Full Length Research Paper

ABSTRACT
We assessed whether the emergency room at Yaoundé Central Hospital (YCH) met international standards; while analyzing factors that are associated with the length of stay, a key performance indicator of the emergency medicine department. Based on the data of patient admissions and discharges recorded from February 2017 to June 2018 in the emergency room of YCH, data was extracted from about two thousand research subjects; then an observational, non-randomized, cross-sectional study was conducted. The mean length of stay was 23.73±0.634 hours in the emergency room of YCH. Using binomial logistic regression analysis, the diagnostic severity was positively associated with a long length of stay when controlled for other factors, ORa=1.65, p=0.037; bed availability in the peripheral care units, however, did play a confounding role in the relationship, p=0.026. Furthermore, the analysis of the variances showed that less than 1% of the change that occured in the mean length of stay was explained by sociodemographic factors alone; whereas, less than 6% of that change was due to clinical factors. The patient’s mean length of stay in the emergency room of YCH did not meet international standards. Sociodemographic and clinical factors could not alone explain 93% of the observed long length of stay. We should look for other inputs from factors such as patient’s financial capacity or health insurance availability, protocols of care, diagnostic and therapeutic effectiveness.
Key words: Emergency medicine department, patient’s length of stay, performance indicator, predictive factors, observational cross-sectional study, low middle income country.
INTRODUCTION
Managing a healthcare organization requires performance control and quality improvement. This assumption reveals a dire need for evidence-based data on the performance of the healthcare units (Greg et al., 2010; Chamberlain and Pollack, 1998; Cameron et al., 2011; Sorup et al., 2013). Among patient care units, emergency medicine department (EMD) represents one of the most sensitive places where indicators can shed light on the performance, henceforth help enhance quality control and improve the organization’s management policy. In the emergency room (ER), the length of stay (LOS) is the elapsed time between the admission and discharge of a patient. Previous research studies had indicated that the LOS could be a relevant performance indicator of the structure and procedure in the ER (Kusumawati et al., 2019; Alemu et al., 2019; Rahman et al., 2015). The structure of the ER refers to the diagnostic equipment such as laboratory and radiology services, drugs and beds availability in the ER and peripheral care units. The procedure on the other hand, is the protocols of care or the decision-making steps that guide healthcare providers on duty (Rahman et al., 2015). Thus, assessing the patient’s LOS could provide reliable information on structural and procedural aspects of the health care unit in charge of acute health conditions. It was in this context, that Kusumawati et al. (2019) had studied the average LOS in ER of Yogyakarta, Indonesia. They found it at 5.5 h, and factors like disease acuity levels, specialist consult and needs of admission to other care units were associated with increased time spent in the ER. In Ethiopia, Alumu et al. (2019) had found the LOS to be higher than 24 h due to inadequacy of bed availability in patient ward, overcrowding, lack of laboratory tests and delayed radiological procedures. In their study, Nanayakkara et al. (2014) in the ER of Australia and New-Zealand, had evaluated the length of patient’s stay before being transferred to another care unit. The median LOS ranked between 2.5 and 5.1 h, according to the decision-making method and after adjustment with diagnosis, type of health facility and its geographical location. In Denmark, Sorup et al. (2013), had led a systematic review of many research articles, on fourteen selected items, time intervals and measures associated with the patient predominantly were in the performance measures identified in the American, British, Swedish and Canadian articles.The LOS, time between patient arrivals and first clinical review, and time between patient arrivals and their first clinical examination were highlighted by many articles. Among fifty-five identified EMD performance measures, the intervals of time spent in the ER were the most recommended performance measurement (Rose et al., 2016; Schroeder et al., 2016; MacFarlane and Benn, 2003).
In Cameroon, we were unable to identify a published research study on this topic. However, Garga and Ongolo-Zogo (2013) had published a backgrounder strategy to inform discussions between policymakers and stakeholders, about the strategic options and considerations, to improve reception and management of emergencies in national and regional hospitals; but, the authors did not carry out an evaluation of the performance indicators of any EMD. Thus, the lack of published work in Cameroon has provided the rationale for conducting a research study of the predicting factors associated with the patient’s average LOS in the ER of Yaoundé Central Hospital.
