Full Length Research Paper

ABSTRACT
Cervical cancer screening is not routinely done in Cameroon because of poor knowledge of the disease. This study evaluated the validity of VIA test, assessed women’s knowledge on cervical cancer and assessed the relationship between knowledge score and previous screening participation. Between June and September 2018, this cross-sectional study enrolled 256 women aged between 25 and 65 years at the Douala General Hospital. After filling in a structured questionnaire, consented respondents were screened for cervical cancer using the Visual Inspection with Acetic Acid (VIA) and the Papanicolaou (Pap) smear. Descriptive statistics were carried out using SPSS v 20. Of the 256 respondents, 30 [11.7%, 95% CI: 8.2 - 16.0] and 34 [13.3%, 95% CI: 9.3 - 17.5] were positive for Pap smear and VIA test, respectively. VIA test had the sensitivity of 80.0% and the specificity of 95.6%. About 251 [98.0%, 95% CI: 96.1 - 99.6] respondents were aware of cervical cancer; 236 [92.2%, 95% CI: 88.7 - 95.3] other had poor knowledge of the disease but 95 [37.1%, 95% CI: 31 - 43] declared previous screening participation. Respondents with satisfactory knowledge score were more likely to have had previous screening participation [OR= 2.89: 95%CI: 1.08-7.70, p= 0.029] than those with poor score. High prevalence of cervical cancer and low previous screening participation were attributed to poor knowledge of the disease, thus necessitating a planned health education.
Key words: Cervical cancer, Pap smear, VIA test, sensitivity, specificity, knowledge.
INTRODUCTION
In Cameroon, cervical cancer is a public health problem in women aged 15 - 44 years. With an annual estimation of 2,356 new cases and 1,546 deaths (Bruni et al., 2019), cervical cancer ranked first representing 52% of all cancer types in the North West Region of Cameroon (Nkfusai et al., 2019). Data on the regional prevalence of cervical cancer in Cameroon vary considerably according to the study population and the technique used. In that respect, the prevalence of 9.0% was documented by DeGregorio et al. (2016) and that of 16.9% was reported by Bekolo et al. (2016) in HIV positive women in Yaoundé.
Persistent Human papillomavirus (HPV) infection, the causative agent of cervical cancer is found in more than 80% of men and women in their lifetime (Gallagher et al., 2016). Infection with the HPV is usually favoured by the number of pregnancies, number of sexual partners, the use of contraceptive methods and the consumption of alcohol and tobacco (Libert et al., 2017).
Awareness about risk factors and symptoms of cervical cancer are limited in most sub-Saharan African countries including Cameroon (Ogembo et al., 2015). Various studies on the level of awareness of cervical cancer have been carried out with different outcome: 91.6% in Gabon (Assoumou et al., 2015) and 86.9% in Ethiopia (Dulla et al., 2017). Cervical cancer is a preventable disease through prophylactic HPV vaccination of girls between 9 and 13 years (Bruni et al., 2019) and screening of women between 25 and 65 years (Donatus et al., 2019); unfortunately, most women in developing countries are not screened for cervical cancer because of the lack of awareness of the disease, limited screening facilities or carelessness (Ubajaka et al., 2015).
HPV testing, cytology and VIA are all recommended screening tests for cervical cancer. The Pap smear described in 1928 had since its introduction, helped to reduce cervical cancer incidence and mortality rates by 75% (Mehta et al., 2009). Though, the Pap smear is widely used as a cancer-screening option, its practice in most African countries remains very limited due to a variety of socioeconomic and logistical barriers (Ogembo et al., 2015). In addition, the Pap smear sensitivity (25 - 50%) is so low that false negative results are common in women who progressed to cervical cancer (Tebeu et al., 2015). Visual screening was later developed based on the principle that a higher concentration of intracellular proteins leads to a dense aceto-whitening effect. The sensitivity of VIA test to detect Cervical Intraepithelial Neoplasia (CIN) 2 and CIN 3 lesions and invasive cervical cancer varies from 49 to 96% and the specificity from 49 to 98% (Sreedevi et al., 2015). Even though VIA test is easy to conduct; its interpretation is challenging (Tebeu et al., 2015).
Considering the fact that lack of public awareness is an important barrier to a successful screening program, the Cameroon Ministry of Health had initiated awareness, educational and free screening campaign supported by the mass media with the objective to inform the population on the disease and the screening tests (McCarey et al., 2011). Despite these opportunistic efforts in some low income countries, lack of awareness, poor knowledge on cervical cancer and the Pap smear persist and constitute the primary barriers for effective cervical cancer prevention (Okunowo et al., 2018). This study evaluated the validity of VIA test, assessed women’s knowledge on cervical cancer and assessed the relationship between knowledge score of respondents and previous screening participation.
