Full Length Research Paper

ABSTRACT
Malnutrition being one of the major public health problems in developing countries, it is still unacceptably high and progress to reduce it in most regions of the world is low. In Eastern Africa region, stunting and being underweight is estimated at 48 and 36% and are expected to increase over the next decade. There is limited information available on the prevalence of malnutrition in this area. This study determined nutritional status, and examined correlates of stunting among the children. This was a cross-sectional study undertaken among 125 preschoolers in western province, drawn from 37 clusters. For each cluster a total of 10 households were selected using systematic simple random sampling. Data were collected on nutritional status, socioeconomic status, food consumption and current malaria infection status. The prevalence of stunting (Z-scores for height for age [HAZ] <-2), wasting (Z-scores for weight for height [WHZ] < -2) and being underweight (Z-scores for weight for age [WAZ] < -2) was 28.9, 1.7 and 6.6%, respectively. Stunting was associated with poverty (OR=4.29, 95% CI: 1.06-17.36, p= 0.037) and lack of consumption of solid foods that include ripe mangoes, pawpaw and guavas (OR=3.15, 95% CI: 1.11-8.94, p=0.025), fish (OR=4.1, 95% CI: 1.15-14.61, p=0.021) and eggs (OR=4.42, 95% CI: 0.97-20.08, p=0.039). Child growth is a good indicator of nutritional status of both the individual and the community. The study demonstrates a high prevalence of stunting. Given the acute and long term consequences of malnutrition, interventions aimed at reducing child malnutrition in such a population should focus on all children less than 5 years of age.
Key words: Stunting, underweight, wasting, preschool children.
INTRODUCTION
Malnutrition is a public health problem which is still unacceptably high and progress to reduce it in most regions of the world is slow as shown in the fourth report on global nutrition (Administrative Committee on Coordination/Sub-Committee on Nutrition (ACC/SCN), 2000). In the year 2000, it was estimated that 182 million pre-school children which was one third of children less than five years old in developing countries were stunted and approximately 27% were estimated to be underweight (World health Organization (WHO), 1995).
The overall trend in nutritional status in developing countries over the last 20 years is one of improvement, whereas Eastern Africa region (which includes Kenya) is the only region where the trend has been in the opposite direction. The prevalence of stunting and being underweight among pre-school children in this region are estimated at 48 and 36% and are expected to increase further over the next decade (ACC/SCN, 2000).
In Kenya, malnutrition is still a serious public health problem (United States Agency for International Development (USAID), 2006) and the situation has been worsening despite the numerous acitivities geared toward improving food and nutrition security. The Kenya Demographic Health Survey findings of 2008 showed that 35% of Kenyan children of under-five years of age were stunted which was an increase in the national stunting rates of children from 30% in 2003, with the highest prevalence between the ages of 18 to 35 months. At the sub-national level, western province recorded at 34.2% (Central Bureau of Statistics, 2009).
The main problems contributing to childhood malnutrition include inadequate household food security, inadequate care giving capacity, and an unhealthy environment predisposing young children to infections (MOH-GOK, 2006). Malnutrition has devastating effects on any population as it increases mortality and morbidity rates, diminishes the cognitive abilities of children and lowers their educational attainment, reduces labour productivity and reduces the quality of life of all affected (Wekesa et al., 2006). Children are more vulnerable to infection and their rapid rate of growth is easily affected by poor nutrition, hence their nutritional status measurements are a good indicator of overall community health (Ngugi and Nyariki, 2006).
The most commonly collected indicators of nutritional status are anthropometric measurements of children under five years of age. Children are more vulnerable to infection and their rapid rate of growth is easily affected by poor nutrition, thus measures of children’s nutritional status are a good barometer of overall community health (Ngugi and Nyariki, 2006). The aim of this study was to determine the nutritional status, dietary patterns, socioeconomic and malaria infection of the children.
METHODOLOGY
Study site
This study was carried out in Western Province of Kenya, outside Nairobi, West of the Eastern Rift Valley and is inhabited mainly by the Luhya people. It harbours 3,358,776 inhabitants within an area of 8,361 km². The main economic activity is farming with maize as the staple food and some animal husbandry (a few heads of cattle and goats or chicken). Other activity includes quarrying for construction materials.
