Full Length Research Paper

ABSTRACT
Sex is a significant prognostic factor in the survival of pediatric acute lymphoblastic leukemia (ALL) with girls having superior outcome. This phenomenon could be partly due to the intrinsic relationship between sex and other prognostic factors. The present study aimed to assess the effect of sex on ALL survival after accounting for interactions of sex with age at diagnosis and radiation, in addition to known prognostic factors. We utilized 1973 to 2009 surveillance epidemiology and end results data. In a multivariable Cox proportional hazard model, stratified by the year of diagnosis, the prognostic value of sex diminished (adjusted hazard ratio (AHR) = 1.21, 95% confidence interval (CI): 0.93, 1.57). The difference in mortality between girls and boys was the lowest in the irradiated children diagnosed between ages 10 and 19 years. In this subgroup, boys’ risk of mortality was not substantially different from that of girls (AHR = 0.96, 95% CI: 0.70, 1.33). In the large population based study, after accounting for the aforementioned interaction effects, the prognostic value of sex in ALL survival diminished, and it is eliminated in the irradiated children diagnosed between ages 10 to 19 years.
Key words: Sex, lymphoblastic leukemia, prognostic factors.
INTRODUCTION
Sex has consistently been shown to be associated with the prognosis and survival in pediatric acute lymphoblastic leukemia (ALL) (Carroll et al., 2003; Sather et al., 1981). Girls have a superior event-free survival compared to boys given equivalent therapy, whereas boys are at higher risk for genetic predispositions to ALL and treatment-related adverse events (Chessells et al., 1995; Dordelmann et al., 1999; Lanning et al., 1992; Nachman et al., 1998; Smith et al., 1996). Other clinical features that have been identified as having prognostic values include age at diagnosis, race, immunophenotype, chromosomal abnormalities and the number of primary tumor sites (Carroll et al., 2003; Hilden et al., 1995; Pui et al., 1994; Reaman et al., 1999; Rubnitz et al., 1997). Although pediatric ALL survival dramatically improved over the years because of advancements in early detection and treatment protocol, the survival difference by sex persists (Möricke et al., 2005; Reaman et al., 1985; Sather, 1986). This phenomenon could be due to the intrinsic relationship between sex and other prognostic prognostic factors. It has been reported that the proportion of boys diagnosed later in childhood is higher than that of girls, while increased age at diagnosis is associated with increased risk of mortality, and T-cell ALL, which has worse prognosis than B-cell ALL, occurs more commonly in boys, and those with T-cell ALL undergo more intensified therapies; on the other hand, the magnitude of the difference in ALL survival by sex is less apparent in recent studies with intensified therapy (Carroll et al., 2003; Möricke et al., 2008; Pui et al., 2009; Silverman et al., 2001).
Research on the relationship between the prognostic factors and their associations with pediatric ALL survival has been scanty, especially in the changing ALL survival and treatment protocols. The five-year survival rate of pediatric ALL patient was 43.2% in 1975 and 87% in 2005, and it has been found that many conventional risk factors have lost predictive strength (Pui, 1997). In this study, we sought to assess the extent of the association of sex and the survival patterns of pediatric ALL patients in the US, using the surveillance epidemiology and end result (SEER) data set from 1973 to 2009 after accounting for age at diagnosis, race, primary tumor sites, ALL immunophenotype, radiation therapy and interactions of sex with age at diagnosis and radiation therapy. In addition, we evaluated the impact of sex on the survival of irradiated ALL patients diagnosed between ages 10 to 19 years. The SEER program of the National Cancer Institute (NCI) is the most comprehensive and reliable source of population-based information in the United States on cancer incidence and survival (Ries et al., 1999). The SEER dataset is large and well representative to ALL patients in the US which is ideal for epidemiological investigation like ours. The patients were diagnosed during 1973 to 2009. Patients diagnosed in 1973 have as long as 37 years of follow-up time, while those diagnosed later had shorter periods of follow-up. In short, the survival patterns of pediatric ALL patients in the SEER dataset are not constant over the follow-up period. To account for this time-varying survival pattern, we stratified the analysis by the year of the diagnosis grouped into 5-year intervals.