MATERIALS AND METHODS
Study area and site
Cameroon, a Central Africa country (GPS coordinates 7°22’10.74 N” and 12°20’40.51 E”) is divided into ten regions. Douala, the economic capital of the Littoral Region (GPS coordinates 4°3’41.5296N and 9°47’9.8592E) has a population of 1,861,463 inhabitants most of whom are involved in business activities. It is a cosmopolitan city with climate being divided into a dry season (November to March) and the wet season (March to November).
The Douala General Hospital (GPS coordinates 4°3’N- 4° 12’N and 9°42’E- 9°51’E) is one of the six reference hospitals in Cameroon. With its capacity of 320 functional beds, it located in the “Cité des Palmiers” Health District. Built in 1992, it is one of the two general hospitals (Douala and Yaoundé) in Cameroon, where cancerous patients receive multidisciplinary management and cancer radiotherapy (Nguefack et al., 2012).
Inclusion criteria
From the period of June to September 2018, this cross-sectional study enrolled 256 women aged between 25 and 65 years who declared being sexually active and visiting the hospital either for minor gynaecological complaints or for other reasons (female relatives of patients). A sensitization campaign was also done to attract non-patient participants using a banner displayed in front of the hospital and media messages (WhatsApp, Facebook).
Non-inclusion criteria
Respondents with the following conditions were not included in the study: (1) cervico-vaginal bleeding; (2) HPV vaccination; (3) pregnancy; (4) radical hysterectomy; (5) virgins; (6) women suffering from cervical cancer or on cancer therapy.
Ethical considerations
Respondents were clearly informed of the objective and the benefits of the study. Verbal and written consents were obtained from each respondent to show compliance with the study. Participation was free of charge. Codes were attributed to respondents for confidentially and anybody was free to withdraw from the study without risk to lose the right to medical care.
Sample size calculation
The sample size (n) was calculated using the Lorentz formula as followed (Charan and Biswas, 2013):
n= Z2P (1-P) ? e2
n= (1.96)2 × 0.169(1-0.169) / (0.05)2
where n= minimum sample size= 232, Z= 1.96 at 95% confidence, e= margin of error 5%, P: expected proportion in population 0.169 (Bekolo et al., 2016). Using the least error of 10%, we actually enrolled 256 respondents.
Data collection
A structured, self-administered questionnaire containing two sections (A and B) with 24 points multiple choice questions (with « yes », « no », « I don’t know» answers ) was designed to capture participant’s personal information and their opinion on frequently asked questions on cervical cancer. The questionnaire, written in simple English, was handed over to consented respondents who after filling without the aid of the neighbour or researcher was retrieved and verified for completeness. In order to minimize bias in data collection, respondents were not allowed to take the questionnaire home neither for themselves nor for their female friends and relatives.
Sample collection for Pap smear
During the gynaecologic examination, a sterile wooden Ayre spatula was placed against the cervix with the sharp end into the endocervix and the blunt end onto the ectocervix, the cervical exfoliated cells were scrapped with the spatula rotated at 360°C using firm pressure to maintain contact with the cervix. The spatula was then gently removed avoiding contamination with the vaginal secretions. This procedure was repeated when enough secretions were not obtained (BCCP, 2015). The exfoliated cells were then evenly spread onto clean dry labelled slide with the endocervical end facing the inside of the slide, immediately fixed with alcohol fixative and stored in plastic slide box in dried environment away from humidity and breakage. The slides were later transported to the cytology laboratory of the “Centre Hospitalier Dominicain Saint Martin de Poores”, stained with the Pap staining method (Solomon et al., 2002). The results of the Pap smear were recorded as normal, atypical squamous cells of undetermined significance (ASCUS), low grade squamous intraepithelial lesions (LSIL), and high grade squamous intraepithelial lesions (HSIL) according to the Bethesda guidelines 2001 (Barut et al., 2015). Positive cases were referred for biopsy.
Visual inspection with acetic acid test
After Pap smear procedure, a 5% acetic acid was applied on the cervix through embedded cotton at the edge of a Cherron forceps. One minute thereafter, the cervix was illuminated with a 100-W bright lamp and examined by naked eyes. Results of VIA were classified as: (1) normal; (2) abnormal; and (3) suggesting cancer. The category of normal includes cases with the presence of cervical mucus, squamous metaplasia, ectopy, cervicitis, ectropion, naboth cysts, and polyps. Lesions suggestive of condyloma, CIN1, CIN2, and CIN3 were included in the abnormal category, and lesions suggesting cancer were recorded separately (Longatto-Filho et al., 2012). Respondents with abnormal Pap and/or VIA results were referred for histological confirmatory test while those with normal results were advised to repeat the test after 1 year according to the Cameroon recommendations.
