Full Length Research Paper

ABSTRACT
Malaria is the world's leading parasitic endemic and the major cause of morbidity and mortality in Côte d'Ivoire. The aim of this study was to analyse the clinical aspects and evaluate a kit’s performance (NovaLisa® Malaria) against a panel of antigens (AMA1, GLURP, CSP and Schizont Extract) to determine the antigen used in diagnosing malaria serology in Côte d’Ivoire. A retrospective study was carried out on patients requesting malaria serological test. The ELISA technique and an antigen panel was respectively used for the multi-antigen approach and to measure the proportion of responders from 28 samples. 345 samples were assayed, with a positive rate of 92.49% (319/345) revealed by the malaria serology test with a mean concentration of 50.1 NTU, 6.38% (22/345) of negativity with a mean concentration of 5.96 NTU and 1.16% (4/345) in the doubtful zone (16.26 NTU). Mean concentration of prescriptions for cervical adenopathy was 73.12 NTU. The antigen panel seroprevalence was 35.72; 50; 64.28 and 78.5% respectively for AMA1, CSP, GLURP and schizont extract for negative samples and the proportion of responders was significant (p = 0.003) for schizont extract. The seroprevalence for the 28 samples was 60.7% for AMA1 and 89.29% for schizont extract. The proportions of responders to CSP (p = 0.008), GLURP (p < 0.001) and schizont extract (p < 0.001) antigens were significantly higher than those of non-responders. GLURP antigen and schizont extract could be used for diagnosing malaria serology in Côte d'Ivoire.
Key words: Malaria, Plasmodium falciparum, antigen, serodiagnosis.
INTRODUCTION
Malaria is one of the major parasitic diseases in the world and the most widespread infection in tropical and subtropical areas with high morbidity and mortality rates (Dinko and Pradel, 2016). It is a febrile erythrocytopathy caused by the genus Plasmodium and transmitted to humans through the bite of an infected female anopheline
mosquito (Pages et al., 2007). Among the five species involved in the pathology such as Plasmodium falciparum, Plasmodium ovale, Plasmodium vivax, Plasmodium malariae Plasmodium knowlesi; P. falciparum is the most virulent species (WHO, 2018). In 2018, According to the World Health Organization (WHO), the number of malaria cases was estimated to 228 million worldwide with 405,000 recorded deaths. Most cases (213 million or 93%) were recorded in the WHO African region, far ahead South-East Asia (3.4%) and the Eastern Mediterranean region (2.1%). The African region is the most affected with 94% of deaths (WHO, 2019).
In Côte d'Ivoire, malaria remains a major public health issue because of its high frequency, severity and significant socio-economic consequences (Chadi, 2014). Indeed, malaria is the leading cause of morbidity with 43% of consultation in the country's health centers with an incidence rate of 105% in the general population with 295% in children under 5 years of age (Assi et al., 2013). The most common plasmodium species encountered is P. falciparum, constituting the first cause of mortality in children under 5 years of age (Lee et al., 2009). Children and pregnant women are the most vulnerable part of the population (WHO, 2018). With the advent of Artemisinin-based Combination Therapies (ACTs) in treatment protocols, a biological confirmation of any suspected case of malaria is a necessity (WHO, 2018). This biological diagnosis is based on a number of tests including stained thick and thin blood film, rapid diagnostic tests (RDTs) and malaria serological test (Siala et al., 2010). The latter technique, according to literature, is of little interest in malaria endemic countries such as Côte d'Ivoire (Goran-Kouacou et al., 2017), except for some chronic clinical forms like progressive visceral malaria and hyper-immune malaria splenomegaly in which antibodies are at high level while parasitological investigations are most often negative (Wong et al., 2014). Malaria infection induces production of antibodies against vaccine candidate antigens including pre-erythrocytic, CircumSporozoite Protein (CSP), Liver Stage Antigen (LSA 3), Sporozoite and Liver Stage Antigen (SALSA) and erythrocytic, Apical Membrane Antigen 1 (AMA1), Glutamate Rich Protein (GLURP), Total Schizont Extract 07/03) antigens. Several sero-epidemiological studies demonstrated that the above-mentioned antigens play a key role in the acquisition of protective immunity against malaria and have been associated with a reduced risk of clinical signs of malaria (Polley et al., 2000; Osier et al., 2008; Diop et al., 2014; Adu et al., 2016). Malaria serological test is performed with commercial kits such as Malaria Novalisa Mal2 using two antigens (CSP and MSP1) from P. falciparum and CSP from P. vivax which specifically targets an antibody.
