Full Length Research Paper

ABSTRACT
Intermittent preventive treatment of malaria during pregnancy with sulfadoxine-pyrimethamine (IPTp-SP) is recommended to prevent maternal and neonatal adverse outcomes. This study aimed to assess IPTp-SP coverage in mothers delivering in six health facilities and factors associated with placental malaria and low birth weight. A multicenter, cross-sectional survey was conducted in Côte d’Ivoire from March to October 2017. Regression logistics were used to study factors associated with placental malaria, IPTp-SP uptake, and LBW (<2.500 grams). Out of all the enrolled participants (n=1236), 632 (51.1) received three or more doses of SP while 288 (23.3%), 221 (17.9%) and 95 (7.7%) received two respectively, one and none dose of SP. Uptake of ≥ 3 doses varied significantly (p < 0.001) according to study site, number of ANC visits and profession. Regression analysis identified primigravidae, single dose IPTp-SP, or no IPTp-Sp as factors associated with placental malaria. IPTp-SP coverage observed in this study was low compared to WHO recommendation and contrasted with the high antenatal care (ANC) visits. There is a need for further research to understand the barriers and enablers of uptake in each context in order to improve uptake of adequate IPTp-SP regimen.
Key words: Coverage, Effectiveness, Malaria, Pregnancy, IPTp-SP, Côte d’Ivoire.
INTRODUCTION
Malaria in pregnancy is a major public health challenge, affecting about 50 million women per year and presents significant risks for the pregnant woman, the developing fetus and the newborn infant (WHO, 2016). Placental malaria (PM) is associated with intrauterine growth restriction, stillbirth, and delivery of low birth weight (LBW) infants (WHO, 2016). In high-malaria transmission area, women are semi-immune, and most malaria infections in pregnancy are asymptomatic.
In areas with moderate to high transmission of Plasmodium falciparum, the World Health Organization (WHO) recommends a package of interventions for controlling malaria and its effects during pregnancy, which includes the promotion and use of insecticide-treated nets (ITNs), the administration during pregnancy of intermittent preventive treatment with sulfadoxine-pyrimethamine (IPTp-SP), and appropriate case management through prompt and effective treatment of malaria in pregnant women (WHO, 2004, 2012). The WHO policy on IPTp-SP considers three and more doses of SP given monthly for intermittent preventive treatment in pregnancy (IPTp-SP 3+) to be optimal, and less than three doses as sub-optimal (Kayentao et al., 2013; WHO, 2018).
Full doses of IPTp-SP are proven to be efficacious and cost-effective strategy delivered through the antenatal care (ANC) (Quakyi et al., 2019). The key goal of the global action plan is to cover 80% of the pregnant women in malaria endemic regions receiving no less than three doses of IPTp-SP in order to reduce the complications that arise from malaria in pregnancy.
The IPTp-SP 3+ policy has been slowly but fully adopted and implemented in sub-Saharan Africa, including Côte d’Ivoire. Today, anti-malaria chemoprophylaxis for pregnant women is therefore a constant in all national malaria control programs in endemic countries. In Côte d’Ivoire a few cross-sectional studies have investigated the effectiveness of IPTp-SP previously (Vanga-Bosson et al., 2011; Toure et al., 2014, 2020). In the context of P. falciparum resistance to SP (van Eijk et al., 2019) in the country regular assessment of IPTp-SP is needed to ensure its effectiveness and efficacy to prevent malaria during pregnancy. Therefore, the aim of this study was to assess the effectiveness of IPTp-SP and its impact on maternal and neonatal birth outcomes in Côte d'Ivoire several years after its adoption. Thus, determining the coverage and effectiveness of this policy is of utmost importance to its sustainability in the country and elsewhere.
MATERIALS AND METHODS
Study sites
This study was a cross sectional study carried out at six National Malaria Control Program (NMCP) sentinel sites for malaria surveillance in Côte d’Ivoire (Abidjan, Abengourou, Man, Yamoussoukro, Korhogo, and San-Pedro). These sites have been NMCP sentinel sites for monitoring of anti-malarial efficacy and IPTp-SP effectiveness since 1996 and 2012, respectively. The criteria for selecting these sites were as followed: sentinels sites for malaria surveillance, implementation of malaria control strategies and Services offered in each site including family planning, antenatal care, delivery, postnatal care, child welfare clinic, and laboratory and pharmacy services. Abidjan is the capital of the country and selected health facilities in this urban site were Anonkoua-Koute and South Abobo facilities.
Study population
The target population was all consenting pregnant women and the study population was all postpartum women aged 15 years and more who had just delivered (< 24 h) and those that delivered at home but visited the health facility of each site for check-up.
Sample size determination
The sample size calculation was based on the estimate of a proportion of PM and LBW after IPTp implementation in previous studies (Vanga-Bosson et al., 2011). With a margin of error of ± 2% using an alpha type-1 error of 5%, at least 1224 pregnant women should be included during the study period, with a minimum of 200 women from each of the six selected sites.