Data management and analysis
Data collected using questionnaire and those using laboratory forms were key in Microsoft Excel 10 and were later analysed using the Statistical Package for Social Sciences (SPSS) version 20. The mean and standard deviation (SD) for continuous variables, frequencies and percentages for categorical variables were presented on tables. A contingency table was constructed to determine the sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) of VIA test (Miller et al., 2002) in comparison to the Pap test used as gold standard (Kalgong et al., 2017). The specific knowledge questions on risk factors, symptoms and prevention were grouped to determine the overall knowledge score of the respondents. The Modified Bloom’s cut off points was used to categorize the knowledge score as followed: a score of 80 to 100% of correct responses equivalent to a good knowledge, a score of 50 to 79% of correct responses equivalent to a satisfactory knowledge and a score of less than 50% of correct responses equivalent poor knowledge (Abdullahi et al., 2016). Finally, Chi square was carried out to assess the association between knowledge score and previous screening participation. The statistical significance was considered at p < 0.05.
RESULTS
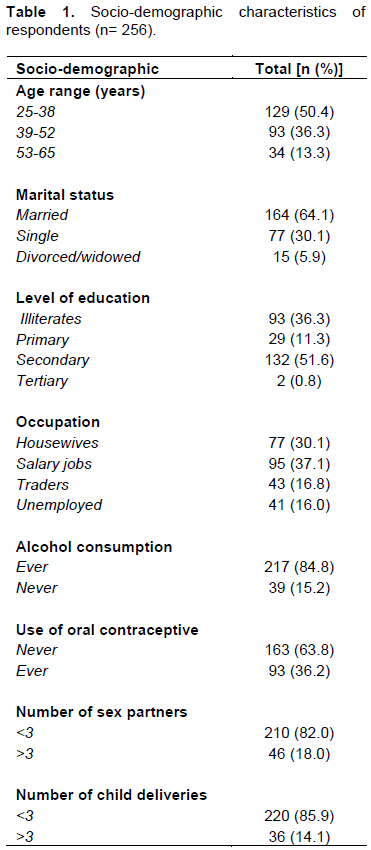
Socio-demographic characteristics of the respondents
Of the 256 respondents [aged 25-65 years; Mean: 40.02+/-9.79 SD], 129 [50.4%, 95% CI: 44.5- 56.6] were aged between 25 and 38 years, 164 [64.1%, 95% CI: 58.2 - 69.9] were married, 95 [37.1%, 95% CI: 31.6-42.6] had salary jobs and 134 [52.3%, 95% CI: 46.5 - 58.6] had secondary/tertiary education level. Also, 217 [84.8%, 95% CI: 80.1 - 89.4] were casual/permanent alcohol consumers and 163 [63.8%, 95% CI: 57.4 - 68.8] ever used oral contraceptive in their life time. Lastly, 210 [82.0%, 95% CI: 77.3 - 86.7] declared less than 3 sexual partners in the past one year and 220 [8.9.5%, 95% CI: 81.3 - 89.8] claimed less than 3 full term child deliveries (Table 1).
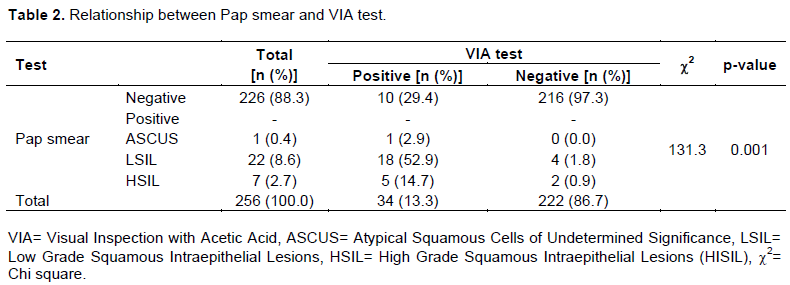
Relationship between Pap smear and VIA test
Of the 256 respondents, 30 [11.7%, 95% CI: 8.2 - 16.0] and 34 [13.3%, 95% CI: 9.3 - 17.5] were positive for the Pap and VIA tests, respectively (Table 2). Of the 34 (13.3%) positive VIA tests, 24 (70.6%) were positive (true positive) and 10 (29.4%) were negative (false positive) for Pap smear, respectively. Likewise, of the 222 (86.7%) negative VIA tests, 6 (2.7%) were positive (false negative) and 216 (97.3%) were negative (true negative) for Pap smear, respectively. The sensitivity (80.0%), specificity (95.6%), PPV (70.6%) and the NPV (97.3%) of VIA test were calculated using the Pap smear as the gold standard (Table 2).