However, this test could sometimes be negative for some patients living in endemic areas such as Ivory Coast (Goran-Kouacou et al., 2017).
According to the great antigenic variability of P. falciparum during its development cycle, it is necessary to investigate through a multi antigenic approach, the diagnosis of malaria serology by a retrospective study in patients at Institut Pasteur de Côte d'Ivoire.
MATERIALS AND METHODS
Types and site of study
A retro-prospective and cross-sectional study was conducted on serum samples collected from patients for malaria serological test at the Malarialogy Unit (Department of Parasitology and Mycology) at Institut Pasteur de Côte d'Ivoire (IPCI). The retrospective study involved patients that were requested to undergo the malaria serological test from September 2016 to 2019. Demographic data (age, sex, sample origin, etc...) and results of malaria serological test were recorded. As for the prospective part, it was performed from September to November 2019 at the Department of Parasitology and Mycology.
Study population
Serum obtained from 345 patients of all ages were used for malaria serological test at Institut Pasteur de Cote d’ivoire.
Antigens and peptides
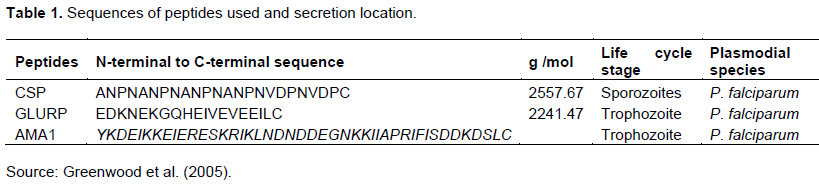
Peptides derived from the liver stage (CSP, LSA3, SALSA) and blood stage antigens (GLURP, AMA1) of P. falciparum were used to measure antibody responses. The antigen description was summarised in Table 1.
Elisa test using NovaLisa® Malaria KIT (Mal 023)
The protocol used for malaria serological test was described by the manufacturer (Nova Tec Immun diagnostica GMBH). This NovaLisa® Malaria kit was intended for the qualitative and quantitative detection of IgG/IgM antibodies against Plasmodium in human serum. It encompassed a sample dilution buffer, wash buffer, controls (negative and positive), cut-off, conjugate, TMB substrate and stop buffer. The serology plate was precoated with two antigens, P. falciparum MSP1 and P. vivax. The wells of the plate in this kit are detachable from each other.
Briefly 100 μl of the standard, controls and diluted samples (1/101) were added to their respective wells and then well A1 was used as blank substrate. The plate was covered with the lid provided in the kit and then incubated for 1 h at 37°C. At the end of this incubation, three washes were performed. Then 100 μl of the conjugate was added to all wells except blank A1 and the plate was incubated again for 30 min at room temperature (25°C). After this incubation, three washes were done and 100 μl of the TMB
Substrate Solution was added to all wells and the plate was incubated for 15 min at room temperature (25°C) in the dark. A blue colour due to the enzymatic reaction appeared and 100 μl of the Stop Solution was added to all wells in the same order and at the same rate as for TMB Substrate Solution, then a colour change from blue to yellow was observed. Absorbance was measured 30 min at 450/620 nm after adding the stop solution. The titration of each sample was determined from the following formula:
Concentration (NovaTec unit) = sample absorbance mean × 10/cut off
According to the kit when the concentration of the sample is less than 9 NTU, it is declared negative. When the sample concentration is higher than 11 NTU, it is declared positive and when the sample concentration is between 9 and 11 NTU, the sample is in the doubtful zone.
Anti-plasmodial antibody assay
ELISA technique was used to determine antibodies specific to a panel of antigens according to the method described by Courtin et al. (2009). It was made with Maxisorp®, Nunc 96-well plates. On each plate, a pool of serum from naïve individuals living in Bordeaux (France), also known as the Bordeaux Negative Control (TNB), was systematically used as a negative control, and a pool of serum from individuals living in Ivory Coast with a positive thick blood stain was used as a positive control. The test was conducted in several successive stages.
