Full Length Research Paper

ABSTRACT
The study aimed to assess the impact of family planning on maternal and infant mortality in Tiko CDC plantation camp. This is a clustered non-randomized controlled trial with a predetermined intervention site (Tiko CDC plantation camp) and a control site (Pena Mboko camp). Four clusters were randomly selected in each group using simple ballot and the intervention administered in all clusters in the intervention site. Households/participants were then systematically sampled (250 in each site) for data collection and analysis. The intervention comprises a triad of health education, facilities strengthening and distribution of contraceptives in the intervention cohort. After baseline study, re-evaluation visits are scheduled for 3rd, 6th and 9th month of intervention and a post-intervention data collection at 12th months of intervention. The pre-intervention phase was conducted from December 2019 to February 2020; data was partially analysed and intervention was designed. Primary outcomes to be measured are contraceptive knowledge, perception and practice while secondary outcomes are maternal and infant morbi-mortality. Ethical clearance was obtained from the institutional ethics committee for research on human health at University of Douala. While the study adds to existing literature, its strengths and limits could be useful in informing similar interventions in the study area and beyond.
Key words: Non-randomized clustered, Family planning, Health education, Maternal, Infant, mortality, Cameroon.
Abbreviation: CDC, Cameroon Development Corporation; MDG, Millennium Development Goals; MMR, Maternal Mortality Ratio; LMIC, Low and Middle Income Countries; HBM, Health Believe Model; STI, Sexually Transmissible Infections; FP, Family Planning; OCPs, Oral Contraceptive Pills; CHW, Community Health Workers; FGD, Focus Group DiscussionINTRODUCTION
Although there has been a global decrease in maternal mortality, the decrease is slow and the Millennium Development Goal (MDG) 5A target to reduce pregnancy related deaths by three-quarter (75%) and 5B target of achieving universal access to reproductive health by 2015 was not achieved (Assefa et al., 2017; Millennium Development Goal 5-Results, 2020). While maternal deaths continue to remain a major public health problem worldwide (Pierre-Marie et al., 2015), it is a major concern in Cameroon. A recent study reported an increase in the maternal mortality ratio (MMR) from 669 in 2004 to 782 in 2011 per 100,000 live births (Meh et al., 2020). Most of these maternal deaths are preventable and occur due to the unavailability of and/or poor quality of health services (Islam and Yoshida, 2009). High risk groups for maternal and infant mortality include younger and older maternal age (<18 and >34 years), high parity (>3 births) and short birth intervals (Brown et al., 2015). Therefore when designing an effective family planning interventions, it must take into consideration these target groups. Long before now, body of evidences had shown a focus on the global need of quality healthcare services and providers as a way to alleviate the high maternal deaths worldwide and thus tackle the slow progress towards achieving the MDG 5A (Islam and Yoshida, 2009). It is now evident that the possibility of achieving quality healthcare globally is not feasible, particularly in the poor settings (GALLUP, 2010). This is due to the multidimensional nature of health and the huge financial constrain this may incur. In recent times, more emphases are being placed on contraception as a means to achieving reduction in maternal and child mortality (Chola et al., 2015). This is because there is a vast possibility of achieving globally availability of contraceptives, even in the very poor settings.
Increasing body of evidence shows that family planning significantly reduces the frequency of exposure to high risk and unwanted pregnancies, and consequently, maternal mortality reduction (Brown et al., 2015; Stover and Ross, 2010). The poorest settings are usually the highest fertility zones and unfortunately, many women in less developed countries do not use family planning (Prata, 2009)thus accounting for high maternal and infant deaths in these settings. In such poor settings where access to quality health service is limited, family planning can considerably improve maternal and child outcome (Prata, 2009). In 2008, contraceptive use averted approximately 44% of maternal deaths around the world (Family Planning and Maternal Health, 2015).
Although studies have attempted to enlighten on the correlation between family planning and reduction of maternal and infant deaths in some countries, very little is known for Cameroon. For instance a study in South Africa estimated that if contraceptive use is scaled up by 0.68% over a period of 15 years, unintended pregnancies, abortions and births can be reduced by 20% and that approximately 7000 new-born and child deaths and 600 maternal deaths can be averted (Chola et al., 2015). Unwanted pregnancy remains a major cause of maternal particularly in low and middle income countries (LMICs) (WHO, 2019).
While there is a strong negative correlation between levels of contraceptive use and the levels of infant mortality at the communal level, women who practice family planning can avoid high-risk births and therefore reduce their chances of having baby who will die in infancy (Guttmacher Institute, 2016). By reducing the number and spacing of children, the use of contraceptives can reduce morbidity and mortality in children by interrupting maternal depletion, sibling competition and birth crowding and infectious diseases (Conde-Agudelo et al., 2012; Molitoris, 2017).
Limited access to family planning services remains a major barrier to the use of contraception in LMICs. In a health report, Ndola pointed out four critical considerations to increase access to family planning in resource-poor settings (Prata, 2009); increasing knowledge about safety of family planning methods, ensuring that contraception is genuinely affordable to the poorest families, ensuring the supply of contraceptives by making family planning a permanent line item in healthcare system's budgets and taking immediate action to remove barriers hindering access to family planning methods. Most studies on contraception have focused on family planning programs but little has been done to assess the effect of family planning as an intervention to alleviate maternal and/or infant morbi-mortality.