Awareness, source of information and previous screening uptake
Results on Table 3 revealed that 251[98.0%, 95% CI: 96.1 - 99.6] of the 256 respondents were aware of the disease and 103 [40.3%, 95% CI: 34.4- 46.5] were able to identify the causative agent. Information on the cervical cancer was obtained mainly from the media and health practitioners as declared by 170 [66.4%, 95% CI: 60.5 - 72.7] and 95 [37.1%, 95% CI: 31.3 - 43.4] respondents, respectively. According to our results, 95 [37.1%, 95% CI: 31 - 43] had taken a previous cervical cancer test.

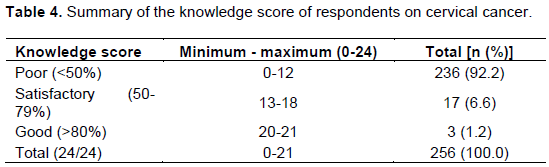
Respondent’s knowledge score of cervical cancer
The knowledge score was obtained by cumulating the 24 questions on cervical cancer risk factors, symptoms and prevention. Of the 256 respondents, 236 [92.2%, 95% CI: 88.7 - 95.3] had low score (< 50%), 17 [6.6%, 95% CI: 3.5 - 9.8] had satisfactory score (50-79%) and 3 [1.2%, 95% CI: 0 - 2.7] had good score (>80%) (Table 4).
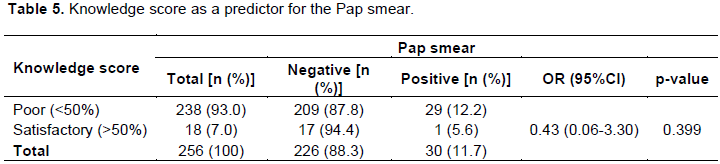
Relationship between knowledge score and Pap smear
Table 5 shows that, of the 238 (93.0%) respondents with poor score, 29 (12.2%) had positive Pap smear. Also, of the 17 (94.4%) respondents with satisfactory score, 1 (5.6%) had positive Pap smear. Respondents with satisfactory score were at reduced risk of positive Pap smear than those with poor score (OR= 0.43; 95%CI: 0.06 - 3.30, p = 0.399).
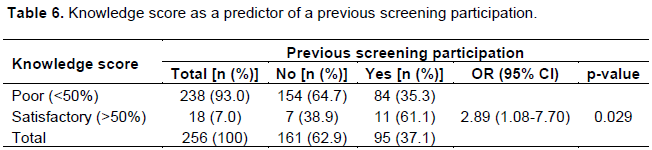
Relationship between knowledge score and a previous screening participation
Of the 238 (39.0%) respondents with poor score, 84 (35.3%) had previously been screened. Also, of the 18 (7.0%) respondents with satisfactory score, 11 (61.1%) had previously been screened. Respondents with satisfactory score were 2.89 times more likely to have had a previous screening participation than those with poor score (Table 6).
DISCUSSION
Cervical cancer, the second cancer type of women in Cameroon can be treated if diagnosed earlier. This study enrolled women aged between 25 and 65 years old which was in accordance with the Cameroon’s recommended age for cervical cancer screening. This age range was different from the United States Preventive Services Task Force recommended age of 21 years (USPSTF, 2018). Their socio-demographic characteristics showed that most of them were between 25 and 38 years and married, had secondary/tertiary school level of education and had salary jobs. These characteristics differed to some extend from those reported in the Democratic Republic of Congo where most women were aged between 16 and 78 years, were single, had a secondary school level of education and were without formal employment (Ali-Risasi et al., 2014). The observed disparities in the characteristics in different studies may not be unconnected to the inclusion criteria of respondents.
