Full Length Research Paper

ABSTRACT
In response to the high occurrence of diarrhea in Ethiopia, the Federal Ministry of Health employed an effective strategy that included administration of zinc together with oral rehydration salt to treat children suffered diarrhea since 2013. Nonetheless, information on zinc bundled with ORS uptake is limited and thus this study has examined zinc utilization among beneficiaries. A community based cross-sectional study was conducted among 422 households whose under-five- children (U5C) had diarrhea in Akaki sub city from February to March, 2016. Prior to selection of households, participants were identified through health facilities and were traced using their household number. Relevant socio-demographic and other important health information were collected from respective caretakers using a pre-tested structured questionnaire through interview. Data were then entered using Epi Info Version 3.5.4, exported and analyzed using SPSS version 20 software. Both bivariate and multivariate regression analyses were used to identify the factors related to zinc utilization and a p-value below 0.05 was considered as statistically significant. All recruited subjects participated in the study with 100% response rate. Of the 422 participants, 283 (67.1%) caretakers used zinc bundles with ORS when the under-five-child had diarrhea. The majority (82.2%) sought treatment from health centers though their major (80.90%) source for zinc was private pharmacies. Following zinc intake, diarrhea subsided within 1-3 days in most (76.3%) of them. About the same proportion of caretakers recommended the zinc for watery diarrhea and the vast majority (90.5%) were satisfied with zinc supplement. Caregivers' whose child diarrhea stopped were more likely (AOR=10.29; 95% CI=2.52-42.05) to use zinc while those whose child diarrhea stopped after six days (AOR=0.09; 95% CI=0.02-0.45) and had mucoid diarrhea (AOR=0.32; 95% CI=0.10-0.97) were less likely to give their children the zinc than their counterparts. The study thus revealed that slightly over two in three children were given diluted zinc and the major augmenting factors for the zinc bundled with ORS uptake were withholding to administer the full dose, stopping the drug when diarrhea improved and recommending zinc therapy. It is thus essential to consider the above determinants, avail the zinc in the government facilities, improve zinc bundled with ORS intake and ultimately reduce deaths emanating from diarrhea.
Key words: Diarrhea, Zinc utilization, determinants, cross sectional community based study, Ethiopia
INTRODUCTION
Children diarrhea is one of the major killers in most developing countries with infants and young children the most vulnerable in most developing countries (Fischer Walker et al., 2012). Studies have shown that under-five-children go through 2.9 episodes of diarrhea per year in developing countries leading to depletion of zinc in the body and consequently aggravate any pre-existing zinc deficiency (Fischer Walker et al., 2012; Brown et al., 2004). Zinc deficiency, in addition to exacerbating diarrheal episode, predisposes to several morbidities and malnutrition (Fischer Walker et al., 2009; Shankar and Prasad, 1998; Bhutta et al., 1999), indicating that zinc is an important micronutrient which plays a critical role in cellular growth and function of the immune system (Omuemu, 2012). Available evidences suggests that supplementing zinc and oral rehydration salt (ORS) would benefit children with diarrhea due to the above mentioned effect and consequently reduces the incidence as well as duration and severity of acute and persistent diarrhea (Walker and Black, 2010; WHO and UNICEF, 2004; Fischer Walker et al., 2009).
Cognizant of the benefits of zinc and the magnitude of diarrhea, WHO and UNICEF recommends 20 mg zinc for young children, 10 mg zinc for infants under six months of age to be given with ORS for 10–14 days for diarrhea treatment (WHO and UNICEF, 2004) while feeding is continued; along with increasing the amount of fluid to reduce dehydration and other health consequences. Based on the guideline of WHO/UNICEF diarrheal management, a number of developing countries including Ethiopia adopted zinc supplement to their national policy on diarrhea treatment, though the majority still are not employing the initiatives due to caretakers and frontline health workers knowledge gap of zinc including unavailability of zinc in the government sectors (Ogunrinde et al., 2011; Uchendu et al., 2011).
