Full Length Research Paper

ABSTRACT
The diagnosis of malaria in pregnancy remains a challenge due to the low parasite density and placental sequestration of Plasmodium falciparum. A field performance evaluation of a malaria diagnostic test was carried out in an intense transmission setting in Nanoro, Burkina Faso. Pregnant women with symptoms suggestive of malaria were recruited and their results compared with microscopy, the current gold standard for P. falciparum diagnosis. Overall, 60% (120/200) pregnant women were malaria positive when using RDT while 49% (98/200) were positive when using microscopy. The sensitivity, specificity, positive (PPV) and negative (NPV) predictive values were 98% (95% CI: 92.8-99.8), 76.5% (95% CI: 67-84.3), 80% (95% CI: 71.7-86.7) and 97.5% (95% CI: 91.3-99.7) respectively. The agreement between microscopy and RDT was strong (Kappa coefficient of 0.74) which is good for the test, although specificity was poor. Nevertheless, in remote settings where microscopy is unavailable, the use of this RDT can limit the over-prescription of antimalarial drugs.
Key words: Febrile pregnant women, HRP-2, RDT performance, high transmission, Burkina Faso.
INTRODUCTION
Malaria in pregnancy (MiP) is still a public health issue despite many interventions (WHO, 2015). World Health Organization (WHO) estimated that about 11 million pregnant women in moderate and high transmission sub-Saharan African countries were exposed to malaria infection in 2018 resulting in 872 000 children with low birthweight (WHO, 2019). In areas with stable transmission of P. falciparum as the most common parasite, one of the common disease outcomes of MiP are maternal anaemia and low birth weight (LBW) (WHO, 2015). Contrariwise, in unstable transmission, malaria infections are the cause of maternal and foetal deaths (Rogerson et al., 2018). In order to prevent the adverse effects of MiP, WHO recommends preventive strategies such as intermittent preventive treatment during pregnancy (IPTp), use of insecticide-treated nets and an adequate clinical case management (WHO, 2015). The latter, considered as the cornerstone for malaria control, comprises an early and adequate diagnosis using rapid diagnostic tests (RDT) or microscopy and efficient treatment. The quality of malaria diagnosis can significantly impact the burden of malaria (Berzosa, 2018). The national malaria control program recommends the confirmation of all malaria cases either microscopically or by RDT where microscopy is not available (PNLP, 2016). Malaria-infected pregnant women are known to be often asymptomatic and usually present with relatively low parasite densities, making detection by microscopy difficult (Cottrell et al., 2015). In remote African regions, with the lack of electricity or qualified microscopists, RDTs become a valuable alternative for microscopy, as they can be easily deployed. In addition, they provide an opportunity for improvement of malaria suspected cases management in health facilities (WHO, 2016). Despite these advantages, true malaria cases with low parasitemia were missed by RDTs, leading to low compliance in case of negative RDT results (Watson et al., 2019). Therefore, in this study we assess the performance of the SD Bioline Malaria Antigen P.f as an alternative to microscopy among pregnant women.
MATERIALS AND METHODS
Study site
The study was carried out at the Clinical Research Unit of Nanoro at two health centres (Nanoro and Nazoanga). Nanoro is located in the centre west of Burkina Faso around 85 km from Ouagadougou, the capital city. Malaria transmission is high, with an entomological inoculation rate (EIR) estimated at 152 potential infectious bites/person/year in 2019 (Epopa et al., 2019). Malaria transmission is seasonal with P. falciparum being the most predominant species (Ministère de la Santé., 2018).
Study design and procedures
This is a secondary analysis of a study aiming to characterize the clinical presentation of malaria in pregnancy. The study method and sample size calculation have been described in detail elsewhere (Tahita et al., 2013). Pregnant women attending antennal care (ANC) were asked to participate in the study. After a written informed consent, they were assigned either in case or control groups depending of the presence of malaria symptoms. The study was conducted during the dry and rainy seasons in order to capture the effect of seasonality.
Laboratory methods
Capillary blood was collected for malaria screening using a rapid diagnostic test, SD Bioline Malaria Antigen P.f (Standard Diagnostics, 2015). This malaria rapid diagnostic test is recommended by the national malaria control program (NMCP). It is a rapid, qualitative test for the detection of histidine-rich protein II (HRP-2) antigen of malaria P. falciparum.