The prevalence of cervical cancer varies across population. We recorded the prevalence of 11.7 and 13.3% using the Pap smear and VIA test, respectively. Similar results of 12.7 and 14.65% using the Pap smear and the VIA test, respectively were reported in the Northern Cameroon (Kalgong et al., 2017). But higher prevalence of 29.1% was reported in Yaoundé by Tufon et al. (2013). The observed variations in the prevalence of cervical cancer in most studies might be linked to the choice of the diagnostic tool and to the inter-examiner variations, thus the necessity for the histological conformation of all positive screening tests. Cellular lesions in this study were graded as ASCUS (2.9%), LSIL (52.9%) and HSIL (14.7%). These findings were in discordance with that of Srivastava et al. (2018) in Lucknow West (India) who reported LSIL (17.2%) in high prevalence than HSIL (0.9%). High prevalence of LSIL in most studies may be linked to a number of factors including recurrent sexually transmitted infections and trauma during childbirth/abortion that cause cellular aggressions at the squamo-columnal junction thus, favouring HPV acquisition (Louie et al., 2009). In the other hand, finding a high prevalence of HSIL (14.7%) in this study compared to that reported (7%) by Alakananda et al. (2016) may be related to low screening participation which delay early diagnosis and treatment of prevalent LSIL thus minimizing progression to HSIL.
Histology is the gold standard for VIA and Pap tests. The reason and the benefits of using Pap smear as gold standard in testing the validity of VIA test in this study was explained by Kalgong et al. (2017). From this study, VIA test had the sensitivity of 80.0%, the specificity of 95.6%, the PPV of 70.6% and the NPV of 97.3%. These findings were almost similar to the sensitivity of 94.87%, the specificity of 97.0%, and the PPV of 82.2% and the NPV of 99.2% observed in the Northern Cameroon (Kalgong et al., 2017). There are variations in the validity of VIA test that could be ascribed to its non-standardization resulting in a wider range of sensitivity and the specificity ranging from 49-96% and 49-98%, respectively, to the choice of the gold standard and to the examiner expertise (Sreedevi et al., 2015). VIA test in this study had a high sensitivity comparable to that of previous studies to be used for primary screening of cervical cancer given the few facilities offering standard tests and the limited use of Pap smear and histology in Cameroon (Tebeu et al., 2015; Kalgong et al., 2017).
The majority of respondents were aware of the cervical cancer (98.0%). Comparable high awareness was also reported in Cameroon (86.0%) by McCarey et al. (2011) and in Uganda (88.2%) by Mukama et al. (2017). Variations in the level of awareness according to studies might be related to the efficiency of the existing communication programme developed to raise public awareness on the disease, to the existing cervical cancer prevention programmes (Modibbo et al., 2016). High level of awareness of cervical cancer in this study might be justified by factors including the urban localisation of the study, sporadic free screening/educational programmes organized by the Cameroon Ministry of Health, private health facilities and research on the topic offer by students of higher education. Regarding their knowledge of the causing agent of cervical cancer, 40.2% of our respondents cited HPV infections. This finding was low compared to 58% mentioned by healthcare workers in Cameroon (McCarey et al., 2011) in previous study. The main source of information about cervical cancer was the media (radio, internet, and television) followed by health personnel and friend/family members similar to another study in Nigeria (Modibbo et al., 2016). The existing geographic disparities in the source of information on cervical cancer observed between studies are often linked to the availability of facilities for mass communication on the disease. On that basis, a study reported that most women in the urban areas are knowledgeable enough of the disease than their counterparts in the rural areas (Mwaka et al., 2015). That was not the case in this study where poor knowledge of cervical cancer might not be unconnected to the inefficient communication on the disease.
Sichanh et al. (2014) documented that education level and economic status of a population are other determinants of knowledge on cervical cancer. The socio-demographic characteristics of respondents (52.3%) in this study showed that the majority of them had secondary/tertiary school level of education a factor that could be a predictor of their adequate knowledge of the disease. Unfortunately, the results revealed that most of them (93.0%) had poor knowledge of the risk factors, symptoms and prevention of cervical cancer. This finding contradicted that of Ekane et al. (2015) who reported 55.3% of his respondents with fair knowledge of the disease presumably because the majority of his study population were university students; some of whom being medical students. Increasing women’s knowledge level on cervical cancer could inevitably reduce their exposure to risk factors of the disease, thus justifying the finding of low positive Pap smears among respondents with satisfactory knowledge score in this study.
As documented in this study, more than the half (62.9%) of respondents had never taken a Pap smear compared to 59.0% among female health care workers in Yaoundé (McCarey et al., 2011). The main reason for no participation to a previous screening as declared by respondents was poor knowledge, but other factors not investigated in this study such as limited screening centres, coast, benefits and accessibility to screening centres are other contributing barriers (Der et al., 2018; Abiodun et al., 2014).