Samples were tested in triplicate (2 wells with antigen called Ag+ and one well without antigen called Ag-). 100 μg/well of each antigen (AMA1, GLURP, CSP were produced in recombinant form and kindly provided by collaborators and Total Schizont Extract) of P. falciparum, were diluted in with a concentration 1 μg / ml in coating buffer (PBS 0.5% phenol red) with the exception of Total Schizont Extract 07/03, which was diluted in 1μg / 1.2 ml. The plates were incubated at +4°C for one night. After removing the plates from the refrigerator, they were washed thrice in a washing buffer (PBS and 0.1% Tween 20). The plates were saturated with 150 μl of saturation solution (PBS, 0.1% Tween-20 and 5% milk) and incubated at 25°C for 1 h. After this incubation, they were washed three time. Serum samples to be tested, positive and negative controls were diluted respectively to a rate of 1 / 50 and 1 / 100 from the sample dilution solution (PBS, 0.1% Tween 20 and 1% milk powder and 0.02% sodium azide). 100 μl of each diluted sample and the positive and negative controls were distributed to the wells according to the plate layout and incubated at 25°C for 2 h. The plates were then removed from the incubator and washed thrice. Hundred (100) μL of anti-human IgG coupled with peroxidase and diluted at a rate of 1 / 7000 in a solution (PBS, 0.1 % Tween and 1 % powdered milk) were distributed in each well. The plates were then re-incubated at 25°C for one hour. After this incubation, the plates were washed four times and 100 μl of TetraMethyl Benzidine solution (TMB one) were added to each well, the plates were incubated for 30 min at room temperature and protected from light. The blue coloration was stopped by adding 100 μl / well of sulphuric acid (H2SO4) at 0.2 M (stop solution). Optical densities (OD) were measured by spectrophotometry at 450 nm and recorded in an Excel file. Individual results were expressed as: ΔOD = ODx - ODn, where ODx represents the mean individual OD value in wells with the antigen and ODn the mean of individual OD value in wells without antigen. The positivity threshold (PT) of the anti-Plasmodium IgG level was calculated using the following formula: PT = mean (ΔOD neg) + 3SD. The mean of (ΔOD neg) of Bordeaux individuals not exposed to Plasmodium was 0.310 for Ag-AMA1; 0.274 for Ag-CSP; 0 for Ag-Schz total extract and 0.277 for Ag-GLURP. Consequently, exposed individuals were then classified as responders to each antigen if ΔOD was above the positivity threshold respectively, 0.31 for Ag-AMA1; 0.274 for Ag-CSP; 0 for Ag-Total Schz Extract and 0.277 for Ag-GLURP.
Ethical consideration
This study was carried out according to the guidelines of the Ivorian National reference center for malaria chemoresistance created by the interministerial decree number 393/08/2006, and conduct research according to the Ivorian National Ethical Committee and Research. Therefore, this study was performed after receiving approval from the Ivorian National Ethical Committee and Research.
Data analysis
Analyses were performed using Graph Pad Prism 5.0 and Epi info 7. The Kruskal-Wallis non-parametric test was used to compare mean concentrations according to age groups. All differences were considered significant at p < 0.05. Then, the Chi-square test (χ2) was used to compare the proportion of responders and non-responders by the antigen.
RESULTS
Analysis of clinical aspects of malaria serologic tests
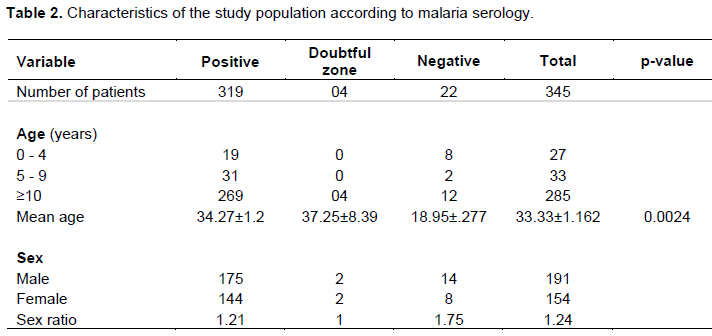
On a total of 345 patients requesting malaria serological test at the Malarialogy Unit (Institut Pasteur de Cote d'Ivoire) 319 patients were positive for malaria serology whereas 22 patients were negative and 4 patients were in the doubtful zone. Patients over 10 years of age were the most numerous among patients declared positive, negative and in the doubtful zone respectively 269; 12 and 04. The mean age of patients in our study was 33.33+ / -1.16 years. Patients positive for malaria serology were older than negative patients; 34.27 + / -1.2 years versus 18.95 + /- 4.27 years with (p = 0.0024). The sex ratio was 1.24 for men (Table 2).
