Full Length Research Paper

ABSTRACT
The epidemiological, clinical and therapeutic outcomes of COVID-19 vary across countries from March 16th to July 30, 2020, 1805 cases were registered in Benin, and among these cases, about 36 deaths occurred. The aim of this work was to study the epidemiological and clinical features associated with the survival of people with COVID-19 in the Department of Littoral in Republic of Benin, from March to July 2020. This was an analytical cross-sectional study that involved 920 cases of COVID-19. The Kaplan Meier method was used to estimate the survival probability and the cumulative death risk in COVID-19 cases. The Cox model was able to identify associated factors with death caused by COVID-19. The median age was 37 (Q1=28; Q3=48) years ranging from 3 to 84; the sex ratio was 0.85 in women’s favor. Most of affected people had a university level of educational attainment (64.02%). The survival probability of patients was 99% 95%CI: [98.4-99.5] at seven days, and 97.7% 95%CI: [96.4-98.5] at 17 days and more. Age (RRadjusted; 95%CI: 6.29; [1.04-37.79]), educational attainment (RRadjusted; 95%CI: 0.11; [0.01-0.95]), place of treatment (RRadjusted; 95%CI: 18.70; [1.27-274.46]) and treatment received (RRadjusted; 95%CI: 238.46; [19.18-2963.77]) were significantly associated with treatment outcome. In conclusion, in the early stage of COVID-19 outreach in the Department of Littoral of Benin, a high level of education showed to be a protective factor against poor outcome of the treatment. Health education and promotion of school attendance remained key strategies to prevent disease in Benin.
Key words: COVID-19, epidemiology, survival probability, associated factors.
INTRODUCTION
Since December 2019, the world has been facing Corona Virus Disease (COVID-19),a novel coronavirus called SARS-CoV2 (Wu et al., 2020b; Kashongwe et al., 2020).
The spreading rate of the infection led the WHO to declare a public health emergency of international concern on January 30th, 2020, and a pandemic on March 11th (Ye et al., 2020).
The origin of this virus is not yet fully understood (Li et al., 2005; Yang et al., 2020). SARS-CoV2 preferentially infects respiratory tract cells, and transmission is through respiratory droplets either directly or indirectly (ECDC, 2020; Chan et al., 2020; Phan et al., 2020). The WHO estimates that 80% of cases have mild symptoms or are asymptomatic (ECDC, 2020). The most severe forms are observed primarily in vulnerable individuals due to their age (over 70 years) or associated diseases (such as high blood pressure, heart problems, diabetes, hemoglobinopathy) (Peiris et al., 2003; Ye et al., 2020).
As of July 18th, 2020, there have been 14,174,345 cases of COVID-19 in 213 countries or territories, with approximately 598,419 deaths (Dong et al., 2020). The United States, the most affected country, has nearly 3.8 million infections and more than 140,600 deaths, or about 23.7% of the total losses of the epidemic. China had about 83,622 cases and 4,634 deaths. Europe had 2,644,929 cases with about 200,000 deaths. In Oceania, 12,909 cases were recorded with 9,730 deceased (OMS, 2020).
The African continent was affected with 686,889 cases and 14,714 deaths. South Africa, which ranks fifth in the world, is the most affected African country with 337,594 cases and 4,804 deaths (Anjorin, 2020). Egypt and Nigeria followed with 86,471 and 35,464 cases with 4,188 and 772 deaths respectively (The Jerusalem Post, 2020).
In Benin, the first case was confirmed on March 16th 2020 (Chan et al., 2020). From this date to July 30th, 2020, 1805 people were infected among which 36 dead (Bonnet et al., 2020; WHO, 2021). The economic consequences of this pandemic are tremendous. According to the Economic Commission for Africa (ECA), between January and March 2020, oil products saw their prices drop by over 50% to reach their lowest level since 2003 (United Nations, 2018; Calderon et al., 2019a; United Nations, 2020). Metal prices have fallen by 20% compared its values at the end of December 2019, the Food and Agriculture Organization (FAO) food price index has lost 5% during this period, while cotton (one of Benin’s export products) fell by 26%. According to the International Monetary Fund (IMF), the COVID-19 pandemic is expected to lead to the contraction of the global economy (in terms of Gross Domestic Product – GDP), of the order of 3% in 2020, a much sharper decline than during the 2008-2009 financial crisis (24 h, 2020). The World Bank predicts that COVID-19 could lead to 50 million people in extreme poverty, including 23 million people in sub-Saharan Africa and 16 million in South Asia (Calderon et al., 2019b; Banque, 2020). Clinical trials continue for an effective COVID-19 vaccine (Matusik et al., 2020). Prevention is about the respect of barrier actions such as hand washing, wearing a mask, and social distancing at least one meter. From a therapeutic perspective, several clinical studies have been published on the effect of hydroxyl chloroquine and chloroquine in patients with COVID-19 (Colson et al., 2020; Touret and de Lamballerie, 2020; Ibáñez et al., 2020). No recommendations have been made to countries for its use. However, in the context of health emergencies, in order to reduce mortality, some jurisdictions recommend the use of these molecules (Davis et al., 2020; Sinha and Balayla, 2020; Almazrou et al., 2020). Since the epidemiological, clinical and therapeutic outcomes of COVID-19 are variable from one continent to another, and from one country to another, our study proposed an analysis of epidemiological and clinical features associated with the survival of people with COVID-19 in the Department of Littoral in Benin Republic. The thematic was inspired based on our daily experiences in the COVID-19 response. The results of our study will enable the health team of this department to reorient future response actions.