Conceptual framework
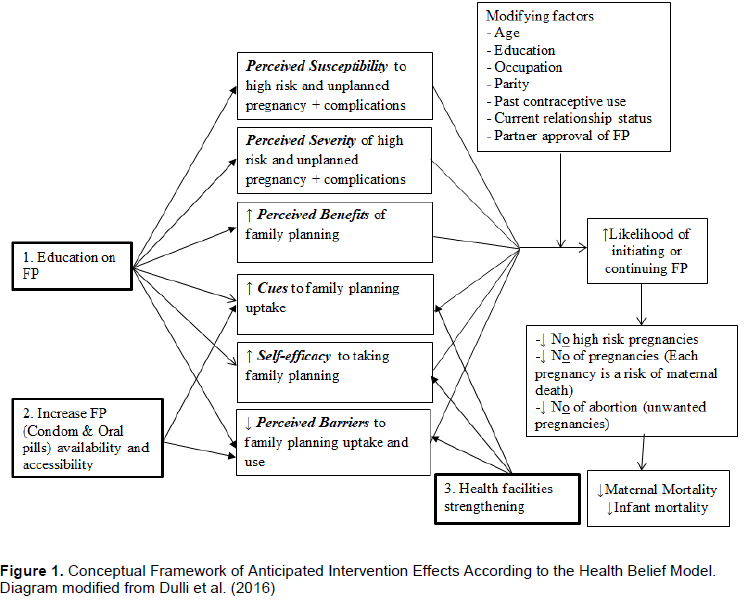
In this study, we used the health belief model (HBM) to design a moderate term intervention with the aim of increasing family planning uptake in the intervention site in anticipation of its subsequent impact on maternal and infant morbi-mortality. The model states that messages will achieve optimal behaviour change if they successfully target perceived barriers, benefits, self-efficacy and threat (Jones et al., 2015). The HBM and its constructs have been very effective in achieving behavioural health changes in several fields of studies (Jeihooni et al., 2016)including compliance to contraception (Hall, 2012). According to this model, there are six (6) constructs which defines the reasons for people’s behaviour: perceived susceptibility, perceived severity, perceived benefits, cues to action self-efficacy, and perceived barriers. Health interventions and promotion programs targeting behavioural changes that could positively impact health indicators should likewise be designed based on these HBM constructs.
It is important to note that family planning as a concept cuts across adopting preventive health behaviours (such as avoiding unwanted pregnancies, abstinence, sexually transmitted infections protection, etc.) to compliance with medical regimens such as the use contraceptives (Hall, 2012). This makes the HBM ideal for designing family planning interventions.
Our study intervention is a triad comprising of (1) health education on contraceptives and contraception, (2) health facility strengthening on family planning services and (3) increasing community availability and accessibility of basic contraceptives. The components of this intervention triad are responses to three major barriers to use of contraception globally and more specifically in our intervention site which includes lack of correct knowledge on contraception to guide inform choices on family planning, lack of basic contraceptive services at the health facility and lack of accessibility of basic contraception. This study has been designed such that in as much as the phase 1 (pre-intervention) of the study provided baseline data for which the impact of our intervention in the test site can be evaluated, it also served to provide information on the different constructs of the HBM on which the intervention has been designed. As such, this intervention is adapted based on the elements of the HBM constructs that were gotten in the pre-intervention phase (phase 1) of the study. Results of the pre-intervention phase of the study have been partially analysed and is under consideration to be forwarded to suitable journals for publications. The contents of the family planning intervention triad and at what levels they are intended to exert their influence in the HBM is shown in Figure 1.
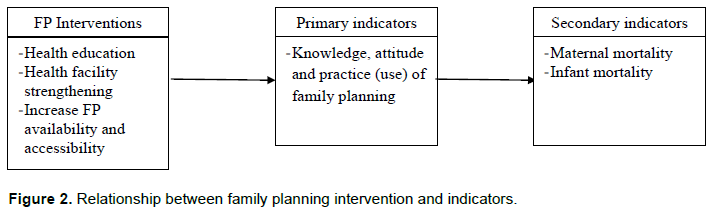
As seen in the Figure 2, although not probably through a direct influence, the final expectation of the intervention is the reduction of maternal and infant morbi-mortality. However, proximal to these indicators are primary (knowledge, attitude and practice of family planning) which bear the HBM constructs and on which the intervention is likely to exert direct influence. Thus by influencing these proximal indicators, family planning can be able to reduce maternal and infant mortality.
Hypotheses and objectives
The principal aim of this study is to determine the impact of family planning on maternal and infant mortality in Tiko CDC plantation camps, South West Region of Cameroon. Since compliance to use family planning can be achieved by influencing its knowledge, attitude and practice, the intervention specifically seeks to correct and increase the knowledge, attitude and practice of family planning in the high maternal mortality zone (Tiko health district) which we believe will subsequently influence maternal and infant mortality in the area. Therefore, the study has two major questions to answer: (1) what is the impact of the family planning intervention triad on the knowledge, attitude and practice of family planning in the Tiko CDC plantation camps? (2) What is the impact of a family planning intervention triad on maternal and infant mortality in the Tiko CDC plantation camps?