METHODOLOGY
Study design
An observational cross-sectional study using secondary data that was collected by the nursing staff of the ER, then stored in the registration books of patient admissions and discharges. The study duration ran from February 2017 to June 2018; within that period, we extracted data of nine months from the registration books.
Choice of the healthcare facility
The Yaoundé Central Hospital (YCH) was opened in 1933 as the Central Africa Hospital and is one of the oldest clinics in Cameroon. It is located within the administrative square of the capital city of Cameroon and hosts many medical specialties, including the Intensive Care Unit (ICU), the Emergency Medicine Department (EMD), and the High Standing Pavilion for upper-class personalities. The EMD admits about two thousand patients annually; more information on YCH can be found on the hospital website (Yaoundé Central Hospital, https://www.hopitalcentral.cm).
Study participants
Participants were any person who sought medical attention in the ER.
Inclusion criteria
All individuals admitted in the ER by the triage nurse and whose sociodemographic and clinical data were collected during the study period.
Exclusion criteria
(1) Any person recorded as dead upon arrival in the ER;
(2) Patient’s file classified as damaged or empty.
Sampling method and size
A non-randomized, non-stratified convenient sampling method was used to select our study participants. It was not necessary to compute our sample size since we were able to secure a large sample. As an observational study, we opted for a large sample bigger than one thousand research subjects to reduce both the impact of missing data, and a type II statistical error. We extracted data from 1987 study participants. However, four hundred and twenty eight persons were reported dead upon arrival at ER triage station and were excluded from the final sample.
Variables
The outcome variable is the patient’s LOS. It was expressed as a quantitative and categorized variable in linear and logistic regressions, respectively. Class levels were “long” versus “short” stay in hours, with short-stay being the class reference. A long stay was defined as higher than 24 h and short stay if otherwise. Since data on arrival and discharge times were not recorded, the median LOS obtained from descriptive statistics was retained as the cut-off point to categorize the LOS. The only quantitative variable among sociodemographic factors (SDF), “age”. It was categorized in three class levels, young if less than 30-year-old, adults between 30 and 60 and elder if higher than 60-year-old. Family annual income levels were defined following the patient profession by low, middle, and high income.
All clinical factors (CF) were quantitative variables including the nursing team that recorded the data. Our main explanatory variable of the patient’s LOS was the diagnosis, made by the ER attending physicians and was categorized in two class levels “severe” and “mild”; severe when clinical decompensation of chronic diseases, shock or impaired consciousness were present; mild if otherwise. Clinical outcomes were categorized in “transfer”, “left without being seen (LWBS)” and “death occurring after admission”. Transferred patients were those admitted in the peripheral care unit or discharged with the consent of the physician to return home. The nursing teams were labeled as A, B, C, D, and unknown teams (UK). The label of the UK team was assigned when the nurse staff who recorded the data forgot to indicate the team’s label.
Statistical methods
We performed descriptive statistics for quantitative variables to assess the central tendency (mean or median) and the spread or dispersion (standard deviation or standard error of the mean). We computed proportions of qualitative variables.When the quantitative variables LOS and “age” followed a normal distribution, the logarithmic transformation was not required to perform a linear regression analysis. We assessed the variances of the patient’s average LOS among categories of SDF and within class levels of SDF and CF through analysis of variances using the Kruskal Wallis test.
Finally, we used a binomial logistic regression to look for a possible alternative explanations of the association between diagnosis and the average LOS, adjusted for covariates in a multivariate analysis. All decisions with respect to our research hypothesis were made based on the statistical significance p-value less or equal to 0.05, issued provided either by the Chi-square test or Fisher exact test for logistic regression, and non-parametric Kruskal Wallis test for analysis of variances. Missing data (MD) were treated as “missed” in all statistical analyses using IBM-SPSS software version 20.