Data collection and quality management
A total of six clinicians and six lab technicians were recruited and trained in data collection methods and management for 2 days, followed by one-day fieldwork. This was done to ensure the data collected were consistent across data collectors, complete and valid. The investigator monitored and supervised the data collectors throughout the data collection exercise.
Enrollment and study procedures
Consenting women who met the study inclusion criteria (singleton pregnancy, IPTp-SP history available, documented HIV negative) were enrolled at the time of delivery.
Socio-demographic characteristics data such as age, educational level, number of children, and occupation were collected directly from participants on Case Report Forms (CRFs).
In addition, data on ANC services were provided including availability or not of SP at the ANC study site, the number of tablets swallowed per dose and whether the drug was administered under supervision were collected directly from participants. For the purpose of accuracy, data on gestational age at first ANC visit, number of ANC visits during their last pregnancy, number of doses of SP taken before delivery and the gestational age at which the first dose of SP was taken, were extracted from the ANC record books of the participants. Other recorded information included, parity, ITNs use, history of malaria illness during pregnancy, and the use of hematinic and anthelmintic drugs.
Sample collection and examination
Blood smears were made using blood collected from mother’s peripheral venous, from the maternal side of the delivered placen, and from the umbilical vein cord. side of the placenta with approximately 2 cm × 2 cm in length and width, and 1 cm in depth and were used to prepare impression smears after swabbing it on blotting paper.
Thick and thin blood smears were also prepared and stained with Giemsa. Blood slides were examined independently by two experienced laboratory technicians using a light microscope. Discrepant findings were reviewed by a third technician until consensus on positivity was reached. Malaria parasitemia from placental impression smears and placental infection status were performed).
Data analysis
Statistical analysis was performed using Stata® version 10.0 (StataCorp LP, College Station, TX, USA). The data were summarized using descriptive statistics including frequencies, percentages, means, standard deviation, median and ranges. The socio-demographic and ANC characteristics were also grouped into categories. Differences in frequencies were compared by either Chi?squared or Fisher’s exact tests as appropriate and continuous variables by Student’s t?test when the data were normally distributed. Nonparametric tests were used for non-normally distributed data. In the multivariable analysis, the factors associated with the dependent variable (LBW or PM or IPTp uptake) based on univariate analysis were included.