This study is based on hypothesise that the family planning intervention will result to an increase in the correct knowledge, attitude and practice of contraception. The provision of essential methods (condoms and OCPs) will reduce the barrier of unavailability and inaccessibility which is a major reason for non-use of contraception as noticed in the pre-intervention study. Correcting the knowledge through tailored health education will then influence the perceptions, attitude and eventually increase in the use and correct practice of family planning. Increase in the use of contraception will be expected to result to the following: (1) Reduction in number of high risk pregnancy in the community, thus maternal mortality, (2) reduction in deadly abortions that should have resulted from unwanted pregnancies, (3) reduction in neonatal mortality that should have accompanied children delivered to mothers with high risk pregnancies.
MATERIALS AND METHODS
Study area
The CDC plantation that has existed since 1947 has several camps all over the country, with over 22409 employees living within the camps (Assoua, 2013.). The study was conducted in CDC camps settings of Tiko (in the South West region) and Pena Mboko (in the Littoral Region) which are the main camps of the CDC. Tiko is bound by Limbe, Buea, Muyuka, Dibombari and Bonaberi to the West, North, North-East, East and the South respectively and has a total surface area of 4,840 km2. Tiko CDC camp has geographical coordinates 4° 4’ 30” North and 9° 22’ 0” East and the Pena Mboko camp coordinates 4° 16’ 30” North and 9° 26’ 30” East (Assoua, 2013). The camps consist of clusters of settlements constructed to harbour CDC plantation worker, for which there are over 600 houses in Tiko camp and 450 in the Pena Mboko camp. A typical labourer works 5 working days a week from 7 am to 6 pm with minimal wages. They also benefit free health services from health dispensary situated with the camps to provide first line management although these facilities do not have any functional family planning service. The low socio-economic status of the camp residents exposes them to a number of health risks including high maternal and infant morbi-mortality (Kimengsi et al., 2016).
Study design
This is a clustered non-randomized controlled community trial in which two different arms will be subjected to two separate study conditions: an intervention site where participants will receive family planning health education, health facilities strengthening and supply, and a control site where no intervention will be done. Eight (8) clusters and 500 households/participants systematically sampled and assigned to the two study arms in a 1:1 ratio based on predetermine criteria (i.e. 4 clusters and then 250 participants per site). After the start of the intervention, follow-up data will be collected at 3, 6 and 9 months period. End-line data will be collected at 12 months of the intervention.
The selection of our intervention site was predetermined by the fact that the Regional Delegation of Health for South West Region recorded an unusual high maternal deaths for 2018/2019 year for which Tiko Health District registered one of highest maternal mortality. Secondly, the Regional Taskforce for the fight against maternal mortality had expressed the necessity for an intervention study in the region to address these high maternal deaths, but nothing has been done to this effect. The CDC plantation camps, in addition to the fact that it provides a typical community lifestyle suitable for a community intervention, the low socio-economic status of residents exposes the community to a number of health risk, including high maternal mortality. Likewise, the selection of Penda Mboko CDC plantation camps as a control site was purposive in that this site is seemingly similar to the Tiko CDC plantation camps in many likes including the general setting.
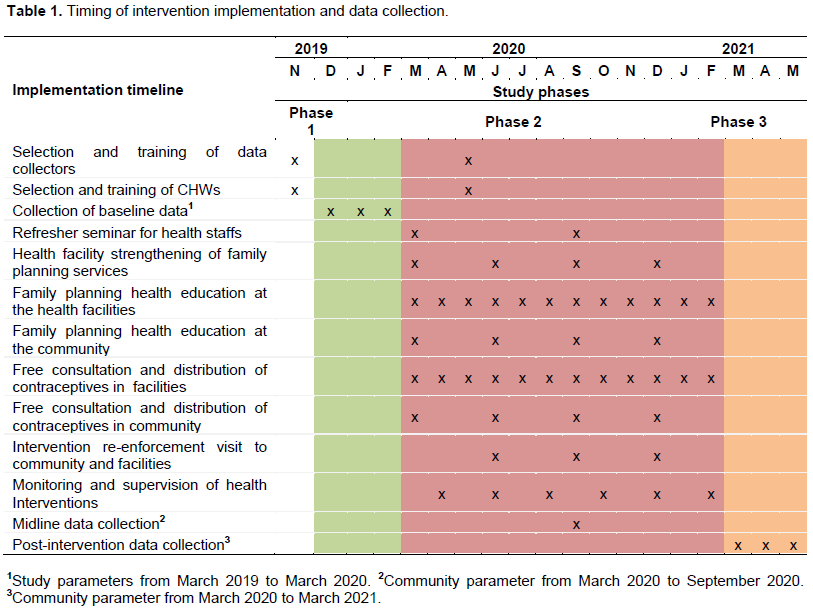
The study was organized into three phases: Phase 1 (Pre-intervention), Phase 2 (Intervention) and Phase 3 (Post-intervention). Measurements of community parameters were done in both the intervention and control sites during these different study phases. The sample units were the clusters (pre-existing camp quarters) and then individuals (within the sampled clusters). The sampling of the clusters and the participants for the study measurements was done already during the first study phase from December 2019 to February 2020. The communities and households that participated in the first phase of the study were sorted and recruited for data collection during the intervention, evaluation and final phase of the study.
