ABSTRACT
In Ethiopia, abortion is illegal except in cases where the mother’s and fetal life is in danger. As such, little is known about safe abortion. This study aimed to assess proportion of safe abortion and associated factors among women who seek abortion care services in Family Health Guidance and Marie Stopes International Clinics, Dessie town, North East Ethiopia. Cross-sectional study was conducted among 422 mothers who sought abortion care services from March to May 2017. The samples were taken consecutively in the study period by considering random client flow. Bivariate and multivariable logistic regression was done. From 422 patients who got abortion care services in the study period, 265 (62.8%) practiced safe abortion. Severe health problems during pregnancy [AOR 12, 95% CI, (3.080, 48.364)], surgical method of abortion [AOR 6, 95% CI, (2.379, 14.374)] and positive attitude of the study group to safe abortion [AOR 1.9, 95% CI, (1.084, 3.182)] were potential predictors of safe abortion. It was found that while the majority of participants were coming to access safe abortion services, there are still a large number of women engaging in unsafe methods for abortion. Thus, there is need for strong pregnancy follow up and behavioral change programs towards safe abortion..
Key words: Safe abortion, Marie Stopes International Clinic, family guidance clinic, abortion care services.
Abbreviation:
WHO, World Health Organization; WU, Wollo University; CSA, Central Statistical Agency of Ethiopia; DHS, demographic health survey; FHG, family health guidance, FMOH, Federal Ministry of Health; FP, family planning; GA, gestational age; MMR, maternal mortality ratio.
Abortion is the termination of pregnancy by the expulsion of a fetus or embryo from the uterus. It can occur spontaneously due to complications or can be induced (Leveno et al., 2007). By convention, induced abortion is usually defined as pregnancy termination prior to 20 weeks for developed countries and 28 weeks for developing countries (World Health Organization (WHO), 2012). Abortion can also be classified as safe or unsafe. World Health Organization defines safe abortion as a procedure for terminating unwanted pregnancy by trained health professionals who have the necessary skills and in an environment that fulfills minimal medical standards (Sedgh et al., 2008).
Among the direct cause of maternal death in the world, unsafe abortion accounts for 8% of overall maternal deaths and as much as 25% in some countries and developing world (Gemzell et al., 2014). More than 40% of the total deaths due to unsafe abortion have occurred in Africa making it a cause of maternal mortality in the region (Tesfaye and Oljira, 2013). Reasons for procuring induced abortions are typically characterized as either therapeutic or elective (Tesfaye and Oljira, 2013). Therapeutic abortion is performed to save the life of the pregnant woman; prevent harm to the woman’s and fetal physical or mental health (Central Statistical Agency (CSA), 2012). An abortion is referred to as an elective or voluntary abortion when it is performed at the request of the woman for non-medical reasons (Federal Minister of Health (FMH), 2006).
The World Health Organization (WHO) estimates that at least 33% of all women seeking hospital care for complication related to abortion are less than 20 years of age. Since illegal abortions have high mortality and morbidity rates, legalizing abortion is highly debatable issue among health policy makers worldwide (Mpangile et al., 1992). In developing countries, the risk of death following complications of unsafe abortion procedures is several hundred times higher than that of an abortion performed professionally under safe conditions (Wilson, 1994; Khasiani and Baker, 1990).
In Ethiopia, abortion is illegal except in cases where the mother’s and fetus life is in danger, rape and incest and cannot be done with the woman request but illegal abortions are easy to obtain and widespread (Federal Minister of Health (FMOH), 2006). According to Ethiopian demographic and health survey report, unwanted and teenage pregnancy accounts for 25% (Central Statistical Agency, 2012). Knowledge and practice of safe abortion are practically important because of high rate of unwanted and teenage pregnancy (Madebo and G/Tsadik, 1993).
Even if all the above facts occurred, proportion of safe abortion, associated facilitators and barriers at abortion care health facilities have not been fully investigated in Ethiopia. So, this study provides information for local planners and policy makers as baseline to other researchers also.
Study area, study design and participants
Health facility based on cross sectional study design was conducted at Family Health Guidance and Marie Stopes International Clinics in Dessie town from March to May 2017. Dessie is Zonal city of South Wollo located in Amhara Region North East Ethiopia which is located 401 km from Addis Ababa. All women who seek abortion care services at Family Health Guidance and Marie Stopes International Clinics in Dessie town were source population and all women who got abortion care services at FHGC and Marie Stopes International Clinic in the study period were study populations. All pregnant women less than 28 weeks gestational age who attended abortion care services in FHG and Marie stops clinics during the study period were invited to participate in the study. Women who were severally ill thus could not respond and gestational age greater than 28 weeks were excluded.