In Ethiopia, diarrhea accounts for about 14% of outpatient visits and 16% hospital admissions attributed to poor hygienic practices and gap of knowledge among caretakers and some frontline health workers with the new diarrheal management initiatives which includes zinc bundles with ORS (Walker and Black, 2010; WHO and UNICEF, 2004). In addition to the above traits, chronic child malnutrition compounded by low consumption of animal sources of food indicates that zinc deficiency is prevalent and there is high possibility for the occurrence of child diarrhea (Fischer Walker et al., 2009; Central Statistical Agency [Ethiopia] and ICF International, 2012; Wanzahun Godana, 2013). According to the 2011 demographic health survey, the magnitude of childhood diarrhea has a diverse figure and ranged from 30 to 13.7%, showing some regional variations while information on zinc utilization is unavailable indicating that it is a gap to be addressed (Wanzahun Godana, 2013). This study has addressed the above gap and examined the utilization of the new zinc initiative including its augmenting factors to provide evidence based information for some program improvement.
METHODS
Study design and settings
A community based cross-sectional study was conducted among 422 households whose under-five children had diarrhea in Akaki sub city, Addis Ababa, Ethiopia from February to March, 2016. The sub-city constitutes 11 districts of which 8 are urban and the rest are partially rural and were home for 224,370 people with female population being 51.5%. The sub city had 6 government owned and one private health centers (Central Statistical Agency [Ethiopia] and ICF International, 2012). Also, 3 districts that reported high figure of diarrhea were purposively selected.
Study populations
Prior to selection of households, participants were identified through health facilities and were traced using their household number. All caretakers who had under-five-children and sought treatment for diarrhea in the last three months prior to the study in the sub-city were identified from all facilities in the sub-city. From this list, household information was picked for the sampled districts and a fresh list of household consisting of 2030 was prepared to constitute the sampling frame.
Sample size determination and sampling procedures
The sample size was determined using single proportion formula based on the estimation of the proportion of diarrhea in the study area; which implies that 50.0% (Central Statistical Agency [Ethiopia] and ICF International, 2012), absolute precision of 5.0 and 95% level of confidence with a non-response rate of 10% yielded a total of 422 subjects. To sample the households, the sampling frame was divided by the sample size and accordingly, every fifth household with a random start was selected from the sampling frame until the required sample size was reached. The sampled households were then traced through the female health extension workers’ place of residence and were recruited after their verbal consent was obtained based on the inclusion criteria (caretakers with under-five children who sought diarrheal treatment and permanent resident with no disability).Each voluntary caretaker from the respective households was face-to-face interviewed at their home at their convenience.
Data collection instrument and procedure
Data were collected using a pre-tested structured questionnaire by reviewing previous similar studies conducted (Brown et al., 2004; Fischer Walker et al., 2009; Shankar and Prasad, 1998; Bhutta et al., 1999; Omuemu, 2012; Walker and Black, 2010; George et al., 2013; Central Statistical Agency [Ethiopia] and ICF International, 2016; Larson et al., 2011) that captured the study objectives. The questionnaire included information on socio-demographic/economic characteristics, caregiver practice in terms of giving fluid during diarrhea, feeding, zinc utilization including its sources and other household hygienic practices. Eleven data collectors comprised of Health Extension workers (HEWs), graduate nurses fluent in the local languages and two supervisors (Health Officers) with relevant experience were recruited and trained for two days by the investigators on the method of data collection. The training addressed issues such as the content of the questionnaire, basic interviewing skills, and filling out of the questionnaire.
Data quality management
The quality was observed at different levels and included the followings: due emphasis was given to questionnaire designing to capture the objectives of the study, logically sequenced, free of scientific terms and non-leading structured questionnaire and pre-tested on 5% of caretakers in non-sampled districts of the sub-city. The data collectors and supervisors were trained on the objective of the study, contents of the questionnaires and how to maintain confidentiality and privacy of the study subjects. The collected data were checked by the investigator on daily basis for any incompleteness and/or consistency and timely action was made.
Statistical analysis
Data were checked for completeness, coded, and entered using Epi-Info version 3.5.4 and then exported to SPSS version 20 for cleaning and analysis. The results are presented in percentages and tables/graphs where appropriate. Binary logistic regression was employed to examine the associations between socio-demographic variables and the outcome variables (zinc bundled with ORS uptake). To ascertain the association between the dependent and explanatory variables, simultaneous control for the aforementioned explanatory variables (all socio-demographic characteristics and other covariates associated in bivariate with p<0.2 were used and entered) step-wise logistic regression was applied and adjusted odds ratios (AORs) and confidence intervals (95% CI) were calculated. In all analyses, P< 0.05 was considered to be statistically significant.