The intervention is designed to run for 12 months with three (3) re-enforcement and evaluation sessions during the intervention period (3, 6 and 9 months after onset of intervention). Intervention will be simultaneously carried out in all the sampled clusters within of the intervention community.
Inclusion and exclusion criteria
Those who participated in the pre-intervention study were women of age 15-49 years, sexually active by the time of the study, resident within the sampled CDC plantation camps (at least 2 years prior to study) and gave consent (assent for participants < 18 years) to freely participate in the study. In addition to the above criteria, participants for the intervention study must be one who had participated in the pre-intervention. Women newly visiting the camp and those who do not meet these study criteria were excluded.
Sample size calculation for the clustered non-randomized controlled trial
The sample size for this community trial was calculated using the formula for comparison between two groups as shown below (Charan and Biswas, 2013):
Where,  =1.44 (from z table), Zβ/2= Z0.15/2=0.75 (from z table at 75%), P1= 61%=0.61, P2 = 66%=0.66, P =pooled prevalence (prevalence in intervention group (p1) + prevalence in control group (p2)/2, P= 0.94
=1.44 (from z table), Zβ/2= Z0.15/2=0.75 (from z table at 75%), P1= 61%=0.61, P2 = 66%=0.66, P =pooled prevalence (prevalence in intervention group (p1) + prevalence in control group (p2)/2, P= 0.94


Considering the 15% non-response rate, the sample size (n) is adjusted to 250 women of reproductive age to be involved in the intervention community and 250 in the control community.
Sampling technique for data collection in the intervention and control arm
The intervention site (Tiko CDC plantation camp) was predetermined by the high maternal mortality record of 2018/2019 in the Tiko Health District of South West Region, Cameroon as reported in an unpublished data from the Regional Delegation of Public Health for South West Region. The control site (Penda Mboko CDC camp) was purposively selected based on the fact it is large enough to be comparable to the Tiko CDC camp and also, the location of the control site is far from the intervention site, thus limiting the spill over effect that may result from interaction between participants in the two study settings. While the intervention will be carried-out in the entire Tiko CDC plantation camp clusters, evaluation of the impact of the intervention in the cohort will be based on data collection from systematically sampled participants with randomly selected clusters in the camp.
A random sample of 4 clusters was selected from 9 clusters in the Tiko CDC plantation camp (experimental site) by simple balloting. Similarly, 4 clusters were selected out of 7 in the Penda Mboko CDC camp (control site). Within each cluster, participants were then systematically selected as such: the main street of the clusters was identified and then a plastic bottle was spine in order to determine the direction of sampling. All households left to the principal surveyor were sampled for eligible participants. The number of participants selected per cluster was proportionate to the size of the cluster. Only one participant was selected per household and this was the first participant who met the inclusion criteria, encountered in the house at the time of visit by the surveyors during the first phase of the study.
Intervention development and implementation
The aim of the intervention is to influence the uptake of family planning and subsequently, impact maternal and infant mortality. This intervention development is based on the Health Belief Model (HBM). It consists of a web of actions that we believe will influence different constructs of the model. These actions that constitute the intervention have been developed in seven (7) logical steps which include a) Selection and training of data collectors and community health worker, b) collection of baseline data, c) health facility strengthening, d) family planning health education, e) increasing family planning availability and accessibility (those accepted for over the counter distribution), f) monitoring and evaluation and g) and mid-line and end-line data collection and analysis.
Step 1: Selection and training of data collectors for the study
Eight (8) community health workers (CHW) were selected (4 for Tiko and 4 for Penda Mboko CDC plantation camps) to guide the data collectors throughout the study as they access the community. The Centre for Research and Health Promotion in Buea provided the data collection team, whom together with the CHWs were trained on the modalities of study. The training that took place in the Tiko District Health Service was headed by the principal investigator with assistance from the Director of the Centre for Research and Health Promotion. The training focused on the rationale of the study, community entry protocols, participant confidentiality issues, the importance of family planning, correct use of available family planning methods, side effects etc. The training was adapted using the training manual of a GTZ family planning sensitization campaign.
Since we anticipated that the covid-19 pandemic may persist during the study period, an emergency training session was conducted in May 2020 with the focus being protective measures and methods of limiting corona virus spread in community during the study.
Step 2: Collection of Baseline Data in the intervention and control site
Data related to socio-demographic and reproductive life of the participants were collected from 333 sampled participants in the intervention site from December 2019 to February 2020. This baseline cross-sectional study was used to inform the family planning intervention that will be carried out in the Tiko CDC plantation camp. Baseline data was equally collected in the control site.
