Full Length Research Paper
ABSTRACT
This study sought to determine the epidemiology of COVID-19 in Trinidad and Tobago by the socio-demographic and clinical characterization and comparison of local and imported cases. There have been limited prior studies on COVID-19 in the Caribbean. As such, this paper attempts to discuss the patterns associated with COVID-19 patients in this Caribbean territory. A retrospective study of 113 patients with confirmed SARS-CoV-2 infection managed at Arima General Hospital and Couva Medical and Multi-Training Facility in Trinidad and Tobago from March 12th, 2020 to April 12th, 2020 was performed. Clinical data, epidemiological characteristics, demographics and clinical symptomology were recorded. Microsoft Excel and SPSS 22.0 were used for statistical analysis. Most patients were females (61.9%) while 38.0% were males. Most patients were between 45 to 64 years of age (43.4%) followed by those >65 years of age (28.8%). Cough was the most common presenting complaint (44.9%), followed by fever (37.1%). Most participants with a travel history were female (F: 61.9%; M: 38%). The occurrence of cough was high among both local cases (46.4%) and imported cases (47.6%). These patterns can inform clinicians and other healthcare workers on the unique findings associated with COVID-19 positive patients, especially those in the Caribbean region.
Key words: COVID-19, SARS-CoV-2, epidemiology, Trinidad and Tobago, Caribbean Region.
INTRODUCTION
Coronavirus disease 2019 (COVID-19) infection is caused by a beta coronavirus known as severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and is currently a pandemic (Zhu et al., 2020). The first known reporting of COVID-19 was in the South China Seafood market (Lake, 2020; Li et al., 2020; Yaqian et al., 2020). The market has a variety of live and freshly slaughtered animals (Li et al., 2020). Evidence has suggested animal to human transmission involving animals such as the Chinese Cobra, horseshoe bats, and pangolin (Lake, 2020; Yaqian et al., 2020). However, overwhelming evidence, including gene sequencing analysis, supports t ransmission from bats to humans, with the Sprotein nucleotide sequence showing >80% homology with bat-SL-CoVZC45 (Yaqian et al., 2020; Zhang et al., 2020).
The COVID-19 infection is characterized by its rapid spread. By the time of the first report, on December 31st, 2019 in Wuhan, SARS-CoV-2 had already spread to 58 Chinese provinces and more than 25 countries. The number of cases reported by March 2020 was 105,586 (Li et al., 2020, Yaqian et al., 2020; Zhang et al., 2020). Human-to-human transmission and contact transmission facilitated the rapid spread of the infections (Khan et al., 2020). Transmission through the gastrointestinal route is also possible since SARS-CoV-2 has been isolated in stool samples (Yaqian et al., 2020; Yuan et al., 2020). Evidence shows that while respiratory tract infection samples may return negative, stool samples may yield positive results (Yuan et al., 2020). Mother-to-child transmission through breast milk is yet to be established (Yaqian et al., 2020).
Global spread of the virus is also attributed to increased travel (Khan et al., 2020; Guan et al., 2020; Siordia, 2020; Pung et al., 2020; Yang et al., 2020). Given that the mean serial interval for the virus infection is between three to eight days, the infection can be transmitted even before the onset of symptoms (Pung et al., 2020; He et al., 2020). Some of the clinical indicators are fever, cough, chest tightness, and dyspnea (Lake, 2020). However, Han et al. (2020) noted that the age of the patient influences the clinical symptoms associated with COVID-19 (Han et al., 2020). It should also be noted that close to half (44%) of the disease transmission is through infected but asymptomatic individuals (He et al., 2020).
Gender is thought to be a risk factor with various studies reporting the number of male patients compared to female patients (Cai, 2020; Wenham et al., 2020). Chen et al. (2020) reported that among 99 confirmed cases of COVID-19, 67 were men while 32 were women (Chen et al., 2020). Evidence also shows that more men are dying due to the infection (Wenham et al., 2020). However, Wenham et al. (2020) also noted that there is a need for further assessment of sex-disaggregated infection rates (Wenham et al., 2020). The twin island Republic of Trinidad and Tobago has an estimated population of 1.4 million (Central Statistical Office, 2019). The country reported its first case of SARS-CoV-2 on March 12, 2020 (Ministry of Health, Trinidad and Tobago, 2020). Since then, public health measures such as border closures, social distancing, and mask-wearing have been implemented to limit the spread of the virus (Government of the Republic of Trinidad and Tobago Ministry of Health, 2022). A parallel healthcare system, independent of the regular public healthcare system, was established to manage and treat exclusively COVID-19 patients in both islands. Patient screening before entry into healthcare facilities aided in identifying suspected COVID-19 patients, who were subsequently isolated, diagnosed and treated via the parallel system (Hunte et al., 2020). There have been limited prior studies on COVID-19 cases in the Caribbean. As such, this paper attempts to discuss the patterns associated with the first group of COVID-19 patients in this Caribbean territory. This study was carried out with the aim to assess and compare the demographic factors, comorbidities, and symptoms associated with COVID-19, for imported and local cases managed at two COVID-19 facilities in the parallel healthcare system of Trinidad and Tobago for the period March 12th, 2020 to April 12th, 2020.