MATERIALS AND METHODS
The study included 14192 children who were diagnosed with ALL between ages 0 to 19 years during 1973 to 2009, whose information was reported to one of the 17 SEER registries. The SEER data are estimated to represent 28% of the US population (Howlader et al., 2013; Ries et al., 1999). The SEER registries collect population data on age, sex, race, year of diagnosis, primary tumor sites, tumor morphology and follow-up for vital status (Howlader et al., 2013; Ries et al., 1999). The subgroup analysis included only children who were diagnosed between 10 and 19 years and received the radiation therapy. The data sets were accessed upon the approval of the SEER Data Access Agreement. The data were used only for the research purpose. All results were presented in a way that no individual could be identified. The study variables are described in brief.
Age at diagnosis
The SEER data included a variable of age at diagnosis recoded as < 1, 1 to 4, 5 to 9, 10 to 14 and 15 to 19 years. This age classification is representative of age based pediatric ALL risk groupings used in most studies and was adopted for the purpose of this paper.
Year of diagnosis
The study covered ALL patients diagnosed between 1973 and 2009. This variable was recorded in single-year interval. We recoded this variable into five-year intervals (1973 to 1977, 1978 to 1982, 1983 to 1987, 1988 to 1992, 1993 to 1997, 1998 to 2002, 2003 to 2007, 2008 to 2009). The interval 2008 to 2009 contains only two years. The maximum follow-up period of this study is 37 years.
Sex
Sex was a nominal variable in the SEER dataset and used as a binary variable with female as the reference group.
Race
In the SEER dataset, the variable race contained information of white, black, Asian/Pacific Islander and others or unknown. Because of the limited number of subjects, we did not include the later two categories in the analysis. We regrouped this variable as Caucasian (White), African American (Black) and Others/unknown (Asian/Pacific Islander, Others or Unknowns). African American (AA) was set as the reference group in our analyses.
Number of primary tumor sites
The minimum number of primary tumor site was 1 in the SEER data, while the maximum number was 3. In our preliminary ex-ploration, we found 1.1% of patients with 2 primary sites and 0.1% with 3 primary tumor sites. Hence, we collapsed the variable into two categories: one primary and two or more primary sites. Patients with one primary tumor site were selected as the reference group.
ALL immunophenotype
The information on the ALL immunologic features was available in the SEER dataset. We used two distinct immunophenotypes: T-cell and B-cell/B-precursor. This variable was treated as binary, with the T-cell as the reference group.
Radiation therapy
Information of radiation therapy was listed as (a) Beam radiation, (b) combination of beam radiation with implant or isotopes, (c) none, (d) radiation, NOS, (e) recommended, (f) refused, and (g) unknown in the SEER dataset. The variable was dichotomized into “yes, had radiation therapy of any kind” versus “no, never had radiation therapy during the time of data collection”.
Follow-up time and survival status
The follow-up time was documented as the duration from the time of diagnosis to death from any cause or the last day of the available survival information in the SEER registry. In the dataset, those who did not experience the event (death) during the follow-up time were censored. The survival status was determined on a binary scale, with 0 for censored and 1 for the event or failure.
Statistical analyses
Clinical features of ALL patients were summarized by sex. Categorical variables were described using frequencies and percentages, while continuous variables were summarized using medians, 75% percentiles, means and standard errors (SE). Pearson’s ?2statistic was used to examine the distribution of clinical features of ALL patients by sex. Five- and ten-year survival rates were calculated for boys and girls. The distribution of mortality was presented by sex, age at diagnosis, and the receipt of radiation. A univariable Cox proportional hazard model was performed to assess the effect of individual study variables. We utilized a multivariable Cox proportional hazard model, stratified by the year of diagnosis, to assess the extent of the association of sex with the survival of ALL after accounting for the effect of other influential factors found in the univariable model and interaction effects of sex with age at diagnosis and radiation therapy. In this regard, we performed two adjusted models with and without the inclusion of immunophenotype in the model. The variable immunophenotype had 5881 missing values. For both adjusted models, analyses were stratified by the year of diagnosis to account for the time varying survival in the follow-up period. In addition, we performed a subgroup analysis to compare the risk of mortality from ALL between girls and boys in irradiated children diagnosed between ages 10 to 19 years. The statistical software SAS version 9.3 (SAS institute, Cary, NC, USA) was used to perform the analyses.