Regarding the relationship between knowledge score and previous screening uptake, this study shows that respondents with satisfactory score were 2.89 times more likely to have had a previous screening participation than those with poor score (p = 0.029). This observation could be supported by the report that in Argentina, screened women were 2.6 times more likely to have adequate knowledge about Pap smear than those non-screened (Paolino and Arrossi, 2011). These findings were in agreement with the suggestion by Paolino and Arrossi (2011) that raising women’s knowledge on cervical cancer and screening tests might increase screening participation. Raising women’s knowledge on cervical cancer in Cameroon is challenging. But it could be achieved via a sustainable health education about the disease, regular free screening, counselling, provision of more screening centres and media sensitization (Donatus et al., 2019). Also, self-screening participation and screening recommendation by health care workers should be encouraged with the objective to increase screening participation and to raise women’s knowledge on screening tests (Ashtarian et al., 2017).
CONCLUSION
Despite preventive measures advocated by the WHO, governmental and non-governmental organisations, cervical cancer remains a public health problem in Cameroon with the prevalence of 11.7 and 13.3% using Pap smear and VIA test, respectively was recorded among woman in Douala. LSIL was the most frequent cytological abnormalities. VIA test showed high sensitivity and PPV to be used as the primary screening test in Cameroon. The majority of respondents were aware of the disease mainly through media information. Despite its high awareness, the majority of respondents had poor knowledge of cervical cancer. Finally, respondents with satisfactory score were more likely to have taken a previous screening than those with poor score, thus the necessity to encourage self-screening participation among women at risk of cervical lesions in Cameroon. Therefore, it is recommended that for effective cervical cancer prevention, health education programme using media facilities should be planned by the National Cervical Cancer Prevention Programme with the objective to raise Cameroonian women’s knowledge on the disease and to increase screening participation.
LIMITATIONS OF THE STUDY
The major shortcoming of this study was inability to conduct biopsy on women with cervical lesions because that was not the objective of this pilot study. Even though, women with positive Pap smear were referred for biopsy, almost all of them did not have the test done because of its high cost. Further studies covering the cost for histology/colposcopy testing become necessary for the confirmation of diagnosed cases of cervical cancer in Cameroon. Furthermore, the organized sensitization campaign might have contributed to the over estimation of the level of awareness of cervical cancer among respondents. Despite these limitations, this study revealed that, there is need for more communication about cervical cancer in Cameroon.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGMENTS
The authors thank women who participated in this study. They are grateful to the administration of the Douala General Hospital for granting the authorization for sample collection.
REFERENCES
|
Abdullahi A, Hassan A, Kadarman N, Saleh A, Baraya YS, Lua PL (2016). Food safety knowledge, attitude and practice toward compliance with abattoir laws among the abattoir workers in Malaysia. International Journal of General Medicine 9:79-87. |
|
|
Abiodun OA, Fatungase OK, Olu-Abiodun OO, Idowu-Ajiboye BA, Awosile JO (2013). An assessment of women's awareness and knowledge about cervical cancer and screening and the barriers to cervical screening in Ogun State, Nigeria. IOSR Journal of Dental and Medical Sciences 10(3):52-58. |
|
|
Alakananda, Sarma U, Biswas I (2016). Histopathological Correlation with Cervical Cytology. IOSR Journal of Dental and Medical Sciences 15(11):53-58. |
|
|
Ali-Risasi C, Mulumba P, Verdonck K, Broeck DVand Praet M (2014). Knowledge, attitude and practice about cancer of the uterine cervix among women living in Kinshasa, the Democratic Republic of Congo. BMC Women's Health 14:30. |
|
|