Sample size and sampling procedure
A total of 422 sample size was calculated, using single population proportion formula by considering the following assumptions, proportion of safe abortion (P) 50%, confidence level (Z) 95%, precision (d) 5%, and finally by considering 10% none response rate. Family Guidance and Marie Stopes International Clinics with comprehensive abortion care facilities in Dessie town were selected purposively. The samples were taken consecutively from the study population in the study period by considering the assumption client flow in the health facility as random.
Data collection and quality control
Data by trained data collectors during exit face to face interview were collected using structured and validated close ended questionnaires in which the questionnaire was developed after reviewing different literatures (Central Statistical Agency, 2012; Federal Minister of Health (FMOH), 2006) and customized based on the study setting and objectives. It was first prepared by English and translated to local language Amharic version by language experts. Pretest was conducted on 5% calculated sample size at Gynecology and Obstetrics clinic which was not selected in the study to check validity and consistency of the tool in which necessary modifications were incorporated before commencing the actual data collection. Six BSc midwife nurses’ data collectors and two BSc nurses supervisors were trained on clarification of the questionnaire and methods of data collection.
For the purposes of this study, safe abortion was defined as termination of pregnancy initiated/induced by a skilled health care provider with proper equipment’s and in a study health facilities while unsafe abortion was defined as termination or try to terminate but failed of unwanted pregnancy either by a person lacking necessary skills or in an environment lacking minimal standard or both. Also, spontaneous abortion was defined as the unintentional expulsion of an embryo or fetus before the 24th week of gestation for developed country and before 28 weeks for developing countries.
For the purposes of this study, knowledge was measured by asking participants, seven knowledge related questions to assess their knowledge about safe abortion and developed a knowledge score (index) by using principal component analysis, taking those who had a mean score and above as good knowledge, and those who scored below the mean score as poor knowledge.
For the purposes of this study, attitude was measured by asking participants, five likely attitude related questions to assess the attitude of study participants toward safe abortion and developed attitude score (index) by using principal component analysis. We took mean and above score as having positive attitude and below mean score as having negative attitude.
In relation to this study, abortion care services were defined as women who came to FHG and Marie stops clinics to seek essential abortion care services which includes; pre abortion counseling, safe abortion to complete incomplete abortions induced by traditional healers and failed treatment of sepsis due to unsafe abortion, post abortion care and post abortion family planning after safe and unsafe abortions.
Ethical consideration
Ethical clearance was obtained from Wollo-University College of Medicine and Health Sciences ethical review committee. An official letter of co-operation was taken to the respective departments and to managers of study areas (FHG and Marie Stopes International Clinics) after both managers were accepted, where the study had been undertaken in their organizations. Informed consent was taken from study participants. Privacy and confidentiality was kept throughout the process.
Data analysis
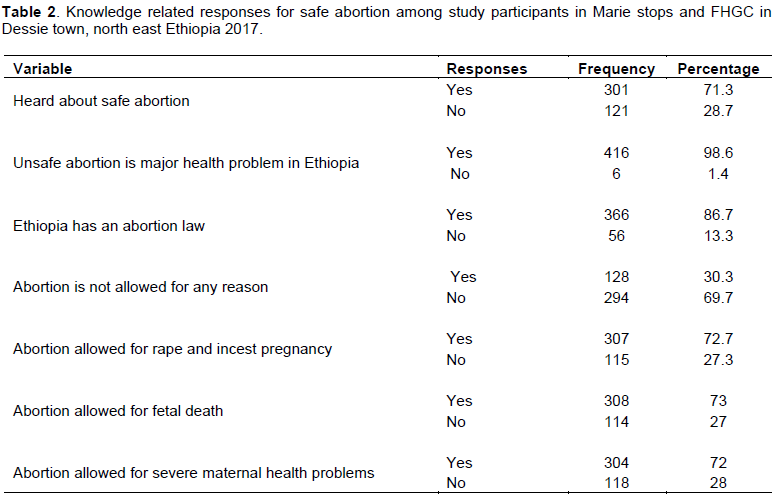
Data were first checked for completeness, edited and coded daily. The extracted data were cleaned and checked for accuracy and consistency, entered to Epi data 3.1 and exported to SPSS version 21.0 software for analysis. Descriptive analysis for continuous variables and proportion to categorical variables were done. Bivariate and multivariable logistic regression was also done. Those variables p-value less than 0.25 in bivariate were entered in multiple variable logistic regressions to identify independent factors for safe abortion utilization. Those variables less than 0.05 with 95% confidence interval had been taken as significance in the final model. media, 63 (14.9%) parents and 12 (9.8%) friends. Respondent were ask preferable gestational age to do safe abortion in which 378 (89.6%) said before three month, 35 (8.3%) said three to six month and 9 (2.1%) said any time of pregnancy. According to the study participants, 300 (71.1%) said safe abortion is permitted in their society culturally and 244 (57.8%) knew where safe abortion is done. For importance of safe abortion from the women perspective, to save mothers life was 187 (44.3%), if pregnancy is due to rape or incest was 50 (11.8%) and to prevent school disruption was 84 (20%). Major complications during abortion mentioned by participants were death (137, 32.5%), bleeding (206, 48.8%), infection (56, 13.3%) and pain (23, 5.4%) (Table 2).