RESULTS
There were 8,113 (57.2%) boys and 6,079 (42.8%) girls among 14,192 pediatric ALL patients in the SEER dataset. Table 1 presented the distributions of clinical and survival features of pediatric ALL by sex. There were no substantial differences in the distribution of girls and boys by race and year of diagnosis, P > 0.05. Compared to girls, more boys were diagnosed in each age at diagnosis group except that in the infants. The proportion of boys increased steadily with increased age of diagnosis (c2 for trend = 79.43, df = 1, P < 0.0001). Approximately, 48 and 68% of children diagnosed at < 1 and 15 to 19 years were boys, respectively. Marginally higher percentages of girls (1.6%) had multiple primary tumor sites compared to boys (1.1%), (c2 = 6.64, df = 1, P = 0.009). There was a highly significant difference in the distribution of immunophenotype by sex (c2 = 127, df = 1, P < 0.0001). Compared to girls (5.1%), a higher percentage of boys (10.4%) were found with T-cell phenotype. About 15.2% girls and 19.4% boys received radiation therapy. The 75th percentile survival time (SE) was 206 (22.55) months in girls and 74 (6.21) months in boys, while the mean survival time (SE) was 339.06 (2.88) months in girls and 323.67 (2.60) months in boys. The 5-year over-all survival rate was 79%, while the 10-year survival rate was 74%. Girls had better 5 and 10-year survival rates (82 and 77%) compared to that of boys (77 and 71%).
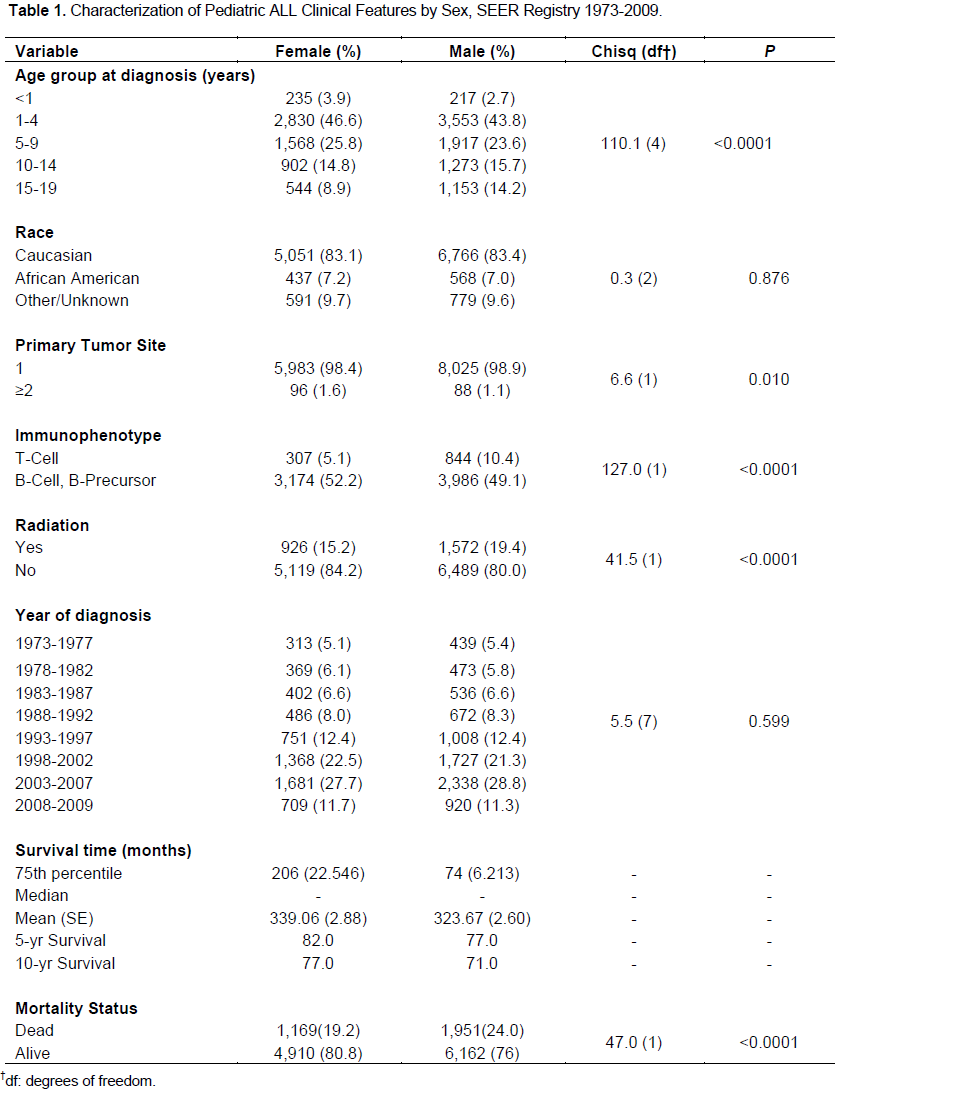
There was a significant difference in the distribution of deaths between boys and girls (c2 = 47, df = 1, P < 0.0001), as all-cause-mortality was 19.2 and 24.0% in girls and boys, respectively. Table 2 displayed the distri-bution of mortality in pediatric ALL patients by sex, age at diagnosis and the receipt of radiation therapy. Although, the proportion of death was higher in boys than that in girls across all ages at diagnoses, this difference varied substantially depending on the receipt of the radiation therapy. Of the 449 children diagnosed at infancy, only 61 patients received radiation therapy of which 30 and 31 were girls and boys, respectively. The proportion of mortality was higher in boys (63.3%) than that in girls (48.3%) in this very young group of irradiated children, while there was no substantial difference in mortality between the non-irradiated girls (49%) and boys (50%) of the same age group of diagnosis.