Operational definitions
Acute diarrhea: Abrupt onset of three or more loose stools per day and lasts no longer than 14 days.
Caretaker: Any caregiver who brought the child to health center.
Zinc supplements: Refers to provision of 20 mg zinc for young children or half for infants below six months of age together with ORS for 10–14 days as diarrhea treatment.
Oral rehydration salts (ORS): Refers to a balanced glucose–electrolyte mixture.
Ethics approval and consent to participate
Ethical approval was obtained from the School of Public Health Research Ethics Review Committee of Addis Ababa University, College of Health Sciences. Permission was also secured from the Regional Health Bureau as well as from the respective district administration and Health Office. Verbal consent was obtained from each caretaker after the objective of the study was explained to all of them in their local language and the right to withdraw from the study at any time was also communicated. Anonymity and confidentiality of the information was assured and privacy of each respondent was maintained throughout the data collection process.
RESULTS
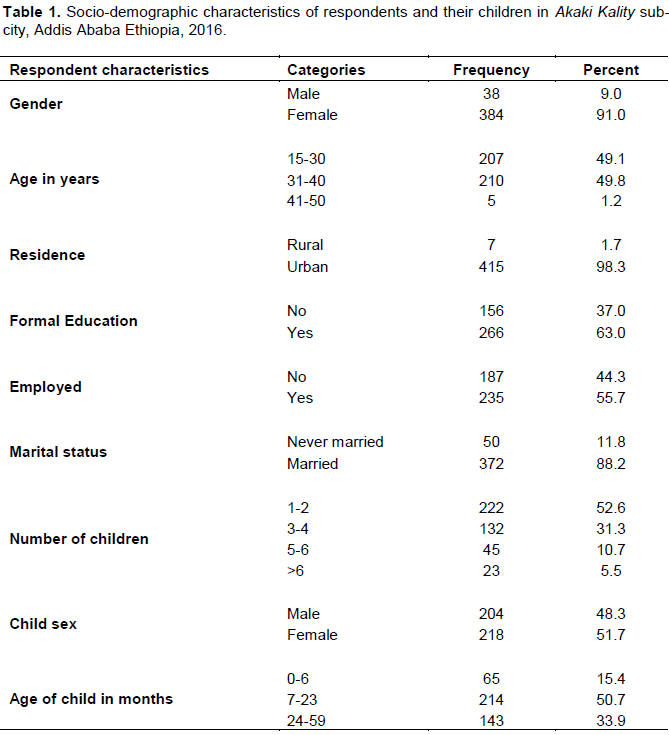
A total of 422 caretakers participated in the study with a response rate of 100%. The majorities (98.3%) of them were from urban settings and were females (91.0%). About half (49.8%) had age range between 31 and 40 years and nearly two-thirds (63.0%) had formal education and over half (55.7%) had their own business. The majorities (88.2%) were married and over half (52.6%) had between one and two children. In terms of child sex, female (51.7%) was slightly higher than male (48.3%) children. Nearly three-quarters (71.1%) of the affected age groups were children below the age of 23 months (Table 1).
As shown in Figure 1, slightly over two-thirds (67.1%) of caretakers used the zinc bundle with ORS during the recent diarrheal attack.
Table 2 demonstrates participants’ response to Zinc bundled with ORS uptake/supplement and other important characteristics. All participants heard about zinc supplement and their major source of information was through television (50.7%). Over a quarter (29.1%) of them preferred treating child with diarrhea with antibiotic and 107 (25.4%) used antispasmodic syrup and 57 (13.5%) mentioned zinc supplements which is low. The majority (82.2%) sought treatment from health centers though their major (80.90%) source of obtaining the zinc was from private pharmacy and about the same proportion of them diluted in water. Slightly over half (52.3%) administered zinc for seven days because the diarrhea stopped in 128 (45.2%). Some of the reasons stated for not giving the prescribed full dose of zinc was due to its unpleasant taste (15.2%), vomiting (12.3%) and diarrhea (26.8%). On the other hand, reasons stated for not using the zinc was unawareness in 57 (41.0%), unsure of administering the zinc in 29 (20.9%) and its cost was expensive in 53 (38.1%). Following zinc intake, over three-quarters mentioned that diarrhea subsided within 1-3 days; about the same number of respondents recommended zinc for watery diarrhea and the vast majority (90.5%) was satisfied with the zinc supplement.