Attitude towards safe abortion
Based on the composite index measurement, 162 (35.7%) of the study participants had negative attitude towards safe abortion. Of the total study participants, 412 (97.6%) agreed that safe abortion saves mothers’ lives and 151 (35.8%) women disagreed about the statement elective abortion should be legal and accessible for any reason. From total respondents, 369 (90%) agreed they were more comfortable with medical abortion than surgical abortion. Out of the total study participants, 396 (93.7%) agreed every program addressing mother’s health should include abortion care service information. Of respondents, 53 (12.5%) disagreed with the statement that “mothers choose abortion because of fetal congenital anomalies”.
Pregnancy and family planning history
From the total study participants 418 (99.1%) think family planning prevents unwanted pregnancy and 405 (96%) ever used contraceptive before pregnancy. Common contraceptive methods ever used by women were pills (113, 26.8%) injectable (189, 44.8%), implants (79, 18.7%) and condom 41 (9.7%). Among respondents 294 (69.7%) were primigravida and 382 (90.5%) were terminating a pregnancy for the first time while the rest (n=40(9.5%)) for the second time. A significant portion of participants (98, 23.2%) had habit of substance abuse and alcohol.
Proportion of safe abortion and reasons
Out of 422 clients who got abortion care services in the study period, 265 (62.8%) practiced safe abortion while the rest (157, 37.2%) practiced unsafe abortion by traditional health workers at home and came to abortion care health facilities with incomplete abortion, sepsis and for post abortion family planning. The mothers were interviewed anonyms and informed about the objective of the study to respond with the truth about unsafe abortion practice.
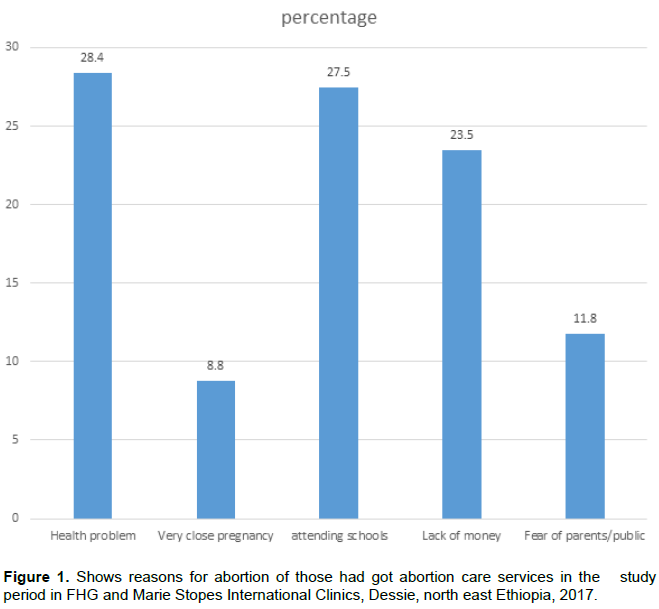
The methods of safe abortion techniques applied to terminate the pregnancy for mothers were 8.5%. Those who involved in the study were medical abortion (138, 52.0%), surgical abortion (53, 19.5%) and combination of both (74); two major reasons mentioned for safe abortion were health problems (120, 28.4%) followed by attending schools (116, 27.5%) (Figure 1).