Among the children diagnosed between 1 to 4 years of ages and received the radiation therapy, 26.3% of girls and 33.4% of boys died, while in the non-irradiated group, 9.9 and 13.0% of girls and boys died, respectively. Of those who were diagnosed at ages 5 to 9 years and received radiation therapy, 27.3% of girls and 34.0% of boys died, while only 14.8% of girls and 18.4% of boys died in non-irradiated patients of the same age at diagno-sis group. Similarly, among children who were diagnosed between 10 to 14 years of age, 36.2 and 34.4% of irradiated girls and boys experienced death, respectively, while 25.2 and 29% of non-irradiated girls and boys died. In the children with age of diagnosis between 15 to 19 years, about 41.1 and 41.4% of irradiated girls and boys died, respectively, while 36.3 and 41.3% of non-irradiated girls and boys died, respectively.
.png)
Table 3 showed the factors associated with mortality in pediatric ALL in the SEER dataset. In this univariable Cox proportional hazard model, there was a highly significant difference in the mortality outcome in pediatric ALL by sexes. Boys were 1.29 times as likely as girls to die from ALL, hazard ratio (HR) = 1.29, 95% confidence interval (CI): 1.20, 1.39. Compared to the reference group, in-fants, the estimated HR of children diagnosed with ALL in the 1 to 4, 5 to 9, 10 to 14 and 15 to 19 age groups were HR = 0.18, 95% CI: 0.15, 0.20, HR = 0.26, 95% CI: 0.2,0.30, HR = 0.44, 95% CI: 0.38, 0.51 and HR = 0.69, 95% CI: 0.59, 0.80, respectively. AA pediatric ALL pa-tients did differ from those of Caucasians with respect to mortality, and 44% were more likely to experience mortality, HR = 1.44, 95% CI: 1.27, 1.62. Although not significant, children diagnosed with multiple primary tumor sites showed a higher risk of death compared to those who had a single primary tumor site at the time of diagnosis, HR = 1.18, 95% CI: 0.92, 1.52. Children with the B-cell and B-precursor ALL had a lower hazard than those with T-cell ALL, HR = 0.57, 95% CI: 0.49, 0.65. Radiation, per se, did not improve survival; rather survival was worsened in patients received radiation therapy. Compared to the children who did not undergo radiation therapy, the irradiated children had an approximately 1.66 times higher hazard, HR = 1.66, 95% CI: 1.53, 1.79, of dying from ALL. The HR decreased monotonically over the year of diagnosis, which implied the time-varying survival pattern during the follow-up period.