Analysis of results according to the reason for requesting malaria serological test (clinical information)
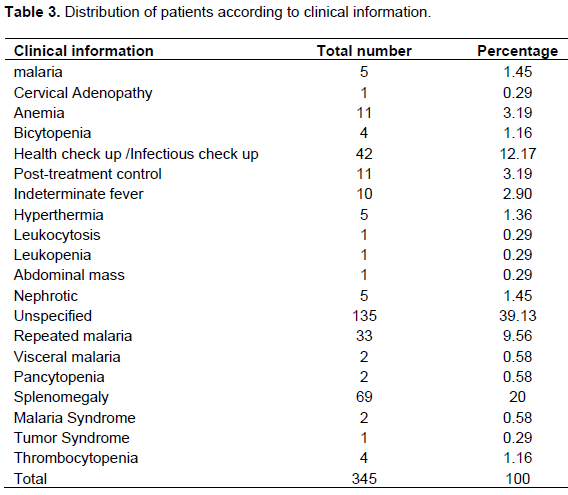
Clinical information on 135 patients (39.13%) were not specified on their analysis reports received at the Malarialogy Unit for a total of 345 patients requesting malaria serological test. Reasons for prescribing malaria serological test were due to splenomegaly with a rate of 20% (69 patients), followed by a general or an infectious check-up with a total of 42 patients (12.17%). Leukocytosis; abdominal mass; tumour syndrome; leukopenia and cervical adenopathy were the causes for requesting malaria serological test with the lowest rate of 0.29% (1 patient) (Table 3).
Relation between mean concentration of IgG antimalarial antibodies and clinical information
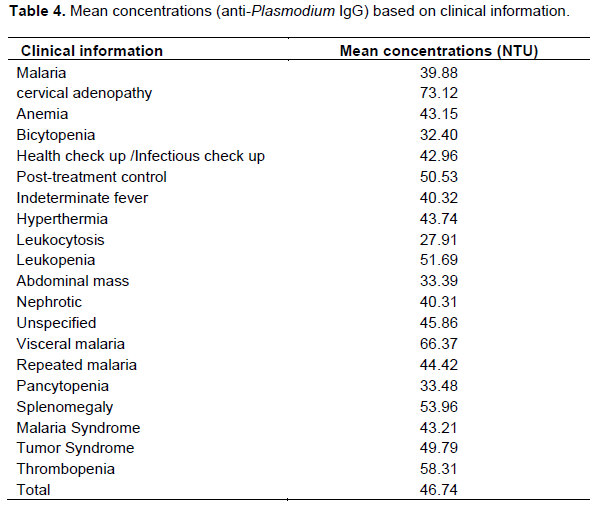
The mean concentration of IgG antimalarial antibodies was above 11 NTU for all causes for requesting malaria serological test. The mean concentration ranged from 27.91 NTU (lowest concentration) for leukocytosis to 73.12 NTU (highest concentration) for cervical lymphadenopathy as clinical information. Causes for prescribing malaria serology, such as visceral malaria, thrombocytopenia, splenomegaly, leukopenia and post-treatment control, had a mean concentration of antimalarial IgG antibodies higher than 50 NTU, respectively 66.37, 58.31, 53.96, 51.69 and 50.53 NTU (Table 4).
Analysis of mean concentration according to malaria serological test results
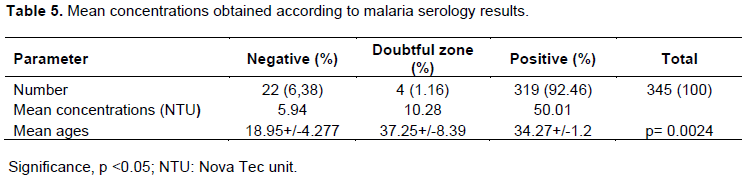
On a total of 345 serum samples received for malaria serology, 319 samples were positive, with a positivity rate of 92.46% with a mean concentration of antimalarial antibodies of 50.1 NTU; 22 serum samples with 6.38% of patients were declared negative for malaria serological test with a mean concentration of 5.94 NTU and 4 patients with 1.16% had a mean concentration of antimalarial antibodies of 10.26 NTU and all 4 patients were in the doubtful zone (Table 5).
Relation between mean concentration of malarial antibody and age
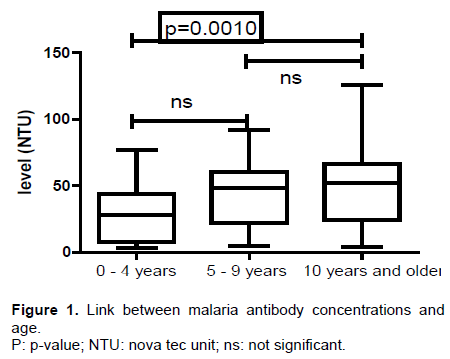
The relation between the concentration of anti-malarial antibodies and age was made by categorizing the study population by age group: 0 to 4 years, 5 to 9 years and 10 years and over. It was noted that the mean concentration of anti-malarial antibodies increases with age. The mean concentration was 29.33; 44.39 and 48.66 NTU respectively in patients with age groups from 0 to 4 years; from 5 to 9 years and eventually in patients over 10 years old. A difference was observed between the mean concentrations of antimalarial antibodies produced by patients with 10 years of age and over was significantly higher than that produced by patients with an age ranging from 0 to 4 years (Figure 1).