Study population
The study population consisted of preschool children aged between 6 and 59 months. The inclusion of the study subjects was based on consenting parents/guardians of children aged 6 to 59 months and without physical disability that would affect height measurement but those who had physical disability were excluded from the study.
Study design and sampling procedure
This study was a cross-sectional study that used a two-stage stratified cluster sample. The households were clustered using National Sample Survey and Evaluation Programme (NASSEP IV). The province was stratified into rural and urban enumeration areas (EAs). The first stage involved selection of primary sampling units (PSUs) which were the EAs using probability proportional to measure of size (PPMOS) method. The second stage involved the selection of households and EAs were selected with a basis of one measure of size (MOS) defined as the ultimate cluster with an average of 100 households and constituted of one (or more) EAs. The household and structure were listed through a quick count, amalgamation/segmentation of EAs to form clusters, physical numbering of the structure of the dwelling unit.
The sample was selected using a stratified two-stage cluster design consisting of 37 clusters, 18 in the urban and 19 in the rural areas. For each cluster a total of 10 households were selected using systematic simple random sampling.
Data collection
A structured and pretested questionnaire was used to record data. It captured demographic, socioeconomic, anthropometric measurements, knowledge and dietary intake on children aged 6 to 59 months.
Anthropometric measurements were recorded: height and weight were measured among children who were in light clothing to determine their nutritional status. The weight measurement was taken using a Seca scale (Hanson mode) to the nearest 0.1 kg and height/length portable wooden constructed scale calibrated for height measurement to the nearest 0.1 cm. Height for age (stunting), weight for age (underweight) and weight for height were calculated using ≤ 2D National Center for Health Statistics (NCHS) reference data. The height for age Z-score (HAZ) of <-2 was classified as stunted and Z-score cut off point of <-2 standard deviations (SD) was used to classify low weight for age, low height for age and low weight for height
Malaria rapid diagnostic kits (RDKs) were used at the household for malaria test using blood collected in EDTA tubes. The RDKs used were Plasmodium falciparum only (HRP2) to capture P. falciparum malaria. Thick blood smears was prepared, stained with Giemsa stain and allowed to dry and observed under a microscope using oil immersion objectives (×100). The presence or absence of malaria was reported as any parasitaemic detected in blood smear.
Dietary intakes of the study participants were assessed by means of food variety scores in the previous 24-h. Parents/Guardians were interviewed by a face-to-face method. They were asked to recall all foods and beverages they consumed by their children during the preceding 24-h. To assist subjects and their parents to recall accurately, household utensils were used.
Statistical analysis
The data was coded and double entered into a computer database using Ms-Access and Ms-Excel and analysis was performed using Statistical Package for Social Sciences (SPSS). In order to maintain the assumption of an equal probability sample, weighting was used to adjust for unequal cluster size due to variation in the number of absentees or refusals between clusters. Chi-square test was used for the relationship between variables. The cut offs used to define stunting, wasting and underweight were those recommended by the World Health Organization, that is, less than two Z-scores were considered to be stunted, wasted and underweight. The relationship of various predictors, with stunting at the individual level was analysed by doing cross tabulations using the Chi-squared test for significance of associations and P-values <0.05 were considered statistically significant.
Ethical clearance
Ethical clearance was sought from scientific steering committee (SSC) and ethical review committee (ERC) of Kenya Medical Research Institute (KEMRI) for approval. Prior consent was sought from parents/guardians of the preschoolers who participated in the study. During the interview privacy and confidentiality was observed.
RESULTS
Characteristics of the study participants
A total of 125 preschoolers aged 6 to 59 months were enrolled in the study and consisted of males 72 (57.6%) and 53 (42.4%) females with a mean age of 35± (10 SD) ranging between 6 and 59 months. A high proportion (29.6%) was aged between 24 and 35 months. The majority (65.6%) of the participants resided in rural areas and a substantive proportion (34.4%) in urban areas. The wealth was defined by the type of house, roofing material and number of sleeping rooms. The study findings indicated that the main material of the (inside) walls of the house was mud (69.6%) and main house roofing materials was corrugated iron (88.8%). The commonly used source of energy for cooking was wood as reported by 72.8% of the participants. The other sources of energy for cooking were liquefied petroleum gas (LPG)/natural gas (4%), charcoal (22.4%) and others (0.8%). The prevalence of malaria among the preschool children was 6.7%. The economic status for each household was determined by means of a wealth index, which was a generic of all the social economic characteristics. Going by the wealth index scale, the bulk of the population (45.6%) were in the second quintile. The minority of the population were in the fifth quintile (4%) as shown in Table 1.