RESULTS
Data was extracted from 1986 research subjects in which 21.55% (428) were found dead upon arrival to the ER and were excluded from the study following our selection criteria. The final sample size was made of 78.45% (1558). The average patient’s LOS was 23.73 [22.49-24.79 h] and the mean age was 48.89 [47.89-49.89] year-old results not displayed in (Table 1).
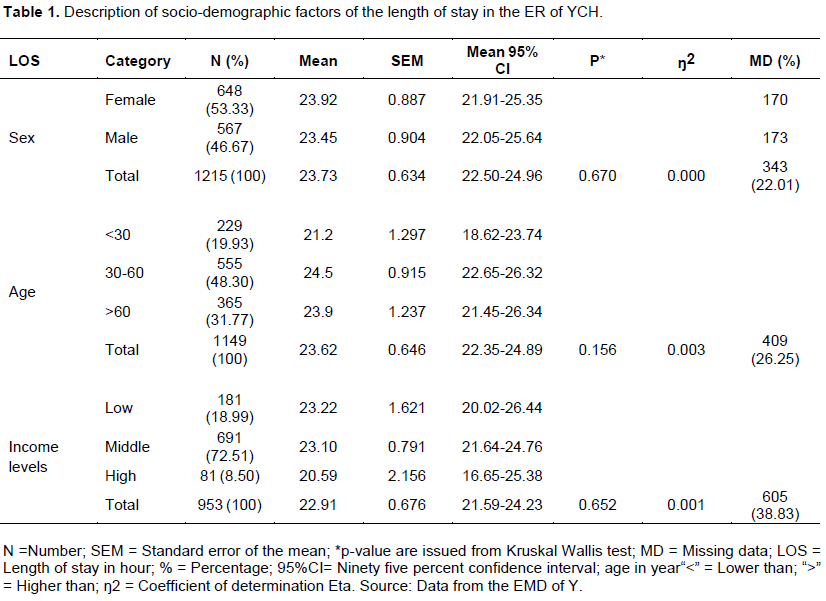
Description of sociodemographic factors (SDF) of the LOS
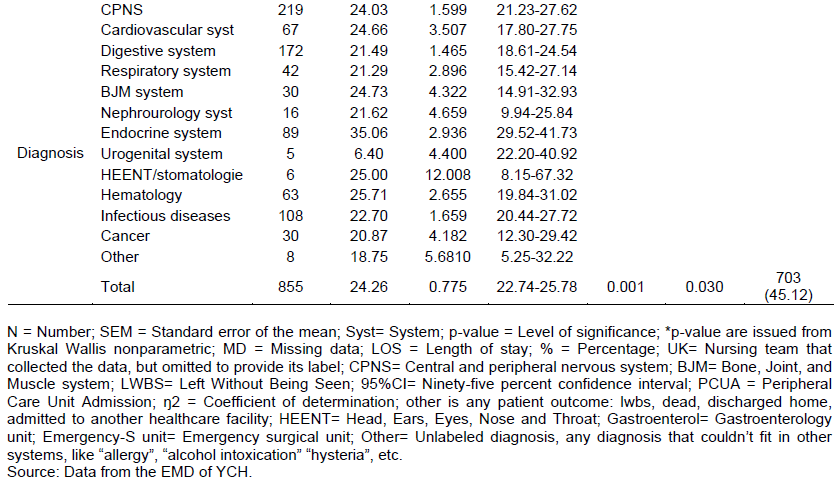
The mean difference within each SDF was statistically non-significant explaining why the mean LOS did not change when it was adjusted for SDF. Consistently, the coefficient of determination (Å‹2) showed that the proportion of variance in the mean LOS that can be explained by SDF was around 0.0%; 0.3% and 0.1% for gender, age, and income, respectively.
