Full Length Research Paper

ABSTRACT
In Burkina Faso, most reported Schistosoma infections are related to urinary schistosomiasis and focus on school-aged children. Here, we aimed to determine the prevalence of intestinal schistosomiasis and associated risk factors among patients in “Vallée du Kou” in Burkina Faso one year after treatment with praziquantel. A longitudinal study involving 980 participants of both sexes aged 6 to 80 years living in “Vallée du Kou” was carried out from February 2007 to March 2008. The participants were requested to answer to a questionnaire based on their activities and hygiene practices. At the inclusion time and during follow-up visits (1.5, 3, 6 and 12 months), stool samples were collected. Schistosoma eggs in stools were detected using the Kato-Katz test method. Patients with stool-egg-positives were treated with a single oral dose of 40 mg/kg praziquantel. Among the 980 participants enrolled, the median age was 18 years, with a minimum age of 6 and a maximum age of 80 and 57.35% were male. At baseline and at follow-up after treatment, a successive decrease in prevalence was observed from 23.10 to 13.43% at 1.5 months and to 7.42% at 3 months, with a slight recrudescence to 8.69% at six months and to 11.46% at 12 months. Swimming, an age of 6-13 years, residence, contact with a river, and defecation in an open field were the main risk factors found to be statistically significantly associated with the occurrence of Schistosoma mansoni. This study showed that one year after treatment with praziquantel, the overall prevalence of S. mansoni infection decreased. The mainly risk factors associated with infection were participant activities, residence and lack of hygiene.
Key words: Schistosoma mansoni, stools, Kato–Katz, praziquantel, prevalence, risk factors.
INTRODUCTION
Schistosomiasis represents a major parasitic disease of humans that affect approximately 200 million people in 74 countries, and the infections occur mostly in sub-Saharan Africa (Engels et al., 2002). The mortality is estimated to be almost 300,000 deaths per year in Africa (Steinmann et al., 2006; Hotez and Fenwick, 2009). Schistosomiasis is caused by a blood fluke trematode belonging to genus Schistosoma, and it is transmitted to humans through direct contact with infected fresh water (WHO, 2017; Pawar et al., 2018). Environmental, climatic, ecological and socio-economic factors drive the transmission cycle by conditioning the probability of infection in both snails and humans (Perez-Saez et al., 2015). Intestinal schistosomiasis caused by Schistosoma mansoni, and urogenital schistosomiasis caused by Shistosoma haematobium are the two endemic forms in sub-Saharan Africa (Van Der Werf et al., 2003). Intestinal schistosomiasis symptoms are diarrhoea, blood in the stool, enlargement of the liver and of the spleen; portal hypertension is common in advanced cases (WHO, 2016).
In Burkina Faso, S. mansoni and S. haematobium are present with variable levels of endemicity, but most of the reports on Schistosoma infections are related to urinary schistosomiasis (Poda et al., 2004a; Ouedraogo et al., 2016; Touré et al., 2008). In addition, previous work focused mainly on school-aged children at sentinel sites designed by the Ministry of Health (Ouedraogo et al., 2016). National programmes for schistosomiasis control are essentially oriented towards chemotherapy with praziquantel (PZQ) to school-aged children (Gabrielli et al., 2006).
In spite of efforts to control through treatment, high prevalence of reinfections have been observed, often reaching pre-treatment prevalence. For example, a study in Ethiopia reported a re-infection prevalence of 13.9% (Woldegerima et al., 2019) and another study in Niger found an overall increase in re-infection rates after treatment(Garba et al., 2013).
Distribution and magnitude of S. mansoni infection in the whole country still needs to be evaluated. Here, we determined the prevalence of intestinal schistosomiasis and associated risk factors among patients at Kou Valley in Burkina Faso treated with PQZ.