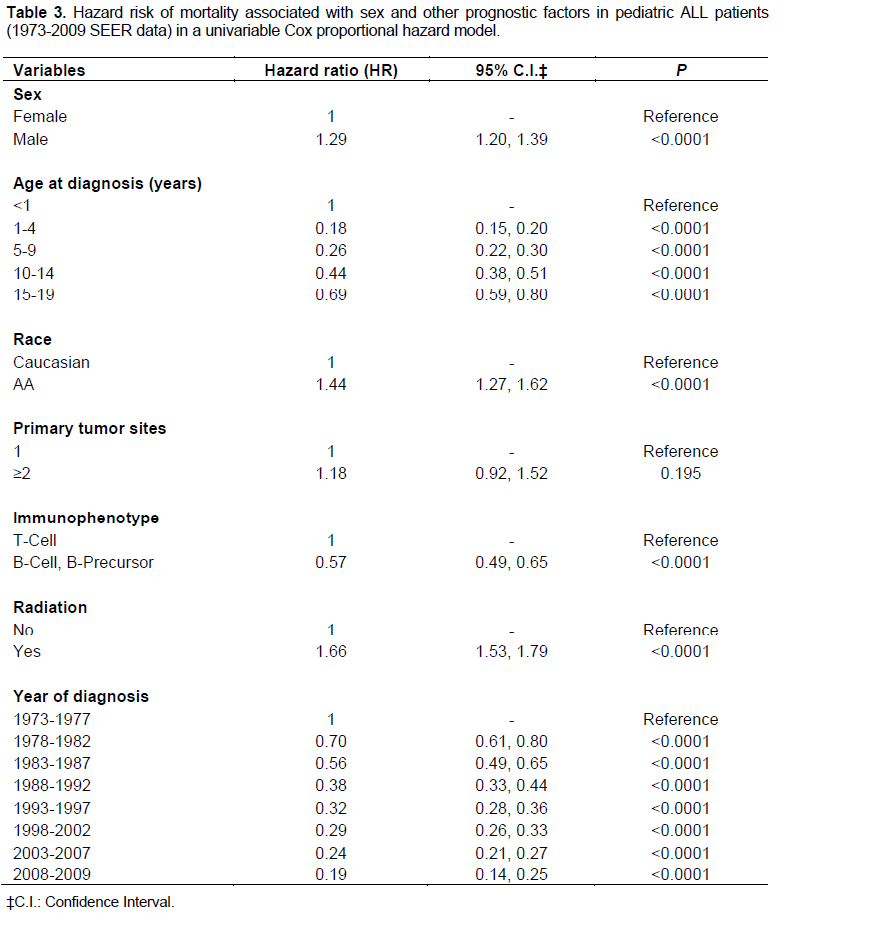
Table 4 presented the risk of mortality associated withsex in pediatric ALL patients estimated from two multivariable variable Cox proportional hazard models. The first model was adjusted for the effects of age at diagnosis, race, number of primary tumors, radiation, interactions of sex with age at diagnosis and radiation. The second model included immunophenotype in addi-tion to the variables in the first model. After accounting for the main and interaction effects in the first model and stratification by the year of diagnosis, the significance of the difference in survival between girls and boys, found in univariable model, failed to persist, adjusted HR (AHR) = 1.21, 95% CI: 0.93, 1.56, P = 0.15. After inclusion of immunophenotype in the model, the significance of the sex difference still failed to persist in a relatively smaller number of patients.
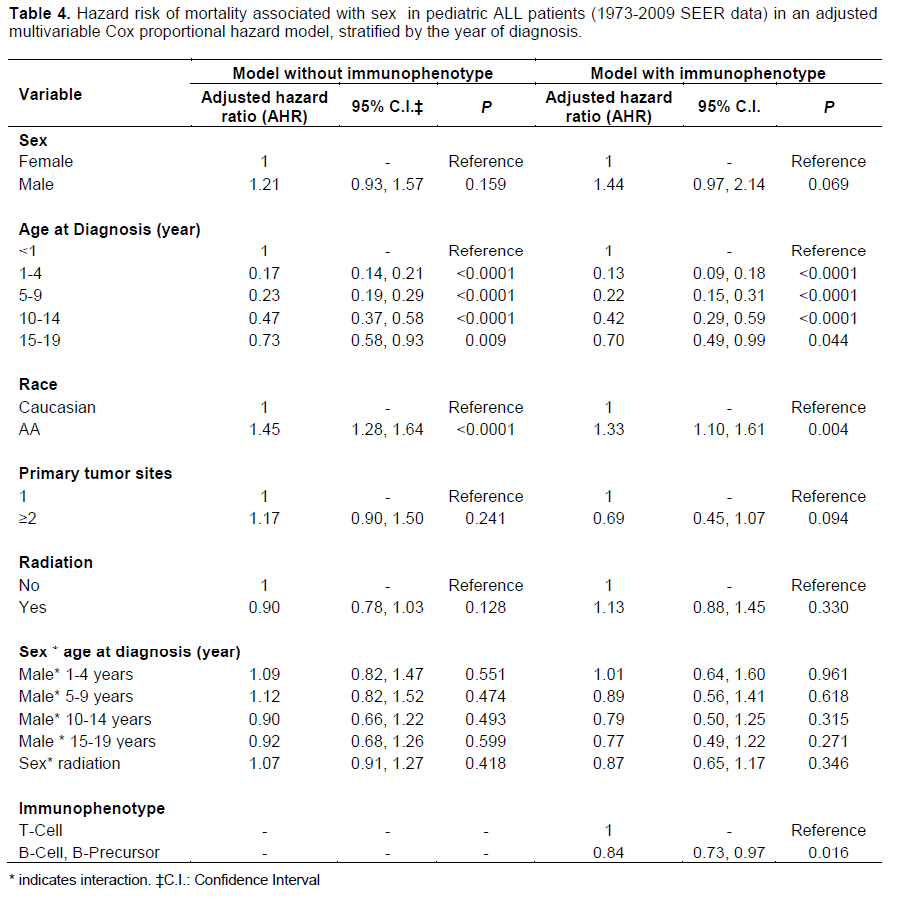
Table 5 illustrated the hazard risk of mortality associated with sex in irradiated pediatric ALL patients diagnosed between ages 10 and 19 years, estimated in two multivariable variable Cox proportional hazard models. The first model was adjusted for the effects age at diagnosis and race, and the other model included immunophenotype in addition to the age at diagnosis and race. There was no substantial sex difference in the risk of mortality in this subgroup of irradiated pediatric ALL patients; AHR = 1.09, 95% CI: 0.89, 1.35 and AHR = 0.96, 95% CI: 0.70, 1.33 in the first and second models, respectively.