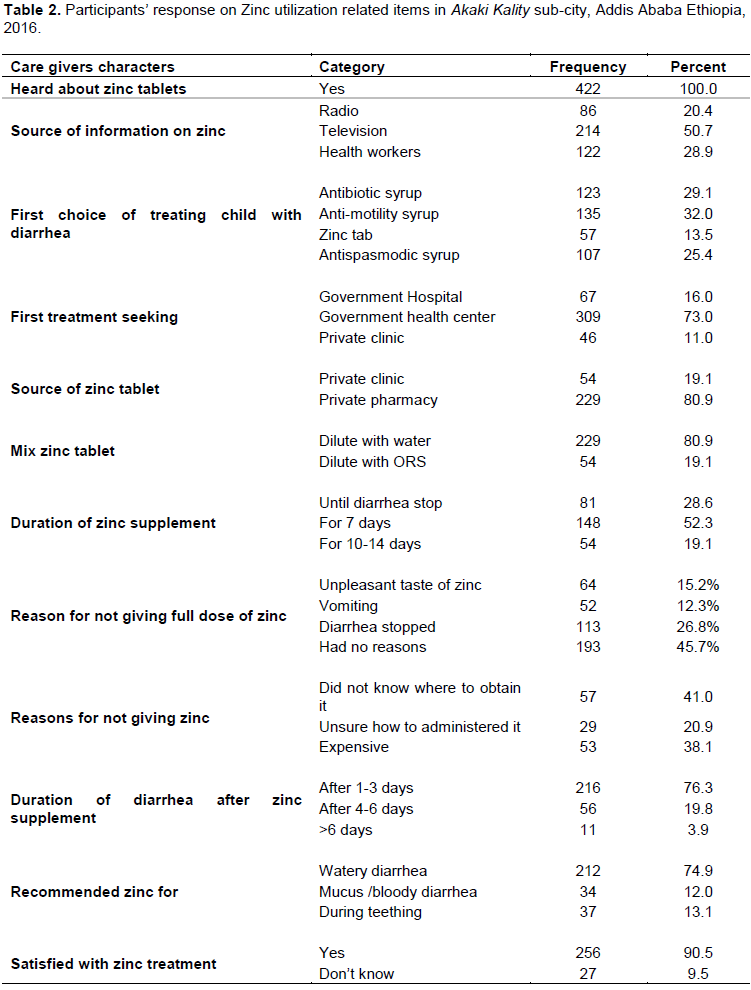
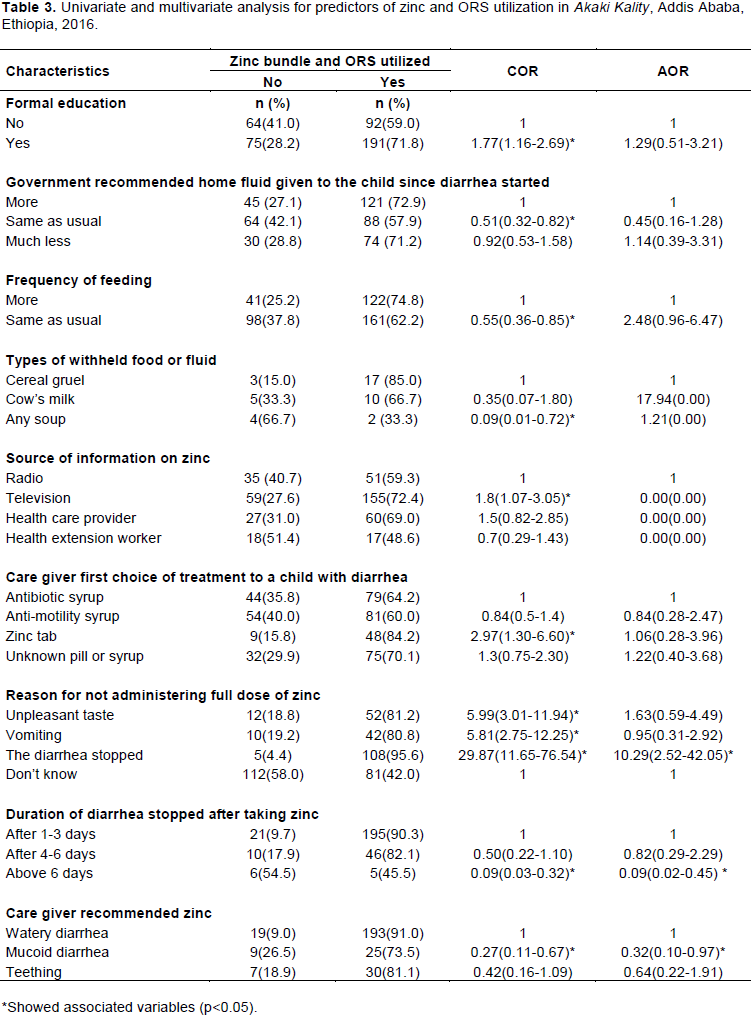
Table 3 displays the result of binary logistic regression and revealed that zinc bundled with ORS utilization was associated with participant education, governmental recommendation of home fluid to the child during diarrhea, frequency of food feeding, types of withheld food or fluid, source of information on zinc, caregiver first choice of treatment to a child with diarrhea, reason for not giving full dose of zinc, duration of diarrhea stopped after taking zinc and caregivers recommending zinc therapy. Nonetheless, after adjusting for the confounding effect of the above variable, only reason for caregivers not giving full dose of zinc, duration of diarrhea stopped after taking zinc therapy, and caregivers recommending zinc therapy remained significantly associated with utilization of zinc bundle with ORS.
Those caregivers who stopped giving full dose of zinc after diarrhea stopped were more likely (AOR=10.29; 95% CI=2.52-42.05) to use zinc while those whose child diarrhea stopped after six days (AOR=0.09; 95% CI=0.02-0.45) and had mucoid diarrhea (AOR=0.32; 95% CI=0.10-0.97) were less likely to give zinc for their children than the referent groups.
DISCUSSION
This study has examined the utilization of zinc bundled with ORS and its determinants. Based on our findings utilization of zinc bundled with ORS as recommended by WHO and UNICEF(2004) is 67.1%.Compared with some previous studies done elsewhere, the current zinc bundled with ORS use is higher than what has been reported for Nigeria (67.1% vs. 8.3%)(George et al.,2013) and comparable to the Kenyan findings (67.1% vs. 67%)