Consumption of solid foods in the previous 24 h by the children
A high proportion (59.2%) of the children consumed bread, rice, noodles or other food made from grains which are carbohydrates rich food sources than vitamin A rich and protein rich foods sources as shown in Table 2.

Nutritional status among children (6-59 months)
The results indicate high prevalence of stunting (height for age ≤ 2D, 28.9%) but wasting was low (weight for height Z-scores ≤ 2 SD, 1.7%) and being underweight (Z-scores for weight for age [WAZ] < -2) was 6.6%.
Bivariate analysis
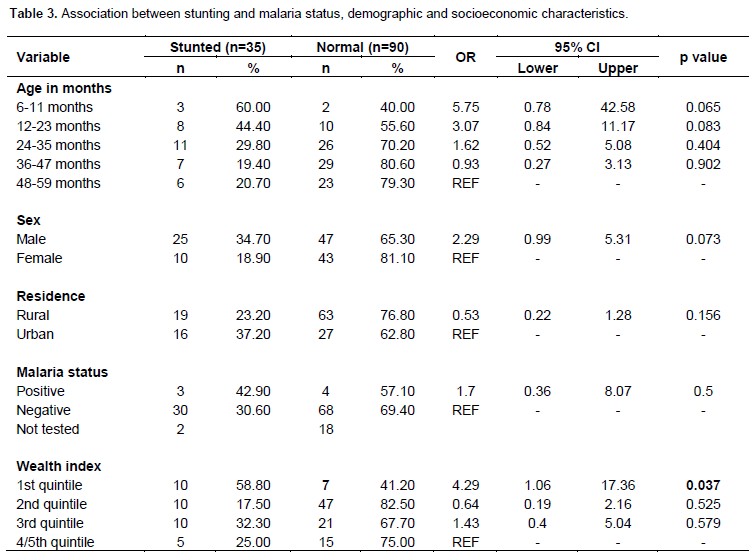
The demographic characteristics were of age in months, sex and residence that were not significantly associated with stunting. Using children of aged 48 to 59 months as the reference, males in all the age groups were at a higher risk of stunting than females (34.7%, OR=2.29, 95% CI: 0.99-5.31, p=0.051). The risk of stunting decreased with age increase among the subjects, progressively lowering with each age group. Living either in a rural or urban set up had no effect with the children being stunted. There was no association between stunting and malaria infection. Using fourth/fifth quintiles as the reference for the relationship between stunting and socioeconomic characteristics, first quintile of the wealth index was significantly associated with stunting (OR=4.29, 95% CI: 1.06-17.36, p=0.037) as shown in Table 3.
The association between stunting and consumption of solid foods in the previous 24 h was analysed as presented in Table 4. Three of the seven foods were identified to be significantly associated with stunting. The foods include ripe mangoes, pawpaw and guavas (OR=3.15, 95% CI: 1.11 to 8.94, p=0.025), fresh/fried fish (OR=4.1, 95% CI: 1.15 to 14.61, p=0.021) and eggs (OR=4.42, 95% CI: 0.97 to 20.08, p=0.039). Children not consuming these three foods are likely to be stunted.


DISCUSSION
Stunting is usually an indication of long term deprivation of nutrients in children and it remains a problem of greater magnitude than underweight or wasting. The Kenyan children aged between 6 and 59 months from both urban and rural areas of intense malaria transmission in western province, 28.9, 6.6 and 1.7% of the children were stunted, underweight and wasted, respectively. The stunting finding concurs with those of the 2008 KDHS with the highest prevalence being between 18 and 35 months. According to the World Health Organization classification of prevalence ranges of stunting, this level is classified as high (WHO, 1995). This is a more accurate reflection of nutritional deficiencies and illness that occur during the critical periods for growth and development in early life (UNICEF, 2009). The study examined the various predictors of stunting among the children of 6 to 59 months.