MATERIALS AND METHODS
For this retrospective study, a judgment sampling technique was employed in collecting data from 113 patients with confirmed SARS-CoV-2 infection, managed at the Arima General Hospital and the Couva Medical and Multi-training Facility in Trinidad and Tobago, from March 12th, 2020 to April 12th, 2020, were analyzed. Cases were confirmed by an accredited laboratory utilizing real-time reverse transcription polymerase chain reaction assay (RT-PCR). The medical records departments of the facilities were engaged and asked to populate a Microsoft Excel sheet with the variables of interest for patients who met the inclusion criteria of the study. These variables included clinical data (comorbidities, symptomology), epidemiological characteristics, and patient demographics. The study included only patients who were confirmed COVID-19 positive via RT-PCR and were subsequently admitted to the two facilities. Patients were excluded if they were admitted to the facility as ‘suspected’ COVID-19 patients that is, with pending RT-PCR results during the study period. The study was approved by the Ministry of Health of Trinidad and Tobago Ethic Committee (3/13/441 Vol. II), and the North Central Regional Health Authority Ethics Committee, Trinidad. As only de-identified data were collected, participant informed consent was waived by the ethics committees.
Case definition
A confirmed case was defined as a case with a positive result using RT-PCR assay. Imported cases were defined as cases that came into the country, that is, a patient had a travel history and tested positive via RT-PCR. Local cases were defined as patients who tested positive via RT-PCR without a travel history but had possible contact with another positive COVID-19 patient.
Statistical analysis
All statistical analysis was processed using IBM SPSS 22.0 statistical software. Student t test or Wilcoxon test were applied to continuous variables. Chi Square was incorporated for analysis or comparison of categorical data, where p< 0.05 was considered statistically significant. Variables were expressed as means, standard deviation or median. Percentages were provided for categorical data.
Logistic regression was used to assess the effect of gender and age on the likelihood of having HTN and DM. Another regression assessed the effect of gender, age, and major comorbidities (DM and HTN) on the likelihood of being asymptomatic with COVID-19.
RESULTS
Baseline characteristics
The majority of the participants were female 70 (61.9%) whereas only 43 (38.0%) were male. 43.4% of the population were between 45 -64 (43.4%), followed by above 65 at 28.8%. The average age of the population was 54.6 years. Table 1 shows that Coughing was the most popular presenting complaint at 44.9% with fever being second at 37.1%. Most participants with a travel history were female (F: 61.9%; M: 38.0%). Of participants with no travel history, 62.0% were female and 37.9% were male.
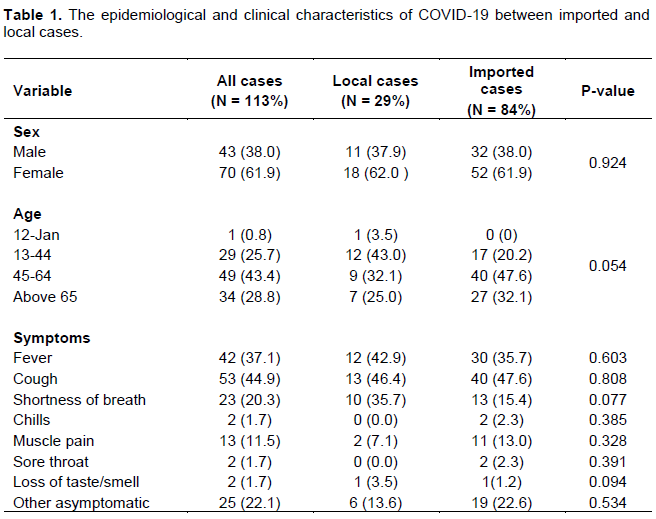
Most local cases (43.0%) were patients aged between 13 and 44 years. Patients with imported cases were mainly between 45 to 64 years (47.6%). Those aged above 65 years comprised 32.1% of the imported cases, which was the second highest. Chi-square showed that age variation between local and imported cases was statistically significant (p= 0.05). Symptoms varied between the local and imported cases, however, there was no statistically significant difference in the reported symptoms between the two categories of cases. The occurrence of cough was high among both the local cases (46.4%) and imported cases (47.6%) Fever was the second most common symptom among both groups, with local cases at 46.4% and imported cases at 35.7%. The frequency of asymptomatic individuals was 22.1% in all cases, with 13.6% among local cases and 22.6% among imported cases (see Table 1).