(Alex–Hart, 2014). On the other hand, when the current findings is compared with the recent EDHS 2016, our result still appears to be two-folds (67.1% vs 33%) (Central Statistical Agency [Ethiopia] and ICF International, 2016). This is likely due to seasonal variation and high occurrence of diarrhea in the study site as well as other important factors such as respondents’ health seeking behavior during diarrhea episode. Even though zinc bundled with ORS utilization was associated with various socio-demographic characters and other health related variables only withholding to administer the full dose, stop giving the drug when the child feels better or his bowel habits improve and recommending zinc therapy were the determinants. Such information are however, limited in our settings and could not compare and contrast with other studies warranting further studies.
In spite of the unavailability of the zinc supplement at government health facilities, all caretakers whose child suffered diarrhea and prescribed zinc in the health centers bought the commodity from private clinic and private pharmacy indicating that the new diarrheal management initiative is acknowledged by the respondents similar to that of Kenyan study (Alex–Hart, 2014).
In terms of awareness of the commodity, all participants heard about zinc supplement and their major source of information was through television. This observation would pave the way for scaling up of the commodity in the community and highlights the need to avail the commodity within the public facilities, private health systems and community level if we are to end the burden of diarrhea and improve child survival. While this finding is encouraging, there were also some unhealthy experiences noted in this study where respondents ranked anti-motility and antibiotic treatment as their first choice to treat and needs some remedial action through an appropriate behavioral change communication diarrhea and bring some attitudinal changes towards the use of the right treatment for child diarrhea such as the use of zinc and ORS.