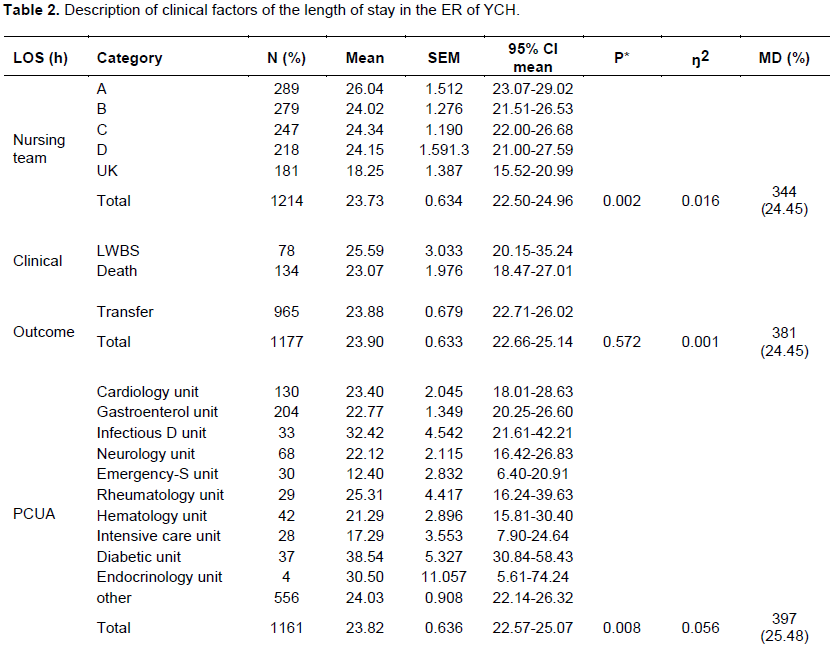
Description of clinical factors (CF) of the LOS
The median LOS for each CF widely varies from 2 to 48 h (Figures 1 and 2). The mean LOS according to CF (Table 3) showed no mean difference within clinical outcome categories (p=0.572); however, the mean difference was statistically significant within diagnosis (p=0.001), PCUA (p=0.008) and nursing team (p=0.002) categories; providing the evidence of change in the LOS when adjusted for CF. The coefficients of determination showed that the proportions of variances of the LOS that can be explained by clinical factors as 0.1 %; 1.2 %; 3.4 %; and 5.3% for clinical outcomes, nursing teams, diagnoses, and PCUA, respectively (Table 2). Those proportions are higher than those observed with SDF. Except for patient clinical outcome and nursing team, our main explanatory factor, the diagnosis has been consistently related to the LOS.
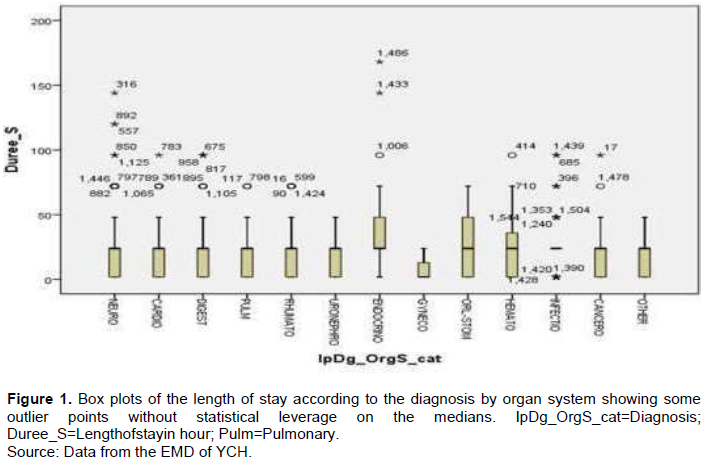
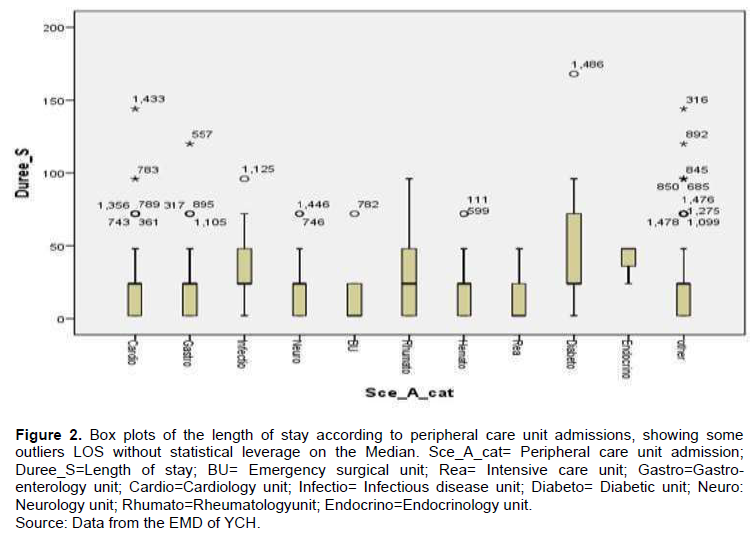