MATERIALS AND METHODS
Study framework
Our study was conducted in the Department of Littoral, also known as Cotonou, the economic capital of Benin Republic. Cotonou is located at the intersection of parallels 6°20 and 6°24 of North latitude and meridians 2°20 and 2°29 of East longitude. It is located at the southern end of Benin Republic, on the edge of the Atlantic Ocean. It extends over 10 km to the west, where it is bordered by the town of Abomey-Calavi, and over 6 km to the east, bordering the town of Sèmè-Kpodji. To the North and South, the city has two natural limits which are respectively Lake Nokoué and the Atlantic Ocean. It covers an area of 79 km² with 829,063 inhabitants in 2020. It consists of thirteen districts grouped into four health zones.
Type and study period
This was an analytical cross-sectional study of COVID-19 confirmed by Polymerase Chain Reaction (PCR) in the Department of Littoral from March 16th to July 15th, 2020.
Study population and sampling
The study population were all COVID-19 cases recorded in the Department of Littoral during the study period. We included anyone regardless of gender or age who has been diagnosed with COVID-19 and has been confirmed by PCR. Persons whose information was not complete were excluded.
Data collection techniques and tools
We did a documentary review. We used the data base of cases recorded in the Department of Littoral since the beginning of the pandemic. We extracted our base there. This database was supplemented by clinical and therapeutic information contained in the medical records of the cases.
Treatment and data analysis
Data collected were entered using Microsoft Excel 2013 and analyzed using Epi-Info 7.2.2.6 and R 3.6.1. Mapping were performed with QGIS 2.8 software. For the qualitative variables, proportions were calculated. The mean and standard deviation were determined for the quantitative variables.
To synthesize survival probabilities of follow-up, we used the survival analysis method. Thus, the event studied was death and the time studied was the duration of follow-up (in days). The Kaplan-Meier method was used to estimate the instantaneous probabilities of survival and the survival trends were compared with the Log-Rank test. Modeling using the Cox regression model was conducted to identify factors associated with death of COVID-19. The model was developed using a top-down, step-by-step approach based on p-value. Thus, the variables whose p-value was ≤ 0.20 (and forced variables) (Degnonvi et al., 2019; Anagonou et al., 2021)in the bivariate analysis were introduced into the initial model and those in the model with the highest p-value were subtracted from the model at each step. The variables used in the final model were those with a p-value < 0.05. The Crude Relative Risks (CRR) and the Adjusted Relative Risk (RR adjusted) were calculated with their 95% confident interval (95%CI) with the Cox model.
Variable
Dependent variable
Therapeutic outcomes (death, healed). Death cases are looked into in the study.
Independent variables
(i) Socio-demographic characteristics: age, sex, occupation, provenance, marital status, educational attainment and nationality;
(ii) Clinical features: medical history, symptomatology;
(iii) Processing variables: start date of treatment, place of treatment, type of treatment received.
Ethical concerns
We submitted and obtained the approval of the Public Health National Direction of the Ministry of Health of Benin, for the study. The data were treated with strict respect for confidentiality and anonymity.