Poverty is associated with inadequate food and poor sanitation and hygiene that lead to increased infections and stunting in children. There was a significant relationship between household wealth and stunting, with children from poorer households being more likely to suffer from stunting. This finding concurs with previous studies regarding wealth status of child’s household and stunting (Christiaensen and Alderman, 2004; Girma and Genebo, 2002; Glewwe et al., 2002). This relationship could be explained by the fact that rich people are able to afford good living conditions that may improve the child’s health including nutrition (Obeng, 2003). The efforts to reduce stunting depend on reducing poverty and raising peoples’ living standards by improving the quality of homes, hygiene and sanitation. This has prompted UNICEF to come up with a social protection programmes focused on the most disadvantaged children helping them and their families by increasing the quality and quantity of food for children through cash or voucher transfer schemes, price subsidies and improving food storage for lean seasons and periods in crisis.
The increased risk of under-nutrition as children reach their second year in life may be due to interactive effects. During this period children are weaned from the breast and mothers do lose their ability to produce enough milk to meet the nutritional demand of a growing infant (Chavez et al., 2000). The child’s age was found not a significant determinant of stunting. The finding differs with those of Ghana which showed that, stunting was high among children of this age. This situation has been attributed to the fact that these children have already been introduced to complementary feeding (Ghana Statistical Service, 2009).
Micronutrients such as vitamins are obtained from consumption of fruits mostly seasonal. Foods containing vitamins A, C and E have shown to have protective effects on young children. Maize is a staple crop commonly grown and consumed by most children. Unfortunately, they lack important nutrients for child growth. The key risk factors for vitamin A deficiency are a diet low in sources of Vitamin A (that is, dairy products, eggs, fruits and vegetables). Findings from the current study, revealed a significant association between stunting and vitamin A food sources, that is, ripe mangoes, pawpaws, guavas and eggs, by comparing stunted and non-stunted children.
Presence of infection has a negative impact on utilization of nutrients. Certain types of parasities can cause anemia. Malnutrition increases one’s susceptibility to and severity of infections and is thus the most important risk factor for illness and death in developing countries. Malaria has enormous impact on the quality of life and likelihood of survival in this vulnerable age group in malaria endemic areas. There is evidence to support that malaria plays part in decreased nutritional status. In this study, malaria outcome does not relate to low height for age z-scores, an indicator of achieved height and long term nutritional status. These findings concur with longitudinal study findings where it found that stunted children had a lower incidence of clinical malaria episodes than not stunted children (Genton et al., 1999). This findings contradict a longitudinal study in Gambia where stunting at the start of transmission season was associated with increased incidence of malaria (Deen et al., 2002).
Deficiency of proteins in diet is seen in stunted children and this deficiency might have a role in the retardation of growth in height (Ibrahim et al., 2002). This study finding shows an association between stunting and fish. Thus animal sourced foods are good sources of nutrients that are required for growth and also of micronutrients that support the immune system. This concurs with a study that was conducted by Dror and Allen (2011) reported that consuming animal sourced foods not only decreased stunting but also improved other anthropometric indices toward the reduction of morbidity and mortality of undernourished children. Educating parents and care-givers about the importance of improving child feeding practices with diverse diet and animal sourced food is a critical public health intervention.
The nutrition surveys are prone to technical error of anthropometric measurements which could result in misclassification of the children’s nutritional status. However, minimization of biases was addressed through appropriate study procedures, standardization of anthropometric measurements, appropriate training of researchers and close supervision of fields activities.
CONCLUSION AND RECOMMENDATION
The child growth and monitoring is a good indicator of nutritional status of both the individual and the community. The study demonstrated a high prevalence of stunting among the preschool children. Given the acute and long term consequences of malnutrition, interventions aimed at reducing child malnutrition in such a population should focus on all children less than 5 years of age. To improve the nutritional status of the children by improving their intake of vitamin A food sources and putting in place mechanisms to improve cost of living of the people in western province.