Comorbidities
Data on comorbidities of COVID-19 was obtained from all the participants (n= 113). As shown in Figure 1, the comorbidity with the highest frequency was hypertension (HTN), which was reported among 68.4% of the patients. Figure 1 also shows that diabetes mellitus (DM) was the second most frequently reported comorbidity (28.2%). The other common comorbidities included asthma (6.2%), Gastroesophageal Reflux Disease (4.4%), and glaucoma (4.4%).
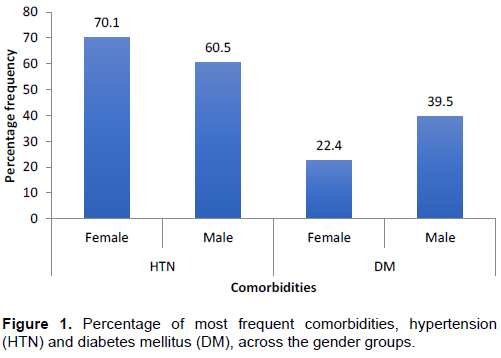
In this study, the Chi-square of association analysis was carried out to determine the association between gender and the two most frequent comorbidities (hypertension and DM). Table 2 shows that the percentage of female patients with hypertension (70.1%) was higher compared to that of male patients (60.5%). However, Chi-square analysis showed that there was no significant association between gender and percentage of hypertension across the gender groups of patients with COVID-19 (χ2(1) = 1.100, p = 0.294). For DM, the percentage was higher among male patients (39.5%). However, Chi-square analysis showed that there was no significant association between gender and DM between male and female patients with COVID-19 (χ2 (1) = 3.733, p = 0.053).
Clinical symptoms
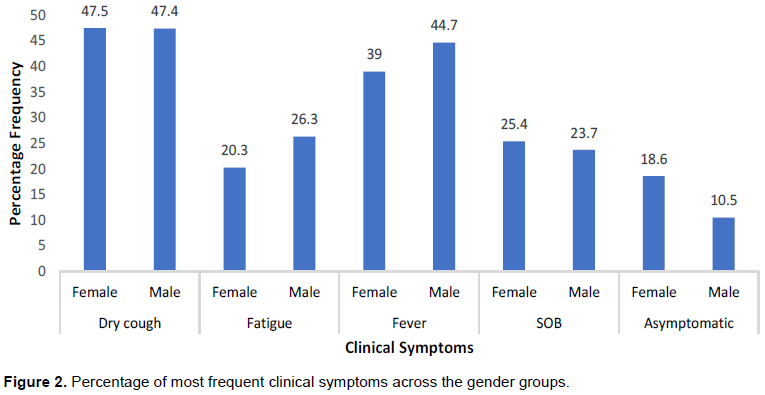
Chi-square of association analysis was carried out to determine the association between gender and four of the most frequently reported symptoms (dry cough, fatigue, fever, and shortness of breath/SOB) and lack of clinical symptoms. There were no significant differences in the frequencies of any symptoms or asymptomatic infection between the genders.
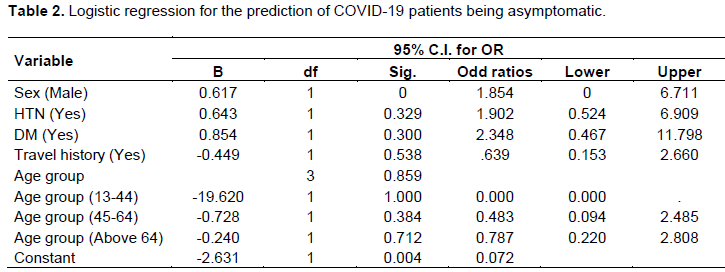
Logistic regression was carried out to assess the effect of major comorbidities (DM and HTN), gender and age on the likelihood of patients with COVID-19 being asymptomatic. The developed regression model for the likelihood of the patients being asymptomatic (χ2(7) = 4.72, p= 0.694) were not statistically significant. As shown in Table 2, none of the predictor variables were statistically significant in predicting the likelihood of the patients being asymptomatic.