Outcome variables
The primary outcome was the coverage rate of IPTp-SP (3 does or more), prevalence of PM and LBW. Secondary outcomes were malaria parasites detected during pregnancy and at delivery, adverse birth outcomes (premature birth, fetal anemia, stillbirth, and spontaneous abortion).
Ethical clearance
Ethical clearance was obtained from the National Ethic Committee of Côte d’Ivoire with approval letter reference number 041/IVISHP/CNER-kp. All study participants were informed in their local language about the study objectives and procedures. For each study participant, written informed consent was obtained and the participant was free to withdraw consent at any time of the study without influencing their access to health services. All activities including sample collection, processing, and analysis were carried out as required by the committee.
RESULTS
Sociodemographic characteristics of participants
The socio-demographic characteristics of the 1,236 participants included in this analysis are presented in Table 1. The mean (± SD) age of the delivering women was 26±6.5 years.
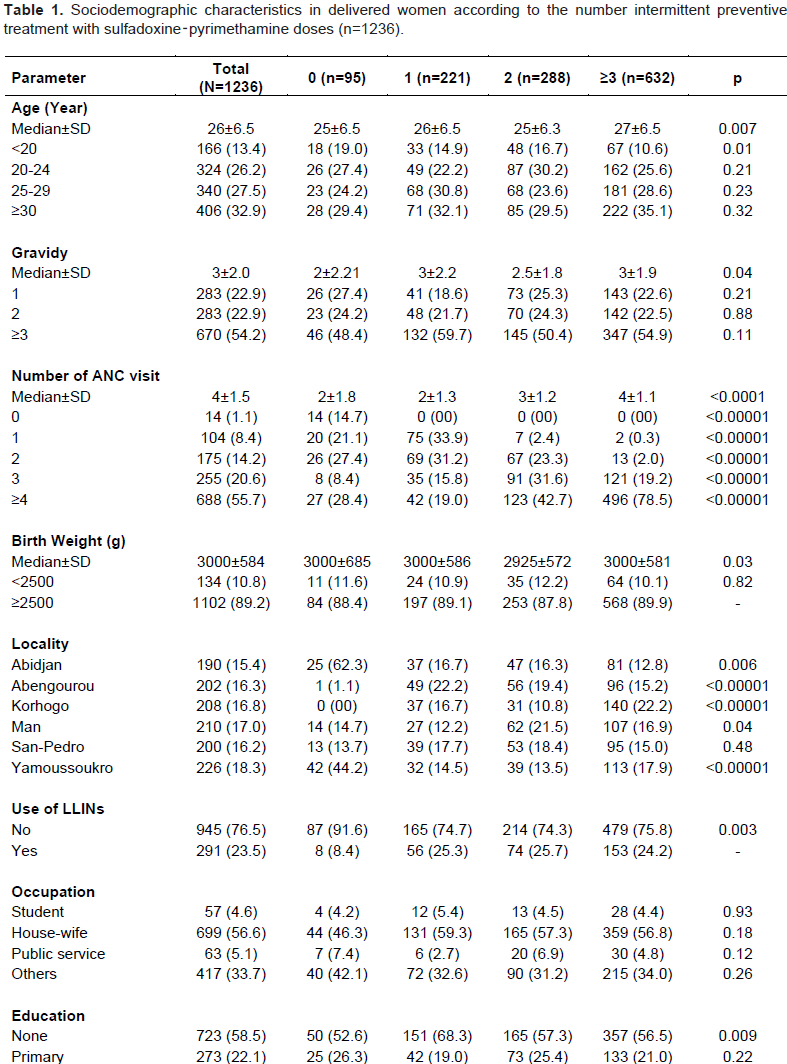

Primigravidae and multigravidae constituted 22.9 % and 54.2 % of the study participants respectively. The majority (32.9%) of the participants were 30 or more years-old followed by participants aged between 25 to less than 30 years. The number of ANC visits made ranged from 1 to 8 with a mean of 4.0 ± 1.5 visits. Most of the women had at least 4 ANC visits (55.7%) followed by 3 ANC visits (76.3%). The Overall coverage of ITN was 23.5%.
Prevalence of IPTP-SP uptake and associated factors
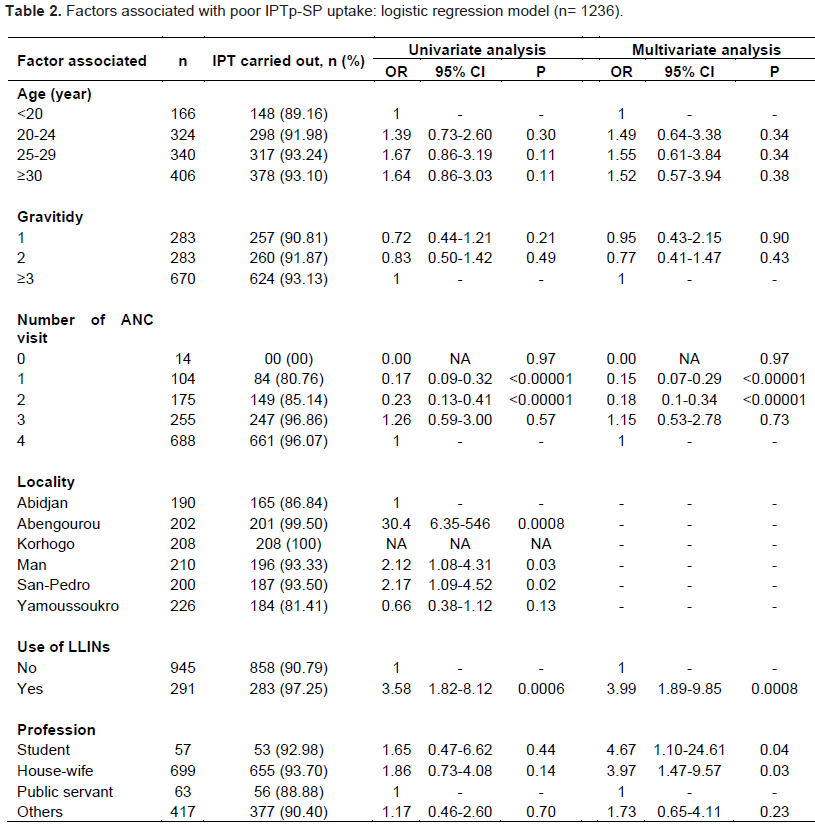
A total of 1,236 women were enrolled into the study. 1,236 women, 632 (51.1%) received three (optimal) or more doses of SP, 604 (48.9%) received two or less doses (poor uptake or suboptimal).
The percentage for completing SP doses was different between primigravida and multigravida (22.6% vs 54.9% respectively). At least four ANC visits made by a pregnant woman was associated with higher proportion of taking three or more SP doses than three or less visits (P<0.00001). Uptake of adequate SP dosage varied significantly (p < 0.0001) according to the sentinel’s site. The highest rate of participants received at least 3 doses of SP was recorded at Korhogo site (67.30%), followed by Man (51%) and Yamoussoukro, and the lowest rate was observed in Abidjan (42.60%) (Table 1). Uptake of ≥ 3 doses varied significantly (p < 0.001) according to study site, number of ANC visits and profession (Table 2).
