, Ronald H, Robert AC (2003). Family connectedness and sexual risk-taking among urban youth attending alternative high schools. Perspectives on Sexual and Reproductive Health 35(4):174–179. |
|
|
Deane KL, Reindeer G (2005). Sexually transmitted infections among adolescents: the need for adequate health services, World Health Organization,Geneva. |
|
|
Derege K, Atalay A, Getnet M, Fikre E, Frehiwot B, Yigeremu A, (2005). Khat and alcohol use and risky sex behavior among in-school and out-of-school youth in Ethiopia. BioMed Central Public Health 5(1):109 |
|
|
Fatch KW, Maggie Z, Du Y (2013). Effective Adolescent Sexual and Reproductive Health Education Programs in Sub-Saharan Africa. Californian Journal of Health Promotion 11(2):32-42. |
|
|
Gurmesa T, Fessahaye A, Sisay D (2012). Risky Sexual Behavior and Predisposing Factors among Students of Jimma University, Ethiopia. Ethiopian Journal of Health Science 22(3). |
|
|
Joy NB, Cynthia WE, Eidi TH and Maxine W (2009). The Influence of Early Sexual Debut and Sexual Violence on Adolescent Pregnancy: Matched Case-Control Study in Jamaica.International Perspectives on Sexual and Reproductive Health 35(1):21-28. |
|
|
Kanako I, Paul S, Olivia McD (2008-2009). Prevalence and Correlates of Sexual Risk Behaviors among Jamaican Adolescents. International Perspectives on Sexual and Reproductive Health 37(1):6-15. |
|
|
Lemessa O (2012). Risky Sexual Behaviors and Predisposing Factors among Ethiopian University Students. Pan African Medical Journal 12:33 |
|
|
Lemessa O, Yemane B, Alemayehu W (2012). Pre-marital sexual debut and its associated factors among in-school adolescents in eastern Ethiopia. BioMed Central Public Health 12(1):375. |
|
|
Likawunt S, Mulugeta TA (2012). Substance use and sexual risk behavior and factors associated with HIV transmission in Hosanna Health Science College, Southern Ethiopia.International Journal of Pharmaceutical Sciences and Research 3(4):1080-1086. |
|
|
Mee-Lian W, Roy Kum-Wah Ch, David K, Hiok-Hee T, Fong-Seng L, Shanta E, George B (2009). Premarital Sexual Intercourse among Adolescents in an Asian Country: Multilevel Ecological Factors. Pediatric 124:44-52. |
|
|
Melisew M (July 2008). Premarital Sexual Practice and Perception of High Risk of HIV/AIDS among school adolescents in Injibara town, Awi Zone, Addis Ababa University (unpublished). |
|
|
Mitike G, Lemma W, Berhane F (2002). HIV/AIDS Behavioral Surveillance Survey, round one, Ethiopia 2001-2002.Addis Ababa, Ethiopia. |
|
|
Nyovani M, Eliya Z, James C (2007). Is Poverty a Driver for Risky Sexual Behaviors? Evidence from National Surveys of Adolescents in four African Countries. African journal of reproductive health 11(3):83-98. |
|
|
Sunday AE, Linnea WU, Antony OA, Elisabeth FA (2010). The attitudes of Kenyan in-School adolescents toward Sexual Autonomy. African Journal of Reproductive Health 14(1):33-41. |
|
|
Tariku D, Lemessa O, Nega A (2012). Patterns of sexual risk behavior among undergraduate university students in Ethiopia: a cross-sectional study. Pan African Medical Journal 12:33. |
|
|
Tesfaye SM, Abulie TM (2013). Sexual and reproductive health problems and service needs of university students in south east Ethiopia: Exploratory qualitative study. Science Journal of Public Health 1(4):184-188. |
|
|
UNAIDS (2008). Report on the global HIV/AIDS epidemic,UNAIDS report, Geneva. |
|
|
UNAIDS (2009). Swaziland country report on monitoring the political declaration on HIV and AIDS, Swaziland, Ministry of Health |
|
|
Victor C, Jesús L, Claire D (2000). A profile of sexually active male adolescent high school students in Lima, Peru. Saúde Pública, Rio de Janeiro 16(3):733-746. |
|
|
World Health Organization (WHO) (2001). The second decade: improving adolescent health and development, Geneva, World Health Organization report: 1-20. |
|
|
World Health Organization (WHO) (2007). Helping parents in developing countries improve adolescents' health, Geneva;WHO report. |
|
|
Yohannis F, Alemayehu W (2002). High risk sexual behavior and pattern of condom utilization of Gonder College of medical science students North West Ethiopia. Ethiopian Journal of Health Development 6(3):335-338. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