RESULTS
Epidemiological characteristics
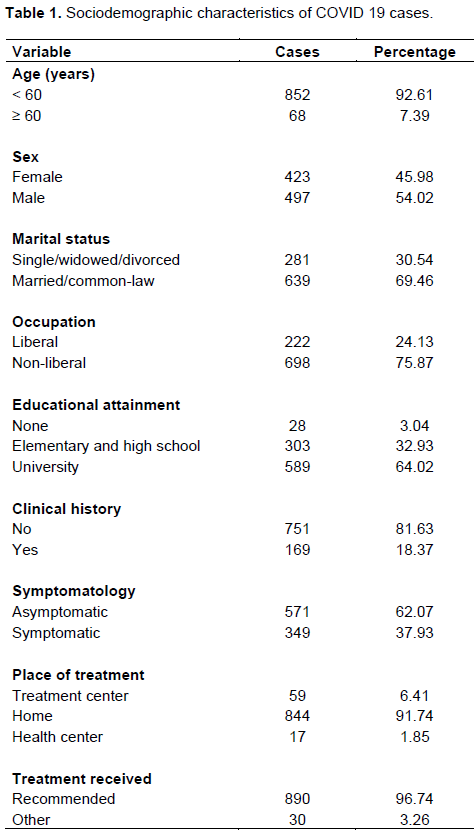
Between March 16th to July 15th 2020 (from the 12th to the 29th epidemiological weeks) 1,243 cases were confirmed with positive for PCR, of which 920 cases met the inclusion criteria. The median age was 37 years (Q1=28; Q3=48) ranging from 3 to 84; the sex ratio was 0.85 in women’s favor. The patients aged under 60 years old represented 92.61%. The largest proportion were married (69.46%), and had a non-liberal occupation (75.87%); 64.02% of people had a higher level of education; 81.63% of the cases had no clinical history. Asymptomatic persons represented 62.07%. Treatment was done at home in 91.7% of cases and 98.9% received treatment recommended by the Ministry of Health of Benin (Azithromycin plus Chloroquine) (Table 1).
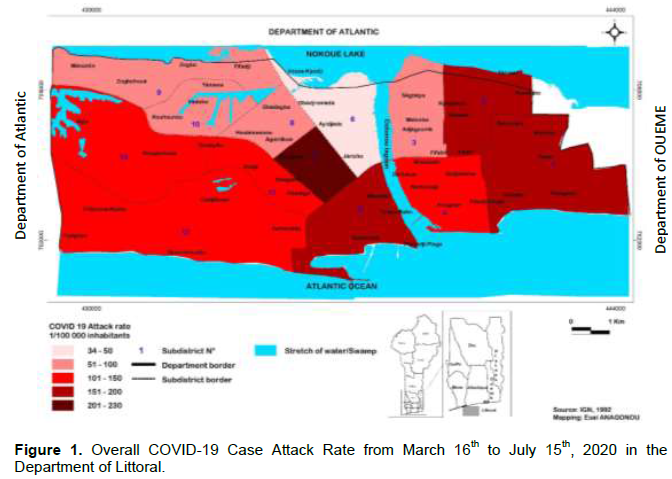
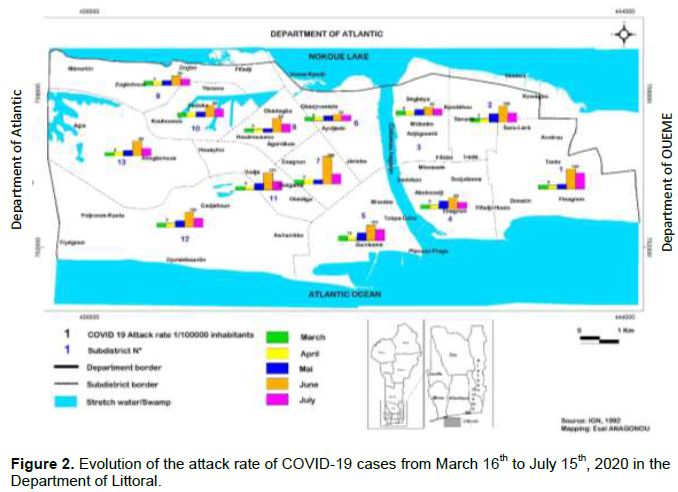
The cumulated attack rate was 150 per 100,000 inhabitants. Cases were more concentrated in the sub-district number 7 (with more than 200 cases per 100 000 inhabitants, followed by the subdistricts 1, 2 and 5 (with 151 to 200 cases per 100 000 inhabitants). The sub-districts number 4, 11, 12 and 13 had a cumulated attack rate ranging from 101 and 150 cases per 100 000 inhabitants. The less affected sub-districts were the 3, 8, 9 and 10, with a cumulated attack rate between 51 and 100 cases per 100 000 inhabitants, and the sub-district 6 with less than 50 cases per 100 000 inhabitants (Figure 1). After the alert at the 11th epidemiological week, the evolution of the disease has experienced a first phase of cases from the 11th to the 17th epidemiological week. The attack rate from March to May was then slightly the same in all districts. A second phase was observed from the 20th to the 28th epidemiological week characterized by an increase of cases. The highest attack rates were recorded in June in all sub-district. However, the one of July was higher in sub-district 1 compared to others (Figure 2).