Antimalarial antibody responses directed with a panel of P. falciparum antigens
On a total of 345 samples were received for malaria serological test, 26 were negative against 319 positives. Thus 14 samples in each group (negative and positive samples) were included in this part of this study. In fact, 14 samples were randomly selected from the group of patients who were positive for the test. As for the negative samples they were all included except 12 serums with an insufficient quantity and quality for ELISA test.
Comparison of sero-prevalence according to antigens tested for seronegative samples
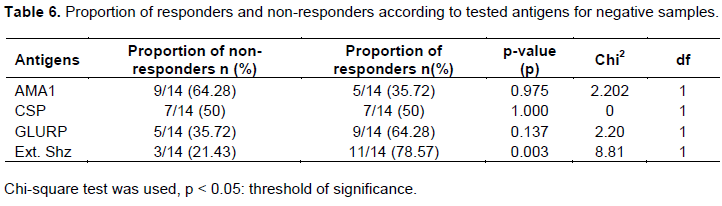
For negative samples, the seroprevalence was 35.72, 50, 64.28 and 78.57% respectively for AMA1, CSP, GLURP and total schizont extract antigens. It ranged from 35.72% for AMA1 to 78.57% for total schizont extract antigen. However, the proportion of responders was significantly higher than that of non-responders (p = 0.003) for total schizont extract (Table 6).
Comparison of seroprevalence according to tested antigens in samples using ELISA
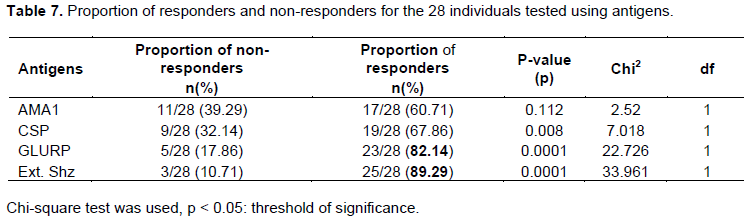
Concerning the 28 samples from which 14 samples were positive and 14 samples negative for malaria serology, the seroprevalence for all tested antigens was over 50%. It ranged from 60.71% for AMA1 to 89.29% for total schizont extract. However, proportions of responders to CSP (p = 0.008); GLURP (p < 0.0001) and total schizont extract (p < 0.0001) antigens were significantly higher than those of non-responders (Table 7).
DISCUSSION
The aim of this study was to use a multi antigenic approach to analyse malaria serodiagnosis examinations and then ponder on the clinical aspects of patients at Institut pasteur de Côte d'Ivoire. Malaria serology positivity was 92.46%, meaning that most patients had persisting antimalarial antibodies.
The mean age of patients in this study was 33.33 years with extremes from 0 to 88 years. The seroprevalence (92.46%) could be explained by the fact that Ivory coast is a stable malaria endemic zone and people living there are exposed to malaria. Children and pregnant women seem to be the most affected (WHO, 2018).
This same reason may explain the fact that there are almost as many men as women in this study with a ratio of 1.24 for men. However, there is a significant difference between the mean concentration observed in patients from 0 to 4 years old and patients from 10 years old and over. Indeed, the permanent contact of the host with the parasite and mosquito bites could lead to a rapid development of host immunity (Marsh and Snow, 1999; Doolan et al., 2009).
Studies indicate that immunity increases with age (Greehouse et al., 2011). This is due to the repetition of P. falciparum malaria infections (Gupta et al., 1999). The studies of Diarra et al. (2012) in Burkina Faso, Mbengue et al. (2016) in Senegal and Yao et al. (2017) in Côte d'Ivoire showed that patients over 10 years of age respond well to Plasmodium antigens than younger children, they might be well protected. In malaria endemic zones, acquisition of immunity occurs with age, the youngest are less protected than older children or adults (Grobusch and Kremsner, 2005). Younger children acquire this immunity during different malaria episodes (Gupta et al., 1999).