Step 3: Health facilities strengthening on family planning services
Cottage hospital and PMI in Tiko town were the two main recognized health facilities offering family planning services to the Tiko population including the Tiko CDC plantation camp residents. Two family planning personnel from each of these facilities were interviewed concerning family planning service deliveries. They were invited to take part in a family planning refresher seminar that took place at March 2020 as part of the intervention. In addition to education on the different family planning methods that they received, they were charged with the duty of continuing individual and programmed group counselling on family planning in the facilities. At the end of the seminar, they were provided with sufficient stocks of male and female condoms and oral contraceptive pills (OCPs) to be distributed free of charge to those with indications. Also, these health facilities (Cottage hospital and PMI) were visited thrice during the intervention period with the objective to maintain a continued education on family planning to providers on different contraceptive methods and encourage the facilities to always maintain their stocks of these different methods and also to provide them with sufficient stocks of male and female condoms and OCPs to be distributed free of charge. The Associate of the Chief Medical Officer of Tiko Health District Service was charged with the duty of ensuring sufficient stock of necessary family planning methods to the different health facilities in the Tiko Health District. No health facility strengthening program was scheduled for the control community.
Step 4: Family planning health education
The information content of the health education intervention has been contextually tailored to handle issues related to the importance and advantages of family planning and different methods, poor knowledge, misconceptions, misuse, barriers to use including availability and accessibility problems. This education will be achieved through periodic distribution of brochures, posters, and individual and group discussion sessions. The control site did not receive any of this family planning Information-education and communication measures (IEC). The distribution of the IEC materials and the discussion sessions was done at the sampled households in the intervention site and at the health facilities offering family planning services in the community. While health education at the households was done on periodic bases during the intervention period, the family planning units of health facilities at the intervention site were programmed to integrate a routine weekly group education session as well as daily individual sessions.
Step 5: Increasing family planning availability and accessibility
This was achieved through free reproductive health consultation and distribution of male condoms, female condoms and oral contraceptive pill in the intervention community. The purpose of the consultation was to assess reproductive health risks and suitable contraceptive methods for the participants in need of contraception. As a cue to contraceptive use, those who were suitable for condoms and/or contraceptive pills were given free of charge during the community visits otherwise they were referred to a nearby health service for their preferred method. While this reproductive health consultation and free distribution of contraceptives at the community level will be done on period bases, the same could be access at the selected health facilities throughout the intervention period.
Step 6: Monitoring and evaluation
The trained family planning providers of the cottage hospital and PMI were charged with monitoring and evaluation of family planning service delivery in these facilities and are required to provide report on monthly bases. At the community level, the sampled households acted as point where reminder group discussions and sensitization on family planning were conducted during the 3rd, 6th and 9th month evaluation of the intervention in the Tiko CDC camp.
The different study phases and proposed timing when they are to be implemented are summarized in Table 1
Step 7: Mid-line and end-line data collection and analysis
While follow-up data were collected at 3, 6 and 9 months of intervention in both study arms, end-line data were scheduled at the end of the study intervention (12 month) using the same data collection tool and procedures as at baseline.
Measurements
Based on the HBM constructs, a number of community indicators were measured in the pre-intervention and in the post intervention phase of the study to assess the impact of the intervention. It is important to note that the impact of the intervention on these different indicators can also be modified by covariates including the socio-demographic variables of the participants. However, this will be controlled for since same participants will be used in the pre-intervention and post-intervention phase of the study.
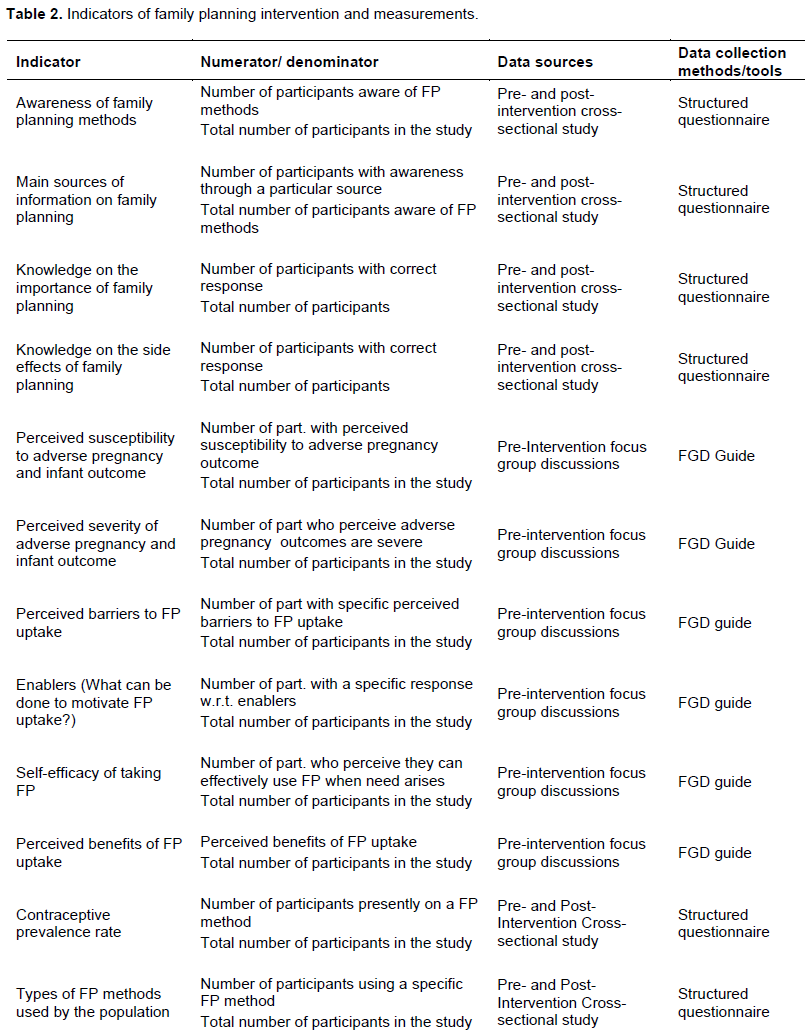
Table 1 summarizes the different indicators to be measured and how they will be measured.