Prevalence of LBW and associated factors
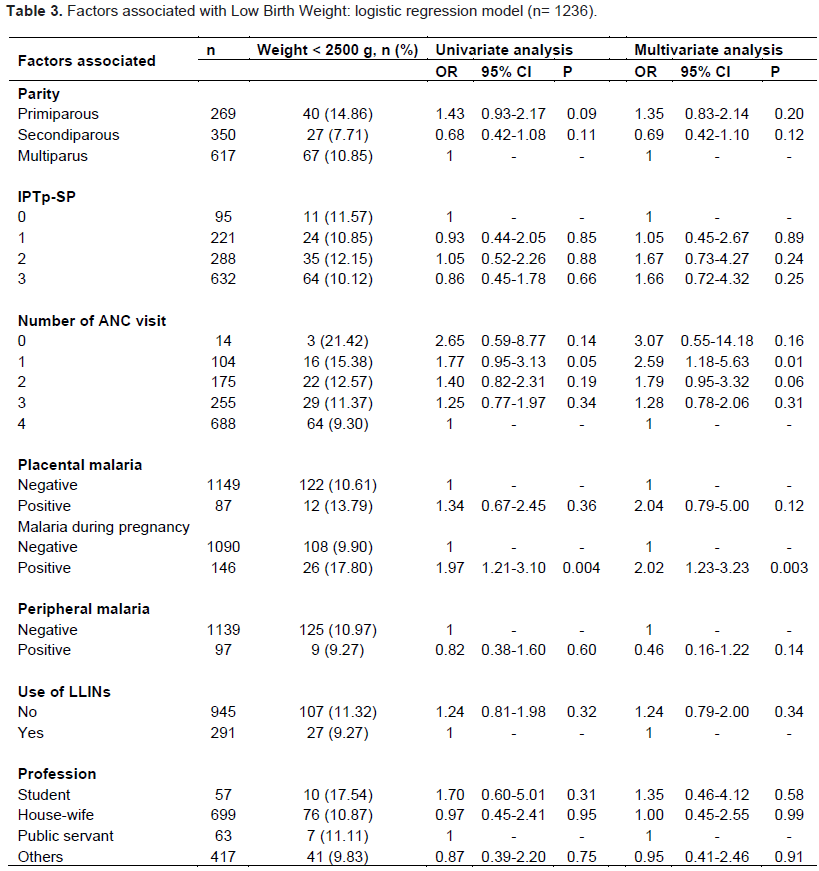
The newborn mean birth weight with one standard deviation was 3,000 (±584) g, and 10.8% (134/1,236) infants had LBW (birth weight less than 2,500 g). The factors associated with LBW in the multivariable analysis were maternal malaria during pregnancy (adjusted odds ratio: 2.02; 95% confidence interval: [1.23–3.23], only one ANC visit (adjusted odds ratio: 2.59; 95% confidence interval: [1.18–5.63] (Table 3).
Prevalence of PM and associated factors
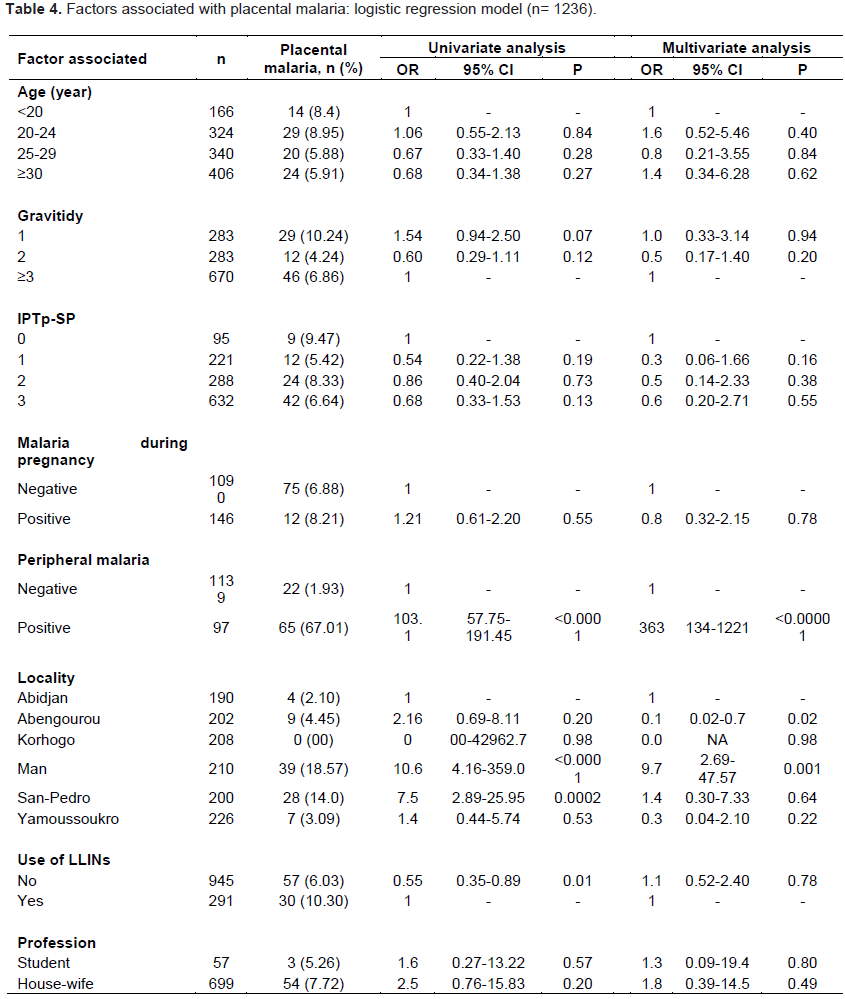
A total of 1,236 placental biopsies were collected and processed for identification of P. falciparum infection. Overall, 7.0% (87) (95% CI 15.2–22.2) women had evidence of PM. The high prevalence was observed at Man site (18.57%) followed by San-Pedro site while none of the participants presented PM at Korhogo site. PM occurred more in primigravidae than in multigravidae (10.24% vs 6.86%). The prevalence of PM in women who had peripheral blood parasitaemia was higher compared to women without peripheral blood parasitemia. The factors associated with PM in the multivariable analysis were maternal malaria at delivery (adjusted odds ratio: 363; 95% confidence interval: [134–1222], Abengourou site (adjusted odds ratio: 0.1; 95% confidence interval: [0.02–0.7] and Man site (adjusted odds ratio: 9.7; 95% confidence interval: [2.69–47.57] (Table 4). The overall prevalence of P. falciparum in maternal peripheral blood at the time of delivery was 8.5% by light microscopy while this prevalence was 13.4% during pregnancy.
DISCUSSION
The purpose of this study was to assess the effectiveness of IPTp-SP in six sentinel sites in Côte d'Ivoire since its adoption by the country in 2005. Usually, ANC serves as a means for providing necessary services during pregnancy, including the provision of insecticide-treated bed nets (ITNs) and IPTp-SP for malaria prevention. Coverage of IPTp with 3 doses of SP found in the current study was 51.1%, similar to those found in West Africa (Amankwah and Anto, 2019; Amoakoh-Coleman et al., 2020) and elsewhere (Diengou et al., 2020). However, some studies reported high coverage of IPTp-SP, more than 80% in Sierra Leone (Buh et al., 2019), Ghana (Ibrahim et al., 2017), and Tanzania (Protas et al., 2016). Nevertheless, the estimated prevalence of IPTp-SP uptake reported in this study is higher than the prevalence reported in other studies (Orish et al., 2015; Azizi et al., 2018; Azizi, 2020; Yaya et al., 2018; Anchang-Kimbi et al., 2020). The number of times ANC attended during