DISCUSSION
This study indicates that infection occurs across the different age groups, but the average age of the patients is 54.6 years. The observed number of cases of infection among individuals as young as nine years is consistent with the findings of recent studies on COVID-19 infection that caution against the ill-informed assumption that the disease only targets the elderly (Liu et al., 2020). The average age of 54.6 years is within the range of mean ages of infected patients as reported by previous researchers (Chen et al., 2020). This, therefore, means that although the disease infects people across all the age groups, most of the infections are among the adults (Siordia, 2020). However, unlike the findings of most studies, this research noted that the frequency of infection among females is higher than males (Cai, 2020; Wenham et al., 2020). The observed disparity could however be due to the unique factors attributed to the study population such as age, gender, and existing comorbidities.
This study also noted that there are various comorbidities associated with COVID-19. Hypertension and Diabetes Mellitus were, however, noted to be the most frequently reported comorbidities, which corroborates with previous evidence. 30.7% of the patients in Wuhan China were reported by Siordia (2020) to have these comorbidities. The other common comorbidities included diabetes and heart diseases (Guan et al., 2020; Siordia, 2020).
Concerning the clinical symptoms, the observed high frequency of dry coughs and fever among COVID-19 patients support the existing studies (Lake, 2020; Yaqian et al., 2020; Chen et al., 2020). Previous findings that support the obtained outcome indicate that the frequently reported symptoms include fever, coughs, chest tightness, and dyspnea (Lake, 2020). COVID-19 patients have also been reported to suffer pneumonia, which sometimes is accompanied by coughs and fatigue Lake, 2020; Yaqian et al., 2020; Chen et al., 2020). Chen et al. (2020) noted that patients also have trouble breathing, muscle ache, chest pains, and vomiting (Siordia, 2020) which were also seen to a lesser extent in this study. The observed wide range of clinical symptoms support the conclusions made by Chen et al. (2020) which noted that coronaviruses can result in multiple system infection and that clinical features associated with COVID-19 infection vary greatly. This study also reaffirms the conclusions made by previous researchers concerning the fact that individuals infected with COVID-19 can be asymptomatic (Pung et al., 2020; He et al., 2020). However, unlike the findings by He et al. (2020) that reported close to half (44%) asymptomatic cases, this study noted that asymptomatic cases ranged between 18.6% for females and 10.5% for males (Figure 2). Both local and imported cases presented with a cough which was consistent with the findings by Chen et al. (2020) who also concluded that local cases from Wuhan presented with a cough as opposed to fever (Chen et al., 2020).
There are various limitations that need to be taken into account when interpreting the findings of this study. As mentioned above, the sample used in this study did not have an equal number of male and female patients, which limited the assessment of the effect of gender on comorbidities and symptoms. Despite the highlighted limitation, the obtained findings give important insights into the epidemiology of COVID-19 patients in the Caribbean. The study raises questions over the distribution of the infections across the gender groups, which needs to be further analyzed by future researchers. The study also singles out individuals who have hypertension and DM to be at the highest risk for COVID-19 infection. The disease prevention strategies should, therefore, focus on limiting the exposure of the identified groups to the disease as well as focus on other public health measures which include containment of positive patients, social distancing, proper hand hygiene and the use of face masks (Chen et al., 2020; Gao, 2020; Kim et al., 2020). Based on the obtained outcome, there is a need to identify dry cough and fever as the main symptoms in the identification of patients infected with COVID-19.
CONCLUSION
In this study, the average age of the patients is 54.6 years. Dry coughs and fever are the most common symptoms among COVID-19 patients while hypertension and DM are the most frequently reported comorbidities. Based on this study, individuals with hypertension and DM should be considered a high-risk group, and strategies should be put in place to limit their exposure to this virus. The study also concludes that dry cough and fever should be considered as the main symptoms used in the identification of patients infected with COVID-19.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGMENTS
The authors have not received any funding or benefits from industry or elsewhere to conduct this study.
The authors thank Professor Hariharan Seetharaman and Dr. Malachy Ojuro for their assistance during the early part of the study, and the North Central Regional Health Authority for making files accessible for preparation of this review.
