Full Length Research Paper

ABSTRACT
The performance of specific antibodies in a post-chemotherapy situation remains a controversial issue. Thus the study aims to investigate the variations of different immunoglobulins, IgG, IgG subclasses, IgM and IgA against Schistosoma mansoni soluble eggs antigens post-treatment and their correlation with eggs excretion. A longitudinal study was conducted on 928 participants over 5 years of age from February 2007 to March 2008 in “Vallée du Kou” in Burkina Faso, a rural area where S. mansoni is endemic. At the inclusion and during follow-up visits (post 1.5, 3, 6 and 12 months), stools and blood samples were examined for Schistosome eggs obtained from stools by the Kato-Katz test method and serum antibodies (IgM, IgA, IgG, IgG1, IgG2, IgG3, IgG4) obtained from blood by ELISA targeting the antigens of schistosome eggs. Subjects who were stool-egg-positive were treated with praziquantel in a single oral dose of 40 mg/kg. The overall prevalence of S. mansoni infection was 23.27% (216/928) with 77.32% (167/216) having a light intensity of infection. Factors associated with parasite eggs load were IgA, IgG1 and IgG4 titres. During each visit, each increase in IgA titre of 1 unit was associated with a significant reduction in parasite egg load of 50 eggs (p <0.002). The increase in IgG1 and IgG4 titres by 1 unit was associated with significant increases in the parasite egg count of 21 and 32, respectively. IgG1, IgG2 and IgG4 titres decreased significantly during the follow-up time (p<0.0001). In contrast, the titre of IgG3 increased significantly (p=<0.0001). This study showed that IgA, IgG1 and IgG4 are associated with decrease in parasite egg loads in stool and could be a good marker for treatment efficacy.
Key words: Immunoglobulins, Schistosoma mansoni, eggs, praziquantel, ELISA, kato-katz, Burkina Faso.
INTRODUCTION
Schistosomiasis remains a major neglected tropical Parasitic disease, particularly in Sub-Saharan Africa, where around 80-90% of the cases are found (LoVerde, 2019). More than 240 million people are infected in 78 countries, especially in poor settings without access to safe drinking water and adequate sanitation (Steinmann et al., 2006; Colley et al., 2014). In Burkina Faso, Schistosoma mansoni and S. haematobium are present with variable levels of endemicity. But most of the reports on Schistosoma infections are related to urinary schistosomiasis (Poda et al., 2004). S. mansoni has been initially described in the Western and Southern parts of the country (Ouedraogo et al., 2016; Poda et al., 2004).
The current global strategy recommended by the World Health Organization (WHO) to control schistosomiasis is based on preventive chemotherapy or mass drug administration in at risk populations (Assaré et al., 2016; Fenwick and Jourdan, 2020). Since 2002, treatment based on Praziquantel (PZQ) was used for schistosomiasis in endemic countries in Africa. This treatment was supported by the Schistosomiasis Control Initiative Program (WHO, 2002). In Burkina Faso, the national program was focused on children in hyper-endemic areas (Ouedraogo et al., 2016).
Praziquantel (PZQ) treatment has been reported to enhance host protective immunity by exposing parasite antigens (Harnett and Kusel, 1986; Doenhoff et al., 2008). Thus, treatment allows the host immune systems to recognize Schistosoma adult worm antigens and to develop protective immunity (Mutapi et al., 2005). In addition, previous studies have shown tremendous variation in the changes in immune responses after chemotherapy between different human populations (Mutapi, 2001). Schistosoma specific antibodies appear to play an important role in this protective immunity after treatment. Schistosoma egg antigen-based tests have proven to be more sensitive than worm antigen-based tests (Mott et al., 1987; Hamilton et al., 1999). Their performance in a post-chemotherapy situation remains a subject of debate. Some studies have shown that antibodies against Schistosoma soluble eggs antigens (SEA) decline after treatment within few months (Rabello et al., 1997; Doenhoff et al., 2004 ; Hamilton et al., 1999). Here, we aim to monitor the different immunoglobulin IgG, IgG subclasses, IgM and IgA against SEA eggs and their correlation with egg excretion.