MATERIALS AND METHODS
Study area and study population
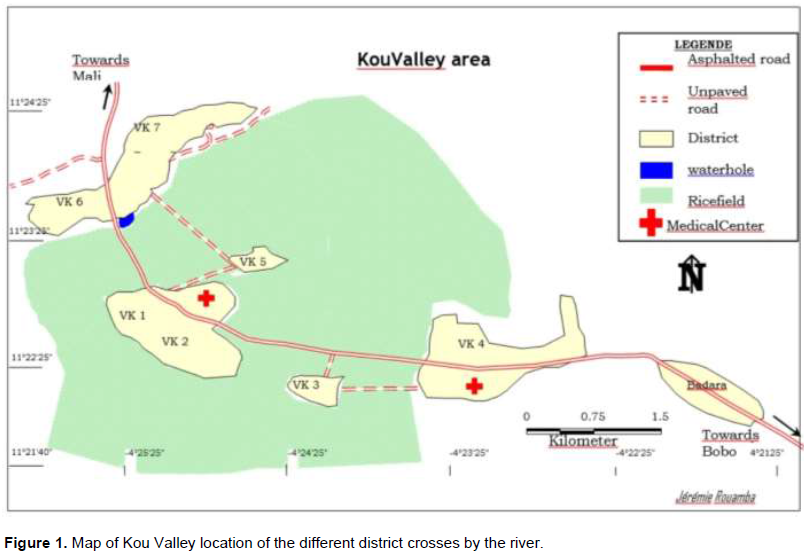
The study was carried out in “Vallée du Kou”, a rural commune located 25 km from Bobo Dioulasso (western Burkina Faso). “Vallée du Kou” is crossed by the river “Kou” which allowed the development of irrigation since 1968 for rice growing. The river crosses the seven (07) different districts of the village (Figure 1). Previous investigations reported the presence of both S. haematobium and S. mansoni in this valley (Poda et al., 2004b). Most of the population (90.3%) work in rice fields. The community uses this river for rice farming, household activities and swimming.
Study design
A longitudinal study, involving participants of both sexes aged 6 to 80 years who were living in “Vallée du Kou” was carried out from February 2007 to March 2008. Regarding the inclusion criteria, only willingness to participate was considered. Based on the study size calculation, 980 participants were enrolled. Study participants have been categorised in age groups 6-13, 14-17, 18-60 and 60-80 years. All participants were examined by trained clinicians in two health districts in the ”Vallée du Kou” (Figure 1). The first medical centre was located between VK1 and VK2, and the second was located on VK4 (Figure 1). Written informed consent forms were signed by all participants’ parents or legal guardians in the case of children. Every participant was requested to answer a questionnaire based on socio-demographic data, their activities and hygienic practices. The clinical parameters were obtained by clinicians. Fresh stool samples were collected in sterile containers and transported to laboratory at Bobo-Dioulasso “Institut de Recherche en Science de la Santé Direction Régionale de l’Ouest” (IRSS-DRO) for parasitological analysis.
Parasitological examination
Stool samples were analysed using the Kato–Katz test method (Katz and Pellegrino, 1999). The stool specimens were processed as previously described (Sorgho et al., 2005). Briefly, two slides for each stool sample were prepared using 42 mg of stool within 24 h. Stool microscopic examination and egg count were performed as previously described (Sorgho et al., 2005). Eggs were counted and the intensity of the infection was expressed as the number of eggs per gram (epg) of faeces (Gupta and Singla 2012). Eggs per gram in Kato–Katz were calculated by multiplying the egg count by the conversion factor 24, according to the World Health Organisation manual (WHO, 2003). The intensity for S. mansoni is considered as light at 1–99 epg, moderate at 100–399 epg and heavy at ≥ 400 epg.
Treatment
Patients found positive for S. mansoni eggs in stool samples at baseline (month 0) received a single dose of PZQ of 40 mg/kg and were followed up at 1.5, 3, 6 and 12 months. During the follow-up visits, all positive patients were treated with the same dose of PZQ.
Statistical analysis
The data from this study were analysed using Stata software version 12. The proportions were compared using the proportion test and the relationships between variables were measured using the chi-square test. To measure the associations between the exposure variables and the disease, we calculated the odds ratios with their 95% confidence intervals and their significance. Adjusted odds ratios were also determined using binomial logistic regression. For all statistical tests performed, a p value of less than 0.05 was considered to be statistically significant.