.png)
DISCUSSION
Sex disparity in the survival of pediatric ALL has long been consistently reported (Carroll et al., 2003; Pui et al., 1999; Sather et al., 1981). The present study have attempted to assess the impact of sex on ALL survival after accounting for the effects other known prognostic factors and their interactions with sex. There are few findings from our study. First, the distribution of mortality from pediatric ALL by sex is substantially different by the receipt of radiation therapy and age at diagnosis. Se-condly, the significance of sex on the survival of pediatric ALL has diminished after accounting for the effects of the following prognostic factors: age at diagnosis, receipt of radiation therapy, race, immunophenotype and interactions of sex with age at diagnosis and receipt of radiation therapy. Thirdly, there is no substantial impact of sex on the survival of pediatric ALL among irradiated patients diagnosed between 10 and 19 years.
In the SEER population based dataset of pediatric ALL, difference in mortality by sex remained consistent over the age at diagnosis in non-irradiated children, except among those diagnosed during infancy (Table 2). The result of this disparity in pediatric ALL survival is supported by findings of the previous studies (Carroll et al., 2003; Chessells et al., 1995; Sather et al., 1981). No difference in mortality by sex has been observed in non-irradiated children diagnosed during infancy. However, among the irradiated children, substantially differential mortality patterns have been observed between girls and boys over the age at diagnosis. The irradiated children, diagnosed during infancy have shown the largest difference in mortality, 15%, between girls (48%) and boys (63%). In fact, the proportion of deaths in girls of this group of children is the same as that in non-irradiated children of the same age of diagnosis. Irradiated boys diagnosed between ages 1 to 9 years are likely to have a higher mortality compared to irradiated girls of the same ages. While, no difference in mortality is observed between irradiated girls and boys diagnosed between ages 10 to 19 years. Radiation therapy may likely to have a key role in the removal of the sex disparity of mortality in this group of pediatric ALL patients. This finding is partly supported by previous studies showing a lessened sex disparity in survival due to the use of intensified therapy (Carroll et al., 2003; Pui et al., 2009; Silverman et al., 2001).
Although boys have shown a highly significantly increased risk of mortality compared to girls in the un-adjusted analysis, the significance of this sex difference in the mortality has diminished after the adjustment for the prognostic factors of age at diagnosis, race, receipt of radiation therapy, interaction of sex with age at diagnosis, and the interaction of sex with the receipt of radiation therapy. In a subgroup analysis of irradiated children diagnosed between ages 10 to 19 years, no substantial effect of sex on the survival of pediatric ALL is observed in a model adjusted for age at diagnosis and race (Table 5). This result is further enhanced with the inclusion immunophenotype in the model (Table 5).
In addition, our study has confirmed the prognostic value of age at diagnosis (Carroll et al., 2003; Möricke et al., 2005; Sather, 1986), immunophenotype (Pui et al., 1993) and race (Bhatia et al., 2002; Kadan-Lottick et al., 2003) which are identified as the important predictors of pediatric ALL survival in previous studies .