The results of this study showed that the reasons for prescribing malaria serological test were dominated by splenomegaly with a rate of 20%. This could be explained by the fact that after the invasion of red blood cells some merozoites are sequestered in the spleen (Talman et al., 2004), increasing its volume. Splenomegaly is therefore part of the chronic forms of malaria in which parasitological research is often negative while antibody concentrations are high (WHO/ UNICEF, 2015). These results are similar to those of Goran-Kouacou et al. (2017). In their studies, these authors obtained a splenomegaly rate of 49.3% as a reason for prescribing malaria serological test. Clinical information was mentioned for 210 patients out of 345, about 60.87% of the reports received. The missing clinical information was 39.13% due to an incorrect completion of the medical analysis request forms and a poor management of record books and patient files. All the information recorded on the analysis bulletins was important for a correct interpretation of results and therefore important for patients’ management, and draw the attention of clinicians and all health personnel. The antiplasmodial antibody concentration ranged from 27.91 to 73.12 NTU and was high in majority of patients. Mean anti-Plasmodium antibody concentrations based on clinical information showed that these concentrations were high for cervical adenopathy (73.12 NTU). However, for all clinical information the mean antibody concentrations were high. Besides, antibody concentrations are proportional to the intensity and duration of infestation (Goran-Kouacou et al., 2017).
The second part of this study was to assess kit’s performance against a panel of antigens (AMA1, GLURP, CSP and Total Schizont Extract) in order to determine which antigen could be used in the diagnosis of malaria serology in Ivory Coast instead of Novalisa test kit. However, seroprevalence was exclusively tested with P. falciparum antigens. Thus, the seroprevalence for 28 samples was assessed from which 14 samples were negative and the other 14 samples were positive to malaria serology with a panel of antigens (AMA1, GLURP, CSP and Total Schizonte Extract) of P. falciparum. This seroprevalence was 35.72; 50; 64.28 and 78.57% respectively for AMA1; CSP; GLURP and Total Schizont Extract antigens for the 14 negative samples and 60.71; 67.86; 82.14 and 89.29% in the same order for the 28 samples. The proportion of responders was high for all samples. A study conducted in Ivory Coast by Coulibaly et al. (2016) found anti-P. falciparum IgG antibodies in all patients during severe malaria. However, a significant difference was observed between responders and non-responders for CSP and GLURP antigens and total schizont extract, in contrast to the group of 14 negative samples the proportion of responders was significant for total schizont extract compared to non-responders. The proportion of responders was more than 50% for all antigens in tested samples (28 samples). This high seroprevalence highlights the antigenic polymorphism of P. falciparum, which could vary from one country to another and within the same country from one region to another. A study in Tanzania found out a high seroprevalence of anti AMA 1 antibodies (40.7%) (Stewart et al., 2009). The study by Kusi et al. (2014) conducted in Ghana showed a high seroprevalence of anti AMA1 and CSP antibodies. A high prevalence of PfMSP1 and PfAMA1 antibodies was found in Indonesia notwithstanding the region and season (Supargiyono et al., 2013). This study showed that the most immunogenic and promising antigens are Total Schizont Extract and GLURP. The proportions of responders to GLURP and Total Schizont Extract antigens were high among the antigens used compared to non-responders. GLURP is described as highly immunogenic. The results obtained are consistent with those of Mbengue et al. (2016) who showed that the GLURP antigen was the most immunogenic during urban malaria in Dakar, Senegal. Therefore, GLURP and Total schizont extract could be serological markers for the diagnosis of malaria serology in Côte d'Ivoire.
In this study some limitations were observed. Firstly, the lack of some data, namely the place of residence and patients’ nationality was not mentioned in the record book. These parameters should have been important for the immunological analysis of patients. Another limitation is the low number of patients used in the second part of this study. In fact analysis of all malaria seronegative samples and even all samples received could provide good results.
CONCLUSION
On completion of this study, it was found that for all samples, the positive patients (92.46%) were more numerous than the negative (6.38%) and those from the doubtful zone (1.16%) according to the malaria serological test using the kit. Unspecified reasons for requesting malaria serological test test were the most numerous. Splenomegaly was the most frequent reason for prescription. It is therefore important to draw the attention of clinicians to put the relevant information on the medical analysis bulletins, for a better management. It should be noted that mean concentrations were high according to clinical information.
Concerning the antigen panel approach, the proportion of responders was significantly high for CSP and GLURP antigens and total schizont extract for all individuals tested compared to non-responders, the proportion of responders was significant only for total schizont extract compared to non-responders for negative samples to malaria serological test. GLURP antigen and Total Schizonte extract could be used as a malaria serological test in Côte d'Ivoire. The time of patient's stay in Côte d'Ivoire and place of residence were not mentioned in this study. This is a limitation to this study.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGEMENTS
The authors are very grateful to all the participants for the realization of this study and appreciate all the staff and students of the Department of Parasitology-Mycology of the Institut Pasteur de Cote d'Ivoire for their respective involvement in the realization of this study. Authors also thank the staff of the Sample Reception Unit at the Institut Pasteur de Cote d'Ivoire and the management of the Institut Pasteur for allowing the study to be carried out.