ACKNOWLEDGEMENTS
The authors wish to thank the Jomo Kenyatta University of Agriculture and Technology (JKUAT), Kenya Medical Research Institute (KEMRI), and all who participated in the study. My gratitude goes to Dr. Kombe for giving me the chance to undertake this research. The authors also thank Moses Mwangi for statistical advice and assistance.
COMPETING INTERESTS
The authors declare no competing interests.
REFERENCES
| ACC/SCN (2000). Fourth Report on the World Nutrition Situation. Geneva: ACC/SCN in collaboration with IFPRI. | ||||
| Central Bureau of Statistics (Kenya) (2009). Ministry of Health (Kenya), ORC Macro: Kenya Demographic and Health Survey 2008. Calverton, MD: CBS, MOH and ORC Macro. | ||||
| Chavez A, Martinez C, Soberanes B, (2000). The effect of malnutrition on human development: A 24-year study of well-nourished and malnourished children living in a poor Mexican village. In: Goodman A, Dufour D, Pelto G (eds), Nutritional Anthropology: Biocultural Perspectives on Food and Nutrition. Mayfield Publishing, San Francisco pp 234-68. | ||||
|
Christiaensen L, Alderman H (2004). Child malnutrition in Ethiopia: can maternal knowledge augment the role of income? Econ. Dev. Cult. Change 52(2):287-312. Crossref |
||||
|
Deen JL, Walraven GE, von Seidlein L (2002). Increased risk for malaria in chronically malnourished children under 5 years of age in rural Gambia. J. Trop. Pediatr. 48:78-83 Crossref |
||||
| Dror DK, Allen LH (2011). The importance of milk and other animal-source foods for children in low-income countries. Food Nutr. Bull. 6:227-243. | ||||
| Genton B, Al-Yaman F, Ginny M, Taraika J, Alpers MP (1999). Relation of anthropometry to malaria morbidity and immunity in Papua New Guinean children. Am. J. Clin. Nutr. 68:734-741. | ||||
| Ghana Statistical Service (GSS) (2009). Noguchi Memorial Institute for Medical Research (NMIMR), ICF Macro: Ghana Demographic and Health Survey 2008. Calverton, Maryland: GSS, NMIMR, and ORC Macro. | ||||
| Girma W, Genebo T (2002). Determinants of nutritional status of women and children in Ethiopia. ORC Macro: Calverton, Maryland, USA. | ||||
|
Glewwe P, Koch S, Nguyen BL (2002). Child nutrition, economic growth, and the provision of healthcare services in Vietnam in the 1990s. World Bank Working Paper. Available at: http://elibrary.worldbank.org/doi/pdf/10.1596/1813-9450-2776. Crossref |
||||
|
Ibrahim SA, Abd el-Maksoud A, Nassar MF (2002). Nutritional stunting in Egypt: which nutrient is responsible? East Mediterr. Health J. 8:272-80. |
||||
| MOH-GOK (2006). National guidelines for Diagnosis, treatment and prevention of Malaria for health workers in kenya. | ||||
|
Ngugi RK, Nyariki DM (2006). Rural livelihoods in the arid and semi-arid environments of Kenya: Sustainable alternatives and challenges. Agric. Hum. Value.22:65-71. Crossref |
||||
| Obeng C (2003). Impart of childhood poverty on health and development. Healthy Gen. 4(1):1-12. | ||||
| UNICEF (2009). Tracking progress on child and maternal nutrition, UNICEF, New York. | ||||
| USAID (2006). Understanding nutrition data and the causes of malnutrition in Kenya. A special report by the Famine Early Warning Systems Network (FEWS NET). | ||||
| Wekesa M, Karani I, Waruhiu S (2006). Emergency interventions in the arid and semi-aridareas of northern Kenya. Humanitarian Exchange Magazine. 35: November. Available at: http://www.odihpn.org/humanitarian-exchange-magazine/issue-35/emergency-interventions-in-the-arid-and-semi-arid-areas-of-northern-kenya. | ||||
| WHO (1995). Physical Status: The Use of and Interpretation of Anthropometry. Geneva: World Health Organization. | ||||
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