pregnancy was positively associated with IPTp coverage, as it has been found in other studies (Nkoka et al., 2018; Yaya et al., 2018; Amoakoh?Coleman et al., 2020). Sensibilization on the dangers of malaria in pregnancy and the beneficial effects of IPTp are factors that contribute to the increase IPTp uptake. This study and the previous one in the country and in other countries in sub-Saharan Africa show that IPTp coverages are not meeting national targets due to various factors (Agarwal et al., 2015; Andrews et al., 2015). Education and timing of antenatal clinic (ANC) visits, economic power to purchase sulfadoxine-pyrimethamine (SP), and stock-outs of SP, ANC user fees, poor counselling are some factors that affected IPTp coverage (Mubyazi et al., 2014; Thiam et al, 2013; Webster et al., 2018). Several reports undertaken in sub-Saharan Africa point to obstacles at all levels of implementation: from healthcare providers, health facility, as well as at higher levels of the health system (Hill et al., 2013; Roman et al., 2019; Olaleye and Walker, 2020).
In this study uptake of adequate SP dosage varied significantly according to the site and the highest rate of participants who received at least 3 doses of SP was recorded at Korhogo in the North, followed by Man in the West and Yamoussoukro in the center. Women in rural areas seem to follow this strategy compared to those in urban areas where the lowest coverage rate has been observed (Abidjan). Achieving high coverage of at least three doses of IPTp (IPTp3) will require delivery of high-quality ANC, as recommended in the updated WHO guidance on ANC (WHO, 2016).
The prevalence of PM was 7.0%, relatively lower than that of 9.0% reported in 2014 (Toure et al., 2014), but is higher than the 4.0% reported among delivering women around the country in 2011 (Vanga-Bosson et al., 2011). In other African countries with stable malaria transmission, the prevalence of infection at delivery ranged from 8.1 to 57.8% (Rantala et al., 2010; Cohee et al., 2014; Chaponda et al., 2015; Mutagonda et al., 2016). The factors associated with PM in this study were maternal malaria at delivery and the locality (Abengourou and Man sites).
In this study, the authors found no significant association between PM and the number of IPTp-SP doses received found in others studies (Fokam et al., 2016; Yoah et al., 2018; Mikomangwa et al., 2020; Mlugu et al., 2020). This may indicate lower effectiveness of SP in clearing or preventing new malaria infection, which is probably due to parasites resistance to SP in the study area (van Eijk et al., 2019).