The extent of zinc treatment practices, the majority diluted in water and most of them used the supplement for seven days and few others provided the full dose for 10 – 14 days. This finding however, when compared with the Bangladesh figure (Larson et al., 2011), is lower (12.8% vs. 19.7%). The discrepancy could be attributed to the difference in caregiver’s knowledge. Although, the observed zinc dose administered is good, zinc still promotional activities through other non-health avenues like mass media and is essential to adhere with the proper dose of treatment in order to reduce diarrhea related morbidities.
In the present study, it appears that considerable number of respondents used the zinc supplement, and close to one-third of them however, did not because of unawareness, unsure of how to administer zinc and its cost. This calls for more advocacy work through continuous reinforcing of health information for health workers to ensure accuracy and consistency in the health messages that they communicate at the health facilities when treating diarrhea. Other approach is to use non health avenues such as media which this study and the Nepal finding have shown (Wang et al., 2011) that media is an important source of information to increase awareness. The other interesting findings of this study is that the vast majority was satisfied with the commodity and recommended zinc for diarrhea suggesting a fertile ground to scale up the commodity in the community; our study is concordant with the study done in Kenya where all caregivers stated that zinc is used for diarrhea (Alex–Hart, 2014).
Although zinc utilization was crudely associated with participant education, governmental recommendation of home fluid to the child during diarrhea, frequency of food feeding, types of withheld food or fluid, source of information on zinc, caregiver first choice of treatment to a child with diarrhea, reason for not giving full dose of zinc, duration of diarrhea stopped after taking zinc and caregivers recommending zinc therapy, only reason for caregivers not giving full dose of zinc, duration of diarrhea stopped after taking zinc therapy, and caregivers recommending zinc therapy remained significantly associated with utilization of zinc bundle with ORS. Those caregivers who stopped giving full dose of zinc after diarrhea stopped were more likely to uses zinc while those whose child diarrhea stopped after six days and had mucoid diarrhea were less likely to give their children the zinc.
It is interesting to note that full dose of zinc had never been administered in this study because since diarrhea stopped and most of the diarrhea cases took six days duration. In addition, respondents who recommended the bundled with ORS uptake of the commodity for mucoid diarrhea and teething were less likely to use the supplement than those who recommended for watery diarrhea.
Strengths and limitations
The study was community based, used primary data with 100% response rate and minimized bias due to the wide variety of potential predictors which were controlled during analysis, including those that have never been examined in association with zinc utilization is the strength of the study. Nonetheless, mothers’ self-report of both the dependent and independent variables may have resulted in information bias. Other than this, the cross-sectional nature of the data we cannot infer causal relationships.
CONCLUSION
Slightly over two in three children used the commodity and the major augmenting factors for the zinc bundled with ORS uptake were withholding to administer the full dose, stop giving the drug when the child feels better or his bowel habits improve and recommending zinc therapy.
RECOMMENDATION
Given the unavailability of the commodity at government facility, it is thus essential to consider to avail the commodity in all public facilities to reinforce the new treatment of diarrheal initiative in order to improve child survival. It is also essential to establish an opportunity to raise awareness and improve practice related to the treatment of diarrhea with zinc and ORS as there were some misconceptions and low awareness on the zinc bundle administration. Other than this, providing free zinc to children whose mothers have low levels of social support, and considering refreshing trainings on diarrheal management may result in meaningful improvements in the zinc bundled with ORS uptake of the commodity.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGEMENTS
The authors are grateful to Addis Ababa University, Postgraduate School for clearing the study; the senior author Prof. Jemal Haidar from the School of Public Health, Addis Ababa University, Ethiopia; the Addis Ababa Regional Health Bureau; the district health offices including the participants for their all-round intensive support.