MATERIALS AND METHODS
RESULTS
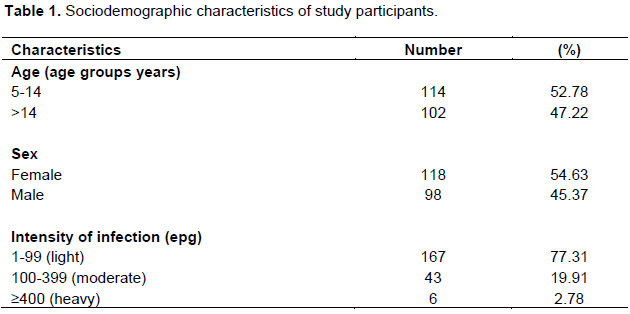
Socio-demographic characteristics of the study participants
Among the 928 participants enrolled, 216 (23.27%) were positive for S. mansoni infection based on microscopy examination. Of the 216 participants with S. mansoni infection, 52.78% were children (5-14 years) and 47.22 % were adults (>14 years). The majority of the positive participants had a light infection (77.31 %) with egp <100 (Table 1).
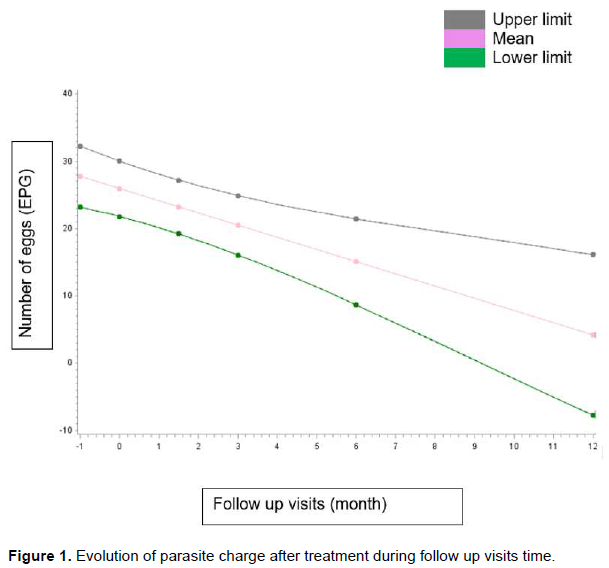
Parasite change evolution after treatment during the follow-up time
At the inclusion, the mean number of eggs was 26 ± 2.11 and during follow-up, there was a reduction of about two eggs at each visit and this reduction was statistically significant (p=0.0006) (Figure 1).
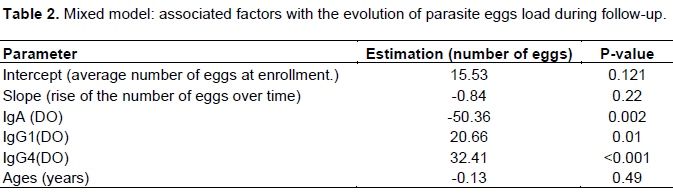
Factors associated with parasite egg load evolution during the follow-up time
The only factor associated with the reduction of the parasite egg count during follow-up was a high IgA titre. Indeed, at each visit, each increase of 1 unit in IgA titre was associated with a significant reduction in the parasite egg load of 50 eggs (p = 0.002). IgG1 and IgG4 were good markers of an increased parasite egg count. In fact, at each visit, the 1-unit increase in IgG1 and IgG4 titres was associated with a significant increase in the parasite egg count of 21 and 32, respectively (Table 2).
Immunoglobulins evolution after treatment during the follow-up time
The evolution of the different antibody titres during follow-up is shown in Figure 2. The immunoglobulins IgG, IgG1, IgG2 and IgG4 titres decreased significantly during the follow-up time (p<0.0001). In contrast, the titre of IgG3 increased significantly (p=<0.0001). The variation of IgA and IgM titres that was observed was not statically significant.

DISCUSSION
The infection intensity reported in our study included light infection levels for most participants, as previously reported, in the same locality (Sorgho et al., 2005). Our results showed a significant decrease in the parasite egg load during the follow-up time. This result was expected, supporting the well-documented effect of PZQ in the significant reduction in egg load after intervention and during follow-up (Reta and Erko, 2013; Bajiro et al., 2016).
The immunoglobulin IgA response led to a reduced egg number, whereas IgG1 and IgG4 titres increased in response to egg excretion. This observation is supported by a previous study that observed a tendency for Schistosoma whole worm antigen–IgA (anti-WWA-IgA) levels to be elevated (Fukushige et al., 2019). IgA response led to a significant reduction in the egg number during the follow-up. Some subjects might have been re-infected during the follow up, which could have induced the increased response of IgA. Indeed, the participants in this study work in rice fields, which explains the continuous exposure to re-infection. It has been shown that the immunoglobulin IgA response increases after S. mansoni egg deposition in the intestines (Poulain-godefroy et al., 1996).