Although the effect of ≥ 3 doses of IPTp-SP in reducing maternal malaria infection at delivery was non-significant, there was a trend of decreasing parasite densities with increasing number of IPTp doses indicating a benefit of higher IPTp-SP uptake on reducing parasite density (Kayentao et al., 2013; Mpogoro et al., 2014; Arnaldo et al., 2018).
Primigravida were found to have increased susceptibility to PM compared to multigravida. The gravidity-dependent differences in susceptibility to malaria during pregnancy are thought to be related to the development of immunity specific to PM in the second and subsequent pregnancies. More strategies targeting this vulnerable group to improve their health and birth outcomes are needed. The other factors related to PM are locality and malaria infection at delivery.
The authors found a prevalence of LBW of 10.8%, which is higher than the prevalence rate of 9.6% reported in a previous study that demonstrated also a strong association between PM and LBW (Toure et al., 2014).
In this study the factors associated with LBW were maternal malaria during pregnancy and only one ANC visit. This study had the following limitations. First, the study participants were recruited from health facility maternity wings.
Therefore, it would not be representative of the wider population of postpartum women in the sites. Second, the study focused on determinants of IPTp-SP uptake in postpartum women from catchment areas of selected Health facilities in sentinel’s district. Results would not be generalized to all districts in Côte d’Ivoire.
CONCLUSION
The adherence to of a full course of IPTp-SP was low in the study sites compared to the national target of 80%. To effectively addressing the poor coverage and utilization rates, it is absolutely essential to identify the limiting factors in order to developing evidence-based intervention strategies.
CONFLICT OF INTERESTS
The authors have declared any conflicts of interests.
FUNDING
This research was funded by WHO Global Fund and NMCP.
REFERENCES
|
Agarwal K, Alonso P, Chico RM, Coleman J, Dellicour S, Hill J, Majeres-Lugand M, Mangiaterra V, Menendez C, Mitchell K, Roman E, Sicuri E, Tagbor H, van Eijk AM, Webster J (2015). Global Call to Action to scale-up coverage of intermittent preventive treatment of malaria in pregnancy: seminar report. Malaria Journal 14:206. |
|
|
Amankwah S, Anto F (2019). Factors Associated with Uptake of Intermittent Preventive Treatment of Malaria in Pregnancy: A Cross-Sectional Study in Private Health Facilities in Tema Metropolis, Ghana. Journal of Tropical Medicine pp. 1-11 |
|
|
Amoakoh?Coleman M, Arhinful DK, Klipstein?Grobusch K, Ansah EK, Koram KA (2020). Coverage of intermittent preventive treatment of malaria in pregnancy (IPTp) influences delivery outcomes among women with obstetric referrals at the district level in Ghana. Malaria Journal 19:222. |
|
|
Anchang-Kimbi JK, Kalaji LN, Mbacham HF, Wepnje GB, Apinjoh TO, Ngole Sumbele IU, Dionne-Odom J, Tita ATN, Achidi EA (2020). Coverage and effectiveness of intermittent preventive treatment in pregnancy with sulfadoxine-pyrimethamine (IPTp-SP) on adverse pregnancy outcomes in the Mount Cameroon area, South West Cameroon. Malaria Journal 19(1):100. |
|
|
Andrews KG, Lynch M, Eckert E, Gutman J (2015). Missed opportunities to deliver intermittent preventive treatment for malaria to pregnant women 2003GÇô2013: a systematic analysis of 58 household surveys in sub- Saharan Africa. Malaria Journal 14:521. |
|
|
Arnaldo P, Rovira?Vallbona E, Langa JS, Salvador C, Guetens P, Chiheb D, Xavier B, Kestens L, Enosse SM, Rosanas?Urgell A (2018). Uptake of intermittent preventive treatment and pregnancy outcomes: health facilities and community surveys in Chókwè district, southern Mozambique. Malaria Journal 17:109. |
|
|
Azizi SC (2020). Uptake of intermittent preventive treatment for malaria during pregnancy with Sulphadoxine-Pyrimethamine in Malawi after adoption of updated World Health Organization policy: an analysis of demographic and health survey 2015-2016. BMC Public Health 20(1):335. |
|
|
Azizi SC, Chongwe G, Chipukuma H, Jacobs C, Zgambo J, Michelo C (2018). Uptake of intermittent preventive treatment for malaria during pregnancy with Sulphadoxine-Pyrimethamine (IPTp-SP) among postpartum women in Zomba District, Malawi: a cross-sectional study. BMC Pregnancy Childbirth 18(1):108. |