Ashtarian H, Mirzabeigi E, Mahmoodi E, Khezeli M (2017). Knowledge about Cervical Cancer and Pap Smear and the Factors Influencing the Pap test Screening among Women. International Journal of Community Based Nursing and Midwidfery 5(2):188-195. PMC5385241 |
|
|
Assoumou SZ, Mabika MB, Mbiguino AN, Mouallif M, Khattabi A and My Mustapha Ennaji. Awareness and knowledge regarding of cervical cancer, Pap smear screening and human papillomavirus infection in Gabonese women. BMC Women's Health 15:37. |
|
|
Barut MU, Kale A, Kuyumcuo?lu U, Bozkurt M, A?açayak E, Özekinci S, Gul T (2015). Analysis of Sensitivity, Specificity and Positive and Negative Predictive Values of Smear and Colposcopy in Diagnosis of Premalignant and Malignant Cervical Lesions. Medical Science Monitor 21:3860-3867. |
|
|
BCCP (2015). The Georgia Breast and Cervical Cancer Program manual, Georgia Department of Public Health. |
|
|
Bekolo CE, O'Bryan G, Tchago FE, Nangue C, Bekoule PS, Kollo B (2016). Integrating Cervical Cancer Screening with HIV Care in Cameroon: Comparative Risk Analysis of Cervical Disease in HIV-Infected Women Receiving Antiretroviral Therapy to Women in the General Population. PLoS ONE 11(2):e0149152. |
|
|
Bruni L, Albero G, Serrano B, Mena M, Gómez D, Muñoz J, Bosch FX, de Sanjosé S. ICO/IARC Information Centre on HPV and Cancer (HPV Information Centre) (2019). Human Papillomavirus and Related Diseases in Cameroon. Summary Report 17 June 2019. |
|
|
Charan J, Biswas T (2013). How to Calculate Sample Size for Different Study Designs in Medical Research? Indian Journal of Psychological Medicine 35(2):121-126. |
|
|
DeGregorio AG, Bradford LS, Manga S, Tih MP, Wamai R, Ogembo R, Sando Z, Liu Y, Schwaiger C, Rao SR, Kalmakis K, Sheldon KL , Nulah K, Welty E, Welty T, Ogembo JG(2016).Prevalence, predictors and same day treatment of positive VIA renhanced by digital cervicography and histopathology results in a Cervical Cancer Prevention Program in Cameroon. PLoS ONE 11(6):e0157319. |
|
|
Donatus L, Nina FK, Sama DJ, Nkfusai NC, Fala Bede, Shirinde J and Cumber SN (2019). Assessing the uptake of cervical cancer screening among women aged 25-65 years in Kumbo West Health District, Cameroon. Pan African Medical Journal 33:106. |
|
|
Dulla D, Daka D, Wakgari N (2017). Knowledge about cervical cancer screening and its practice among female health care workers in southern Ethiopia: a cross-sectional study. International Journal of Women's Health 9:365-372. |
|
|
Ekane HEG , Obinchemti ET, Nguefack TC, Nkambfu MD, Tchounzou R, Nsagha SD, Nkwele MG, Orock EG (2015). Pap smear screening, the way forward for prevention of cervical Cancer? A community based study in the Buea Health District, Cameroon. Open Journal of Obstetrics and Gynecology 5:226-233. |
|
|
Gallagher KE, Baisley K, Grosskurth H, Vallely A, Kapiga S, Vandepitte J, Kamali A, De Sanjosé S, Changalucha J, Hayes R, and Watson-Jones D (2016). The association between cervical Human Papillomavirus infection and subsequent HIV acquisition in Tanzanian and Ugandan Women: A Nested Case-Control Study. The Journal of Infectious Diseases 214(1):87-95. |
|
|
Kalgong G, Kamdje AN, Tagne RS, Amvene JMBO, Nangue C (2017). Cervical Cancer Screening with Visual Inspection with Acetic Acid and Lugol as Primary Screening Test, a Comparable Result to Conventional PAP Smear in Northern Cameroon. Journal of Cancer Science and Research 2:109. |
|
|
Libert EEE, Koanga MML, Banai T, Doh NG, Tiekwe E, Kojom FLP, Assokom OEV, Eloumou EL, Mouelle SA and Ngono NAR (2017). Dynamics of factors responsible for the resurgence of cervical cancer lesions in women in developing countries. Journal of Applied Life Sciences International 11(2):1-10. |
|
|
Longatto-Filho A, Naud P, Derchain SFM, Roteli-Martins C, Tatti S, Hammes LS, Sarian LO, Eržen M, Branca M, De Matos JC, Gontijo R, Maeda MYS, Lima T, Costa S, Syrjänen S, Syrjänen K (2012). Performance characteristics of Pap test, VIA, VILI, HR-HPV testing, cervicography, and colposcopy in diagnosis of significant cervical pathology. Virchows Archives 460(6):577-85. |
|
|
Louie KS, De Sanjose S, Diaz SM, Castellsagué X, Herrero R, Meijer CJ, Shah K, Franceschi S, Muñoz N, Bosch FX (2009). Early age at first sexual intercourse and early pregnancy are risk factors for cervical cancer in developing countries. British Journal of Cancer. 100:1191-1197. |
|
|