REFERENCES
|
Cai H (2020). Sex difference and smoking predisposition in patients with COVID-19. The Lancet Respiratory Medicine 8(4):e20. |
|
|
Central Statistical Office (2019). Provisional mid year population estimate by age and sex, 2005-2021. |
|
|
Chen N, Zhou M, Dong X, Qu J, Gong F, Han Y, Zhang L (2020). Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. The Lancet 395(10223):507-513. |
|
|
Gao ZC (2020). Efficient management of novel coronavirus pneumonia by efficient prevention and control in scientific manner. Zhonghua jie he he hu xi za zhi= Zhonghua jiehe he huxi zazhi= Chinese journal of tuberculosis and respiratory diseases 43:E001-E001. |
|
|
Government of the Republic of Trinidad and Tobago Ministry of Health (2022). COVID-19 novel coronavirus. |
|
|
Guan WJ, Ni ZY, Hu Y, Liang WH, Ou CQ, He JX, Zhong NS (2020). Clinical characteristics of 2019 novel coronavirus infection in China. MedRxiv. |
|
|
Han YN, Feng ZW, Sun LN, Ren XX, Wang H, Xue YM, Fang Y (2020). A comparative?descriptive analysis of clinical characteristics in 2019?coronavirus?infected children and adults. Journal of Medical Virology 92(9):1596-1602. |
|
|
He X, Lau EH, Wu P, Deng X, Wang J, Hao X, Leung GM (2020). Temporal dynamics in viral shedding and transmissibility of COVID-19. Nature Medicine 26(5):672-675. |
|
|
Hunte SA, Pierre K, Rose RS, Simeon DT (2020). Health systems' resilience: COVID-19 response in Trinidad and Tobago. The American Journal of Tropical Medicine and Hygiene 103(2):590. |
|
|
Khan S, Siddique R, Ali A, Bai Q, Li Z, Li H, Nabi G (2020). The spread of novel coronavirus has created an alarming situation worldwide. Journal of Infection and Public Health 13(4):469. |
|
|
Kim JY, Choe PG, Oh Y, Oh KJ, Kim J, Park SJ, Oh MD (2020). The first case of 2019 novel coronavirus pneumonia imported into Korea from Wuhan, China: implication for infection prevention and control measures. Journal of Korean Medical Science 35(5). |
|
|
Lake MA (2020) What we know so far: COVID-19 current clinical knowledge and research. Clinical Medicine 20(2):124-127. |
|
|
Li R, Pei S, Chen B, Song Y, Zhang T, Yang W, Shaman J. (2020). Substantial undocumented infection facilitates the rapid dissemination of novel coronavirus (SARS-CoV-2). Science 368(6490):489-493. |
|
|
Liu W, Zhang Q I, Chen J, Xiang R, Song H, Shu S, Liu Y (2020). Detection of Covid-19 in children in early January 2020 in Wuhan, China. New England Journal of Medicine 382(14):1370-1371. |
|
|
Ministry of Health, Trinidad and Tobago (2020). Statement from the honourable Terence Deyalsingh, Minister of Health at the media conference to advise of the first confirmed (imported) case of COVID-19 in Trinidad and Tobago. |
|
|
Pung R, Chiew CJ, Young BE, Chin S, Chen MI, Clapham HE, Ang LW (2020). Investigation of three clusters of COVID-19 in Singapore: implications for surveillance and response measures. The Lancet 395(10229)1039-1046. |
|
|
Siordia Jr JA. (2020). Epidemiology and clinical features of COVID-19: A review of current literature. Journal of Clinical Virology 127:104357. |
|
|
Wenham C, Smith J, Morgan R (2020). COVID-19: the gendered impacts of the outbreak. The Lancet 395(10227):846-848. |
|
|
Yang X, Yu Y, Xu J, Shu H, Liu H, Wu Y, Shang Y (2020). Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: a single-centered, retrospective, observational study. The Lancet Respiratory Medicine 8(5):475-481. |
|
|
Yaqian M, Lin W, Wen J, Chen G (2020) Clinical and pathological characteristics of 2019 novel coronavirus disease (COVID-19): a systematic review. medRxiv 2020.02.20.20025601. |
|
|
Yuan H, Cao X, Ji X, Du F, Zhou X, He J, Zhu Y. (2020). A current emerging respiratory infection: epidemiological and clinical characteristics, diagnosis and treatments of COVID-19. Diagnosis and Treatments of COVID-19 (3/6/2020). |
|
|
Zhang JJ, Dong X, Cao YY, Yuan YD, Yang YB, Yan YQ, Gao YD. (2020). Clinical characteristics of 140 patients infected with SARS?CoV?2 in Wuhan, China. Allergy 75(7):1730-1741. |
|
|
Zhu N, Zhang D, Wang W, Li X, Yang B, Song J, Tan W (2020). A novel coronavirus from patients with pneumonia in China, 2019. New England Journal of Medicine 382(8):727-33. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