Ethical consideration
Before starting data collection in the field, the study protocol was approved by the local ethics committee of the “Centre Muraz” under the number: N/Ref. 016-2005/CE-CM. Participant confidentiality was maintained.
RESULTS
Socio-demographic characteristics
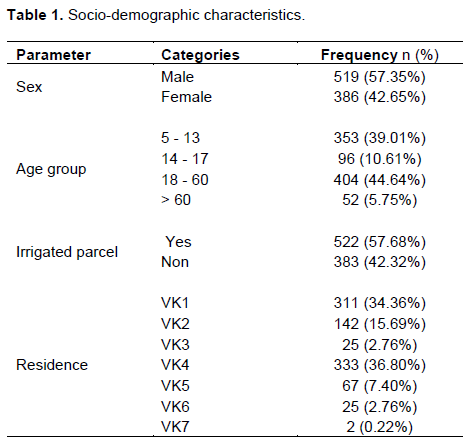
Among the 980 participants enrolled, the median age was 18 old years with minimum age of 6 and maximum 80. There were slightly more males (57.35%) than females (42.6%). Participants were slightly more in 6-13 years age group (39.01%) and 18-60 years (44.64%). About (57.78%) of participants worked on irrigated parcels; 34.36% were from district VK1, and 36.80% were from district VK4. Table 1 summarises the main socio-demographic results.
Prevalence of S. mansoni infection with socio-demographic data before treatment
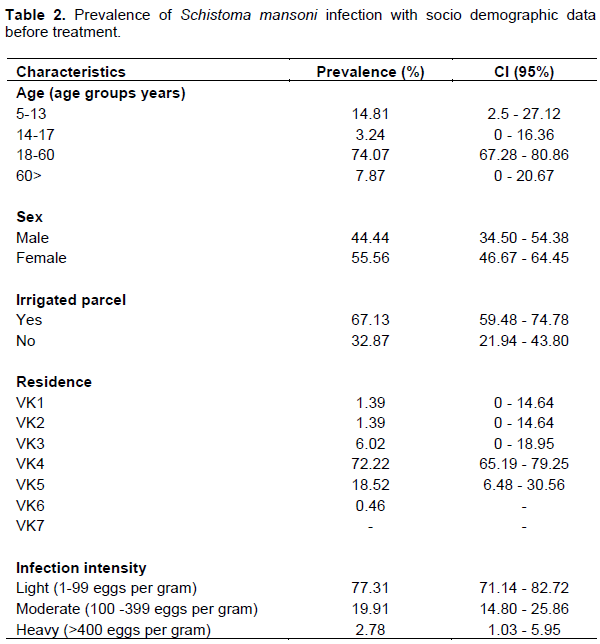
Prevalence was high [74.07% (95% CI: 68.18 - 79.96)] in age group 18 - 60 years, followed with age group 6 - 13 and low in group age 14 - 18 3.34 % (95% CI: 0.86 - 5.62) years (Table 2). The prevalence was slightly higher in female 55.56% (95% CI: 46.67 - 64.45) compared to male 44.44% (95% CI: 37.76 - 51.12). Similarly the prevalence was greater in participants working on irrigated parcel 67.13% (95% CI: 60.82 - 73.44) compared to those who did not 32.87% (95% CI: 26.66 - 39.18). The district VK 4 recorded the predominance prevalence 72.22% (95% CI: 66.20 - 78.24) (Table 2).