Factors associated with safe abortion
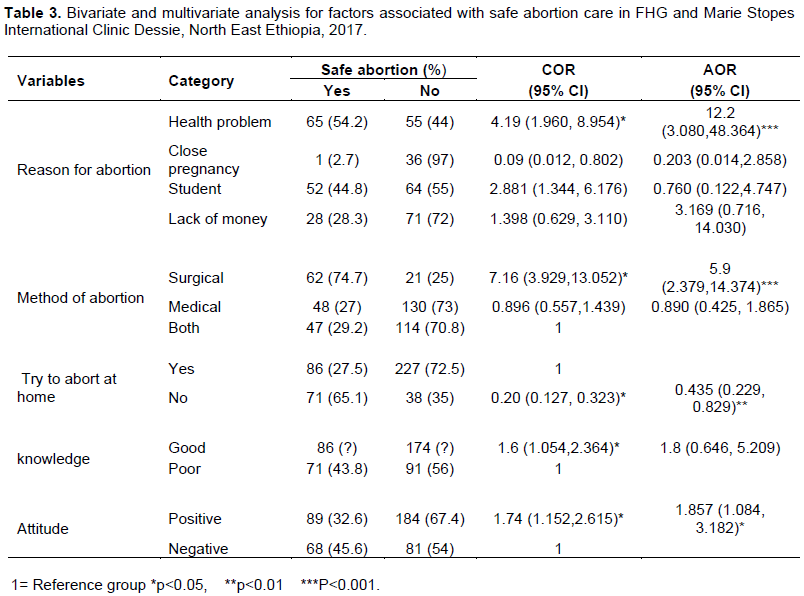
Health problems during pregnancy, surgical abortion practice, knowledge about safe abortion, and positive attitude to safe abortion were associated with safe abortion practice in the study area. Women who had reasons for abortion having severe health problems during pregnancy were 12 times more likely to practice safe abortion as compared to those women who mentioned that their reasons are due to shortage of money to care for the new born after birth [AOR 12, 95% CI, (3.080, 48.364)]. Those women who had surgical method of abortion were six times more likely to utilize safe abortion as compared to women who practiced both medical and surgical abortion [AOR 6, 95% CI, (2.379, 14.374)]. Women who tried to abort pregnancy at home were 57% less likely to practice safe abortion than who do not try at home [AOR 0.435, 95% CI, (0.229, 0.829)]. Having positive attitude toward safe abortion was found to increase the usage of safe abortion by 1.9 times as compared to those who had a negative attitude and believed abortion to be socio culturally unacceptable [AOR 1.9, 95% CI, (1.084, 3.182)] (Table 3).
Safe abortion accounted for 62.8% of abortion care services at the FHG and Marie Stopes International Clinics in Dessie town whereas, in other study, it was found that the Eastern Europe sub region has the highest safe abortion rate (98.5%) of any sub region (Madebo and G/Tsadik, 1993; Nojomi et al., 2006). When compared to this study it shows that prevalence of safe abortion in this region was low, which could probably be explained by variation in legalization of the safe abortion. A previous study done at Mizan tepi showed the prevalence of safe abortion was 1.18% in all the study groups (Andualem, 2015). There was also another study done at Wolayta Sedo University and the proportion of safe abortion was 16% (Amha et al., 2014). This may be due to difference in study period and setting and also might be because of more mothers are having information about safe abortion currently from different sources.
This study showed significant association between reasons to abortion category of having a severe health problem during pregnancy. This makes the odds of having safe abortion increased by 12 times, for this reason when compared to the reason mentioned above (lack of money to care the new born after delivery). This may be due to poor regular ANC follow up of those pregnant mothers to relive health problems during pregnancy. Surgical method of abortion was found to increase the usage of safe abortion by five times as compared to medical abortion; this could be also due to the drug side effects during medical abortion. The major reasons mentioned for safe abortion were health problems, followed by attending schools, lack of money to raise the child and fear of the public. It is consistent with the study conducted in Ghana and Addis Ababa (Mote et al., 2011; Tadesse et al., 1994).
The study also found significant association with the place of abortion; those having tried to abort at home their pregnancy was 60% less likely to practice safe abortion. This could be due to cultural influence and lack of information about safe abortion. The other facilitator for safe abortion that was identified in this study was positive attitude of the study group for safe abortion which was found to increase the usage of safe abortion by 1.8 times as compared to those have negative attitude. This study is consistent with the study at Wolayta Sedo University (Amha et al., 2014). This may be due to having a positive attitude toward safe abortion practice of the study population by improving their culture, getting enough information; improving their knowledge and understanding the complications of unsafe abortion bring behavioral changes.
Some social desirability bias may not be eliminated.