In addition, the increase of IgG1 and IgG4 titres is found to be associated with significant increases in the egg number in this study, which might be related to the presence of egg excretion by the parasite. The increased titres of IgG1 and IgG4 could be a response against re-infection after treatment. In addition, PZQ kills only mature worms, so immature worms may escape treatment. Thus, the time interval between each monitoring period could allow the immature worms to mature and explain the excretion of eggs or reinfection. Previous studies have shown that IgG4 response is associated with higher parasite burdens and susceptibility to reinfection post-treatment (Mutapi, 2001; Satti et al., 1996).
Regarding the evolution on antibody response, the significantly decreased level of IgG, IgG1, IgG2 and IgG4 titres during the follow-up time is associated with the reduction of parasite egg excretion after treatment. Similar observations have been reported previously (Fukushige et al., 2019). In contrast, IgG3 titres increased after treatment during the follow-up. This result is similar to a previous observation in one year post-treatment (Abebe et al., 2001). Immunoglobulin IgG3 response was observed to kill schistosomula in the presence of activated eosinophil (Chisango et al., 2019). The IgG3 responses could be a response to the parasite stage of those that escaped the PZQ treatment. The main limitation of our study was the loss of follow up during each follow up visit. Although, to our knowledge no further study has been carried out before now on the study area despite the fact that the data had been collected for a long time. Thus, data might be some indication of schistosomiasis situation in the study area.
CONCLUSION
Praziquantel treatment reduced the S. mansoni egg load one year post-treatment. Immune responses are potentials factors associated with a significant reduction in the parasite egg load. The titres of IgA, IgG1 and IgG4 are found to be associated with parasite egg load and could be a good marker for treatment efficacy.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGMENTS
This research was funded by UNDP / World Bank / WHO Special Programme for Research and Training in Tropical Diseases (TDR). The authors would like to thank the district health workers at Kou Valley, and also the school and local community at Kou Valley.
REFERENCES
|
Abebe F, Gaarder PI, Petros B, Gundersen SG (2001). Age- and sex-r5elated differences in antibody responses against Schistosoma Mansoni soluble egg antigen in a Cohort of school children in Ethiopia. APMIS 109:816-24. |
|
|
Assaré RK, Tian-Bi YT, Yao PK, N'Guessan NA, Ouattara M, Yapi A (2016). Sustaining control of Schistosoma mansoni in Western Côte d ' Ivoire : results from a score Study , One Year after Initial praziquantel administration. PLoS Neglected Tropical Diseases 10(1):e0004329. |
|
|
Bajiro M, Dana D, Ayana M,l Emana D, Mekonnen Z, Zawdie B, Garbi A, Kure A, Zeynudin A (2016). Prevalence of Schistosoma Mansoni infection and the therapeutic efficacy of praziquantel among school children in Manna District, Jimma Zone, Southwest Ethiopia. Parasites and Vectors 9(1):4-9. |
|
|
Chisango TJ, Ndlovu B, Vengesai A, Nhidza AF, Sibanda EP, Zhou D, Mutapi F, Mduluza T (2019). Benefits of annual chemotherapeutic control of schistosomiasis on the development of protective immunity. BMC Infectious Diseases 19(1):219. |
|
|
Colley DG, Amaya LB, Secor WE, King CH (2014). Human schistosomiasis. The Lancet 383 (9936):2253-2264. |
|
|
Doenhoff MJ, Chiodini PL, Hamilton JV (2004). Specific and Sensitive Diagnosis of Schistosome Infection: Can It Be Done with Antibodies?" Trends in Parasitology 20(1):35-39. |
|
|
Doenhoff MJ, Cioli D, Utzinger J (2008). Praziquantel: Mechanisms of Action, Resistance and New Derivatives for Schistosomiasis. Current Opinion in Infectious Diseases 21:659-667. |
|
|
Fenwick A, Jourdan P (2020). Schistosomiasis elimination by 2020 or 2030 ? International Journal for Parasitology 46(7):385-388. |
|
|