Survival analysis
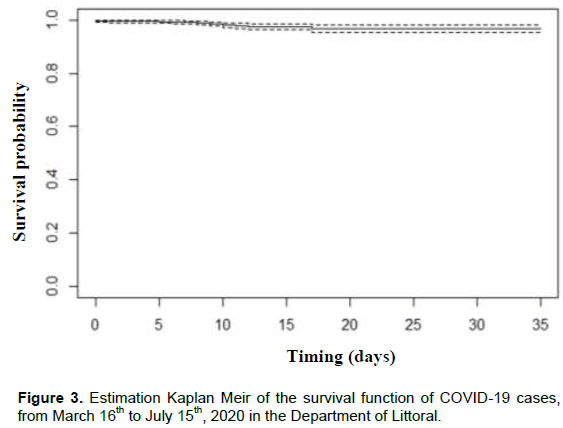
A total of 23 deaths were recorded in the period. The survival probability of patients were respectively 99% 95%CI: [98.4-99.5] at seven days, 98% 95%CI: [97.1-98.9] at 10 days and 97.7% 95%CI: [96.4-98.5] at 17 days and after (Figure 3).
Factors associated with outcomes
Bivariate analysis
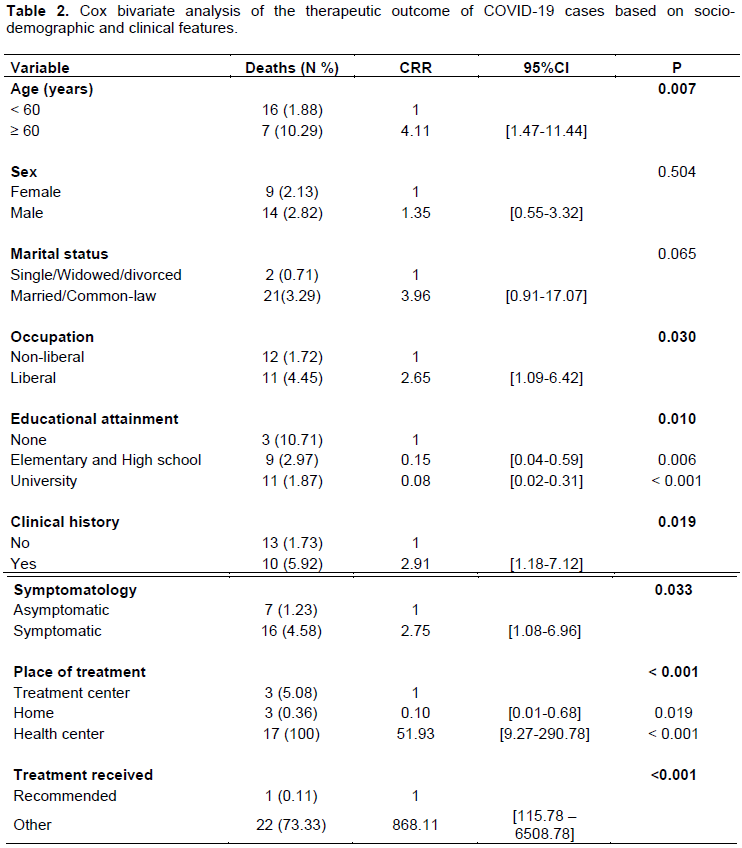
Age (Crude RR = 4.11, 95%CI: [1.47-11.44]), occupation (CRR = 2.65 95%CI: [1.09-6.42]), educational attainment(CRR = 0.08, CI 95%: [0.02-0.31]), clinical history (CRR = 2.91, 95%CI: [1.18-7.12]), symptomatology (CRR = 2.75, 95%CI: [1.08-6.96]), the place of treatment (CRR = 51.96, 95%CI: [9.27-290.78]), and treatment received (CRR = 868.11, 95%CI: [115.78-6508.78]) were significantly associated with the therapeutic outcomes (Table 2).
Multivariate analysis
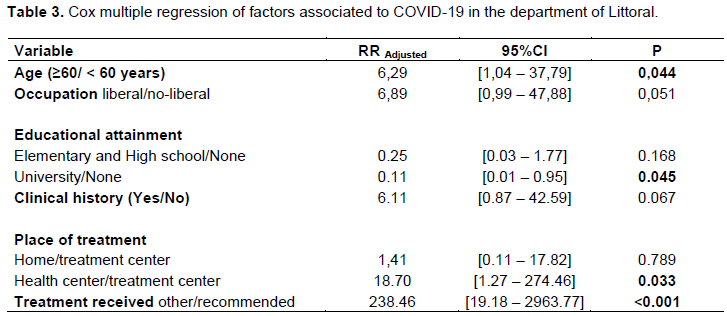
After the Cox multiple regression, the following factors remained significantly associated with treatment outcome: Age (RRadjusted; 95%CI: 6.29; [1.04-37.79]), educational attainment (RRadjusted; 95%CI: 0.11; [0.01-0.95]), place of treatment (RRadjusted; 95%CI: 18.70; [1.27-274.46]) and treatment received (RRadjusted; 95%CI: 238.46; [19.18-2963.77]) (Table 3). Thus, people over the age of 60, cared for in structures other than specialized COVID-19 treatment centers, with a treatment protocol other than the one recommended by the State, had a higher risk of death. Those with a university level were, on the other hand, protected against a poor treatment outcome.