Like other epidemiological studies, the current study is not without limitation. First, our results may be driven in part by the effect of unmeasured confounders. There is no other treatment information except radiation therapy in the SEER data. Secondly, the follow-up periods tend to be shorter for children diagnosed more recently. How-ever, our results are not limited by this variability of the follow-up time, since we have stratified the analysis by the year of diagnosis. Despite the limitations, epidemio-logic studies often utilize population based large datasets and are able to provide naive insight into the etiology of the disease and treatment processes which are later verified through intensive investigations.
CONCLUSION
The sex disparity in the survival of pediatric ALL may be partly explained by its interaction with age at diagnosis and radiation treatment; and the radiation therapy could eliminate the sex disparity in the survival of ALL patients after diagnosed of 10 years. Further research is warranted to validate the findings of this study.
CONFLICT OF INTERESTS
The author(s) have not declared any conflict of interests.
REFERENCES
|
Bhatia S, Sather HN, Heerema NA, Trigg ME, Gaynon PS, Robison LL (2002). Racial and ethnic differences in survival of children with acute lymphoblastic leukemia. Blood 100(6):1957-1964. Crossref |
||||
|
Carroll WL, Bhojwani D, Min DJ, Raetz E, Relling M, Davies S, Downing JR, Willman CL, Reed JC (2003). Pediatric acute lymphoblastic leukemia. American Society of Hematology Education Program 102-131. Crossref |
||||
|
Chessells JM, Richards SM, Bailey CC, Lilleyman JS, Eden OB (1995). Gender and treatment outcome in childhood lymphoblastic leukaemia: report from the MRC UKALL trials. Br. J. Haematol. 89(2):364-372. Crossref PubMed |
||||
|
Dördelmann M, Reiter A, Borkhardt A, Ludwig W D, Gotz N, Viehmann S, Gadner H, Riehm H, Schrappe M (1999). Prednisone response is the strongest predictor of treatment outcome in infant acute lymphoblastic leukemia. Blood 94:1209-1217. PubMed |
||||
|
Hilden JM, Frestedt JL, Moore RO, Heerema NA, Arthur DC, Reaman GH, Kersey JH (1995). Molecular analysis of infant acute lymphoblastic leukemia: MLL gene rearrangement and reverse transcriptase-polymerase chain reaction for t(4;11)(q21;q23). Blood 86(10):3876-3882. PubMed |
||||
| Howlader N, Noone AM, Krapcho M, Garshell J, Neyman N, Altekruse SF, Kosary CL, Yu M, Ruhl J, Tatalovich Z, Cho H, Mariotto A, Lewis DR, Chen HS, Feuer EJ, Cronin KA (2013). SEER Cancer Statistics Review, 1975-2010, National Cancer Institute. Bethesda, MD. Accessed December 24, 2013. | ||||
|
Kadan-Lottick NS, Ness KK, Bhatia S, Gurney JG (2003). Survival variability by race and ethnicity in childhood acute lymphoblastic leukemia. JAMA 290(15):2008-2014. Crossref |
||||
|
Lanning M, Garwicz S, Hertz H, Jonmundsson G, Kreuger A, Lie SO, Moe PJ, Salmi TT, Schröder H, Siimes MA, Wesenbergs F, Yssing M, Ahstrom A, Gustafsson G (1992). Superior treatment results in females with high-risk acute lymphoblastic leukemia in childhood. Acta Paediatr. 81(1):66-68. Crossref |
||||
|
Möricke A, Reiter A, Zimmermann M, Gadner H, Stanulla M, Dördelmann M, Löning L, Beier R, Ludwig WD, Ratei R, Harbott J, Boos J, Mann G, Niggli F, Feldges A, Henze G, Welte K, Beck JD, Klingebiel T, Niemeyer C, Zintl F, Bode U, Urban C, Wehinger H, Niethammer D, Riehm H, Schrappe M; German-Austrian-Swiss ALL-BFM Study Group (2008). Risk-adjusted therapy of acute lymphoblastic leukemia can decrease treatment burden and improve survival: treatment results of 2169 unselected pediatric and adolescent patients enrolled in the trial ALL-BFM 95. Blood 111(9):4477-4489. Crossref |
||||
|