Fukushige M, Mutapi F, Woolhouse MEJ (2019). Population Level Changes in Schistosome-Specific Antibody Levels Following Chemotherapy. Parasite Immunology 41(1):e12604. |
|
|
Gupta SK, Singla LD (2012). Diagnostic trends in parasitic diseases of animals. In: Veterinary Diagnostics: Current Trends. Gupta RP, Garg SR, Nehra V and Lather D (Eds), Satish Serial Publishing House, Delhi pp. 81-112 |
|
|
Hamilton JV, Klinkert M, Doenhoff MJ (1999). Diagnosis of schistosomiasis: antibody detection, with notes on parasitological and antigen detection methods. Parasitology 117(7):41-57. |
|
|
Harnett W, Kusel JR (1986). Increased exposure of parasite antigens at the surface of adult male Schistosoma mansoni exposed to praziquantel in Vitro. Parasitology 93(401-405):5. |
|
|
Katz N, Chaves A, Pellegrino PJ (1972). A simple device for quantitative stool thick-smear in Schistosoma Mansoni. Revista del Instituto de Medicina Tropical 14(6):397-400. |
|
|
LoVerde P T ( 2019). Schistosomiasis. In: Toledo R., Fried B, editors Digenetic Trematodes. Advances in Experimental Medicine and Biology, vol 1124. Springer: Cham pp. 45-70. |
|
|
Mott KE, Dixon H, Carter CE, Garcia E, Ishii A, Matsuda H, Mitchell G, Owhashi M, Tanaka H, Tsang VC (1987). Collaborative study on antigens for ammunodiagnosis of Schistosoma japonicum infection. Bulletin of the World Health Organization 65(2):233-244. |
|
|
Mutapi F (2001). Heterogeneities in anti-Schistosome humoral responses following chemotherapy. Trends in Parasitology 17(11):518-524. |
|
|
Mutapi F, Burchmore R, Mduluza T, Foucher A, Harcus Y, Nicoll G, Midzi N, Turner CM, Maizels RM (2005). Praziquantel treatment of Individuals exposed to Schistosoma haematobium enhances serological recognition of defined parasite antigens. The Journal of Infectious Diseases 192(6):1108-1118. |
|
|
Ouedraogo H, Drabo F, Zongo D, Bagayan M, Bamba I, Pima T,Yago-Wienne F, Toubali E, Zhang Y ( 2016). Schistosomiasis in school-age children in Burkina Faso after a decade of preventive chemotherapy. Bulletin of the World Health Organization 94(1):37-45. |
|
|
Pawar PD, Singla LD, Kaur P, Bal MS (2018). Prevalence and associated host factors of caprine and ovine schistosomosis in Punjab, India. Ruminant Science 7(2):261-264. |
|
|
Poda JN, Traoré A, Sondo BK (2004). L'endémie Bilharzienne Au Burkina Faso. Bulletin de La Societe de Pathologie Exotique 97(1):47-52. |
|
|
Poulain-godefroy O, Gaubert S, Lafitte S, Grzych JM (1996). Immunoglobulin A response in murine schistosomiasis : Stimulatory role of egg antigens. Infection and Immunity 64(3):763-768. |
|
|
Rabello ALT, Garcia MMA, Pinto Da Silva, Rocha RS, Katz N ( 1997). Humoral immune responses in patients with acute Schistosoma mansoni infection who were followed up for two years after treatment. Clinical Infectious Diseases 24(3):304-308. |
|
|
Reta B, Erko B ( 2013). Efficacy and side effects of praziquantel in the treatment for Schistosoma mansoni infection in school children in Senbete Town, Northeastern Ethiopia. Tropical Medicine and International Health 18(11):1338-1343. |
|
|
Satti MZ, Lind P, Vennervald BJ, Sulaiman SM, Daffalla AA, Ghalib HW (1996). Specific immunoglobulin measurements related to exposure and resistance to Schistosoma mansoni infection in Sudanese canal cleaners. Clinical and Experimental Immunology 106(1):45-54 |
|
|
Sorgho H, Bahgat M, Poda JN, Song W, Kirsten C, Doenhoff MJ, Zongo I, Ouédraogo JB, Ruppe A ( 2005). Serodiagnosis of Schistosoma mansoni infections in an endemic area of Burkina Faso: Performance of several immunological tests with different parasite antigens. Acta Tropica 93(2):169-180. |
|
|
Steinmann P, Jennifer K, Robert B, Tanner M, UtzingerJ (2006). Schistosomiasis and water resources development: Systematic review, meta-analysis, and estimates of people at risk. Lancet Infectious Diseases 6(7):411-425. |
|
|
World Health Organization (2002). Prevention and control of schistosomiasis and soil-transmitted helminthiasis: report of WHO expert committee. Genova, Switzerland. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