In this study, it was found that while the majority of participants in these two clinics were coming to access safe abortion services, there are still a large number of women engaging in unsafe methods for abortion. This has public health importance among those attended for abortion care services in the Family Health Guidance and Marie Stopes International Clinics. The knowledge of the study participants on safe abortion care service was good, that most participants properly stated all the conditions for safe abortion care service and its legalization in Ethiopia. Women who had negative attitude towards safe abortion and culturally unacceptable practiced less likely to practice abortion. Even if there was contraceptive ever used report, it shows failure to proper use that leads unintended pregnancy and abortion. Health problem during pregnancy, surgical method of safe abortion and positive attitude to safe abortion were predictors to practice safe abortion.
It is recommended that sustainable extension of safe abortion care services to other public health institution which provide quality service like family planning to prevent unsafe abortion should be provided. Furthermore, support and extension of safe abortion care service to other public health facilities and creating accessibility of the service to the nearby health facility is recommended. Additionally, they should be focus on proper utilization of birth control methods through information, education, communication and attitude behavior change to safe abortion care services in the community and also strong follow up of all pregnant women to early detection of health problems and management is recommended. Lastly, it is recommended that socio cultural barriers should be explored and accessibility of safe abortion care services should be provided in the community.
The authors have not declared any conflict of interests.
REFERENCES
|
Amha A, Kalemelekot N, Tesfa M (2014). Magnitude and risk factors of abortion among regular female students in Wolaita Sodo University, Ethiopia.
|
|
|
|
Andualem H (2015). Knowledge, Attitude and Practice towards Safe Abortion among Female Students of Mizan-Tepi University, South West Ethiopia.
|
|
|
|
|
Central Statistical Agency (CSA) (2012). Ethiopia and ICF International Ethiopia Demographic and Health Survey Addis Ababa 2011. Calverton, Maryland, USA March 2012.
View.
|
|
|
|
|
Federal Minister of Health (FMH) (2006). Technical and Procedural Guidelines for Safe Abortion Services in Ethiopia. In: health Fmo, editor. Addis Ababa. pp. 74-98.
|
|
|
|
|
Gemzell-Danielsson K, Kallner HK, Faúndes A (2014). Contraception following abortion and the treatment of incomplete abortion. Int. J. Gynecol. Obstetrics 126:52-56.
Crossref
|
|
|
|
|
Khasiani S, Baker J (1990). The link between Abortion and Contraceptive Use in Kenya. Nairobi, Kenya.
|
|
|
|
|
Leveno K, Cunningham F, Alexander J, Bloom S, Casey B, Dashe J (2007). Williams's manual of Obstetrics: Pregnancy complications. McGraw Hill Professional 163:63-67.
|
|
|
|
|
Madebo T, G/Tsadik T (1993). A six month prospective study on different aspects of abortion. Ethiop. Med. J. 31(3):165-172.
|
|
|
|
|
Madebo T, G/Tsadik T (1993) A six month prospective study on different aspects of abortion. Ethiop. Med. J. 31:55-59.
|
|
|
|
|
Mote CV, Otupiri E, Hindin MJ (2011). Factors associated with induced abortion among women in Hohoe, Ghana. Afr. J. Reprod. Health 14(4).
|
|
|
|
|
Mpangile GS, Leshabari MT, Kihwele DJ (1992). Factors Associated with Induced Abortion in Public Hospitals in Dar Es Salaam, Tanzania.
|
|
|
|
|
Nojomi M, Akbarian A, Ashory-Moghadam S (2006). Burden of abortion: induced and Spontaneous abortion. Arch. Iran Med. 9(1):39-45.
|
|
|
|
|
Sedgh G, Singh S, Shah IH, Åhman E, Henshaw SK, Bankole A (2008). Induced abortion Incidence and trends worldwide from 1995 to 2008. 379(6):625-632.
|
|
|
|
|
Tadesse E, Yoseph S, Gossa A (1994). Illegal abortion in five hospitals in Addis Ababa: Ethiop. Med. J. 32:24-27.
|
|
|
|
|
Tesfaye G, Oljira L (2013). Post abortion care quality status in health facilities of Guraghe zone, Ethiopia. Reprod. Health pp. 0-35.
|
|
|
|
|
Wilson A (1994). Prepared remarks for the International Planned Parenthood Federation Conference on Unsafe Abortion and Post Abortion Family Planning in Africa. pp. 102-145.
|
|
|
|
|
World Health Organization (WHO) (2012). Safe and unsafe induced abortion: Global and regional levels and trends during 1995-2008.
|
|