DISCUSSION
From our study, it was found that in the early beginning of the COVID-19 outreach in Benin, the probability of survival was very high, compared to what was observed in other countries, especially in western countries. Age, occupation, education, background or clinical history, symptomatology, the place of treatment and treatment received were linked to the therapeutic outcome of COVID-19 cases in the Department of Littoral. After the multivariate analysis, only age, education, place of treatment and treatment received are independently associated with the therapeutic outcome of the treatment of COVID-19 in a case confirmed by PCR in the Department of Littoral in Benin.
Our study revealed that subjects over 60 years old had a decease relative risk of 6.29 [1.04-37.79] than those under 60-year-old. One study conducted in China found that mortality rates increase with age (Verity et al., 2020). According to this study, a modelling based on 44,672 confirmed cases worldwide, including 1,023 deaths, estimated an adjusted fatality rate of 1.4%, reaching 6.4% in the population over 60 years old. Likewise, in a study by Shi et al. (2020) multivariate analysis finding indicated that advanced age was associated with a serious illness upon admission; therefore, a death risk (Shi et al., 2020). Williamson also confirmed this fact in his OpenSAFELY study, which found that the death risk from COVID-19 by age follows an exponential curve (Williamson et al., 2020). Compared with the 50-59 age group, the risk of death from COVID-19 was 14 times lower in those younger than 40 years and 3 times lower in those 40-50 years. For those over 80, the adjusted death risk for all variables appeared multiplied by 12 compare to 50-59 years (Williamson et al., 2020).
People with elementary, secondary or higher (university) education were protected compared to the uneducated. This protection was significantly more noticeable in the higher level (university) as notified in the multivariable model. Indeed, studies of infectious diseases have shown that people with low levels of education are more likely to develop these diseases (Pouillot et al., 2007). Studies have therefore shown that education improves health because it increases the effectiveness of action, enhancing the sense of personal control that encourages and enables a healthy lifestyle (Ross and Wu, 1995; Hahn and Truman, 2015). People with a high level of education would be more accessible to awareness messages about COVID-19 and would adhere to them more easily than an uneducated individual. The recognition of the signs of the disease would be easier in educated people, which leads to an early recourse to care. In the specific case of COVID-19, at the early stage of the outreach in Benin, high level educated peoples were the one most likely to be more informed about the disease, its seriousness and actions to be taken, and appeared then to be protected against poor outcome of treatment. Since then, several communications measures have been taken by the government of Benin, to bring the information to the less educated layers of the population. Other socio-demographic factors such as ethnicity, precariousness and poverty have been identified by some studies as factors associated with COVID-19 (Williamson et al., 2020; de Lusignan et al., 2020; Peres et al., 2021).
In terms of symptomatology, our bivariate analysis found that 62.1% of cases were asymptomatic, but this variable is not statistically significant in multivariate model. The CDC estimates that the proportion of asymptomatic cases is in the order of 25% (Qin et al., 2020), while the WHO estimates that 80% of cases have mild or no symptoms (ECDC, 2020). We also noted that symptomatic individuals had 2.75 times the risk of dying from COVID-19 compared to asymptomatic. In multivariate analysis, symptomatic cases had a relative risk of 2.80 [1.1-7.04] to die compared to asymptomatic cases. The lethality rate among symptomatic cases was 4.58%. This rate is higher than 1.4% found by Wu et al. (2020a) among symptomatic cases. This could be explained by the occurrence in about 20% of infected people of a symptomatic phase with possible aggravation of respiratory symptoms leading to an acute respiratory distress syndrome (ARDS) whose management requires an intensive care in highly equipped hospitals with specialized care and monitoring. Wu et al, studies showed that fever ≥ 39°C was associated with the occurrence of ARDS (Wu et al., 2020a). Similarly, according to Zhou et al. (2020) polypnea is significantly associated with mortality (Zhou et al., 2020) due to COVID 19. These are the symptoms frequently encountered in symptomatic cases of COVID 19.