Furthermore, the findings of Figure 1 showed many outlier points above the median LOS. It was found out that a patient ranked number 1486th had spent 168 hour in the ER, representing a stay of one week, suffering from an endocrinology condition, and was later on transferred to the diabetic care unit (Figure 2). It could be assumed that the number 1486th might have suffered from a severe decompensation of diabetes, could neither leave the ER sooner, nor pay four hundred dollars, a preexisting condition for admission to the intensive care unit. On the other hand, the 1433 and 316th patients suffering from an endocrinology and neurology conditions, respectively, each of them had spent 144 h, representing six days before the former (1433th) went to the cardiology unit, and the latter (316th) left the ER without physician approval or LWBS. We could assume that a lack of beds in the neurology care unit forced 1433th patient for admission into the cardiology care unit, which was inappropriate for this patient, whereas 316th patient left without physician approval probably because of financial hardships.
Are there any confounding/interaction factors in the relationship between LOS and diagnosis?
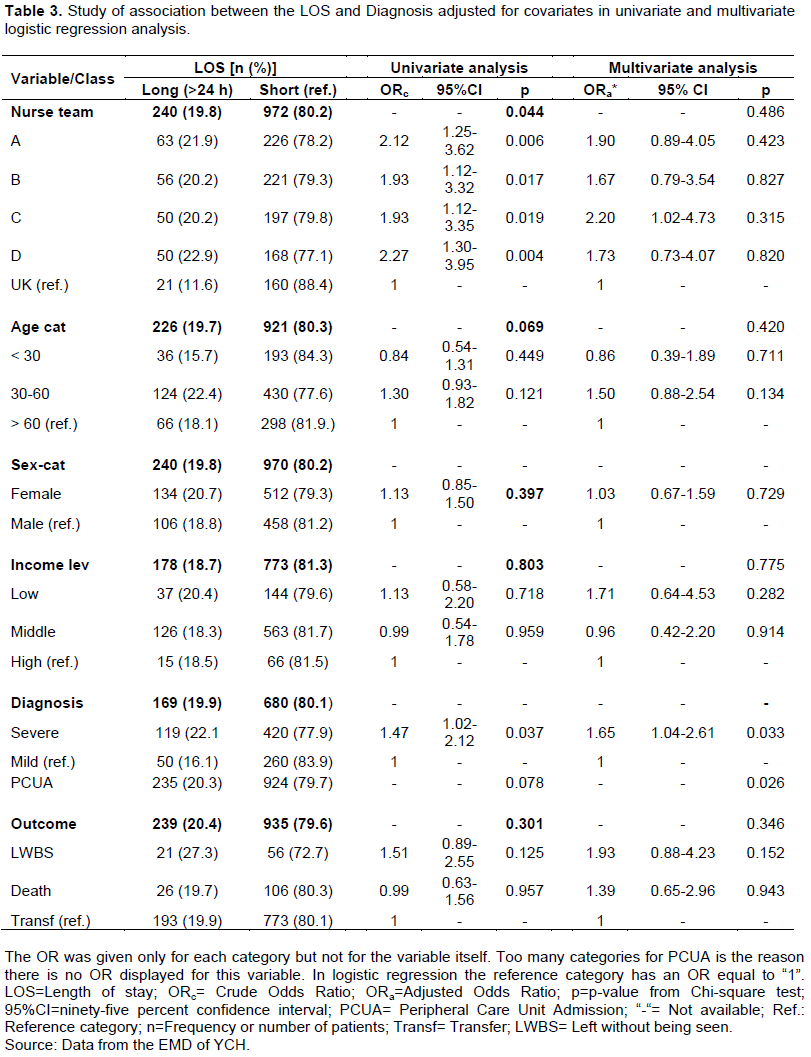