|
|
Buh A, Kota K, Bishwajit G, Yaya S (2019). Prevalence and Associated Factors of Taking Intermittent Preventive Treatment in Pregnancy in Sierra Leone. Tropical medicine and infectious disease 4(1):32. |
|
|
Chaponda EB, Chandramohan D, Michelo C, Mharakurwa S, Chipeta J, Chico RM (2015). High burden of malaria infection in pregnant women in a rural district of Zambia: a cross-sectional study. Malaria Journal 14:380. |
|
|
Cohee LM, Kalilani-Phiri L, Boudova S, Joshi S, Mukadam R, Seydel KB, Mawindo P, Thesing P, Kamiza S, Makwakwa K, Muehlenbachs A, Taylor TE, Laufer MK (2014). Submicroscopic malaria infection during pregnancy and the impact of intermittent preventive treatment. Malaria Journal 13:274. |
|
|
Diengou NH, Cumber SN, Nkfusai CN, Mbinyui MS, Viyoff VZ, Bede F, Akwah L, Tsoka-Gwegweni JM, Anchang-Kimbi J (2020). Factors associated with the uptake of intermittent preventive treatment of malaria in pregnancy in the Bamenda health districts, Cameroon. Pan African Medical Journal 35:42. |
|
|
Fokam EB, Ngimuh L, Anchang-Kimbi JK, Wanji S (2016). Assessment of the usage and effectiveness of intermittent preventive treatment and insecticide-treated nets on the indicators of malaria among pregnant women attending antenatal care in the Buea Health District, Cameroon. Malaria Journal 15:172. |
|
|
Hill J, Hoyt J, van Eijk AM, D'Mello-Guyett L, ter Kuile FO, Steketee R, Smith H, Jayne Webster J (2013). Factors affecting the delivery, access, and use of interventions to prevent malaria in pregnancy in sub-Saharan Africa: a systematic review and meta-analysis. PLoS Medicine 10(7):e1001488 |
|
|
Ibrahim H; Maya ET; Issah K; Apanga PA; Bachan EG; Noora CL (2017). Factors influencing uptake of intermittent preventive treatment of malaria in pregnancy using sulphadoxine pyrimethamine in Sunyani Municipality, Ghana. The Pan African Medical Journal 28:122. |
|
|
Kayentao K, Garner P, van Eijk AM, Naidoo I, Roper C, Mulokozi A, MacArthur JR, Luntamo M, Ashorn P, Doumbo OK, ter Kuile FO (2013). Intermittent preventive therapy for malaria during pregnancy using 2 vs 3 or more doses of sulfadoxine-pyrimethamine and risk of low birth weight in Africa: systematic review and meta-analysis. JAMA 309(6):594-604. |
|
|
Mikomangwa WP, Minzi O, Mutagonda R, Baraka V, Mlugu EM, Aklillu E, Kamuhabwa AAR (2020). Effect of sulfadoxine-pyrimethamine doses for prevention of malaria during pregnancy in hypoendemic area in Tanzania. Malaria Journal 19(1):160. |
|
|
Mlugu EM, Minzi O, Asghar M, Färnert A, Kamuhabwa AAR, Aklillu E (2020). Effectiveness of Sulfadoxine-Pyrimethamine for Intermittent Preventive Treatment of Malaria and Adverse Birth Outcomes in Pregnant Women. Pathogens 9(3):207. |
|
|
Mpogoro FJ, Matovelo D, Dosani A, Ngallaba S, Mugono M, Mazigo HD (2014). Uptake of intermittent preventive treatment with sulphadoxinepyrimethamine for malaria during pregnancy and pregnancy outcomes: a cross-sectional study in Geita district, North-Western Tanzania. Malaria Journal 13:455. |
|
|
Mubyazi GM, Byskov J, Magnussen P, Bygbjerg IC, Ijumba JN, Marero M, Mboera LEG, Molteni M, Bloch P (2014). Health facility-based data on women receiving sulphadoxine-pyrimethamine during pregnancy in Tanzania: lessons to learn from a cross-sectional survey in Mkuranga and Mufindi districts and other national survey reports. Reproductive Health 11:6. |
|
|
Mutagonda RF, Kamuhabwa AAR, Minzi OMS, Massawe SN, Maganda BA, Aklillu E (2016). Malaria prevalence, severity and treatment outcome in relation to day 7 lumefantrine plasma concentration in pregnant women. Malaria journal 15:278. |
|
|
Nkoka O, Chuang TW, Chen YH (2018). Association between timing and number of antenatal care visits on uptake of intermittent preventive treatment for malaria during pregnancy among Malawian women. Malaria Journal 17(1):211. |
|
|
Olaleye AO, Walker O (2020). Impact of Health Systems on the Implementation of Intermittent Preventive Treatment for Malaria in Pregnancy in Sub-Saharan Africa: A Narrative Synthesis. Tropical Medicine and Infectious Disease 5(3):134. |
|
|
Protas J, Tarimo D, Moshiro C (2016). Determinants of timely uptake of ITN and SP (IPT) and pregnancy time protected against malaria in Bukoba, Tanzania. BMC Research Notes 9:318. |