Haemoglobin levels and blood smears for malaria parasite detection (microscopy) were performed as a measure of comparison. A double reading system was performed for the microscopic slides reading.
Malaria microscopists were blinded from the RDT results as well as the parasite counts of the individual microscopists. In case of discrepancy, a third independent reading was done and the final result was the mean of the two closest results.
Haemoglobin was measured using a portable spectrophotometer Hemocue Hb 201 + (Hemocue®, Angelholm, Sweden).
Patient management
At inclusion, the RDT test performed was used for the participant’s clinical management. The NMCP recommends the use of amodiaquine-artésunate (AQ-AS) (standard adult dose) to treat malaria cases. Participants in the second and third trimester of pregnancy with positive RDT were treated using the recommended antimalarial. All malaria cases during the first trimester were managed using parenteral quinine for seven days (8 mg quinine base/kg every eight hours). Pregnant women with anaemia were treated using oral ferrous sulphate (200 mg) and folic acid (0.25 mg) daily for one month. At the time of the study onset, the free health care for pregnant women and children under-five years was already implemented. A nurse was available onsite 24 h a day for better management of the study participants.
Statistical methods and definitions
Epidata 3.1 was used for entry, validation and cleaning of data while STATA.10 (STATA Corporation, College Station, TX, USA) was used for statistical analysis. Pregnant women were classified as positive or negative depending on the presence of asexual parasites. Pregnant women were classified anemic if Hb <11 g/dl. In order to assess the performance of the SD Bioline Malaria Antigen P.f, sensitivity, specificity and predictive value of the test and their respective 95% confidence intervals were estimated using expert microscopy as gold standard. Furthermore, the agreement between the microscopy and the RDT was computed using the Cohen-Kappa coefficient.
Ethical consideration
The study staffs were trained on good clinical practice and study procedures before the onset of the study. The study protocol was approved by the Institutional Ethics Committee of Centre Muraz (registration no. 005-2010/CE-CM). Informed consent was sought by the study nurses. The presence of an impartial witness attending the individual sensitization and consent processes was mandatory for illiterate pregnant women. The perceived benefit of the study to the participants was a prompt diagnosis with an adequate case management free of charge.
RESULTS
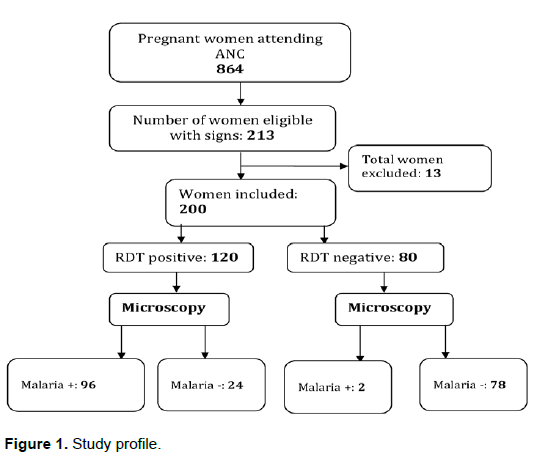
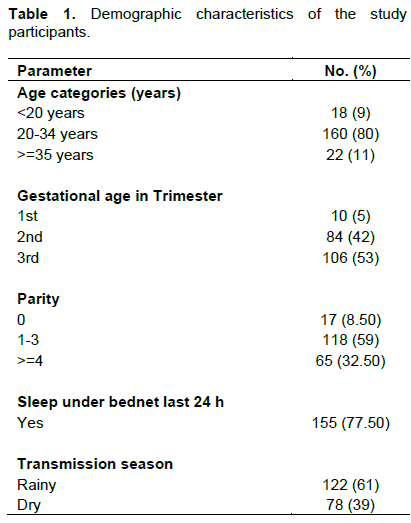
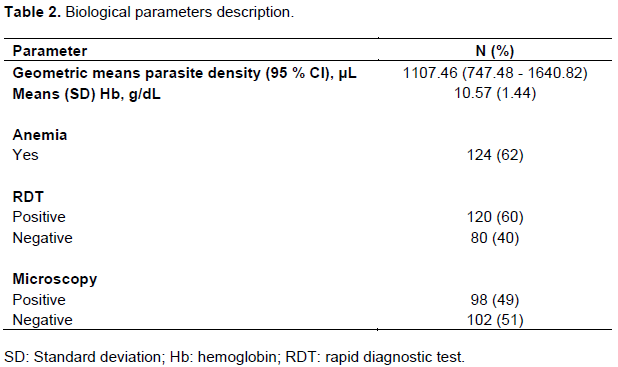
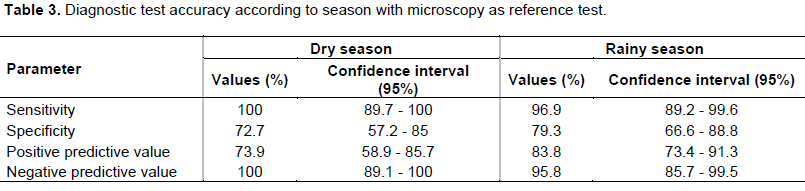
Out of a total of 864 pregnant women attending antenatal care (ANC), 200 with suspicion of malaria were included in the study as illustrated in Figure 1. The mean (standard deviation) age was 27.17 (±5.67) years and the majority of women were in the second and third trimester. Baseline characteristics were summarized in Table 1. Using microscopy, the slide positivity rate at enrolment was 49% (98/200) compared to 60% (120/200) when using RDTs (Table 2). No co-infections of P. falciparum with other plasmodial species were detected and half of the study participants had a parasite density lower or equal to 100 parasites/μL. The overall sensitivity, specificity, positive predictive value and negative