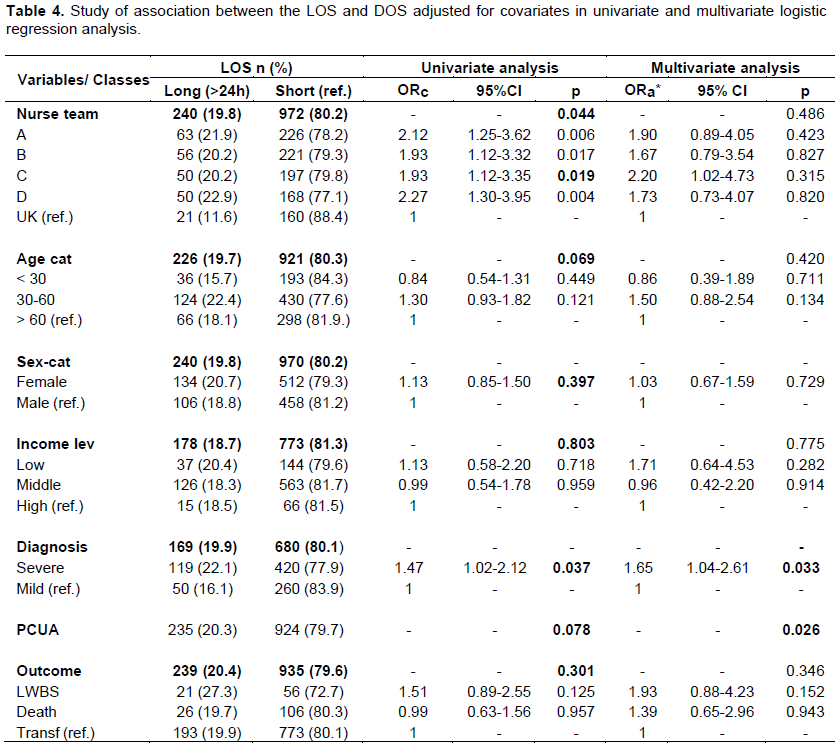
A binomial logistic regression modeling was conducted to assess the effect size of this association, potential confounding and interaction factors (Table 4). In univariate analysis, only the variables nursing team and diagnosis severity were statistically significant, p=0.044, 0.037 respectively; while age and PCUA were marginally significant, p=0.069, 0.078 respectively, associated with the increased stay in the ER. In multivariate analysis, the age factor has lost its marginal association (p=0.069; 0.420), the PCUA however, showed significant statistical association with a long stay (p=0.078; 0.026). Also, the effect size of the association between diagnosis severity and increased LOS shows more than 10% change in the crude ORc=1.47 and adjusted ORa=1.67; suggesting that the PCUA could be a potential confounding factor. These results suggested that the mean LOS varying from one diagnostic class to another, with patients who suffered from endocrinologic and neurologic conditions having the longest stay. In addition, there was no evidence of association between SDF and LOS.