Socio-demographics and clinical risk factors associated with S. mansoni infection before treatment
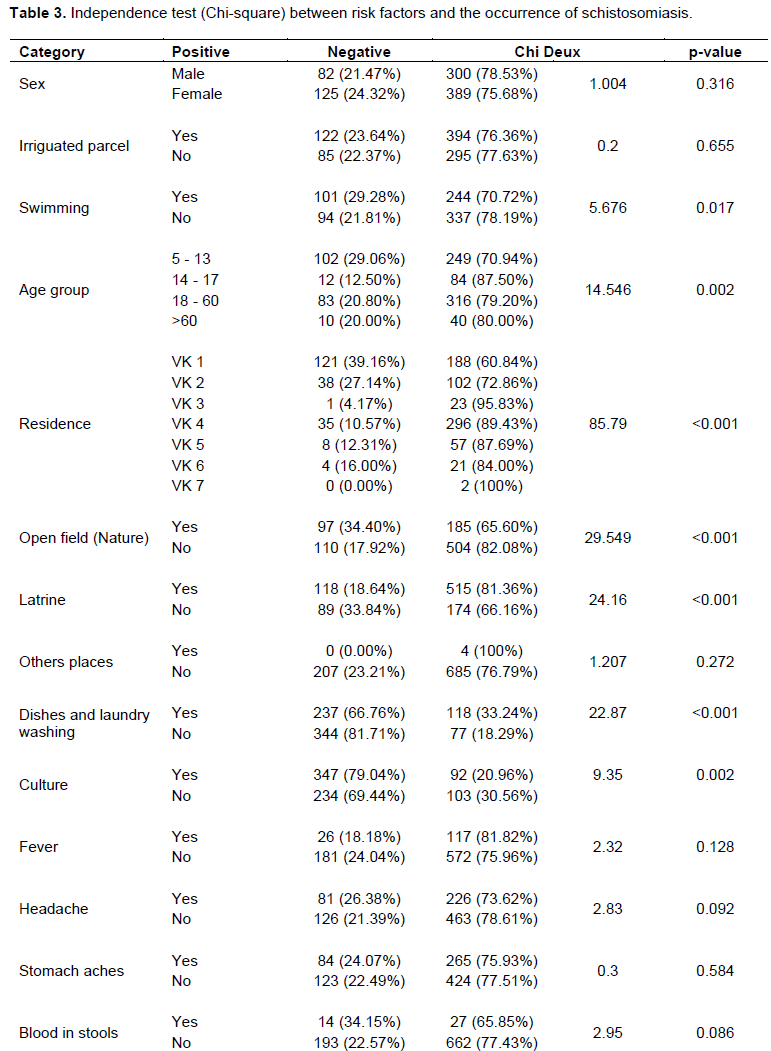
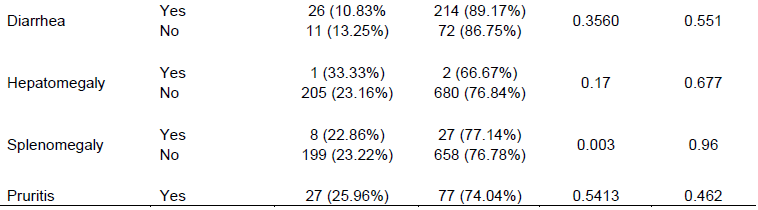
Swimming, the age group 6 - 13 years, residence, dishes and laundry washing, culture in contact with a river, and defecation in the open field and the lack of latrines, were the main risk factors found statistically significantly associated with the occurrence of S. mansoni infection based on independent Chi-square test (Table 3). Indeed, the children from this range group 6 - 13 years were more likely to swim or play in rivers. Concerning residence, district VK1 is located in an irrigated area and people living in this residence present a risk for infection with S. mansoni. Defecation in an open field and individuals who are not using latrines maintain the infection cycle through egg excretion in stools. However, most clinical factors were not significantly associated with occurrence of schistosomiasis (Table 3). Females were likely to have infection, but this observation was not statistically significant (p=0.316) (Table 3). However, household activities such as dishes and laundry washing in contact with fresh water was a significant risk for schistosomiasis (p<0.001) (Table 3).
Crude odds ratio analysis of risk factors associated with S. mansoni infection before treatment
In the modelling process, crude odds ratio analysis was first done. All the variables for which a p value was less than 0.05 had a statistical link with the occurrence of schistosomiasis. Clearly, the occurrence of schistosomiasis can be linked to age, neighbourhood of residence and to lifestyle habits such as bathing, doing laundry in waterways, culture, defecating in nature or not using latrines (Table 4).