predictive value of the RDT were respectively 98% (95% CI: 92.8-99.8), 76.5% (95% CI: 67-84.3), 80% (95% CI: 71.7-86.7) and 97.5% (95% CI: 91.3-99.7). The agreement between microscopy and RDT was strong (Kappa coefficient of 0.74). The RDT false-positive rate was 12% (24/200). During the low transmission season, the sensitivity and NPV of the RDT were very good (100%) but dropped in the rainy season to 96.9 and 95.8% respectively according to Table 3. The specificity went from 72.7% (95% CI 57.2 – 85) during the low transmission season to 79.3% (95% CI: 66.6-88.8) during the high transmission season (p=0.2813), and the PPV from 73.9% (95% CI: 58.9-85.7) to 83.8% (95% CI: 73.4-91.3) during low to high-transmission seasons (p=0.0881) in Table 3. The observed seasonal variations were however not statistically significant (p values > 0.05).
DISCUSSION
In this study, we determined the performance of the SD Bioline Malaria Antigen P.f rapid diagnostic test among pregnant women with suspicion of malaria infection. Almost half of the study population had malaria when using microscopy as reference. This is high compared to the result of another study conducted in pregnant women in the same region one year later with a prevalence of almost one in three (Kattenberg et al., 2012). This extensive decrease can be explained by the massive distribution of insecticide-treated materials (ITM) targeting pregnant women and children under five years implemented the same year.
During pregnancy, malaria is generally associated with substantial risks for the pregnant woman, her fetus, and the newborn (Rogerson et al., 2018). In the present study, half of the pregnant women at baseline had less than 100 parasites/μL. The same trend was also observed by Moody et al (2002). Given this high sensitivity, almost all malaria suspected cases will be accurately diagnosed and treated, validating the good choice of this RDT by the NMCP. The high sensitivity of the HRP2 based RDT in our study is comparable to those reported in previous studies carried out in Nanoro (Tinto et al., 2015; Kattenberg et al., 2012) and in West Africa (Adu-Gyasi et al., 2018; Ajumobi et al., 2015). In addition, the high negative predictive value (NPV) is an indication that very few true malaria cases might be missed, which may contribute to ensuring a rational antimalarial use (Bastiaens et al., 2014).
The SD Bioline Malaria Antigen P.f rapid diagnostic has shown low specificity due to the substantial number of false positives. Our specificity was comparable with those of others studies (Adu-Gyasi et al., 2018; Ajumobi et al., 2015). This low specificity can be explained by the persistence of the HRP2 antigens due to a delay of clearance after the treatment (Dalrymple et al., 2018; Murungi et al., 2017). Indeed, it has been demonstrated that HRP2 antigens can persist up to 28 days in circulation even after a rapid clearance of microscopically detectable parasites and therefore is not useful for the prediction of parasite responses to therapy (Kattenberg et al., 2012). In our study, pregnant women were not interviewed for history of previous malaria attacks which could have explained the persistence of HRP2 antigens. However, high specificities were seen in others studies, which can be explained either by the difference in intensity of transmission or the age of the study population (Ajumobi et al., 2015). Indeed, these studies investigated children under five years while our study was based on pregnant women.