REFERENCES
|
Adu B, Cherif MK, Bosomprah S, Diarra A, Arthur FKN, K Dickson EK, Corradin G, Cavanagh DR, Theisen M, Sirima SB, Nebie I, Daniel DD (2016). Antibody levels against GLURP R2, SP1 block 2 hybrid and AS202.11 and the risk of malaria in children living in hyperendemic (Burkina Faso) and hypo-endemic (Ghana) areas Bright. Malaria. Journal 15:123. |
|
|
Assi SB, Henry MC, Rogier C, Yovo JD, Audibert M, Mathonnat J, Teuscher T, Carnevale P (2013). Inland valley rice production systems and malaria infection and disease in the forest region of western Côte d'Ivoire. Malaria Journal 12(233):1-13. |
|
|
Chadi F (2014). Le paludisme en Côte d'Ivoire Etat des lieux, stratégies de lutte. Thèse pour l'obtention du diplôme d'état de docteur en pharmacie. UFR des sciences pharmaceutiques, Université Bordeaux, Bordeaux (France) 144 p. |
|
|
Coulibaly M, Sansan H, Kouakou P, Yeboah R, Timité AM, Sombo MF (2016). Titrage des immunoglobulines G anti-Plasmodium falciparum chez les enfants atteints de paludisme grave au CHU de Yopougon. Revue Malienne d'Infectiologie et de Microbiologie 2016, Tome 8. |
|
|
Courtin D, Oesterholt M, Huismans H, Kusi K, Milet J, Badaut C, Gaye O, Roeffen W, Remarque EJ, Sauerwein R, Garcia A, Luty AJ (2009). The quantity and quality of Africanchildren's IgG responses to merozoite surface antigensreflect protection against. Plasmodium falciparum malaria. PLoS One 4(10):e7590. |
|
|
Diarra A, Nebie I, Tiono A, Soulama I, Ouedraogo A, Konate A, Theisen M, Dodoo D, Traore A, Sirima SB (2012). Antibodies to malaria vaccine candidates are associatedwith chloroquine or sulphadoxine/pyrimethaminetreatmentefficacy in children in an endemic area of Burkina Faso. Malaria. Journal 11(1):79-84. http://www.malariajournal.com/content/11/1/79 |
|
|
Dinko B, Pradel G (2016). Immune evasion by Plasmodium falciparum parasites: converting a host protection mechanism for the parasite's benefit. Advances in Infectious Diseases 6(2):82-95. 95. |
|
|
Diop F, Richard V, Diouf B, Sokhna C, Diagne N, Trape JF, Faye MM, Tall A, Diop G, Balde AT (2014). Dramatic declines in seropositivity as determined with crude extracts of Plasmodium falciparum schizonts between 2000 and 2010 in Dielmo and Ndiop Senegal. Malaria Journal 13(1):83-91 |
|
|
Doolan DL, Dobaño C, Baird JK (2009). Acquiredimmunity to malaria. Clinical. Microbiology. Reviews 22(1):13-36. |
|
|
Goran-Kouacou VPA, Dou GS, Zika KD, Adou AH, Yéboah OR, Aka RA, Hien S, Siransy LK, N'guessan K, Djibangar TA, Dassé SR Adoubryn KD (2017). Sérologie palustre : quel apport dans un pays d'endémie palustre comme la Côte d'Ivoire ? Pan African medical journal. 26: 221-227 |
|
|
Greenwood BM, Bojang K, Whitty CJM, Targett GAT (2005). Malaria. Lancet 365(9469):1487-1498. |
|
|
Grobusch MP, Kremsner PG (2005). Uncomplicated malaria. Current Topics in Microbiology and Immunology 295:83-104 PMID: 16265888. |
|
|
Gupta S, Snow RW Donnelly C, Newbold C (1999). Acquired immunity and postnatal clinical protection in childhood cerebral malaria. Proceedings Biological Sciences 266(1414):33-38. |
|
|
Kusi KA, Bosomprah S, Dodoo D, Kyei-Baafour E, Dickson EK, Mensah D, Angov E, Dutta S, Sedegah M, Koram KA (2014). Anti-sporozoite antibodies as alternative markers for malaria transmission intensity estimation. Malaria journal 13(1):103-113 |
|
|