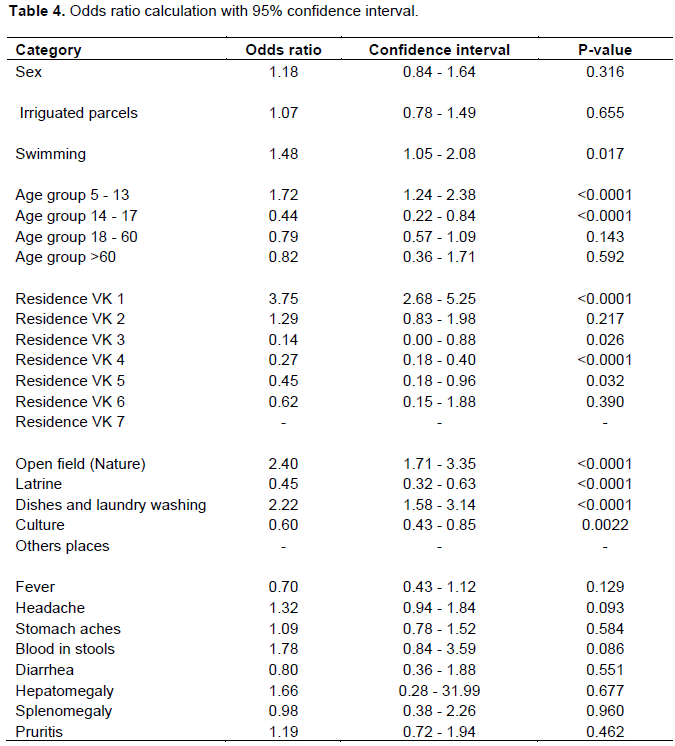
Swimming (1.48) or doing laundry (2.22) in water courses, being between 6 and 13 years old (1.72), defecating in the open (2.40) or living in the VK1 neighbourhood (3.75) were risk factors for developing schistosomiasis (Table 4). However, having age between 14 and 17 years (0.44), residing in VK3 (0.14), VK4 (0.27) or VK5 (0.45) neighbourhoods or using were protective factors for the disease (Table 4). These factors decrease the risk of developing schistosomiasis.
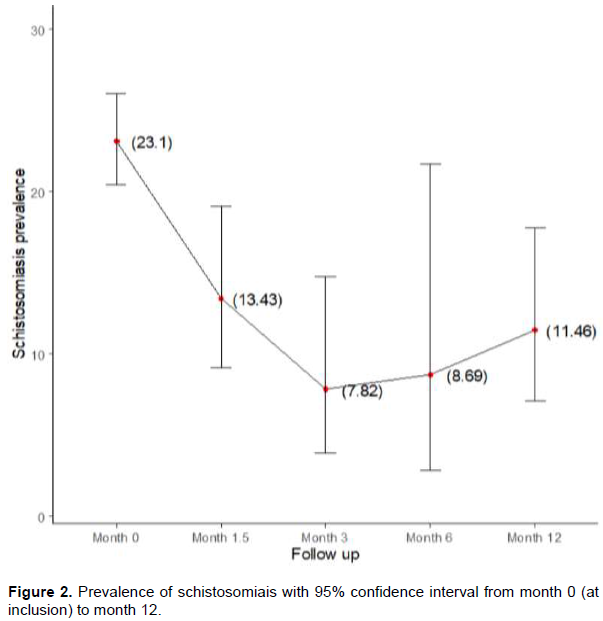
Prevalence of S. mansoni after treatment
Overall decreased prevalence was observed from baseline to the third month of follow-up then slightly increasing up to the final month of follow-up (Figure 2).