A variation according to the season was seen, although the difference was not statistically significant. The good negative predictive value suggests a negative RDT could be seen as an indicator towards another infection. However, this needs to be further investigated.
The choice of antigen-based RDT is guided by the frequency of the species encountered in the regions. Only P falciparum mono-specific infections were seen in our study. This is in contrast with the findings of the study conducted by Pfeiffer et al. (2008) in the northwest of the country where P. malaria and P. ovale were found alone or in co-infection with P. falciparum. Nevertheless, the high rate of P. falciparum detected in our study give credit to the NMCP for choosing HRP2 based RDT for malaria diagnostics in Burkina Faso.
In 2017, it was reported that HRP-2 detecting tests were less sensitive, particularly for parasites that express little or no target antigen, resulting in a false-negative result (Kozycki et al., 2017). The high sensitivity reported in our study confirms that the HRP-2 gene deletion in not a common problem in Burkina Faso. This was confirmed by a review which showed a much lower prevalence estimates of HRP-2 genes deletions in West Africa (Cheng et al., 2014).
This study has some limitations. We did not cover the entire year which would have allowed us to capture all seasonal variations of the test performance. However, it is assumed that results obtained in the present study covering the end of the dry season and the starts of the rainy season have not biased these results. Storage conditions (humidity and temperature) and user performance are likely to influence RDTs accuracy but this was not evaluated in the present study (Watson et al., 2019). Moreover, the use of PCR could have contributed to ascertain the number of false positive and false negative tests.
CONCLUSION
The present study has shown that the SD Bioline Malaria Antigen P.f® rapid diagnostic test was able to detect almost all the malaria cases among pregnant women with suspicion of malaria due to the high sensitivity of the test. Thus, the test can be used for the diagnosis of malaria during pregnancy in the absence of qualified microscopists. The relatively low specificity is of concern as potential implications include overtreatment with an artemisinin-based combination therapy and under treatment of other causes of febrile illness.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGEMENTS
The authors are grateful to all the women who participated in this study; the entire medical laboratory and administrative staff of the Clinical Research Unit of Nanoro; and the medical staff at the CSPSs of Nanoro and Nazoanga for their valuable contribution. Thanks specifically go to Dr Kabore William for his commitment to the implementation of the study in the field, Ouedraogo Sayouba and Rebecca Czolk (Luxembourg Institute of Health) for their useful advice and inputs on the manuscript. Finally, Esther Traore is also appreciated for coordinating the slide reading.
REFERENCES
|
Adu-Gyasi D, Asante KP, Amoako S, Amoako N, Ankrah L, Dosoo D, Owusu-Agyei S (2018). Assessing the performance of only HRP2 and HRP2 with pLDH based rapid diagnostic tests for the diagnosis of malaria in middle Ghana, Africa. PloS One 13(9):e0203524. |
|
|
Ajumobi O, Sabitu K, Nguku P, Kwaga J, Ntadom G, Gitta S, Poggensee G (2015). Performance of an HRP-2 rapid diagnostic test in Nigerian children less than 5 years of age. The American Journal of Tropical Medicine and Hygiene 92(4):828-833. |
|
|
Bastiaens GJH, Bousema T, Leslie T (2014). Scale-up of malaria rapid diagnostic tests and artemisinin-based combination therapy: challenges and perspectives in sub-Saharan Africa. PLoS Medicine 11(1):e1001590. |
|
|
Cheng Q, Gatton ML, Barnwell J, Chiodini P, McCarthy J, Bell D, Cunningham J (2014). Plasmodium falciparum parasites lacking histidine-rich protein 2 and 3: a review and recommendations for accurate reporting. Malaria Journal 13:283. |
|
|