Our study showed that the risk of death was higher in health facilities than in specialized centers for the management of cases of COVID 19. In fact, unlike the health facilities, the COVID 19 case management centers have benefited the support from the Government of Benin in the acquisition of large batches of medical materials and equipment, in order to strengthen the technical platform for better patient care. This situation could explain the high number of deaths recorded in health facilities. We also found that COVID 19 cases who received other treatments had a higher relative risk of death than those who received the standard government-recommended treatment of Hydroxychloroquine and Azithromycin, demonstrating the effectiveness of this protocol when applied early and properly. Indeed, data from in vitro and in vivo studies indicated that chloroquine and hydroxychloroquine may have antiviral activity against SARS-CoV and SARS-CoV-2 and may influence the regulatory mechanisms of inflammation (Pascarella et al., 2020; Song et al., 2020)and our findings tend to confirm these assertions. This study was based on detected cases following suspicion and not on cases identified during a mass campaign. So, the concept of death has taken into account all deaths of infected individuals and not just deaths clearly attributed to COVID-19. Data were collected retrospectively. There were therefore missing data, leading to a certain lack of precision, as shown by sometimes very wide confidence intervals for certain variables in this study.
CONCLUSION
In the early stage of COVID-19 outreach in the Department of Littoral of Benin, the probability of survival was very high. Age over 60 years old, treatment delivered outside specialized centers, and the non-compliance with the government-recommended treatment protocol were associated with a higher risk of death from COVID-19 infection whereas university level of education was a protective factor. Public health policymakers must ensure that prevention activities prioritize the elderly and less educated. Health education and promotion of school attendance remained key strategies to prevent disease in Benin, but also in Africa in large.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGMENTS
The authors appreciate the contribution of Dr. Esaï Gimatal ANAGONOU and Mr. Alphonse Chabi BIAOU of the Benin National Buruli ulcer and Leprosy control Program, in the statistical analysis, the mapping, the shaping and finalization of the English version of this manuscript. They are also grateful to all members of staff and authorities of the Ministry of Health of Benin, who gave their authorization and had facilitated the data collection for this study.
REFERENCES
|
Almazrou SH, Almalki ZS, Alanazi AS, Alqahtani AM, Alghamd SM (2020). Comparing the impact of Hydroxychloroquine based regimens and standard treatment on COVID-19 patient outcomes: A retrospective cohort study. Saudi Pharmaceutical Journal 28(12):1877-1882. |
|
|
Anagonou GE, Sopoh GE, Biaou CA, Barogui YT, Wadagni AC, Gnimavo SR, Ayelo GA, Saka KE, Houezo JG, Johnson RC (2021) Environmental and behavioural factors associated with Mycobacterium ulcerans infection in the district of Lalo in Benin: A case-control study. Journal of Public Health and Epidemiology 13(2):54-63. |
|
|
Anjorin AA (2020). The coronavirus disease 2019 (COVID-19) pandemic: A review and an update on cases in Africa. Asian Pacific Journal of Tropical Medicine 13(5):199. |
|
|
Banque M (2020). Table ronde sur les conséquences économique du COVID-19 et le soutien de la Banque mondiale en faveur de l'Afrique. In: World Bank. https://www.banquemondiale.org/fr/events/2020/06/13/the-economic-impacts-of-COVID-19-and-world-bank-support-to-africa-roundtable. Accessed 23 Jul 2021 |
|
|
Bonnet E, Bodson oriane, Marcis FL, Faye A, Sambieni E, Fournet F, Boyer F, Coulibaly A, Kadio K, Diongue FB, Ridde V (2020) The COVID-19 Pandemic in Francophone West Africa: From the First Cases to Responses in Seven Countries. In Review. |