Outcomes
Depending on where the intervention exerts its influence shown in Figure 2, the study focuses on two levels of outcomes (Vetter and Mascha, 2017): proximal (primary) and distal (secondary) outcomes.
Proximal outcomes
The primary outcomes are those that could be directly influence by the intervention and in the shortest possible time. They include community knowledge, attitude and practice (use) of family planning. Indicators of knowledge on contraception captured in the study questionnaire include awareness of different forms of contraceptive methods (either heard or seen), information held concerning family planning (definitions, short and long term implications, side effects of contraceptive methods, etc.) and sources of information on family planning. Indicators of attitude and practice of contraception to be assessed include contraceptive method mix (prevalence of different forms of contraceptive use present and past), unmet needs for contraception and reasons for non-use of contraception, preferences and barriers to use of
contraception. The methods of data collection and calculation of these different indicators are shown in Table 1. Being observational data, they were calculated as rates. For example, the awareness rate of family planning is operationalized as the number of participants who are aware (has heard or seen) of family planning or a contraceptive methods divided by the total number of study participants. This was calculated for the pre-intervention and the post-intervention phase of the study and the change represent the impact of the intervention on that particular parameter.
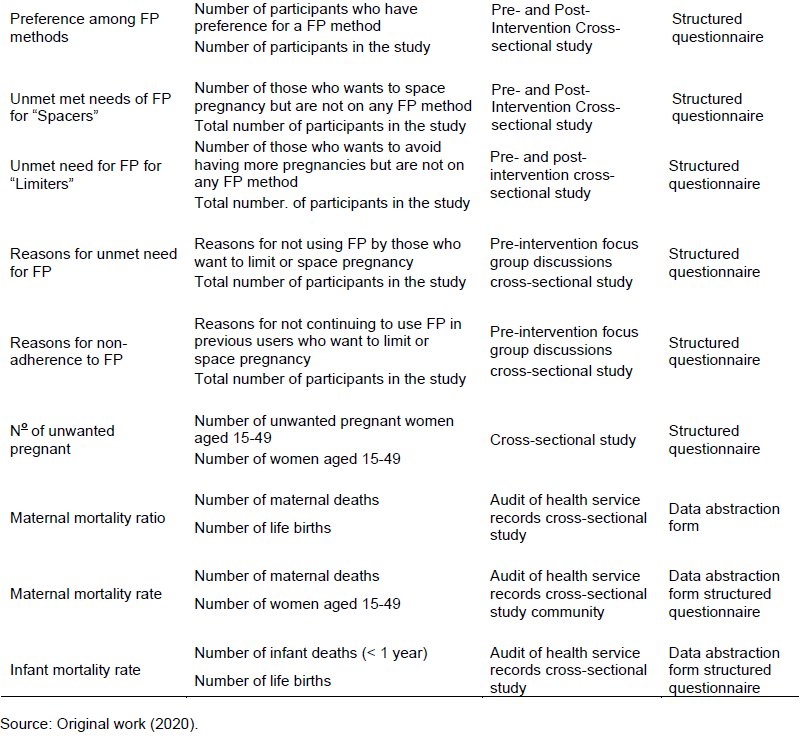
Distal outcomes
These represent those outcomes on which the intervention will exert its influence indirectly by influencing the primary outcomes (Figure 2). The impact of the intervention on these outcomes may not be immediate. The secondary outcomes include maternal and infant morbi-mortality indicators. The indicators for maternal morbi-mortality that will be measured include (1) Number of pregnancies (as an indicator of high risk pregnancies), (2) Number of abortions/miscarriages, (3) maternal mortality rate and (4) maternal mortality ratio while the indicator for infant morbi-mortality is infant mortality rate. The mode of data collection and calculations of these different outcomes and indicators are presented in Table 2. Since the same study participants will be used for the pre and the post-intervention study, the difference in the number of pregnancies (high risk), number of abortions/miscarriages, maternal and infant mortality will represent the impact of the intervention on the pregnancies, abortions, maternal and infant mortality respectively. Beside the maternal and infant mortality, the other distal outcomes are operationalized as point prevalence for women of reproductive age (in the CDC camps) in the before and the after intervention study. The maternal mortality ratio and rate will be operationalized using the population based survey direct estimation method as the number of maternal deaths in the study population in the previous one year, divided by the number of life births and women 15-49 years in the study population respectively (World Health Organization, 2006). Likewise, the infant mortality rate will be operationalized as point prevalence representing the number of infant deaths among the study population household that has occurred with the previous one year divided by the number of infants among the study households. As a limitation of this study, it is its scope to identify the death-specific cause of the maternal or infant deaths.