DISCUSSION
The LOS is four-time longer in the ER of YCH compared to international standards where the median LOS varies between 2 and 6 h (Sorup et al., 2013; Kusumawati et al., 2019). Meeting international standards can be daunting for some ER of many some low-and-middle income countries. Like Yaoundé Central Hospital, findings from another study conducted in southern Ethiopia had shown an increased time spent in ER, Our results showed the mean LOS varying from one diagnostic class to another; findings that are consistent with what Nanayakkara et al. (2014) and Sorup et al. (2013) had reported in Australia and Denmark, respectively. Conversely, PCUA was found to be the only possible confounding factor in the relationship between diagnostic severity and a long stay in the ER of YCH. More often, patients got stuck in the ER for lack of beds in the peripheral care unit. The so-called “Hebergement” or temporary housing is a common procedure where the patients are transferred to an unfitted peripheral care unit to wait for admission as a bed becomes available in the qualified peripheral care unit(https://www.indexmundi.com/cameroon/hospital_bed_density.html). We were unable to find an evidence of association between SDF and LOS. Rose et al. (2016), also reported the absence of direct impact of SDF on the patient’s LOS. As an LMIC, Cameroon has not yet implemented universal health coverage, we thought income levels could have a tremendous impact on the patient’s LOS in the ER of YCH; surprisingly, like the gender and age factors, it was not the case in this study.
In the present study, we find the diagnostic severity; bed unavailability in peripheral care units and for some extends a poor financial capacity to be linked with the long stay in the ER of Yaoundé central hospital.
Study advantages and relevance
This study sheds light on the performance of an EMD by providing concrete evidence-based information on various factors that may help to predict the LOS in the ER of a healthcare facility in a LMIC. The results could lead to decision-making capacity in the sense that enhances patient quality of care. Accounting for a few published studies in the field of EMD in LMIC, this pioneering work could pave the way for further researches especially in Cameroon. Although we could not assess the impact of health insurance on the patient’s average LOS in the ER was to raise awareness on the main urgency of the moment in healthcare, which is the necessity for implementing universal health coverage in LMIC like Cameroon.
Study limitations
The patient’s LOS could have been misestimated in our study. The lack of data on the time the patient was admitted and discharged (Cameron et al., 2011; Sorup et al., 2013; Rose et al., 2016) constrained us to assign a default stay of 24 h to any patient who was discharged the next day, if admitted the day before. However, some of those patients could have been admitted in the evening and discharged the next morning, leading to a short stay.
Furthermore, the lack of data on the patient’s capacity to pay for health related bills rendered difficult to assess the impact of the healthcare expenses on the LOS. The results showed that only 2.4% of patients were admitted in the Intensive care unit (ICU), compared to 17.6% and 11.2% for gastroenterology and cardiology units, respectively. At Yaoundé central hospital, while the admission in peripheral care units like cardiology and gastroenterology is free of charge, a down-payment of about four hundred dollars is required for admission in the ICU, a preexisting condition that too many patients could not afford. As a result, the lack of financial resources might have deterred the access of many severe health conditions to the ICU and reciprocally extended their stay in the ER; an assumption that could support a dire need of Universal Health Coverage (World Health Organization, 2017).
Finally, information bias could have occurred during the process of categorizing patient’s income levels. The students were classified as lower income however, their parents who may be wealthier are the ones paying the student’s healthcare bills. The same reasoning applies for the housewife status, considered as middle income patients in this study, when their partners could have been classified as either lower, middle or higher income. Thus, the likelihood that a differential misclassification occurred is higher in this study, a bias that could have led to a diluted estimate of the effect size, shifting the association between the LOS and family income towards the null.
CONCLUSIONS
Although some biases have been highlighted, this pioneering study in Cameroon provides evidence-based information on factors associated with the increased length of stay in the ER of Yaoundé Central Hospital. When compared with study conducted in other parts of the world, there is a broad number of factors that varies from one country to another. These factors such as diagnostic severity, bed unavailability in peripheral care units, lack of diagnostic and therapeutic capability, and poor financial capacity can substantially increase the mean length of stay in the ER of a Low and middle income country. In the ER of YCH diagnostic severity was strongly associated with increased length of stay in the emergency room and the bed unavailability in peripheral care units played a confounding role in that relationship. In addition, less than 1% of the change that occurred in the mean LOS was explained by socio-demographic factors; while only about 6% of that change accounted for clinical factors. These findings provide a rationale for conducting new study designs that would assess other structural and procedural factors, including the impact of universal health coverage on the remaining 93% unexplained change of the mean LOS in ER of Yaoundé Central Hospital (Liu et al., 2013; Hung and Chalut, 2008; World Health Organization, 2017).