|
|
Calderon C, Kambou G, Korman V, Kubota M, Cantu Canales C (2019a). Une analyse des enjeux façonnant l'avenir économique de l'afrique. The World Bank. |
|
|
Calderon C, Kambou G, Korman V, Kubota M, Cantu Canales C (2019b). Une analyse des enjeux façonnant l'avenir économique de l'afrique. The World Bank, Washigton DC. |
|
|
Chan JF-W, Yuan S, Kok K-H, To KK-W, Chu H, Yang J, Xing F, Liu J, Yip CC-Y, Poon RW-S, Tsoi H-W, Lo SK-F, Chan K-H, Poon VK-M, Chan W-M, Ip JD, Cai J-P, Cheng VC-C, Chen H, Hui CK-M, Yuen K-Y (2020). A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: a study of a family cluster. Lancet 395(10223):514-523. |
|
|
Colson P, Rolain J-M, Lagier J-C, Brouqui P, Raoult D (2020). Chloroquine and hydroxychloroquine as available weapons to fight COVID-19. International Journal of Antimicrobial Agents 55(4):105932. |
|
|
Davis JS, Ferreira D, Denholm JT, Tong SY (2020). Clinical trials for the prevention and treatment of COVID-19: current state of play. Medical Journal of Australia 213(2):86-93. |
|
|
de Lusignan S, Dorward J, Correa A, Jones N, Akinyemi O, Amirthalingam G, Andrews N, Byford R, Dabrera G, Elliot A, Ellis J, Ferreira F, Lopez Bernal J, Okusi C, Ramsay M, Sherlock J, Smith G, Williams J, Howsam G, Zambon M, Joy M, Hobbs FDR (2020). Risk factors for SARS-CoV-2 among patients in the Oxford Royal College of General Practitioners Research and Surveillance Centre primary care network: a cross-sectional study. The Lancet Infectious Diseases 20(9):1034-1042. |
|
|
Degnonvi H, Fleuret S, Coudereau C, Gnimavo R, Giffon S, Yeramian E, Johnson RC, Marion E (2019). Effect of well drilling on Buruli ulcer incidence in Benin: a case-control, quantitative survey. Lancet Planet Health 3(8):e349-e356. |
|
|
Dong E, Du H, Gardner L (2020). An interactive web-based dashboard to track COVID-19 in real time. Lancet Infectious Diseases 20(5):533-534. |
|
|
European Centre for Disease Prevention and Control (ECDC), (2020). Coronavirus disease 2019 (COVID-19) in the EU/EEA and the UK - ninth update. 50Hahn RA, Truman BI (2015).Education Improves Public Health and Promotes Health Equity. International Journal of Health Services 45(4):657-678. |
|
|
Ibáñez S, Martínez O, Valenzuela F, Silva F, Valenzuela O (2020). Hydroxychloroquine and chloroquine in COVID-19: should they be used as standard therapy? Clinical Rheumatology 39:2461-2465. |
|
|
Kashongwe IM, Lepira F, Nani H, Situakibanza T, Rissassy J-R, Sumaili E, Kayembe JMN (2020). Manifestations cliniques de l'infection à Coronavirus SARS-Cov-2 (COVID-19) Clinical characteristics of coronavirus infection disease (COVID-19). Annales Africaines de Médecine 13(3):3685-3693 |
|
|
Li W, Shi Z, Yu M, Ren W, Smith C, Epstein JH, Wang H, Crameri G, Hu Z, Zhang H, Zhang J, McEachern J, Field H, Daszak P, Eaton BT, Zhang S, Wang L-F (2005) Bats Are Natural Reservoirs of SARS-Like Coronaviruses. Science 310(5748):676-679. |
|
|
Matusik É, Ayadi M, Picard N (2020). COVID-19, management, therapeutic and vaccine approaches. Actual Pharmacy 59(599):27-33. |
|
|
Organisation mondiale de la Santé (OMS) (2020). Estimation de la mortalité due à la COVID-19. |
|
|
Pascarella G, Strumia A, Piliego C, Bruno F, Del Buono R, Costa F, Scarlata S, Agrò FE (2020). COVID?19 diagnosis and management: a comprehensive review. Journal of Internal Medicine 288(2):192-206. |
|
|
Peiris JSM, Chu CM, Cheng VCC, Chan KS, Hung IFN, Poon LLM, Law KI, Tang BSF, Hon TYW, Chan CS, Chan KH, Ng JSC, Zheng BJ, Ng WL, Lai RWM, Guan Y, Yuen KY, HKU/UCH SARS Study Group (2003). Clinical progression and viral load in a community outbreak of coronavirus-associated SARS pneumonia: a prospective study. Lancet 361(9371):1767-1772. |
|
|
Peres IT, Bastos LSL, Gelli JGM, Marchesi JF, Dantas LF, Antunes BBP, Maçaira PM, Baião FA, Hamacher S, Bozza FA (2021). Sociodemographic factors associated with COVID-19 in-hospital mortality in Brazil. Public Health 192:15-20. |
|
|