Qualitative data
The subjects of interest covered by the focus group discussions include the 6 HBM constructs related to our family planning interventions as shown in Figure 1: (1) perceived susceptibility to high risk pregnancies, unplanned pregnancies and their associated complications, (2) perceived severity of these high risk and unplanned pregnancies and their outcomes, (3) perceived benefits of family planning, (4) cues to uptake or/and adherence to family planning, (5) self-efficacy of taking and using family planning method(s), (6) perceived barriers to family planning. The participants of the different focus groups were requested to freely discuss their perceptions on these different subjected which has given rise to the information content of our health education and IEC materials to be used for the intervention.
Data management and analysis plan
Daily fieldwork activities will be recorded in a research log book and entered into EpiData version 3.1 on a weekly base by a data clerk. Data were checked for inconsistencies, errors and incompleteness before, during and after entry into the software and then were exported and analysed in SPSS version 23. Descriptive statistics were explained using counts, mean, intervals. Statistical significance were considered at p-value < 0.05 and regression analysis were used to assess associations between different variables. To assess the impact of the intervention on the different contraceptive and maternal indicators, a comparison of the pre- and post-intervention data were conducted using the Wilcoxon sign rank test.
Ethical considerations
This protocol has been read and approved by the Institutional Ethics Committee for Research on Human Health of the University
of Douala (IEC-UDo) with reference N° 2069 IEC-UD/12/2019/T. Any change in the underline protocol was forwarded first to the IEC-UDo for approval before it was executed. Administrative clearances were obtained from the Regional Delegation of Health of the South West Region and Littoral Region. A written authorization was obtained from the Director of Human Resources of the CDC. Only consenting women were included in the study and for those who were aged below 18 years, assent was obtained from their parents or legal representatives.
Trial registration
The trial is currently under-going registration at the Pan African Clinical Trials Registry (PACTR). The last correspondence with the registry was on 11 August 2020.
RESULTS
The pre-intervention study was conducted from December 2019 to February 2020 and the baseline data is presently being analysed and under consideration for publication in appropriate journals. The information obtained from the baseline study, including the different HBM constructs has been incorporated into the health education aspect of this intervention. During the first phase of study, communities and households to participate in the study and intervention were already sampled and marked out. As of now, 8 clusters (4 in Tiko and 4 in Pena Mboko CDC plantation) were sampled and five hundred (500) houses (250 in Tiko and Pena Mboko CDC camps each) were marked out for the data collection.
The first contact with the community for the purpose of the intervention was conducted in March 2020 during which health education, health facility strengthening and provision of basic contraception was done. A second, third and fourth re-enforcement and evaluation visit that was planned for June, September and December 2020 has been greatly modified with the persistence of the covid-19 pandemic. The detailed study results will be available after the completion of the study. This study is part of an academic project which is expected to be completed by June 2021.
DISCUSSION
The purpose of this study is to assess the impact of a 12 months family planning intervention on reproductive health parameters in a high maternal mortality community in Cameroon. The family planning intervention is a triad of health education on the family planning, health facility strengthening and increase community availability and accessibility of basic contraceptive methods. The impact of family planning on maternal morbi-mortality, infant morbi-mortality, financial status of family, etc. has been long reported (Brown et al., 2015; Family Planning and Maternal Health, 2015, Guttmacher Institute, 2016)must of which evidence has emanated from logical reasoning and analysis of long term family planning programs. However, intervention studies conducted in attempt to understand the direct or indirect impact of family planning on these parameters are lacking.
A limitation associated with our study design is the fact that the contribution of family planning to reduction of maternal and infant mortality is normally small and a longer time may be needed to produce a measurable impact of community family planning intervention on maternal and infant mortality and this impact is not a direct one. To address this challenge, 1) we have designed the study such that indicators of the impact of our intervention will be measured at different levels (proximal and distal indicators) so that a measurable impact on the proximal indicators may presume impact on the distal indicators in a long run 2) although according to the study design we intend to carryout end-line data analysis at the 12 months of our intervention, more distal measurements will be made if the analysis does not provide a reasonable conclusion.
CONCLUSION
Improvement in the quality of healthcare services that was supposed to be a major strategy to achieve reduction of high maternal deaths worldwide is greatly limited by lack of finances particular in the less develop countries. The use of contraceptives to reduce high risk pregnancies accounting for majority of these deaths is the most accessible strategy. This protocol is a clustered non-randomized controlled trial which aims at assessing the impact of health education, facility strengthening and family planning distribution on maternal and infant mortality in the Tiko CDC plantation camp. Eight (8) clusters and 500 households/participants were selected using simple balloting and systematic sampling respectively in both the intervention (Tiko CDC plantation camp) and control site (Pena Mboko CDC plantation camp) in a 1:1 ratio (that is 250 participants per site). Primary indicators assessed include contraceptive knowledge, perception and practice while secondary indicators are maternal and infant morbi-mortality. The pre-intervention phase has been conducted and a twelve (12) month intervention is on-going. However, the programmed timing of the different study phases of the study has been modified with the persistence of the covid-19 pandemic. The study is part of a PhD project in Public Health in the department of Public Health and Hygiene at the University of Buea, Cameroon.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGMENTS
The authors acknowledge the University of Buea for hosting this study. The assistance of the Centre for Research and Health Promotion, Buea for providing fieldworkers for the data collection is acknowledged. We remain thankful to all the participants of this study for their time and corporation.