ETHICAL CONSIDERATIONS
The Director of Yaoundé Central Hospital granted a written contract N°088/DHCY/CM/CG, for this study. In order to prevent the leak of patient information from occur occurring, each patient identifier was matched to a numeric code and kept secret. The principal investigator claims to be an external, independent evaluator who was neither closely nor furtherly associated to the management of clinical or administrative affairs of the Yaoundé Central Hospital.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGMENTS
The authors would like to express their sincere gratitude to the Director of Yaoundé Central Hospital who gave his approval to this research, to the ER staff who collected and provided the database used in the research, and to the reviewers who took the time to make this work near perfect, we do appreciate your expertise and good will; thank you all, so much.
REFERENCES
|
Alemu GH, Negari KG, Rodamo, KM (2019). Factors associated with the length of stay in emergency departments in Southern-Ethiopia. BMC Research Notes 12(1):239. |
|
|
Cameron PA, Schull MJ, Cooke MW (2011).A framework for measuring quality in the emergency department. Emergency Medicine Journal 28:735-740. |
|
|
Chamberlain JM, Pollack MM (1998). A method for assessing emergency department performance using patient outcomes. Academic Emergency Medicine 5(10):986-991. |
|
|
Garga H, Ongolo-Zogo P. Améliorer l'accueil et la prise en charge des urgences dans les hôpitaux nationaux et régionaux au Cameroun. Note d'Information Stratégique SURE¬¬. Yaoundé, Cameroon: CDBPS, 2013. |
|
|
Greg MD, Pratt D, Glickman SW, Brice JH, Glickman LT, Cabañas JG, Cairns CB (2010). The North Carolina EMS Data System: A comprehensive integrated emergency medical services quality improvement program. Prehospital Emergency Care 14(1):85-94. |
|
|
Hung GR, Chalut D (2008). A consensus-established set of important indicators of pediatric emergency department performance. Pediatric Emergency Care 24(1):9-15. |
|
|
Kusumawati HI, Magarey J, Rasmussen P (2019). Analysis of factors influencing length of stay in the Emergency Department in public hospital, Yogyakarta, Indonesia. Australasian Emergency Care 22(3):174-179. |
|
|
Liu K, Jain S, Shi J (2013).Physician performance assessment using a composite quality index. Statistics in Medicine 32(15):2661-2680. |
|
|
MacFarlane C, Benn CA (2003). Evaluation of emergency medical services systems: a classification to assist in determination of indicators. Emergency Medicine Journal 20(2):188-191. |
|
|
Nanayakkara S, Weiss H, Bailey M, van Lint A, Cameron P, Pilcher D (2014). Admission time to hospital: A varying standard for a critical definition for admissions to an intensive care unit from the emergency department. Australian Health Review 38(5):575-579. |
|
|
Rahman NH, Tanaka H, Do Shin S, Ng YY, Piyasuwankul T, Lin CH, Ong MEH (2015). Emergency medical services key performance measurement in Asian cities. International Journal of Emergency Medicine 8(1):1-6. |
|
|
Rose L, Scales DC, Atzema C, Burns KE, Gray S, Doing C, Lee JS (2016). Emergency department length of stay for critical care admissions. A population-based study. Annals of the American Thoracic Society 13(8):1324-1332. |
|
|
Schroeder LL, Alpern ER, Blecher SM, Peska PA, White ML, Shaw JA, Alessandrini EA (2016). Assessing Structural Quality Elements of Pediatric Emergency Care. Pediatric Emergency Care 32(2):63-68. |
|
|
Sorup CM, Jacobsen P, Forberg JL (2013).Evaluation of emergency department performance-A systematic review on recommended performance and quality-in-care measures. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine 21(1):1-14. |
|
|
World Health Organization: Speech from the Director-General, July 17, 2017. |
|
|
Yaoundé Central Hospital website. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