REFERENCES
|
Alex–Hart BANOaBA (2014). Home Management of Diarrhoea by Caregivers Presenting at the Diarrhoea Training Unit of a Tertiary Hospital in Southern Nigeria. British Journal of Medicine and Medical Research 4(35):5524-5540. |
|
|
Bhutta ZA, Black RE, Brown KH, Gardner JM, Gore S, Hidayat A, Khatun F, Martorell R, Ninh NX, Penny ME, Rosado JL (1999). Prevention of diarrhea and pneumonia by zinc supplementation in children in developing countries: pooled analysis of randomized controlled trials.Journal of pediatrics 135(6)689-697. PubMed PMID: 10586170. |
|
|
Brown KH, Rivera JA, Bhutta Z, Gibson RS, King JC, Lonnerdal B, (2004). International Zinc Nutrition Consultative Group (IZiNCG) technical document #1. Assessment of the risk of zinc deficiency in populations and options for its control. Food and nutrition bulletin 25(1Suppl 2):S99-203. Epub 2007/12/01. PubMed PMID: 18046856. |
|
|
Central Statistical Agency [Ethiopia] and ICF Internationa (2012). Ethiopia Demographic and Health Survey 2011. Addis Ababa, Ethiopia, and Calverton, Maryland, USA: Central Statistical Agency and ICF international . |
|
|
Central Statistical Agency [Ethiopia] and ICF International (2016). Ethiopia Demographic and Health Survey. Addis Ababa, Ethiopia, and Calverton, Maryland, USA: Central Statistical Agency and ICF international. |
|
|
Fischer WCL, Ezzati M, Black RE (2009) Global and regional child mortality and burden of disease attributable to zinc deficiency. European journal of clinical nutrition 63(5):591. |
|
|
Fischer WCL, Perin J, Aryee MJ, Boschi-Pinto C, Black RE (2012). Diarrhea incidence in low- and middle-income countries in 1990 and 2010: a systematic review. BMC Public Health 12:220. Epub 2012/03/23.PubMed PMID: 22436130; PubMed Central PMCID: PMC3323412. |
|
|
Fischer WCL, Fontaine O, Young MW, Black RE (2009). Zinc and low osmolarity oral rehydration salts for diarrhoea: a renewed call to action. Bulletin of the World Health Organization 87:780-786. |
|
|
George A, Otieno GMB, Bryan O, Nyawanda FA, Robert F, Breiman RF, Larson CP (2013).Caretakers' Perception towards Using Zinc to Treat Childhood Diarrhoea in Rural Western Kenya. Journal of health population and nutrition 31(3):321. |
|
|
Larson CP, Koehlmoos TP, Sack DA (2011). Scaling up zinc treatment of childhood diarrhoea in Bangladesh: theoretical and practical considerations guiding the SUZY Project. Health Policy Plan. Epub 2011/02/24 |
|
|
Ogunrinde OG, Raji T, Owolabi OA, Anigo KM (2011). Knowledge, Attitude and Practice of Home Management of Childhood Diarrhoea among Caregivers of Under-5 Children with Diarrhoeal Disease in Northwestern Nigeria.Journal of tropical pediatrics 58(2):143-146. |
|
|
Omuemu VO (2012). Knowledge and Use of Zinc Supplementation in the Management of Childhood Diarrhoea among Health Care Workers in Public Primary Health Facilities in Benin-City,Nigeria. Global Journal of Health Science 4(2):68. |
|
|
Shankar AH, Prasad AS (1998). Zinc and immune function: the biological basis of altered resistance to infection. American Journal of clinical nutrition 68(2)447-463. |
|
|
Uchendu UO, Emodi IJ, Ikefuna AN (2011). Pre-hospital management of diarrhoea among caregivers presenting at a tertiary health institution: implications for practice and health education. African health sciences 11(1):41-7. |
|
|
Walker CL, Black RE (2010). Zinc for the treatment of diarrhoea: effect on diarrhoea morbidity, mortality and incidence of future episodes. International journal of epidemiology 39(suppl_1):63-69. |
|
|
Wang W, MacDonald VM, Paudel M, Banke KK (2011).National scale-up of zinc promotion in Nepal: results from a post-project population-based survey. Journal of health population and nutrition 29(3):207-217. |
|
|
Wanzahun GBM (2013).Environmental factors associated with acute diarrhea among children under five years of age in derashe district, Southern Ethiopia. Science Journal of Public Healh 1(3):119-124. |
|
|
WHO (2004). UNICEF Clinical management of acute diarrhoea (WHO/FCH/CAH/04.07). Geneva and New York: World Health Organization & United Nations Children's Fund. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