Möricke A, Zimmermann M, Reiter A, Gadner H, Odenwald E, Harbott J, Ludwig WD, Riehm H, Schrappe M (2005). Prognostic impact of age in children and adolescents with acute lymphoblastic leukemia: data from the trials ALL-BFM 86, 90, and 95. Klin. Padiatr. 217(6):310-320. Crossref |
||||
|
Nachman J, Sather HN, Cherlow JM, Sensel MG, Gaynon PS, Lukens JN, WolffL, Trigg ME (1998). Response of children with high-risk acute lymphoblastic leukemia treated with and without cranial irradiation: A report from the children's cancer group. J. Clin. Oncol. 16:920-930. PubMed |
||||
|
Pui CH, Behm FG, Downing JR, Hancock ML, Shurtleff SA, Ribeiro RC, Head DR, Mahmoud HH, Sandlund JT, Furman WL (1994). 11q23/MLL rearrangement confers a poor prognosis in infants with acute lymphoblastic leukemia. J. Clin. Oncol. 12:909-915. PubMed |
||||
|
Pui CH, Behm FG, Crist WM (1993). Clinical and biologic relevance of immunologic marker studies in childhood acute lymphoblastic leukemia. Blood 82(2):343-62. PubMed |
||||
|
Pui CH, Boyett JM, Relling MV, Harrison PL, Rivera GK, Behm FG, Sandlund JT, Ribeiro RC, Rubnitz JE, Gajjar A, Evans WE (1999). Sex differences in prognosis for children with acute lymphoblastic leukemia. J. Clin. Oncol. 17(3):818-824. PubMed |
||||
|
Pui CH, Campana D, Pei D, Bowman WP, Sandlund JT, Kaste SC, Ribeiro RC, Rubnitz JE, Raimondi SC, Onciu M, Coustan-Smith E, Kun LE, Jeha S, Cheng C, Howard SC, Simmons V, Bayles A, Metzger ML, Boyett JM, Leung W, Handgretinger R, Downing JR, Evans WE, Relling MV (2009). Treating childhood acute lymphoblastic leukemia without cranial irradiation. N. Engl. J. Med. 360(26):2730-41. Crossref |
||||
|
Pui CH (1997). Acute lymphoblastic leukemia. Pediatr. Clin. North Am. 44:831-846. Crossref |
||||
|
Reaman G, Zeltzer P, Bleyer WA, Amendola B, Level C, Sather H, Hammond D (1985). Acute lymphoblastic leukemia in infants less than one year of age: a cumulative experience of the Children's Cancer Study Group. J. Clin. Oncol. 3(11):1513-1521. PubMed |
||||
|
Reaman GH, Sposto R, Sensel MG, Lange BJ, Feusner JH, Heerema NA, Leonard M, Holmes EJ, Sather HN, Pendergrass TW, Johnstone HS, O'Brien RT, Steinherz PG, Zeltzer PM, Gaynon PS, Trigg ME, Uckun FM (1999). Treatment outcome and prognostic factors for infants with acute lymphoblastic leukemia treated on two consecutive trials of the Children's Cancer Group. J. Clin. Oncol. 17:445-455. PubMed |
||||
|
Rubnitz JE, Shuster JJ, Land VJ, Link MP, Pullen DJ, Camitta BM, Pui CH, Downing JR, Behm FG (1997). Case-control study suggests a favorable impact of TEL rearrangement in patients with B-lineage acute lymphoblastic leukemia treated with antimetabolite-based therapy: a Pediatric Oncology Group study. Blood 89(4):1143-1146. PubMed |
||||
|
Sather H, Miller D, Nesbit M, Heyn R, Hammond D (1981). Differences in prognosis for boys and girls with acute lymphoblastic leukaemia. Lancet 1(8223):739-43. Crossref |
||||
|
Sather HN (1986). Age at diagnosis in childhood acute lymphoblastic leukemia. Med. Pediatr. Oncol. 14(3):166-172. Crossref |
||||
|
Silverman LB, Gelber RD, Dalton VK, Asselin BL, Barr RD, Clavell LA, Hurwitz CA, MoghrabiA, Samson Y, Schorin MA, Arkin S, Declerck L, Cohen HJ, Sallan SE (2001). Improved outcome for children with acute lymphoblastic leukemia: results of Dana-Farber Consortium Protocol 91-01. Blood 97 (5):1211-8. Crossref |
||||
|
Smith M, Arthur D, Camitta B, Carroll AJ, Crist W, Gaynon P, Gelber R, Heerema N, Korn EL, Link M, Murphy S, Pui CH, Pullen J, Reamon G, Sallan SE, Sather H, Shuster J, Simon R, Trigg M, Tubergen D, Uckun F, Ungerleider R (1996). Uniform approach to risk classification and treatment assignment for children with acute lymphoblastic leukemia. J. Clin. Oncol. 14(1):18-24. PubMed |
||||
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