|
|
Orish VN, Onyeabor OS, Boampong JN, Afoakwah R, Nwaefuna E, Acquah S, Sanyaolu AO, Iriemenam NC (2015). Prevalence of intermittent preventive treatment with sulphadoxine-pyrimethamine (IPTp-SP) use during pregnancy and other associated factors in Sekondi-Takoradi, Ghana. African Health Sciences 5(4):1087-96. |
|
|
Quakyi I, Tornyigah B, Houze E, Kusi KA, Coleman N, Escriou G, Laar A, Cot M, Fobil J, Asare GQ, Deloron P, Anang AK, Cottrell G, Ofori MF, Ndam NT (2019). High uptake of Intermittent Preventive Treatment of malaria in pregnancy is associated with improved birth weight among pregnant women in Ghana. , Scientific Reports 9:19034. |
|
|
Rantala AM, Taylor SM, Trottman PA, Luntamo M, Mbewe B, Maleta K, Kulmala T, Ashorn P, Meshnick SR (2010). Comparison of real-time PCR and microscopy for malaria parasite detection in Malawian pregnant women. Malaria Journal 9:269. |
|
|
Roman E, Andrejko K, Wol f K, Marianne H, Youll S, Florey L, Ferenchick E, Gutman JR (2019). Determinants of uptake of intermittent preventive treatment during pregnancy: a review. Malaria Journal 18:372. |
|
|
Thiam S, Kimotho V, Gatonga P (2013). Why are IPTp coverage targets so elusive in sub-Saharan Africa? A systematic review of health system barriers. Malaria Journal 12:353.. |
|
|
Toure OA, C Konan CB, Kouame VN, Gbessi EA, Soumahoro A, Bassinka I, Jambou R (2020). Risk factors for placental malaria and associated low birth weight in a rural high malaria transmission setting of Cote d'Ivoire. Tropical Parasitology 10(2):102-108. |
|
|
Toure OA, Kone PL, Coulibaly MA, Ako BA, Gbessi EA, Coulibaly B, N' Guessan LT, Koffi D, Beourou S, Soumahoro A, Bassinka I, Nogbou M, Swa T, Gba B, Esmel B, Bokossa EM (2014). Coverage and efficacy of intermittent preventive treatment with sulphadoxine pyrimethamine against malaria in pregnancy in Côte d'Ivoire five years after its implementation. Parasites and Vectors 7:495. |
|
|
Vanga-Bosson HA, Coffie PA, Kanhon S, Sloan C, Kouakou F, Eholie SP, Kone M, Dabis F, Menan H, Ekouevi DK (2011). Coverage of intermittent prevention treatment with sulphadoxine-pyrimethamine among pregnant women and congenital malaria in Côte d'Ivoire. Malaria Journal 10:105. |
|
|
van Eijk AM, Larsen DA, Kayentao K, Koshy G, Slaughter DEC, Roper C, Okell LC, Desai M, Gutman J, Khairallah C, Rogerson SJ, Sibley CH, Meshnick SR, Taylor SM, ter Kuile FO (2019). Effect of Plasmodium falciparum sulfadoxine-pyrimethamine resistance on the effectiveness of intermittent preventive therapy for malaria in pregnancy in Africa: a systematic review and meta-analysis. Lancet Infectious Diseases 19:546-556. |
|
|
World Health Organization (WHO) (2004). A strategic framework for malaria prevention and control during pregnancy in the African region. Brazzaville, World Health Organization, Regional Office for Africa. |
|
|
World Health Organization (WHO) (2012). Evidence Review Group: Intermittent Preventive Treatment of malaria in pregnancy (IPTp) with Sulfadoxine-Pyrimethamine (SP). WHO Headquarters, Geneva. Meeting report |
|
|
World Health Organization (WHO) (2018). Intermittent preventive treatment in pregnancy (IPTp). Geneva: World Health Organization. |
|
|
World Health Organization (WHO) (2016). World malaria report 2016. Geneva: World Health Organization. |
|
|
Webster J, Ansariadi, Burdam FH, Landuwulang CUR, Bruce J, Poespoprodjo JR, Syafruddin D, Ahmed R, Hill J (2018). Evaluation of the implementation of single screening and treatment for the control of malaria in pregnancy in Eastern Indonesia: a systems effectiveness analysis. Malaria Journal 17(1):310. |
|
|
Yaya S, Uthman OA, Amouzou A, Bishwajit G (2018). Use of intermittent preventive treatment among pregnant women in sub-Saharan Africa: evidence from malaria indicators surveys. Tropical Medicine and Infectious Disease 3:18. |
|
|
Yoah AT, Fru-Cho J, Kah E, Njukang E, Wirsiy FS, Duamor CT, Nkuo-Akenji T (2018). Impact of Adherence to a Full Course of Intermittent Preventive Treatment of Malaria in Pregnancy on Pregnancy Outcome in Muyuka Health District: A Cross-Sectional Study. International Archives of Public Health and Community Medicine 2:008. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