DISCUSSION
To our knowledge, this is the first published report to have investigated the effect of PZQ on S. mansoni infection one year after treatment of a cohort in “Vallée du Kou”. A previous malacological survey reported in the Kou river the presence of snail Biomphalaria pfeifferi vector of S. mansoni transmission and estimated the prevalence of intestinal schistosomiasis (Poda and Sondo, 2003). Overall, the prevalence at baseline of the infection was 23.10% and most participants came from VK1 and VK4 where the health facilities were located. This prevalence is low compared to previous findings, 45% in 2003 (Poda and Sondo, 2003) and 52.7% in 2005 (Sorgho et al., 2005), but it is similar to the 26.30% found in a sentinel site in Panamasso, a rural area of the “Hauts-Bassins” region (Ouedraogo et al., 2016). The decrease in prevalence could be related to the improvement of sanitation or health education on transmission of schistosomiasis delivered to the endemic communities.
In addition, most of the study participants (77.31%) harboured light infections as previously reported in the same locality (Sorgho et al., 2005) and “Hauts-Bassins” rural regions (Ouedraogo et al., 2016), where regular mass drug administration focused on school children might have contributed to the drop of the infection intensity. Although we reported a decrease prevalence and light infection, the persistence of the transmission of infection might be explained by the presence of a schistosomiasis vector. In addition, the main approach for schistosomiasis control in Burkina Faso was focused on school-based mass treatment in endemic areas. However, this approach leaves out other members of the community who are also infected who could contribute to maintain the transmission.
The prevalence of the infection has decreased since enrolment and initiation of the treatment with PZQ, a good indication of the PZQ efficacy on the infection (adult worms). These results are in line with previous findings in Côte d’Ivoire (19.7 to 12.8%) (Assaré et al., 2016), Sudan (59.1 to 37.4%) (Ahmed et al., 2012), and Sierra Leone (69.0 to 38.2%) (Hodges et al., 2012). However, slight re-crudescence of prevalence were observed at six months and at 12 months (Figure 2). Similar re-crudescences have been previously observed after six months of treatment in Yemen (Abaidani et al., 2016). The slight increase of prevalence could be explained either by reinfection or adult worm emerging from previous infection; because the drug is only effective on adult worms, other infections (immature worms) occurring at the time for the treatment initiation would not be impacted.
In contrast, with others studies (Sorgho et al., 2005; Tefera et al., 2020; Sitotaw et al., 2019), S. mansoni infection was more prevalent in females because of domestic activities that involve more frequent contact with the river through dishes and laundry washing.
Additionally, the high prevalence of infection observed in the age group 18-60 years represents the active age, where the exposure to the infection is high in relation to field activities. Children 6 to 13 years of age were infected through swimming and games in infested water. The risk factors associated with intestinal schistosomiasis infection including swimming, age, residency (VK1), defecation in the open field, domestic activities, and rice field work are in line with results of previous studies (Nalugwa et al., 2015; Sow et al., 2008; Utzinger et al., 2000). These risks are related to the sustained contact with the infested water in “Vallée du Kou”.
The high prevalence reported in Vk4 and Vk5 could be explained by the close contact of local people with irrigation water in the rice fields.
The main limitation of our study was the loss to follow-up at each follow-up visit. Nevertheless, to our knowledge, no further study was carried out until now in the study area despite the long time since the data were collected. Thus, data might provide some indication of the schistosomiasis situation in the study area.
CONCLUSION
The present study showed that, one year after treatment with praziquantel, the overall prevalence of S. mansoni infection had decreased but the even slight return could be an indication of reinforcement of the sanitation conditions, provision of adequate individual protective equipment and probably the addition of further mass campaigns. Finally, given the endemicity of the infection in the “Vallée du Kou”, regular surveys are warranted to follow-up with efforts to reduce the burden of the disease in these areas.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGEMENT
The authors appreciate the study participants, their parents/guardians for participating in this study.
FUNDING
This research was funded by UNDP / World Bank / WHO Special Programme for Research and Training in Tropical Diseases (TDR).