Lee KS, Cox-Singh J, Brooke G, Matusop A, Singh B (2009). Plasmodium knowlesi fro marchival blood films:Further evidence that human infections are widely distributed and not newly emergent in Malaysian Borneo. International Journal of Parasitology 39 (10):1125- 1128. |
|
|
Marsh K, Snow RW (1999). Malaria transmission and morbidity. Parassitologia 41(1-3):241- 246. PMID: 10697862. |
|
|
Mbengue B, Kpodji P, Sylla NM, Varela ML, Thiam A, Sow A, Ndiaye K, Aidara M, Thiam F, Ndiaye R, Diop G, Nguer CM, Perraut R, Dièye A, (2016). Profiles of IgG responsesagainst CSP, GLURP and LSA-3NR2 in urban malaria (Dakar): relations with haemoglobin levels and parasite densities. Bulletin De La Société De Pathologie Exotique 109(2):91-98. |
|
|
Osier FH, Fegan G, Polley SD, Murungi L, Verra F, Tetteh KK, Lowe B, Mwangi T, Bull PC, Thomas AW, Cavanagh DR, Mcbride JS, Lanar DE, Mackinnon MJ, Conway DJ, Marsh K (2008). Breadth and magnitude of antibody responses to multiple Plasmodium falciparum merozoite antigens are associated with protection from clinical malaria. Infection and Immunity 76(5):2240-2248. |
|
|
Pages F, Orlandi-Pradines E, Corbel V (2007). Vecteurs du paludisme : biologie, diversité, contrôle et protection individuelle. Médecine et Maladies Infectieuses 37:153-161. |
|
|
Polley SD, Mwangi T, Kocken CH, Thomas AW, Dutta S, Lanar DE, Remarque E, Ross A, Williams TN, Mwambingu G, Lowe B, Conway DJ, Marsh K (2004). Human antibodies to recombinant protein constructs of Plasmodium falciparum Apical Membrane Antigen1 (AMA1) and their associations with protection from malaria. Vaccine 23 (5):718-728. |
|
|
Siala E, Ben Abdallah R, Bouratbine A, Aoun K (2010). Actualités du diagnostic biologique du paludisme. Revue Tunisienne d'Infectiologie 4(1):5-9. |
|
|
Stewart L, Gosling R, Griffin J, Gesase S, Campo J, Hashim R, Masika P, Mosha J, Bousema T, Shekalaghe S, Cook J, Corran P, Ghani A, Riley EM, Drakeley C (2009). Rapid assessment of malaria transmission using Age-specific sero-conversion rates. PLoS One 4(6):e6083 |
|
|
Supargiyono S, Bretscher MT, Wijayanti MA, Sutanto I, Nugraheni D, Rozqie R, Kosasih AA, Sulistyawati S, Hawley WA, Lobo N, Cook J Drakeley CJ, (2013). Seasonal changes in the antibodyresponsesagainstPlasmodium falciparum merozoite surface antigens in areas of differing malaria endemicity in Indonesia. Malaria Journal 12(1):444- 455. |
|
|
Talman AM, Domarle O, McKenzie FE, Ariey F, Robert V (2004). Gametocytogenesis: the puberty of Plasmodium falciparum. Malaria Journal 3(1):24-38 |
|
|
Wong J, Hamel MJ, Drakeley CJ, Kariuki S, Shi YP, Lal AA, Nahlen BL, Bloland PB, Lindblade KA, Were V, Otieno K, Otieno P, Odero C, Slutsker L, Vulule JM Gimnig JE (2014). Serological markers for monitoring historical changes in malaria transmission intensity in a highly endemic region of Western Kenya, 1994-2009. Malaria Journal 22(13):451-465. |
|
|
World Health Organization (WHO) (2018). Rapport sur le paludisme dans le monde, Genève (suisse), 210 p |
|
|
World Health Organization (WHO) (2019). World malaria report, Genève (suisse), 232p. |
|
|
WHO/UNICEF (2015). Atteinte de la cible des OMD pour le paludisme : inversion de la tendance entre 2000 et 2015. |
|
|
Yao SS, Offianan AT, Tiacoh NL, Ako AAB, Koffi D, Kouame E, Tuo K, Beourou S Djaman J (2017). Associations between IgG antibodyresponses to multiple Plasmodium falciparum antigens and treatmentoutcomeswith ACTs in Man, Côte d'Ivoire, African. African Journal of Parasitology 4(7):234 |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