McCarey C, Pirek D, Tebeu PM, Boulvain M, Doh AS and Petignat P (2011). Awareness of HPV and cervical cancer prevention among Cameroonian healthcare workers. BMC Women's Health 11:45. |
|
|
Mehta V, Vasanth V, Balachandran C (2009). Pap smear. Indian Journal of Dermatology Venereology Leprology 75:214-6. |
|
|
Miller DC, Dunn, RL, Wei LT (2002). Assessing the Performance and Validity of Diagnostic Tests and Screening Programs. Clinical Research for Surgeons. D. F. Penson and J.T. Wei © Humana Press Inc., Totowa, NJ pp 157-174 |
|
|
Modibbo FI, Dareng E, Bamisaye P, Jedy-Agba E, Adewole A, Oyeneyin L, Olayinka Olaniyan O, Adebamowo C (2016). Qualitative study of barriers to cervical cancer screening among Nigerian women. BMJ Open 6:e008533. |
|
|
Mukama T, Ndejjo R, Musabyimana A, Halage AA, Musoke D (2017). Women's knowledge and attitudes towards cervical cancer prevention: a cross sectional study in Eastern Uganda. BMC Women's Health 17:9. |
|
|
Mwaka DA, Orach GC, Were ME, Lyratzopoulos G, Wabinga H and Roland M (2015). Awareness of cervical cancer risk factors and symptoms: cross-sectional community survey in post-conflict northern Uganda. Health Expectations 19:854-867. |
|
|
Nguefack TC, Biwole EM, Massom A, Kamgaing TJ, Njamen NT, Ekane HG, Obinchemti ET, Priso BE (2012). Epidemiology and surgical management of breast cancer in gynecological department of Douala General Hospital. Pan African Medical Journal 13: 35. |
|
|
Nkfusai NC, Cumber SN, Takang W, Anchang-Kimbi JK, Yankam BM, Cho Sabastine Anye, Tsoka-Gwegweni JM, Enow-Orock GE 10, Anong ND (2019). Cervical cancer in the Bamenda Regional Hospital, North West Region of Cameroon: a retrospective study. Pan African Medical Journal 32:90. |
|
|
Ogembo RK, Gona PN, Seymour AJ, Soo-Min Park H, Bain PA, Maranda L, Ogembo JG (2015). Prevalence of Human Papillomavirus Genotypes among African Women with Normal Cervical Cytology and Neoplasia: A Systematic Review and Meta-Analysis. PLoS ONE 10(4):e0122488. |
|
|
Okunowo AA, Daramola SE, Soibi-Harry PA, Ezenwankwo CF, Kuku OJ, Okunade SK , Anorlu IR (2018). Women's knowledge of cervical cancer and uptake of Pap smear testing and the factors influencing it in a Nigerian tertiary hospital. Journal of Cancer Research and Practice 5; 105e111. |
|
|
Paolino M, Arrossi S (2011). Women's Knowledge About Cervical Cancer, Pap Smear and Human Papillomavirus and Its Relation to Screening in Argentina. Women & Health, 51:72-87. |
|
|
Sichanh C, Quet F, Chanthavilay P, Diendere J, Latthaphasavang V, Longuet C and Buisson Y (2014). Knowledge, awareness and attitudes about cervical cancer among women attending or not an HIV treatment center in Lao PDR. BMC Cancer 14:161. |
|
|
Solomon D, Davey D, Kurman R, Moriarty A, O'Connor D, Prey M, Raab S, Sherman M, Wilbur D, Wright T Jr, Young N; Forum Group Members; Bethesda 2001 Workshop (2002). The 2001 Bethesda System: terminology for reporting results of cervical cytology. The Journal of the American Medical Association 287(16):2114-2119. |
|
|
Sreedevi A, Javed R, Dinesh A (2015). Epidemiology of cervical cancer with special focus on India. International Journal of Women's Health 7:405-414. |
|
|
Srivastava AN, Misra Jata S, Kunwar S, Fatima N, Khan Mohshin A (2018). Identifying Different Risk Factors of Cervical Cancer in Rural Women Population of Lucknow West, India: A 5 Years Study. Open Access Journal of Oncology and Medicine 2(4). |
|
|
Tebeu PM, Domgue FJ, Crofts V, Flahaut E, Catarino R, Untiet S, Vassilakos P and Petignat P (2015). Effectiveness of a two-stage strategy with HPV testing followed by visual inspection with acetic acid for cervical cancer screening in a low-income setting. International Journal of Cancer 136:E743-E750. |
|
|
Tufon EN, Yuwun NB, Egba SI, Ndohnui NN (2013). Prevalence, associated risk factors and methods of diagnosing cervical cancer in two hospitals in Yaoundé, Cameroon. International Journal of Advanced Research in Pharmaceutical Bio Sciences: 3(1), 55-59. |
|
|
Ubajaka C, Ukegbu A, Ilikannu S, Ibeh C, Onyeonoro U, Ezeanyim A (2015). Knowledge of Cervical Cancer and Practice of Pap Smear Testing among Secondary School Teachers in Nnewi North Local Government Area of Anambra State, South Eastern Nigeria. Advances in Sexual Medicine 5:13-21. USPSTF. Screening for Cervical Cancer (2018). |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