Phan LT, Nguyen TV, Luong QC, Nguyen TV, Nguyen HT, Le HQ, Nguyen TT, Cao TM, Pham QD (2020). Importation and Human-to-Human Transmission of a Novel Coronavirus in Vietnam. New England Journal of Medicine 382(9):872-874. |
|
|
Pouillot R, Matias G, Wondje CM, Portaels F, Valin N, Ngos F, Njikap A, Marsollier L, Fontanet A, Eyangoh S (2007). Risk Factors for Buruli Ulcer: A Case Control Study in Cameroon. PLoS Neglected Tropical Diseases 1(3):e101. |
|
|
Qin C, Zhou L, Hu Z, Zhang S, Yang S, Tao Y, Xie C, Ma K, Shang K, Wang W, Tian D-S (2020). Dysregulation of Immune Response in Patients With Coronavirus 2019 (COVID-19) in Wuhan, China. Clinical Infectious Diseases 71(15):762-768. |
|
|
Ross CE, Wu C (1995). The Links Between Education and Health. American Sociological Review 60(5):719-745. |
|
|
Shi H, Han X, Jiang N, Cao Y, Alwalid O, Gu J, Fan Y, Zheng C (2020) Radiological findings from 81 patients with COVID-19 pneumonia in Wuhan, China: a descriptive study. The Lancet Infectious Diseases 20(4):425-434. |
|
|
Sinha N, Balayla G (2020). Hydroxychloroquine and COVID-19. Postgraduate Medical Journal 96(1139):550-555. |
|
|
Song Y, Zhang M, Yin L, Wang K, Zhou Y, Zhou M, Lu Y (2020). COVID-19 treatment: close to a cure?-a rapid review of pharmacotherapies for the novel coronavirus. International Journal of Antimicrobial Agents 56(2):106080. |
|
|
The Jerusalem Post (2020). Eswatini in Southern Africa reports first coronavirus case. In: The Jerusalem Post | JPost.com. |
|
|
Touret F, de Lamballerie X (2020). Of chloroquine and COVID-19. Antiviral Research 177:104762. |
|
|
United Nations (2018). COVID-19 in African cities impacts,responses and policies. |
|
|
United Nations (2020). Policy brief?: impact of COVID-19 in Africa. |
|
|
Verity R, Okell LC, Dorigatti I, Winskill P, Whittaker C, Imai N, Cuomo-Dannenburg G, Thompson H, Walker PGT, Fu H, Dighe A, Griffin JT, Baguelin M, Bhatia S, Boonyasiri A, Cori A, Cucunubá Z, FitzJohn R, Gaythorpe K, Green W, Hamlet A, Hinsley W, Laydon D, Nedjati-Gilani G, Riley S, van Elsland S, Volz E, Wang H, Wang Y, Xi X, Donnelly CA, Ghani AC, Ferguson NM (2020). Estimates of the severity of coronavirus disease 2019: a model-based analysis. The Lancet Infectious Diseases 20(6):669-677. |
|
|
World Health Organization (WHO) (2021). WHO Health Emergency Dashboard, WHO COVID-19 homepage. |
|
|
Williamson EJ, Walker AJ, Bhaskaran K, Bacon S, Bates C, Morton CE, Curtis HJ, Mehrkar A, Evans D, Inglesby P, Cockburn J, McDonald HI, MacKenna B, Tomlinson L, Douglas IJ, Rentsch CT, Mathur R, Wong AYS, Grieve R, Harrison D, Forbes H, Schultze A, Croker R, Parry J, Hester F, Harper S, Perera R, Evans SJW, Smeeth L, Goldacre B (2020). Factors associated with COVID-19-related death using Open SAFELY. Nature 584(7821):430-436. |
|
|
Wu C, Chen X, Cai Y, Xia J, Zhou X, Xu S, Huang H, Zhang L, Zhou X, Du C, Zhang Y, Song J, Wang S, Chao Y, Yang Z, Xu J, Zhou X, Chen D, Xiong W, Xu L, Zhou F, Jiang J, Bai C, Zheng J, Song Y (2020a). Risk Factors Associated With Acute Respiratory Distress Syndrome and Death in Patients With Coronavirus Disease 2019 Pneumonia inWuhan, China. JAMA internal medicine 180(7):934-943. |
|
|
Wu Y, Ho W, Huang Y, Jin D-Y, Li S, Liu S-L, Liu X, Qiu J, Sang Y, Wang Q, Yuen K-Y, Zheng Z-M (2020b) SARS-CoV-2 is an appropriate name for the new coronavirus. Lancet 395(10228):949-950. |
|
|
Yang Y, Peng F, Wang R, Yange M, Guan K, Jiang T, Xu G, Sun J, Chang C (2020). The deadly coronaviruses: The 2003 SARS pandemic and the 2020 novel coronavirus epidemic in China. Journal of Autoimmunity 109:102434. |
|
|
Ye Q, Wang B, Mao J, Fu J, Shang S, Shu Q, Zhang T (2020) Epidemiological analysis of COVID-19 and practical experience from China. Journal of Medical Virology 92(7):755-769. |
|
|
Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z, Xiang J, Wang Y, Song B, Gu X, Guan L, Wei Y, Li H, Wu X, Xu J, Tu S, Zhang Y, Chen H, Cao B (2020) Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet 395(10229):1054-1062. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