Cottrell G, Moussiliou A, Luty AJF, Cot M, Fievet N, Massougbodji A, Tuikue Ndam N (2015). Submicroscopic Plasmodium falciparum Infections Are Associated With Maternal Anemia, Premature Births, and Low Birth Weight. Clinical Infectious Diseases: An Official Publication of the Infectious Diseases Society of America 60(10):1481-1488. |
|
|
Dalrymple U, Arambepola R, Gething PW, Cameron E (2018). How long do rapid diagnostic tests remain positive after anti-malarial treatment? Malaria Journal 17(1):228. |
|
|
Epopa PS, Collins CM, North A, Millogo AA, Benedict MQ, Tripet F, Diabate A (2019). Seasonal malaria vector and transmission dynamics in western Burkina Faso. Malaria Journal 18(1):113. |
|
|
Tinto H, Sombié O, Valea I, Lankoandé F, Yara S, Lompo P, Tahita MC, Kazienga A,Ouédraogo S, Sorgho H,De Kroop M, Ravinetto R (2015). Field evaluation of SD Bioline Malaria Antigen P.f® for Plasmodium falciparum malaria diagnosis in Nanoro, Burkina Faso. African Journal of Parasitology Research 4(11):161-165. |
|
|
Kattenberg JH, Tahita CM, Versteeg IAJ, Tinto H, Traore-Coulibaly M, Schallig H DFH., Mens PF (2012). Antigen persistence of rapid diagnostic tests in pregnant women in Nanoro, Burkina Faso, and the implications for the diagnosis of malaria in pregnancy. Tropical Medicine & International Health?: TM & IH 17(5):550-557. |
|
|
Kattenberg J H, Tahita MC, Versteeg IAJ, Tinto H, Traore-Coulibaly M, D'Alessandro U, Mens PF (2012). Evaluation of antigen detection tests, microscopy, and polymerase chain reaction for diagnosis of malaria in peripheral blood in asymptomatic pregnant women in Nanoro, Burkina Faso. The American Journal of Tropical Medicine and Hygiene 87(2):251-256. |
|
|
Kozycki CT, Umulisa N, Rulisa S, Mwikarago EI, Musabyimana JP, Habimana JP, Krogstad DJ (2017). False-negative malaria rapid diagnostic tests in Rwanda: impact of Plasmodium falciparum isolates lacking hrp2 and declining malaria transmission. Malaria Journal 16(1):123. |
|
|
Ministère de la Santé (Burkina Faso). (1994). Statistiques sanitaires. Ouagadougou; 1994 Ministère de la Santé (Burkina Faso): Statistiques sanitaires. Ouagadougou; 1994. |
|
|
Moody A (2002). Rapid diagnostic tests for malaria parasites. Clinical Microbiology Reviews, 15(1):66-78. |
|
|
Murungi M, Fulton T, Reyes R, Matte M, Ntaro M, Mulogo E, Boyce RM (2017). Improving the Specificity of Plasmodium falciparum Malaria Diagnosis in High-Transmission Settings with a Two-Step Rapid Diagnostic Test and Microscopy Algorithm. Journal of Clinical Microbiology 55(5):1540-1549. |
|
|
Pfeiffer K, Some F, Müller O, Sie A, Kouyaté B, Haefeli WE, Sauerborn R (2008). Clinical diagnosis of malaria and the risk of chloroquine self-medication in rural health centres in Burkina Faso. Tropical Medicine & International Health 13(3):418-426. |
|
|
PNLP (2016). Plan stratégique national de lutte contre le paludisme 2016-2020. |
|
|
Rogerson SJ, Desai M, Mayor A, Sicuri E, Taylor SM, van Eijk AM (2018). Burden, pathology, and costs of malaria in pregnancy: new developments for an old problem. The Lancet Infectious Diseases. |
|
|
Standard Diagnostics (2015). Test rapide en une étape de détection d'antigène de la malaria Plasmodium falciparum. |
|
|
Tahita MC, Tinto H, Menten J, Ouedraogo JB, Guiguemde RT, van Geertruyden JP, D'Alessandro U (2013). Clinical signs and symptoms cannot reliably predict Plasmodium falciparum malaria infection in pregnant women living in an area of high seasonal transmission. Malaria journal 12:464. |
|
|
Watson OJ, Sumner KM, Janko M, Goel V, Winskill P, Slater HC, Parr JB (2019). False-negative malaria rapid diagnostic test results and their impact on community-based malaria surveys in sub-Saharan Africa. BMJ Global Health 4(4):e001582. |
|
|
World Health Organization (WHO) (2015). Guidelines for the treatment of malaria. 3rd ed. Geneva: World Health Organization. 2015. |
|
|
World Health Organization (WHO) (2016). Malaria microscopy quality assurance mannual, version 2. World Health Organization. 2016. |
|
|
World Health Organization (WHO) (2019). World malaria report 2019. Geneva, Switzerland. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