REFERENCES
|
Abaidani IA, Al-abri S, Shaban M, Ghugey SL, Al Kathery S, Al-mashikhi K, Garba A, Gabrielli AF ( 2016). Decline in transmission of Schistosomiasis mansoni in oman. Infectious Diseases of Poverty 5:112. |
|
|
Ahmed AM, El Tash LA, Mohamed EY, Adam I (2012). High levels of Schistosoma mansoni infections among school children in central sudan one year after treatment with praziquantel. Journal of Helminthology 86(2):228-232. |
|
|
Assaré RK, Yao PK, N Guessan NA, Ouattara M, Yapi A (2016). Sustaining control of Schistosoma mansoni in western côte d ' ivoire : results from a score study, one year after initial praziquantel administration. PLoS Neglected Tropical Diseases 10(1):e0004329. |
|
|
Engels DL, Chitsulo AM, Savioli L (2002). The global epidemiological situation of schistosomiasis and new approaches to control and research. Acta Tropica 82(2):139-146. |
|
|
Gabrielli AF, Touré S, Sellin B, Sellin E, Ky C, Ouedraogo H, Yaogho A, Wilson MD, Thompson H, Sanou S, Fenwick A (2006). A combined school- and community-based campaign targeting all school-age children of Burkina Faso against schistosomiasis and soil-transmitted helminthiasis: performance, financial costs and implications for sustainability. Acta Tropica 99(3):234-242. |
|
|
Garba A, Lamine MS, Barkiré N, Djibo A, Sofo B, Gouvras AN, Labbo R, Sebangou H, Webster JP, Fenwick A, Utzinger J (2013). Efficacy and safety of two closely spaced doses of praziquantel against Schistosoma haematobium and S. mansoni and re-infection patterns in school-aged children in Niger. Acta Tropica 128(2):334-344. |
|
|
Gupta SK, Singla LD (2012). Diagnostic trends in parasitic diseases of animals. In: Veterinary Diagnostics: Current Trends. Gupta RP, Garg SR, Nehra V and Lather D (Eds), Satish Serial Publishing House, Delhi pp. 81-112 |
|
|
Hodges MH, Dada N, Warmsley A, Paye J, Bangura MM, Nyorkor E, Sonnie M, Zhang Y (2012). Mass drug administration significantly reduces infection of schistosoma mansoni and hookworm in school children in the national control program in Sierra Leone. BMC Infectious Diseases 12:16. |
|
|
Hotez PJ, Fenwick A (2009). Schistosomiasis in Africa : an emerging tragedy in our new global health decade. PLoS Neglected Tropical Diseases 3(9):485. |
|
|
Katz N, Chaves A, Pellegrino JP (1999). A simple device for quantitative stool thick-smear in Schistosoma mansoni. Revista del Instituto de Medicina Tropical 14(6):397-400. |
|
|
Nalugwa A, Olsen A, Tukahebwa ME, Nuwaha F (2015). Intestinal schistosomiasis among preschool children along the shores of lake Victoria in Uganda. Acta Tropica 142:115-121. |
|
|
Ouedraogo H, Drabo F, Zongo D, Bagayan M, Bamba I, Pima T, Yago-Wienne F, Toubali E, Zhang Y (2016). Schistosomiasis in school-age children in burkina faso after a decade of preventive chemotherapy. Bulletin of the World Health Organization 94(1):37-45. |
|
|
Pawar PD, Singla LD, Kaur P and Bal MS (2018). Prevalence and associated host factors of caprine and ovine schistosomosis in Punjab, India. Ruminant Science 7(2):261-264. |
|
|
Perez-Saez J, Mari L, Bertuzzo E, Casagrandi R, Sokolow SH, De Leo GA, Mande T, Ceperley N, Froehlich JM, Sou M, Karambiri H, Yacouba H, Maiga A, Gatto M, Rinaldo A (2015). A theoretical analysis of the geography of schistosomiasis in Burkina Faso highlights the roles of human mobility and water resources development in disease transmission. PLoS Neglected Tropical Diseases 9(10):e0004127 |
|
|