REFERENCES
|
Assefa Y, Damme WV, Williams OD, Hill PS (2017). Successes and challenges of the millennium development goals in Ethiopia: Lessons for the sustainable development goals. BMJ Global Health 2(2):e000318. |
|
|
Assoua EN (2013). Plantations Industrielles de Bananiers au Cameroun: Le Cas des Plantations de la Region du Sud-Ouest. CIRAD. |
|
|
Brown W, Ahmed S, Roche N, Sonneveldt E, Darmstadt GL (2015). Impact of family planning programs in reducing high-risk births due to younger and older maternal age, short birth intervals, and high parity. Seminars in Perinatology 39(5):338-344. |
|
|
Charan J, Biswas T (2013). How to Calculate Sample Size for Different Study Designs in Medical Research? Indian Journal of Psychological Medicine 35(2):121. |
|
|
Chola L, McGee S, Tugendhaft A, Buchmann E, Hofman K. (2015). Scaling Up Family Planning to Reduce Maternal and Child Mortality: The Potential Costs and Benefits of Modern Contraceptive Use in South Africa. PLOS ONE 10:e0130077. |
|
|
Conde-Agudelo A, Rosas-Bermudez A, Castaño F, Norton MH (2012). Effects of birth spacing on maternal, perinatal, infant, and child health: A systematic review of causal mechanisms. Studies in Family Planning 43(2):93-114. |
|
|
Dulli LS, Eichleay M, Rademacher K, Sortijas S, Nsengiyumva T (2016). Meeting Postpartum Women's Family Planning Needs Through Integrated Family Planning and Immunization Services: Results of a Cluster-Randomized Controlled Trial in Rwanda. Global Health: Science and Practice 4(1):73-86. |
|
|
Family Planning and Maternal Health (2015). Matern. Health Task Force. |
|
|
GALLUP (2010). Improving Healthcare: A Global Challenge. Gallup.Com. |
|
|
Guttmacher Institute (2016). Family Planning Can Reduce High Infant Mortality Levels. |
|
|
Hall KS (2012). The Health Belief Model Can Guide Modern Contraceptive Behavior Research and Practice. Journal of Midwifery and Women's Health 57(1):74-81. |
|
|
Islam M, Yoshida S. (2009). MDG 5: How close are we to success? BJOG: An International Journal of Obstetrics and Gynaecology 116(1):2-5. |
|
|
Jeihooni AK, Hidarnia A, Kaveh MH, Hajizadeh E, Askari A (2016). Application of the health belief model and social cognitive theory for osteoporosis preventive nutritional behaviors in a sample of Iranian women. Iranian Journal of Nursing and Midwifery Research 21(2):131-141. |
|
|
Jones CL, Jensen JD, Scherr CL, Brown NR, Christy K, Weaver J (2015). The Health Belief Model as an Explanatory Framework in Communication Research: Exploring Parallel, Serial, and Moderated Mediation. Health Communication 30(6):566-576. |
|
|
Kimengsi JN, Lambi J, Gwan SA (2016). Reflections on the Role of Plantations in Development: Lessons from the Cameroon Development Corporation (CDC). |
|
|
Meh C, Thind A, Terry AL (2020). Ratios and determinants of maternal mortality: a comparison of geographic differences in the northern and southern regions of Cameroon. BMC Pregnancy Childbirth 20:194. |
|
|
Millennium Development Goal 5 - Results (2020). Maternity Worldwide. Saving Lives in Childbirth. |
|
|
Molitoris J (2017). The Effect of Birth Spacing on Child Mortality in Sweden, 1878-1926: The Effect of Birth Spacing on Child Mortality in Sweden, 1878-1926. Population and Development Review 43(1):61-82. |
|
|
Pierre-Marie T, Gregory H-E, Maxwell DI, Robinson EM, Yvette M, Nelson FJ (2015). Maternal mortality in Cameroon: a university teaching hospital report. Pan African Medical Journal 21(1). |
|
|
Prata N (2009). Making family planning accessible in resource-poor settings. Philosophical Transactions of the Royal Society B: Biological Sciences 364(1532):3093-3099 |
|
|
Stover J, Ross J (2010). Stover J, Ross J (2010).How increased contraceptive use has reduced maternal mortality. Maternal and Child Health Journal 14(5):687-695. |
|
|
Vetter TR, Mascha EJ (2017). Defining the primary outcomes and justifying secondary outcomes of a study: usually, the fewer, the better. Anesthesia and Analgesia 125(2):678-681. |
|
|
World Health Organization (WHO) (2006). Reproductive health indicators: guidelines for their generation, interpretation and analysis for global monitoring. World Health Organization, Geneva. |
|
|
World Health Organization (WHO) (2019). High rates of unintended pregnancies linked to gaps in family planning services: New WHO study. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