Poda JN, Traoré A, Sondo BK (2004a). L'endémie bilharzienne au Burkina Faso. Bulletin de La Societe de Pathologie Exotique 97(1):47-52. |
|
|
Poda JN, Wango SP, Sorgho H, Dianou D (2004b). Evolution récente des schistosomoses dans le complexe hydroagricole du sourou au Burkina Faso Bulletin de La Societe de Pathologie Exotique 97(1):15-18. |
|
|
Poda JN, Sondo B (2003). Influence des hydro-aménagements sur la distribution des bilharzioses et de leurs hôtes intermédiaires au Burkina Faso. Cahiers Santé 13:49-53 |
|
|
Sitotaw B, Mekuriaw H, Damtie D (2019). Prevalence of intestinal parasitic infections and associated risk factors among Jawi primary school children, Jawi town, north-west Ethiopia. BMC Infectious Diseases 19 (1):1-10. |
|
|
Sorgho H, Bahgat M, Poda JN, Song W, Kirsten C, Doenhoff MJ, Zongo I, Ouédraogo JB, Ruppe A ( 2005). Serodiagnosis of Schistosoma mansoni Infections in an Endemic Area of Burkina Faso: Performance of Several Immunological Tests with Different Parasite Antigens. Acta Tropica 93(2):169-180. |
|
|
Sow S, Polman K, Vereecken K, Vercruysse J, Gryseels B, de Vlas SJ (2008). The role of hygienic bathing after defecation in the transmission of Schistosoma mansoni. Transactions of the Royal Society of Tropical Medicine and Hygiene 102(6):542-547. |
|
|
Steinmann P, Jennifer K, Robert B, Tanner M, UtzingerJ (2006). Schistosomiasis and Water Resources Development: Systematic Review, Meta-Analysis, and Estimates of People at Risk. Lancet Infectious Diseases 6(7):411-425. |
|
|
Tefera A, Belay T, Bajiro M (2020). Epidemiology of Schistosoma mansoni infection and associated risk factors among school children attending primary schools nearby rivers in Jimma town, an urban setting, southwest Ethiopia. Plos One 15 (2):e0228007. |
|
|
Touré S, Zhang Y, Bosqué-Oliva E, Ky C, Ouedraogo A, Koukounari A, Gabrielli AF, Sellin B, Webster JP, Fenwick A (2008). Two-year impact of single praziquantel treatment on infection in the national control programme on schistosomiasis in Burkina Faso. Bulletin of the World Health Organization 86(10):780-787. |
|
|
Utzinger J, N'Goran EK, Tanner M, Lengeler C (2000). Simple anamnestic questions and recalled water-contact patterns for self-diagnosis of Schistosoma mansoni infection among schoolchildren in western Côte d'Ivoire. American Journal of Tropical Medicine and Hygiene 62(5):649-655. |
|
|
Van Der Werf MJVD, De Vlas SJ, Brooker S, Looman CWN, Nagelkerke NJD, Habbema JDF, Engels D (2003). Quantification of clinical morbidity associated with schistosome infection in Sub-saharan Africa. Acta Tropica 86 :125-139. World Health Organization (2003). Manual of basic techniques for a health laboratory, 2nd ed World Health Organization. |
|
|
World Health Organization (WHO) (2017). Weekly Epidemiological Record Relevé Épidémiologique Hebdomadaire 92:749-760. |
|
|
World Health Organization (WHO) (2003). Manual of basic techniques for a health laboratory, 2nd ed World Health Organization. |
|
|
World Health Organization (WHO) (2016). Schistosomiasis and soiltransmitted helminthiases:number of people treated in 2015. Weekly Epidemiological Record Relevé Épidémiologique Hebdomadaire 91:585-600. |
|
|
Woldegerima E, Bayih AG, Tegegne Y, Aemero M, Ayalew Jejaw Zeleke AJ (2019). Prevalence and Reinfection Rates of Schistosoma mansoni and Praziquantel Efficacy against the Parasite among Primary School Children in Sanja Town, Northwest Ethiopia . Journal of Parasitology Research (24):3697216. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


